Embed Size (px)
DESCRIPTION
Â
Citation preview
Care of Adults in the Emergency Department, Theatres and Anaesthetics and Critical Care Services
Noble’s Hospital, Isle of Man
Visit Date: 26th November 2013 Report Date: April 2014
Images courtesy of NHS Photo Library and Department of Health, Isle of Man
INDEX
Introduction .......................................................................................................................................................... 3
Emergency Department ........................................................................................................................................ 4
Theatres and Anaesthetics .................................................................................................................................... 6
Critical Care .......................................................................................................................................................... 8
Systemic Issues ..................................................................................................................................................... 9
Appendix 1 Membership of Visiting Team..................................................................................................... 14
Appendix 2 Compliance with Quality Standards ............................................................................................ 15
Emergency Department ..................................................................................................................................... 18
Theatres & Anaesthetics .................................................................................................................................... 33
Critical Care ........................................................................................................................................................ 44
Version No. Date Change from Previous Version
V1 28.02.14 N/A
V2 25.03.14 Small change to wording Section 5: Commissioning (page 11)
V2.1 08.04.14 Proof reading changes and addition of two footnotes
WMQRS Iom ED TA CC Report V2.1 20140408 3
INTRODUCTION
This report presents the findings of the review of the care of adults in the Emergency Department, theatre and
anaesthetic, and critical care services which took place on 26th November 2013. The purpose of the visit was to
review compliance with: West Midlands Quality Review Service (WMQRS) Quality Standards for:
Urgent Care: Hospital-wide and Emergency Department, Version 2 Draft 7
Theatre and Anaesthetic Services, Version 1, November 2013
Cheshire and Mersey Critical Care Network ‘Service Specification for Adult Critical Care’, 2012.
These Quality Standards are based on latest English guidance on effective healthcare and form the basis of the
external quality assurance of Isle of Man health services commissioned by the Isle of Man Department of Health.
The aim of all WMQRS standards and review programmes is to help to improve clinical outcomes and service
users’ and carers’ experiences by improving the quality of services. The specific aims of the Isle of Man review
programme are:
1 To provide an assessment to the Manx public, politicians and the Isle of Man Health Service itself of the
quality of care provided to Manx patients.
2 To identify areas where services are in need of improvement, with special reference to any areas in which
there is an unacceptable risk to patient and/or staff safety.
3 To comment upon the sustainability, or otherwise, of services currently provided in the Isle of Man.
The report reflects the situation at the time of the visit. The text of this report identifies the main issues raised
during the course of the visit. Appendix 1 lists the visiting team which reviewed the services at Noble’s Hospital.
Appendix 2 contains the details of compliance with each of the standards and the percentage of standards met.
During the course of the visit, the visiting team met with some members of Tynwald, some patients and a wide
range of staff. The visiting team also looked at the responses to 75 patient and carer questionnaires (Emergency
Department: 35; Theatres and Anaesthetics: 30; Critical Care: 10), other written feedback from patients and
members of Tynwald and a range of written evidence provided by the services being reviewed.
Most of the issues identified by quality reviews can be resolved by providers’ own governance arrangements and
many can be tackled by the use of appropriate service improvement approaches. Individual organisations are
responsible for taking action and monitoring this through their usual governance mechanisms. The Isle of Man
Department of Health is responsible for ensuring action plans are in place and monitoring their implementation.
ABOUT WEST MIDLANDS QUALITY REVIEW SERVICE
WMQRS was set up as a collaborative venture by NHS organisations in the West Midlands to help improve the
quality of health services by developing evidence-based Quality Standards, carrying out developmental and
supportive quality reviews - often through peer review visits, producing comparative information on the quality of
services and providing development and learning for all involved.
Expected outcomes are better quality, safety and clinical outcomes, better patient and carer experience,
organisations with better information about the quality of clinical services, and organisations with more
confidence and competence in reviewing the quality of clinical services. More detail about the work of WMQRS is
available on www.wmqrs.nhs.uk
ACKNOWLEDGMENTS
West Midlands Quality Review Service would like to thank the staff and service users and carers of
Noble’s Hospital for their hard work in preparing for the review and for their kindness and helpfulness during the
course of the visit. Thanks are also due to the visiting team and their employing organisations for the time and
expertise they contributed to this review.
WMQRS Iom ED TA CC Report V2.1 20140408 4
EMERGENCY DEPARTMENT
General Comments and Achievements
Staff in the Emergency Department (ED) were caring and committed to providing good patient care. Thirty-five
patient feedback questionnaires showed that patients were generally very satisfied with the care they had
received, although a few patients commented on the length of time they had to wait to be seen. The Department
was starting to engage with the Cheshire and Merseyside Critical Care Network on the management of trauma.
Good Practice
1 The Department had actively adopted the ‘Releasing Time to Care’ initiative and there was good evidence
of implementation of improvements as a result.
2 An Associate Specialist was running a ‘see and treat’ training programme for nursing staff.
3 The Air Ambulance Service provided a good, resilient system for transfer of patients between Emergency
Departments with clear and comprehensive documentation and guidelines.
Immediate Risks: No immediate risks were identified.
Concerns
1 See also Systemic Issues section of this report (all sections)
2 Trauma
The Department’s system of managing patients with trauma did not meet expected UK Standards. In
particular, general and orthopaedic surgeons and anaesthetists were not routinely called for trauma
patients. Trauma surgery lists were not available daily and guidelines on the management of trauma were
not in place. Afternoon orthopaedic trauma lists were scheduled on Tuesdays to Fridays only. The hospital
response to the draft report was that Monday sessions were sometimes run when theatre staffing was
sufficient and other lists cancelled but theatre utilisation data did not confirm this. Reviewers were
concerned that the number of trauma patients seen by clinicians in the Department was too low for clinical
competence to be maintained.
3 Senior Medical Staffing and Competences
Senior medical staffing of the Emergency Department comprised one consultant and two associate
specialists. Eight specialty doctors provided middle-grade cover, supported by four F2 doctors. These staff
were highly committed to supporting the Department but the number of patients seen was so low (27,000
new attendances per annum) that reviewers found it difficult to see how competence in Emergency
Medicine was being maintained1. Some medical staff did not have up to date advanced trauma-related life
support competences.
4 Data Collection
Data on most ED Clinical Quality Indicators were not available for reviewers to see. Clinical performance
could not therefore be compared with other Emergency Departments.
Further Consideration
1 Reviewers encouraged senior medical staff to review the time spent in patient areas of the Department.
The Department was not meeting the Standard of 16 hours per day of senior medical staff presence in the
Emergency Department. Reviewers suggested that the impact of this could be mitigated if senior staff were
more actively involved in supervising and training other staff during the time that they were available.
1 Conclusion based on The College of Emergency Medicine ‘Emergency Medicine Operational Handbook: The Way Ahead’. Version 2. December 2011.
WMQRS Iom ED TA CC Report V2.1 20140408 5
2 In relation to the care of patients with trauma, senior staff in the Department did not appear fully to
appreciate the principles behind the introduction of standards for the care of people with trauma. Some
services were being offered which would, in England, be confined to Major Trauma Centres, for example,
treatment of pelvic injuries. In practice, the low level of trauma activity on the Isle of Man may be more
appropriate for a ‘Local Emergency Hospital’, possibly combined with bringing in specific staff with
appropriate competences during race weeks. Reviewers were told of plans to link with Aintree Hospital but
it was not clear how these were being progressed or that clinical staff were committed to this approach.
3 Given the issues raised above relating to number of patients attending the Emergency Department and,
specifically, the number of patients with trauma, further strategic consideration should be given to the type
of service which the Department is expected to provide and how competence can be maintained.
Reviewers considered that a number of solutions were possible which would meet the needs of the Isle of
Man population while ensuring appropriate maintenance of competence. Possible solutions include
stabilisation and transfer of all seriously ill patients and rotation of staff with other services in order to
maintain competences, possibly combined with bringing in additional staff during race weeks. In any case,
linking with another service for guideline development, training and audit should be considered.
4 Data on the proportion of patients admitted were not available but, based on verbal information from staff,
the proportion of patients admitted was high compared to Emergency Department services in England.
Reviewers considered that the number of admissions could be reduced significantly and quickly by work on
a small number of common pathways. Dedicated day case facilities were not available and the day case rate
was reported as 30%. These data suggest considerable scope for improving efficiency and reducing
pressure on in-patient beds.
5 Some nursing staff were permanently on night shifts (although only one had a permanent night shift
contract). Permanent night work may result in difficulty in accessing training and development, clinical
supervision, a lack of contact with senior medical staff and a lack of understanding of expected clinical
practice and is therefore not recommended.
6 Reviewers were given varying views about arrangements for liaison between the Emergency Department
and both mental health and drug and alcohol services. Some staff said that patients could wait a
considerable time before receiving an appropriate assessment or direction to an appropriate service but
the results of an audit showed that response times were usually within the expected timescales. Further
joint work in this area may be helpful.
7 The patient surveys returned (35) indicated a significant lack of discharge information for patients.
Reviewers were told that GPs were sent a letter up to 10 days after the patient’s attendance when coding
was delayed. Further consideration should be given to providing discharge information to patients. This
also has the potential to streamline the process of getting information to GPs.
8 Staffing did not appear to be organised to meet fluctuations in attendances as shift patterns were rigidly
organised. More flexible staffing arrangements might improve the service’s ability to match staffing to
demand.
9 An urgent care group as described in the Quality Standards was not yet in place. Reviewers suggested that
this could be a useful forum for resolving some of the operational issues with other departments.
Return to Index
WMQRS Iom ED TA CC Report V2.1 20140408 6
THEATRES AND ANAESTHETICS
General Comments and Achievements
Staff working in theatres and anaesthetics were keen, committed and highly experienced. Staff were open,
welcoming and focussed on improving patient care. A chronic pain service had been developed. The patient and
carer survey which had been undertaken showed that patients were very satisfied with the service they received.
Good Practice
1 The theatre environment was clean, calm, uncluttered, quiet and bright.
Immediate Risk
1 Staff Vacancies and 24/7 Emergency Theatre
Vacancy levels for theatre nurses and operating department practitioners (ODPs) were high. The service
had 14.25 wte vacancies (of which 5.5 wte were newly created posts) out of an establishment of 64.6 wte
(excluding housekeepers) (22%). Theatres were sometimes staffed with one theatre nurse, one ODP and
one circulatory nurse which is below the level recommended by the Association for Perioperative
Practitioners. This issue was compounded by a shortage of ‘scrub midwives’ for Caesarean sections. Only
one ODP was available out of hours which was a particular problem for Caesarean sections and because of
the lack of a daytime emergency theatre.2
An emergency theatre or alternative arrangements for timely access to emergency surgery was not
available during daytime hours. Staff would interrupt other theatre lists if a patient needed life-saving
emergency surgery. However, in 2012 61% of emergency patients were operated on outside of normal
working hours. This issue links with the lack of a daily trauma list (see Emergency Department above).
Concerns
1 See also Systemic Issues section of this report (all sections)
2 Actions Noble’s Hospital committed to take in response to the Immediate Risk (9.12.13):
“Monitor recruitment and take action accordingly
Maintain Agency staffing levels to complement existing staffing
Monitor Theatre lists weekly. The Divisional Manager will meet with the Theatre Manager each week to review the forthcoming lists for the following week and ensure that adequate staffing levels are in place for all lists. Should this not be the case action will be taken to ensure staffing is adequate and meets the AfPP guidance.
Amalgamate Theatres lists as necessary.
Cancel Theatre lists as necessary.
Cancel Theatre lists should staffing levels not be appropriate.
Audit Theatre lists against UK lists as many of our Theatre lists contain many local cases, day cases and endoscopies which may be higher than the average in the UK.
Maternity will be reminded that they must use their own midwifery team to scrub rather than telephoning Theatre as the first option.”
WMQRS response: These actions should ensure appropriate staffing for lists which are run but do not ensure appropriate availability of theatres, including for emergencies. The wording of the Immediate Risk has been revised to make this point clearer. Reviewers were aware of an external review which suggested that a 24/7 Emergency Theatre was not necessary because of the small number of patients requiring emergency surgery. The WMQRS finding is not inconsistent with this external review. Timely surgery for emergency patients could be achieved 24/7 by flexible use of theatres and staffing without having a staffed theatre ‘standing empty’ at all times. The reviewers’ concern was that this was not being achieved at the time of the review.
WMQRS Iom ED TA CC Report V2.1 20140408 7
2 WHO Checklist
Reviewers were seriously concerned that the World Health Organisation Safer Surgery Checklist was not
always completed. This had been shown by a departmental audit and reviewers observed a lack of team
briefs. It was also not clear that all surgeons and anaesthetists were committed to implementation of the
Checklist.
3 Consent
Consent for elective surgery was being done on the day of surgery which did not comply with latest
guidance on best practice. Both copies of the consent form were not signed on some of the case notes seen
by reviewers.
4 Staff Training and Development
Limited up to date training records were available and it was not clear that all staff had appropriate
competences for their work, including Association of Anaesthetists of Great Britain and Ireland (AAGBI)
competences for post-anaesthetic staff and training in use of equipment. Staff had little time available for
training because of the high level of vacancies although there were plans to start to use the AAGBI
competences from 2014 and preparations for this were underway. Training in equipment and timescales
for updating on equipment were not clearly defined.
5 Consultant Anaesthetist Staffing
Consultant staffing levels were low with eight consultants and three middle grade doctors. Advertisements
had been placed for three new consultant posts and a further three posts were being considered.
Consultant anaesthetists were covering a wide range of responsibilities, including theatres, maternity,
critical care and the air ambulance.
6 Critical Care Unit Overflow
When the critical care unit did not have sufficient capacity, patients were cared for in recovery. This area
was separate from the critical care unit and medical cover was stretched even further when it was in use.
Further Consideration
1 Although paediatric anaesthesia services were not reviewed in detail on this visit, reviewers noted that
arrangements for organisation of lists and separation of children and adults in recovery may not be fully
compliant with expected standards. This will be looked at in detail during the review of paediatric
anaesthesia.
2 Reviewers suggested that further ‘capacity and demand’ work is undertaken. The lack of a 24/7 Emergency
Theatre and daily trauma lists, and the presence of some waiting lists for surgery suggests that theatre
capacity is insufficient for the current demand. Data on theatre under-runs suggest that current capacity
may not be being fully utilised. Reviewers were told that staff were sometimes called at short notice and
reviewers were concerned that the high workload could result in staff becoming over-tired – with
associated potential for errors. The response to shortages of theatre staff included cancelling and
amalgamating theatres lists. This may result in unacceptably long delays for emergency and elective surgery
with adverse implications for patients’ outcomes. Based on Association for Perioperative Practice (AfPP)
guidance, running a theatre for 10 sessions per week (Monday to Friday) requires seven wte staff.
3 The skill mix appeared ‘top heavy’ and the unit did not have any Band 5 staff.
Return to Index
WMQRS Iom ED TA CC Report V2.1 20140408 8
CRITICAL CARE
General Comments and Achievements
Critical care services were provided by keen and committed staff with very good nursing leadership. Equipment
was of a high standard. Contingency planning was good, including planning for transfer to England. Some nursing
audits had been undertaken. The service was working with the Cheshire and Mersey Critical Care Network who
had also undertaken a review of the care provided. Progress was being made in addressing the issues identified by
that review. Several improvements were due to start on 1st December 2013 including an outreach service and
Intensive Care National Audit and Research Centre (ICNARC) data collection. Additional consultant posts were
being advertised. Staff were keen to continue to improve the service offered. A good organ donation policy was in
place, staff had been trained on its use and implementation had been audited. The patient and carer survey which
had been undertaken showed that most patients were very satisfied with the service they received. Some
feedback from patients and relatives highlighted exemplary communication, compassion and nursing skills.
Reviewers noted that a WMQRS review took place soon after, and substantially duplicated, a peer review of
critical care services by the Cheshire and Mersey Network. Reviewers saw two versions of the Cheshire and
Mersey visit report and noted that the earlier version was very similar to this report.
Good Practice
1 Infection control was good with a history of no hospital-acquired infections within the critical care unit.
Immediate Risks
1 Medical staffing
The critical care service had no medical lead. A consultant with critical care competences was not available
24/7. There was no evidence that consultant anaesthetists covering the unit had undertaken continuing
professional development of relevance to their work in critical care. Consultants did not have dedicated
time for their work on the critical care unit and a doctor was not always immediately available as they may
be in theatre. Continuity of care was poor, with the responsible consultant changing each day, although
there were plans to move to continuity of care over five days when new appointments were in place.
Patients were not all reviewed by a critical care consultant within 12 hours of admission.3
Concerns
1 See also Systemic Issues section of this report (all sections)
2 Handover / Transfer Documentation
Handover / transfer when patients left the unit was not formally documented.
3Actions Noble’s Hospital committed to take in response to the Immediate Risk (9.12.13):
Advertise for three consultant anaesthetists, one of which is a lead for critical care, with interviews planned in January 2014.
Submit a business case for further consultant anaesthetist posts.
Review the competences and training of consultant staff using the Faculty of Intensive Care Medicine guidance.
Review of relevant Continuing Professional Development of all current medical staff within the next four weeks.
Ensure staff are trained in critical care management.
Develop a training plan as necessary. WMQRS Response: These actions have the potential to ensure the Immediate Risk is addressed.
WMQRS Iom ED TA CC Report V2.1 20140408 9
3 Maintaining Competence
Activity levels were not clearly defined but the reported level of ventilated patients per year (92 in 2012
and 121 in 2013) was too low for maintaining competence of staff in providing critical care. The number of
patients on renal replacement therapy was below the minimum number as defined by the Cheshire and
Mersey Critical Care Network.
Further Consideration
1 Decisions about admission to the unit did not always involve both the parent team and critical care
consultant. Reviewers were told of a number of disagreements about admissions which did not appear to
be being effectively resolved.
2 Reviewers were given several examples of ways in which critical care services were not linking effectively
with other departments. The hospital did not have a ‘critical care group’ or other mechanism for driving
joint work with other hospital services.
3 Reviewers were impressed by the willingness of staff to provide care for people with a wide range of
conditions and, when necessary, undertake transfers. There was no formal on call rota for transfers,
however, and arrangements appeared to rely on “good will”. This could lead to delays in transfers with the
potential for the patient’s condition to deteriorate. This issue should be considered in future planning for
the critical care service.
4 Additional consultant anaesthetists were being recruited but there did not appear to be an agreed plan for
the unit’s development. Reviewers considered there were several options for addressing the issues
identified in this report which are not mutually exclusive:
a. Extending the roles of nursing staff, for example into prescribing and intubation, could partially
address the lack of an immediately available doctor.
b. Increasing further the number of consultants and / or reducing workload by the use of advanced
practitioners or physicians assistants in critical care and anaesthetics.
c. Establishing a formal arrangement with a hospital in England whereby medical and nursing staff
could regularly spend some time in a busy unit in order to ensure competences are maintained.
A formal link could also be useful for reducing the work needed on guideline production and
have other benefits in relation to training and audit.
d. Changing the nature of the service provided on the Isle of Man so that patients needing level 3
care are stabilised and transferred. This arrangement could function either at all times or,
alternatively, outside of race weeks with staff with appropriate competences being brought in
during race weeks.
Return to Index
SYSTEMIC ISSUES
This section of the report summarises the views of the visiting team at the end of the first visit. Later reviews may
change these findings and further detail will be added on governance issues when this area is reviewed.
Staff at Noble’s Hospital face a difficult challenge of providing comprehensive acute health care to a small, island
population of fewer than 90,000. Reviewers were impressed by the commitment of staff in the face of this
challenge and by the quality of some of the care provided. Staff throughout the hospital were clearly dedicated
and most of the patient feedback was very positive about the care they had received.
WMQRS Iom ED TA CC Report V2.1 20140408 10
Some issues, however, emerged as strong common themes from the three services reviewed. The combination of
these inter-related issues left reviewers with significant concerns both about the quality and safety of services at
Noble’s Hospital and about the Island’s ability to improve the situation without external support.
1 Culture
Reviewers considered that the systemic issues described in this section of this report may have
compromised the ability of politicians, managers, clinical staff and the public to work together to improve
the quality of care for patients. The culture which came through to the visiting team was of committed and
caring staff but also:
a. Blame - with managers, politicians and clinical staff blaming each other and clinical staff blaming
other clinical staff. The prevalence of blame was undermining morale of staff and confidence of
patients.
b. A lack of trust, a perceived lack of openness and staff frustration. Reviewers saw some evidence
to support these perceptions and allegations.
c. A culture and governance of the services reviewed which had drifted away from what is
considered good practice in England, including a loss of insight into what constitutes a good
healthcare system and good clinical practice. There will always be the potential for clinical staff
on the Isle of Man to become isolated from developments in clinical practice and reviewers saw
some evidence of this happening.
2 Adherence to ‘due process’
Reviewers saw, and were told about, many examples of ‘due process’ not being followed. Politicians need
occasionally to bring individual cases to the attention of hospital managers. Very occasionally clinical staff
will, in accordance with ‘whistle-blowing’ policies, need to bring issues to the attention of senior managers,
politicians or the press. The evidence presented to reviewers, however, was that these routes had become
the accepted norm rather than the exception. Issues raised outside of ‘due process’ were being accepted
rather than being referred back to the appropriate managerial and governance process. This was, in turn,
undermining managerial and governance systems with time and energy being dominated by responding to
issues raised outside of ‘due process’.
Management’s influence over medical staff appeared very limited. There was an apparent acceptance
within the hospital that collaborative working between operational management and clinical staff in the
best interests of patients had been lost, partly due a lack of management influence on the behaviour,
conduct and clinical practice of some medical staff. (NB. This issue is closely linked with sections 3 and 6
below).
Reviewers met many staff who were frustrated that decision-making processes had become very slow.
Government headcount restrictions were frequently quoted as a reason for delays in decisions and some of
the measures being taken to circumvent the restrictions, for example by the use of bank and agency staff,
were sub-optimal from financial, human resources and quality perspectives.
Reviewers saw clearly the large amount of time and effort being taken up by people not adhering to due
process and were concerned about the demoralising effect of this on staff and the resulting anxiety for
patients. (An exception to this finding is the Minister for Health, about whom all reports were of
appropriate behaviour and appropriate adherence to process.)
Reviewers were told by several clinical staff about why they no longer had respect for due process. They
reported having tried hard over several years to get issues addressed and services improved through
appropriate routes. The response they perceived was of their concerns and suggestions being ignored, with
little or no communication back to them, and no action taken as a result. General Medical Council (2012)
guidance ‘Raising and Acting on Concerns about Patient Safety’ includes a responsibility on doctors to
contact the General Medical Council or another appropriate regulatory body:
WMQRS Iom ED TA CC Report V2.1 20140408 11
If you cannot raise the issue with the responsible person or body locally because you believe them
to be part of the problem, or
If you have raised your concern through local channels but are not satisfied that the responsible
person or body has taken appropriate action.
Clinical staff on the Isle of Man do not have another appropriate regulatory body to contact in these
situations. The absence of a mechanism for clinical staff to raise concerns about patient safety in these
circumstances is likely to have contributed to an ongoing lack of adherence to due process.
3 Clinical staff responsibility for improving quality and for working collaboratively with colleagues
Clinical staff who met the visiting team were open and honest about the problems facing services at
Noble’s Hospital. All registered healthcare professionals have responsibilities for quality and safety
improvement but several of those who met the visiting team appeared to have either given up on these
responsibilities or had them taken away from them. Active involvement in quality and safety improvement,
including data collection, by healthcare professionals outside of management roles did not appear to be
routine or routinely expected. Reviewers commented that, for medical staff, this may lead to difficulties in
revalidation. In addition, some medical staff may not be undertaking sufficient activity in some areas to
maintain their competence.
The duties of a doctor include a duty of ‘Communication, Partnership and Teamwork’ (General Medical
Council ‘Good Medical Practice’, 2013). Nurses and other healthcare professionals have similar
responsibilities. Reviewers saw significant scope for improvement in the extent to which staff were carrying
out their duty to work collaboratively with colleagues to maintain and improve patient care. Particular
problems in relationships between some surgeons and some anaesthetists were evident.
4 Governance
Governance systems throughout the Isle of Man health services will be the topic for a future WMQRS
review. Incident reporting and complaints systems were in place but a culture of actively using these to
improve services was not evident. There was very little evidence of multi-disciplinary review and learning,
‘closing the loop’ from incidents, complaints and positive feedback by translating learning into improved
clinical practice.
The detailed report on compliance with Quality Standards shows several areas where expected guidelines
and protocols were not yet in place. Document control was not robust and several of the policies and
guidelines that were in place were out of date. Reviewers also commented on a selective approach to the
adoption of NICE guidance. The need for clinical practice to be based on published evidence of
effectiveness did not appear always to be understood and mechanisms for implementing and monitoring
implementation of evidence-based guidelines applicable to the Isle of Man were not evident. A Clinical
Recommendations Committee advised on prioritisation and encouraged the use of evidence-based
guidelines. The recommendations from this committee appeared to relate mainly to whether treatments
were made available by the Department of Health. Its influence over the implementation of evidence-
based guidelines was not apparent.
The lack of available data on activity and outcomes, and a resulting lack of comparative information, was of
significant concern to reviewers. The critical care unit and Emergency Department were, however, about to
start collecting ICNARC and Trauma Audit Research Network (TARN) data respectively.
5 ‘Commissioning’
In the services reviewed there did not appear to be a clear, documented understanding of the services that
the hospital was expected to provide and not provide. Reviewers were told that this was a more general
problem. The Strategic Plan seen by reviewers did not give detail of the services which should be provided
locally or which service developments would be supported on the Isle of Man or by arrangement with
another hospital.
WMQRS Iom ED TA CC Report V2.1 20140408 12
6 Leadership
Reviewers considered that the hospital management team will need considerable support if they are
successfully to address the issues identified in this report. Achieving a change in culture, driving adherence
to ‘due process’, ensuring all clinical staff fulfil their responsibilities for improving quality and for working
collaboratively with colleagues, and implementing robust governance systems will not be easy and the
hospital Medical Director and Director of Nursing may need particular support.
7 Patient and Carer Involvement
Reviewers did not see evidence of a systematic and effective approach to involving service users, carers and
the public in the monitoring and development of services. A plethora of individual surveys and initiatives
was evident but it was not clear how the results would be used or whether action had been taken as a
result of the issues raised.
8 Mandatory Training
Only 50% of nursing staff in the Emergency Department had completed mandatory training and
information was not available for other staff. Information on mandatory training for theatres and
anaesthetic staff was not available4. Reviewers concluded that hospital-wide systems for monitoring
completion of mandatory training may not be sufficiently robust.
Further Consideration
1 The visiting team recommended that the following actions should be given urgent consideration:
a. A published protocol for politicians and senior managers with the aim of ensuring issues raised
by individual patients and staff are, wherever possible, dealt with through appropriate
governance and managerial processes.
b. A mechanism for clinical staff to raise concerns about patient safety when a) they cannot raise
the issue with the responsible person locally because they believe they are part of the problem
or b) have done so and adequate action has not been taken.
c. Implementing service-level multi-disciplinary review and learning in all hospital services,
ensuring learning from incidents, complaints and positive feedback is translated into improved
clinical practice. Ongoing feedback from patients and carers may be a useful ‘feed’ into the
multi-disciplinary review and learning in each service.
d. Reminding all staff of their responsibilities under their contract of employment and, where
applicable, as registered healthcare professionals in particular in relation to:
i. Working with colleagues in ways that best serve patients’ interests
ii. Procedures for raising issues of concern
iii. Contacting the press or placing information in other publicly available media
iv. Whistle-blowing
Staff who do not comply with these responsibilities should be disciplined and, where applicable,
reported to their regulatory body.
e. Providing additional support or mentoring from outside the Isle of Man for the hospital
management team (individually and as a group) as they work to change culture, drive adherence
to ‘due process’, ensure all clinical staff fulfil their responsibilities for improving quality and for
working collaboratively with colleagues, and implement robust governance arrangements.
Tackling these issues imposes obligations on the management team as much as on clinical staff.
4 Critical care services were reviewed using the Cheshire and Mersey Critical Care Network Standards which are not specific about mandatory training.

WMQRS Iom ED TA CC Report V2.1 20140408 13
2 Other issues which the visiting team recommend should be given further consideration include:
a. A review of the systems by which the limit on the headcount of government employees is
achieved, with particular emphasis on achieving speedy decision-making at an appropriate level,
an appropriate number and skill mix of healthcare staff, and the impact of bank and agency staff
and other mechanisms for circumventing the headcount limit.5
b. An information strategy with clear plans for achieving appropriate data collection on hospital
services.
c. Introducing systems for ensuring and monitoring implementation of NICE and other published
evidence of effectiveness or for formally agreeing if guidance is not applicable to the Isle of Man.
If this is within the remit of the Clinical Recommendations Committee then this should be made
explicit and the Committee should actively take on this role.
d. Clarifying what services Noble’s Hospital is expected to provide and for what services patients
should be referred elsewhere. As part of this work, the tension between providing services
locally and meeting expected standards for the quality of services will need to be openly debated
and discussed.
e. Arrangements for funding off-Island referrals and treatment, in particular, to make sure that
these arrangements ensure appropriate robust, timely pathways of care.
Return to Index
5 “Since 2002 the number of professionally qualified clinical staff within the NHS [in England] has risen by 20.14 per cent. This
rise includes an increase in doctors of 40 per cent; a rise in the number of nurses of 10 per cent; and 19 per cent more qualified ambulance staff.” http://www.nhsconfed.org/priorities/political-engagement/Pages/NHS-statistics.aspx#staff (accessed 27.11.13)
WMQRS Iom ED TA CC Report V2.1 20140408 14
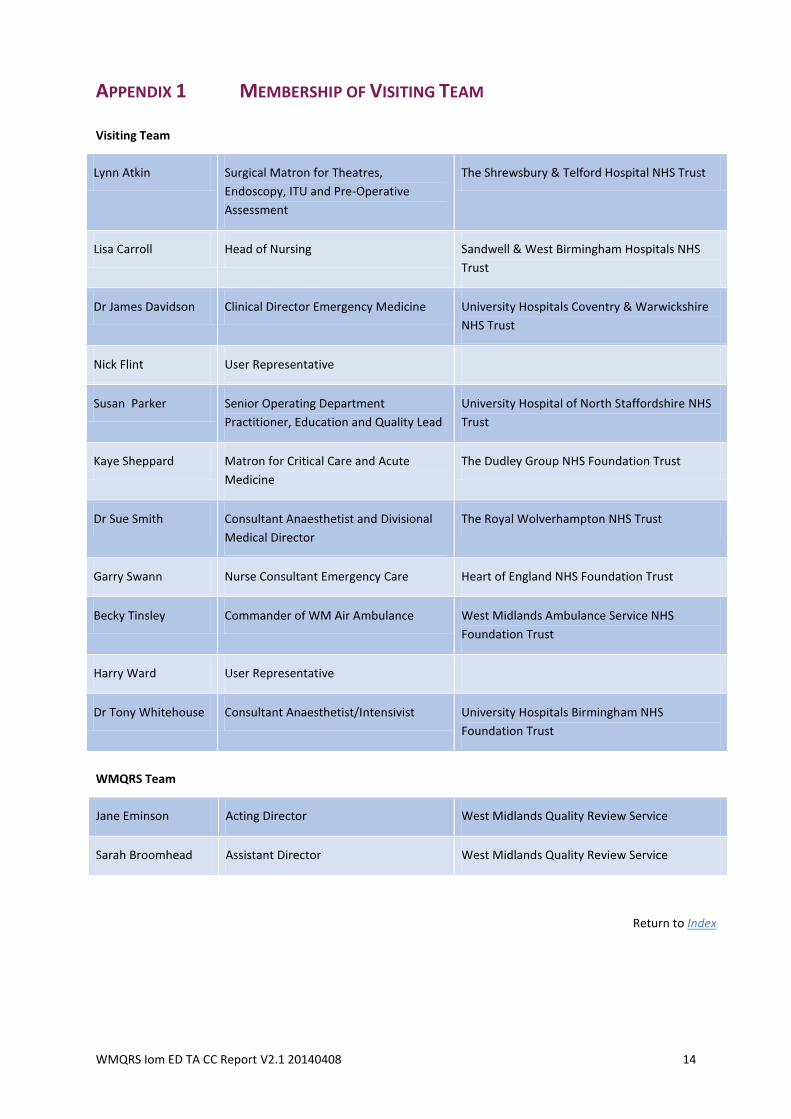
APPENDIX 1 MEMBERSHIP OF VISITING TEAM
Visiting Team
Lynn Atkin Surgical Matron for Theatres,
Endoscopy, ITU and Pre-Operative
Assessment
The Shrewsbury & Telford Hospital NHS Trust
Lisa Carroll Head of Nursing Sandwell & West Birmingham Hospitals NHS
Trust
Dr James Davidson Clinical Director Emergency Medicine University Hospitals Coventry & Warwickshire
NHS Trust
Nick Flint User Representative
Susan Parker Senior Operating Department
Practitioner, Education and Quality Lead
University Hospital of North Staffordshire NHS
Trust
Kaye Sheppard Matron for Critical Care and Acute
Medicine
The Dudley Group NHS Foundation Trust
Dr Sue Smith Consultant Anaesthetist and Divisional
Medical Director
The Royal Wolverhampton NHS Trust
Garry Swann Nurse Consultant Emergency Care Heart of England NHS Foundation Trust
Becky Tinsley Commander of WM Air Ambulance West Midlands Ambulance Service NHS
Foundation Trust
Harry Ward User Representative
Dr Tony Whitehouse Consultant Anaesthetist/Intensivist University Hospitals Birmingham NHS
Foundation Trust
WMQRS Team
Jane Eminson Acting Director West Midlands Quality Review Service
Sarah Broomhead Assistant Director West Midlands Quality Review Service
Return to Index
WMQRS Iom ED TA CC Report V2.1 20140408 15
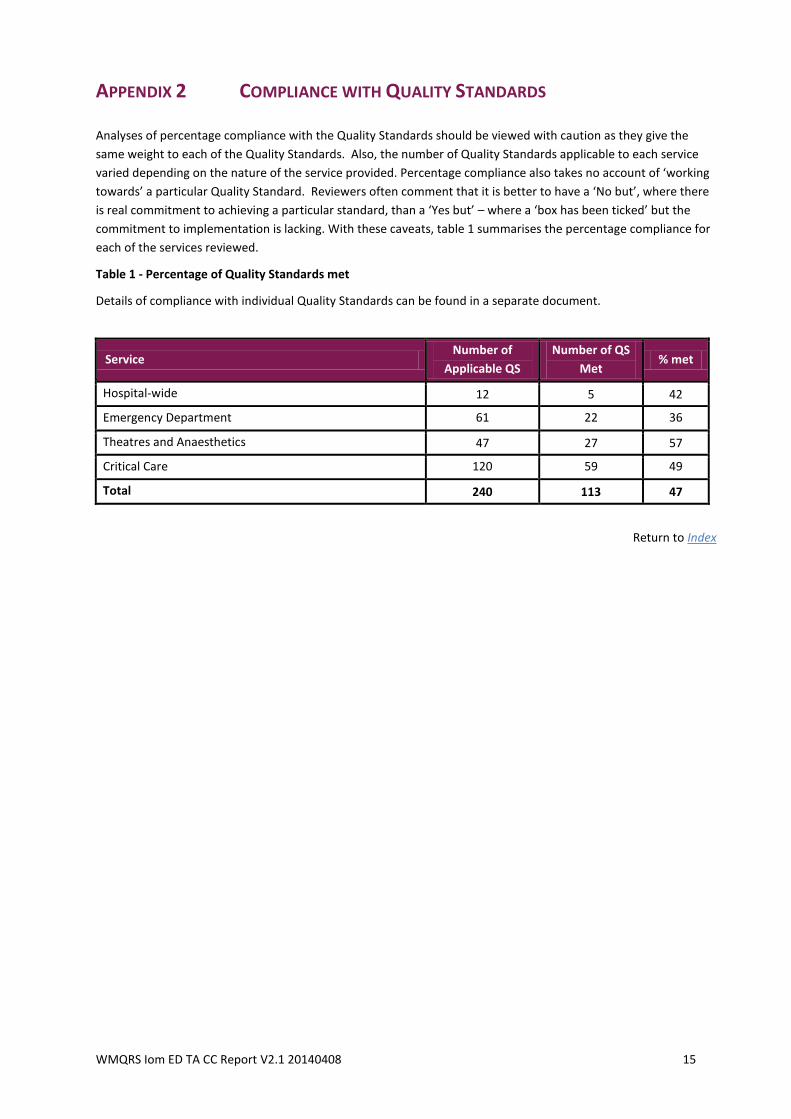
APPENDIX 2 COMPLIANCE WITH QUALITY STANDARDS
Analyses of percentage compliance with the Quality Standards should be viewed with caution as they give the
same weight to each of the Quality Standards. Also, the number of Quality Standards applicable to each service
varied depending on the nature of the service provided. Percentage compliance also takes no account of ‘working
towards’ a particular Quality Standard. Reviewers often comment that it is better to have a ‘No but’, where there
is real commitment to achieving a particular standard, than a ‘Yes but’ – where a ‘box has been ticked’ but the
commitment to implementation is lacking. With these caveats, table 1 summarises the percentage compliance for
each of the services reviewed.
Table 1 - Percentage of Quality Standards met
Details of compliance with individual Quality Standards can be found in a separate document.
Service Number of
Applicable QS
Number of QS
Met % met
Hospital-wide 12 5 42
Emergency Department 61 22 36
Theatres and Anaesthetics 47 27 57
Critical Care 120 59 49
Total 240 113 47
Return to Index
WMQRS Iom ED TA CC Report V2.1 20140408 16
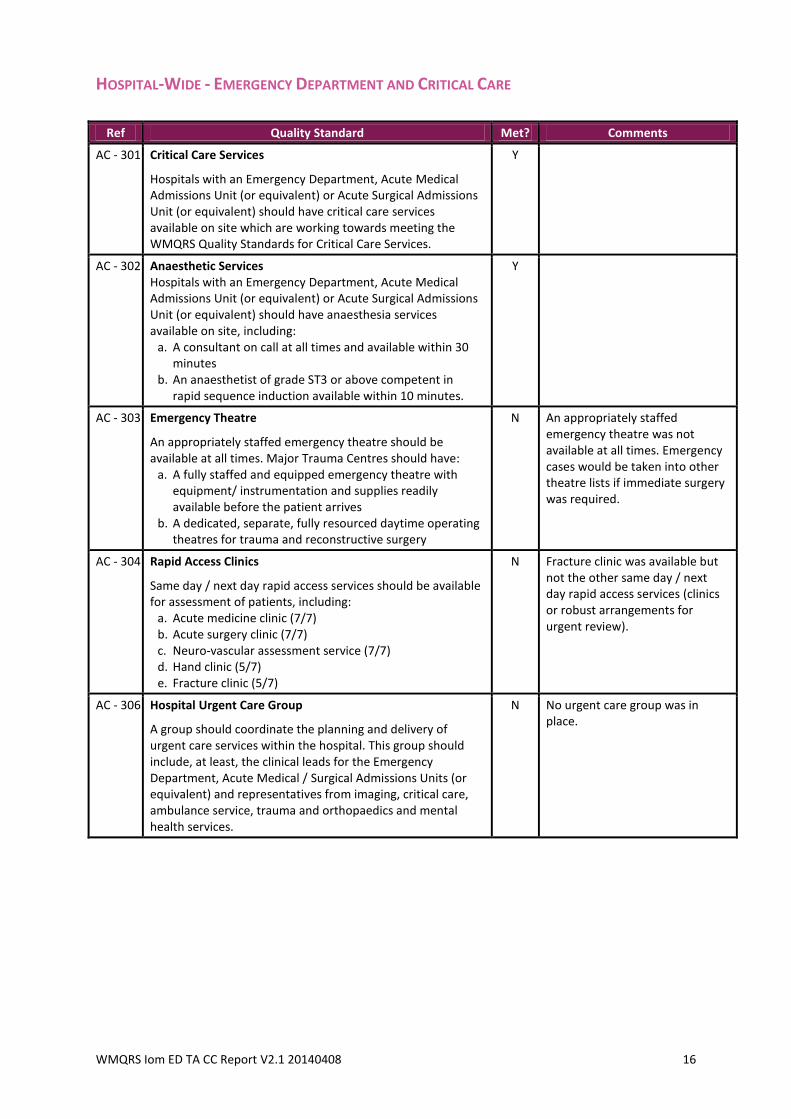
HOSPITAL-WIDE - EMERGENCY DEPARTMENT AND CRITICAL CARE
Ref Quality Standard Met? Comments
AC - 301 Critical Care Services
Hospitals with an Emergency Department, Acute Medical Admissions Unit (or equivalent) or Acute Surgical Admissions Unit (or equivalent) should have critical care services available on site which are working towards meeting the WMQRS Quality Standards for Critical Care Services.
Y
AC - 302 Anaesthetic Services Hospitals with an Emergency Department, Acute Medical Admissions Unit (or equivalent) or Acute Surgical Admissions Unit (or equivalent) should have anaesthesia services available on site, including:
a. A consultant on call at all times and available within 30 minutes
b. An anaesthetist of grade ST3 or above competent in rapid sequence induction available within 10 minutes.
Y
AC - 303 Emergency Theatre
An appropriately staffed emergency theatre should be available at all times. Major Trauma Centres should have:
a. A fully staffed and equipped emergency theatre with equipment/ instrumentation and supplies readily available before the patient arrives
b. A dedicated, separate, fully resourced daytime operating theatres for trauma and reconstructive surgery
N An appropriately staffed emergency theatre was not available at all times. Emergency cases would be taken into other theatre lists if immediate surgery was required.
AC - 304 Rapid Access Clinics
Same day / next day rapid access services should be available for assessment of patients, including:
a. Acute medicine clinic (7/7) b. Acute surgery clinic (7/7) c. Neuro-vascular assessment service (7/7) d. Hand clinic (5/7) e. Fracture clinic (5/7)
N Fracture clinic was available but not the other same day / next day rapid access services (clinics or robust arrangements for urgent review).
AC - 306 Hospital Urgent Care Group
A group should coordinate the planning and delivery of urgent care services within the hospital. This group should include, at least, the clinical leads for the Emergency Department, Acute Medical / Surgical Admissions Units (or equivalent) and representatives from imaging, critical care, ambulance service, trauma and orthopaedics and mental health services.
N No urgent care group was in place.
WMQRS Iom ED TA CC Report V2.1 20140408 17
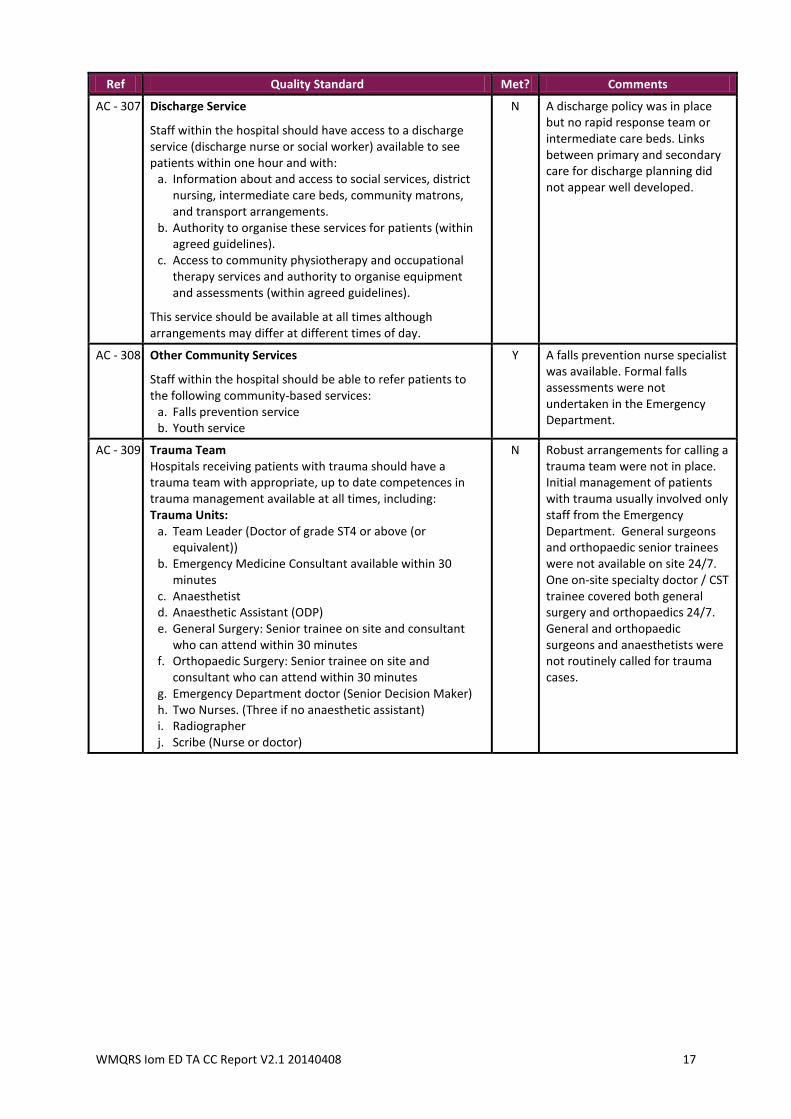
Ref Quality Standard Met? Comments
AC - 307 Discharge Service
Staff within the hospital should have access to a discharge service (discharge nurse or social worker) available to see patients within one hour and with:
a. Information about and access to social services, district nursing, intermediate care beds, community matrons, and transport arrangements.
b. Authority to organise these services for patients (within agreed guidelines).
c. Access to community physiotherapy and occupational therapy services and authority to organise equipment and assessments (within agreed guidelines).
This service should be available at all times although arrangements may differ at different times of day.
N A discharge policy was in place but no rapid response team or intermediate care beds. Links between primary and secondary care for discharge planning did not appear well developed.
AC - 308 Other Community Services
Staff within the hospital should be able to refer patients to the following community-based services:
a. Falls prevention service b. Youth service
Y A falls prevention nurse specialist was available. Formal falls assessments were not undertaken in the Emergency Department.
AC - 309 Trauma Team Hospitals receiving patients with trauma should have a trauma team with appropriate, up to date competences in trauma management available at all times, including: Trauma Units:
a. Team Leader (Doctor of grade ST4 or above (or equivalent))
b. Emergency Medicine Consultant available within 30 minutes
c. Anaesthetist d. Anaesthetic Assistant (ODP) e. General Surgery: Senior trainee on site and consultant
who can attend within 30 minutes f. Orthopaedic Surgery: Senior trainee on site and
consultant who can attend within 30 minutes g. Emergency Department doctor (Senior Decision Maker) h. Two Nurses. (Three if no anaesthetic assistant) i. Radiographer j. Scribe (Nurse or doctor)
N Robust arrangements for calling a trauma team were not in place. Initial management of patients with trauma usually involved only staff from the Emergency Department. General surgeons and orthopaedic senior trainees were not available on site 24/7. One on-site specialty doctor / CST trainee covered both general surgery and orthopaedics 24/7. General and orthopaedic surgeons and anaesthetists were not routinely called for trauma cases.
WMQRS Iom ED TA CC Report V2.1 20140408 18
Ref Quality Standard Met? Comments
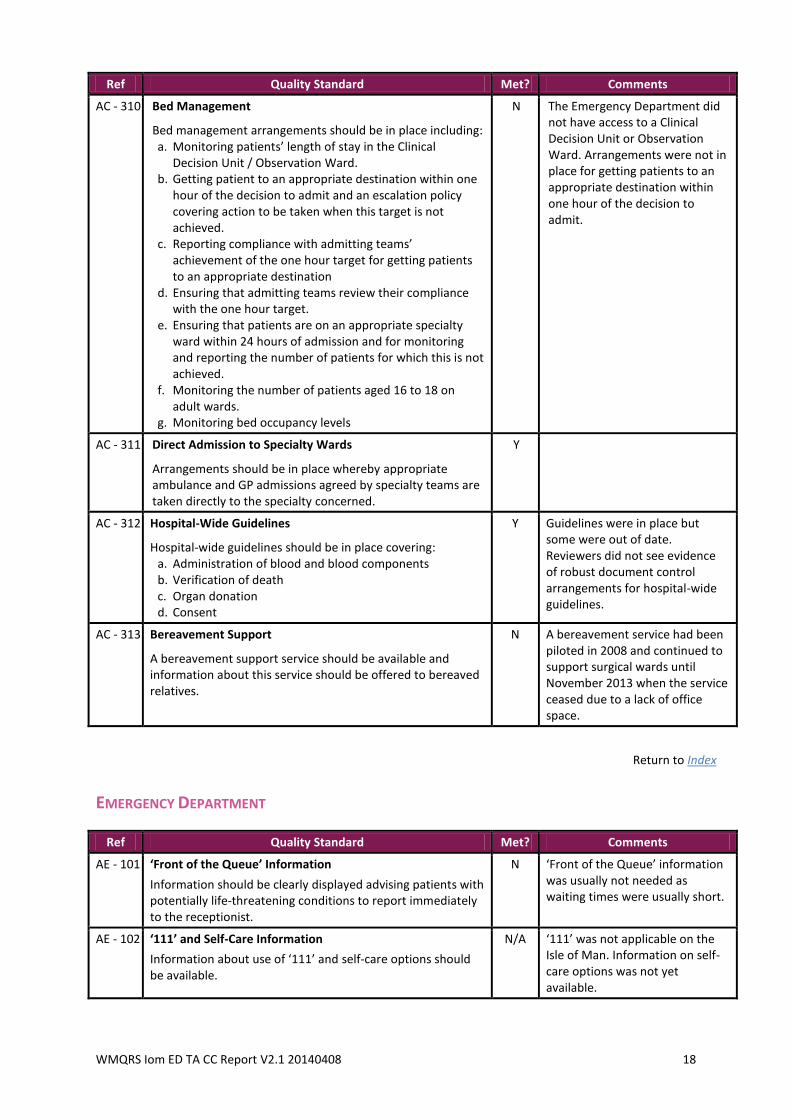
AC - 310 Bed Management
Bed management arrangements should be in place including: a. Monitoring patients’ length of stay in the Clinical
Decision Unit / Observation Ward. b. Getting patient to an appropriate destination within one
hour of the decision to admit and an escalation policy covering action to be taken when this target is not achieved.
c. Reporting compliance with admitting teams’ achievement of the one hour target for getting patients to an appropriate destination
d. Ensuring that admitting teams review their compliance with the one hour target.
e. Ensuring that patients are on an appropriate specialty ward within 24 hours of admission and for monitoring and reporting the number of patients for which this is not achieved.
f. Monitoring the number of patients aged 16 to 18 on adult wards.
g. Monitoring bed occupancy levels
N The Emergency Department did not have access to a Clinical Decision Unit or Observation Ward. Arrangements were not in place for getting patients to an appropriate destination within one hour of the decision to admit.
AC - 311 Direct Admission to Specialty Wards
Arrangements should be in place whereby appropriate ambulance and GP admissions agreed by specialty teams are taken directly to the specialty concerned.
Y
AC - 312 Hospital-Wide Guidelines
Hospital-wide guidelines should be in place covering: a. Administration of blood and blood components b. Verification of death c. Organ donation d. Consent
Y Guidelines were in place but some were out of date. Reviewers did not see evidence of robust document control arrangements for hospital-wide guidelines.
AC - 313 Bereavement Support
A bereavement support service should be available and information about this service should be offered to bereaved relatives.
N A bereavement service had been piloted in 2008 and continued to support surgical wards until November 2013 when the service ceased due to a lack of office space.
Return to Index
EMERGENCY DEPARTMENT
Ref Quality Standard Met? Comments
AE - 101 ‘Front of the Queue’ Information
Information should be clearly displayed advising patients with potentially life-threatening conditions to report immediately to the receptionist.
N ‘Front of the Queue’ information was usually not needed as waiting times were usually short.
AE - 102 ‘111’ and Self-Care Information
Information about use of ‘111’ and self-care options should be available.
N/A ‘111’ was not applicable on the Isle of Man. Information on self-care options was not yet available.
WMQRS Iom ED TA CC Report V2.1 20140408 19
Ref Quality Standard Met? Comments
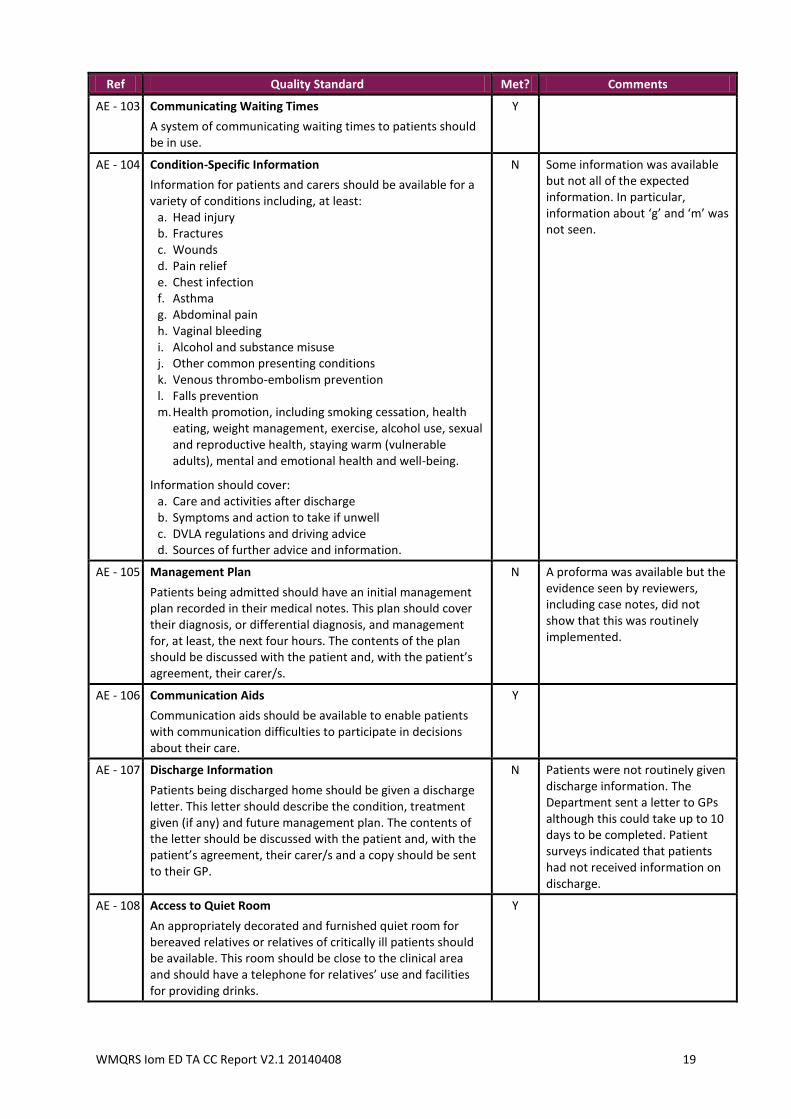
AE - 103 Communicating Waiting Times
A system of communicating waiting times to patients should be in use.
Y
AE - 104 Condition-Specific Information
Information for patients and carers should be available for a variety of conditions including, at least:
a. Head injury b. Fractures c. Wounds d. Pain relief e. Chest infection f. Asthma g. Abdominal pain h. Vaginal bleeding i. Alcohol and substance misuse j. Other common presenting conditions k. Venous thrombo-embolism prevention l. Falls prevention m. Health promotion, including smoking cessation, health
eating, weight management, exercise, alcohol use, sexual and reproductive health, staying warm (vulnerable adults), mental and emotional health and well-being.
Information should cover: a. Care and activities after discharge b. Symptoms and action to take if unwell c. DVLA regulations and driving advice d. Sources of further advice and information.
N Some information was available but not all of the expected information. In particular, information about ‘g’ and ‘m’ was not seen.
AE - 105 Management Plan
Patients being admitted should have an initial management plan recorded in their medical notes. This plan should cover their diagnosis, or differential diagnosis, and management for, at least, the next four hours. The contents of the plan should be discussed with the patient and, with the patient’s agreement, their carer/s.
N A proforma was available but the evidence seen by reviewers, including case notes, did not show that this was routinely implemented.
AE - 106 Communication Aids
Communication aids should be available to enable patients with communication difficulties to participate in decisions about their care.
Y
AE - 107 Discharge Information
Patients being discharged home should be given a discharge letter. This letter should describe the condition, treatment given (if any) and future management plan. The contents of the letter should be discussed with the patient and, with the patient’s agreement, their carer/s and a copy should be sent to their GP.
N Patients were not routinely given discharge information. The Department sent a letter to GPs although this could take up to 10 days to be completed. Patient surveys indicated that patients had not received information on discharge.
AE - 108 Access to Quiet Room
An appropriately decorated and furnished quiet room for bereaved relatives or relatives of critically ill patients should be available. This room should be close to the clinical area and should have a telephone for relatives’ use and facilities for providing drinks.
Y
WMQRS Iom ED TA CC Report V2.1 20140408 20
Ref Quality Standard Met? Comments
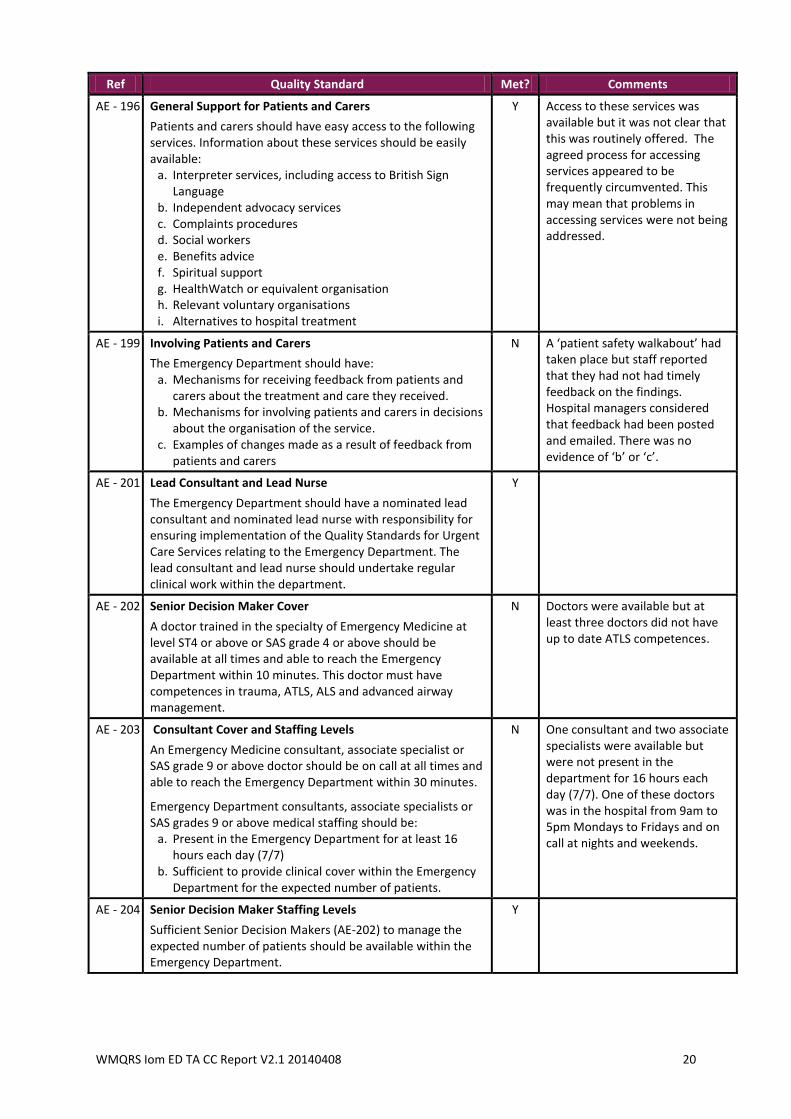
AE - 196 General Support for Patients and Carers
Patients and carers should have easy access to the following services. Information about these services should be easily available:
a. Interpreter services, including access to British Sign Language
b. Independent advocacy services c. Complaints procedures d. Social workers e. Benefits advice f. Spiritual support g. HealthWatch or equivalent organisation h. Relevant voluntary organisations i. Alternatives to hospital treatment
Y Access to these services was available but it was not clear that this was routinely offered. The agreed process for accessing services appeared to be frequently circumvented. This may mean that problems in accessing services were not being addressed.
AE - 199 Involving Patients and Carers
The Emergency Department should have: a. Mechanisms for receiving feedback from patients and
carers about the treatment and care they received. b. Mechanisms for involving patients and carers in decisions
about the organisation of the service. c. Examples of changes made as a result of feedback from
patients and carers
N A ‘patient safety walkabout’ had taken place but staff reported that they had not had timely feedback on the findings. Hospital managers considered that feedback had been posted and emailed. There was no evidence of ‘b’ or ‘c’.
AE - 201 Lead Consultant and Lead Nurse
The Emergency Department should have a nominated lead consultant and nominated lead nurse with responsibility for ensuring implementation of the Quality Standards for Urgent Care Services relating to the Emergency Department. The lead consultant and lead nurse should undertake regular clinical work within the department.
Y
AE - 202 Senior Decision Maker Cover
A doctor trained in the specialty of Emergency Medicine at level ST4 or above or SAS grade 4 or above should be available at all times and able to reach the Emergency Department within 10 minutes. This doctor must have competences in trauma, ATLS, ALS and advanced airway management.
N Doctors were available but at least three doctors did not have up to date ATLS competences.
AE - 203 Consultant Cover and Staffing Levels
An Emergency Medicine consultant, associate specialist or SAS grade 9 or above doctor should be on call at all times and able to reach the Emergency Department within 30 minutes.
Emergency Department consultants, associate specialists or SAS grades 9 or above medical staffing should be:
a. Present in the Emergency Department for at least 16 hours each day (7/7)
b. Sufficient to provide clinical cover within the Emergency Department for the expected number of patients.
N One consultant and two associate specialists were available but were not present in the department for 16 hours each day (7/7). One of these doctors was in the hospital from 9am to 5pm Mondays to Fridays and on call at nights and weekends.
AE - 204 Senior Decision Maker Staffing Levels
Sufficient Senior Decision Makers (AE-202) to manage the expected number of patients should be available within the Emergency Department.
Y
WMQRS Iom ED TA CC Report V2.1 20140408 21
Ref Quality Standard Met? Comments
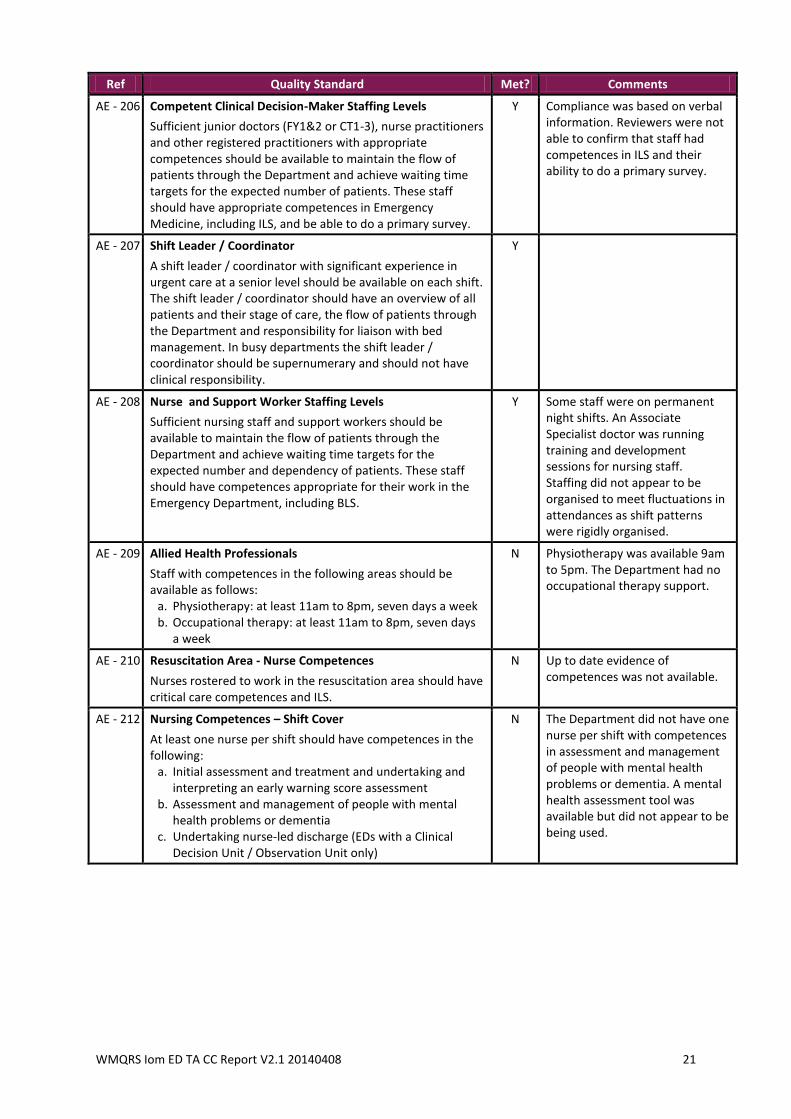
AE - 206 Competent Clinical Decision-Maker Staffing Levels
Sufficient junior doctors (FY1&2 or CT1-3), nurse practitioners and other registered practitioners with appropriate competences should be available to maintain the flow of patients through the Department and achieve waiting time targets for the expected number of patients. These staff should have appropriate competences in Emergency Medicine, including ILS, and be able to do a primary survey.
Y Compliance was based on verbal information. Reviewers were not able to confirm that staff had competences in ILS and their ability to do a primary survey.
AE - 207 Shift Leader / Coordinator
A shift leader / coordinator with significant experience in urgent care at a senior level should be available on each shift. The shift leader / coordinator should have an overview of all patients and their stage of care, the flow of patients through the Department and responsibility for liaison with bed management. In busy departments the shift leader / coordinator should be supernumerary and should not have clinical responsibility.
Y
AE - 208 Nurse and Support Worker Staffing Levels
Sufficient nursing staff and support workers should be available to maintain the flow of patients through the Department and achieve waiting time targets for the expected number and dependency of patients. These staff should have competences appropriate for their work in the Emergency Department, including BLS.
Y Some staff were on permanent night shifts. An Associate Specialist doctor was running training and development sessions for nursing staff. Staffing did not appear to be organised to meet fluctuations in attendances as shift patterns were rigidly organised.
AE - 209 Allied Health Professionals
Staff with competences in the following areas should be available as follows:
a. Physiotherapy: at least 11am to 8pm, seven days a week b. Occupational therapy: at least 11am to 8pm, seven days
a week
N Physiotherapy was available 9am to 5pm. The Department had no occupational therapy support.
AE - 210 Resuscitation Area - Nurse Competences
Nurses rostered to work in the resuscitation area should have critical care competences and ILS.
N Up to date evidence of competences was not available.
AE - 212 Nursing Competences – Shift Cover
At least one nurse per shift should have competences in the following:
a. Initial assessment and treatment and undertaking and interpreting an early warning score assessment
b. Assessment and management of people with mental health problems or dementia
c. Undertaking nurse-led discharge (EDs with a Clinical Decision Unit / Observation Unit only)
N The Department did not have one nurse per shift with competences in assessment and management of people with mental health problems or dementia. A mental health assessment tool was available but did not appear to be being used.
WMQRS Iom ED TA CC Report V2.1 20140408 22
Ref Quality Standard Met? Comments
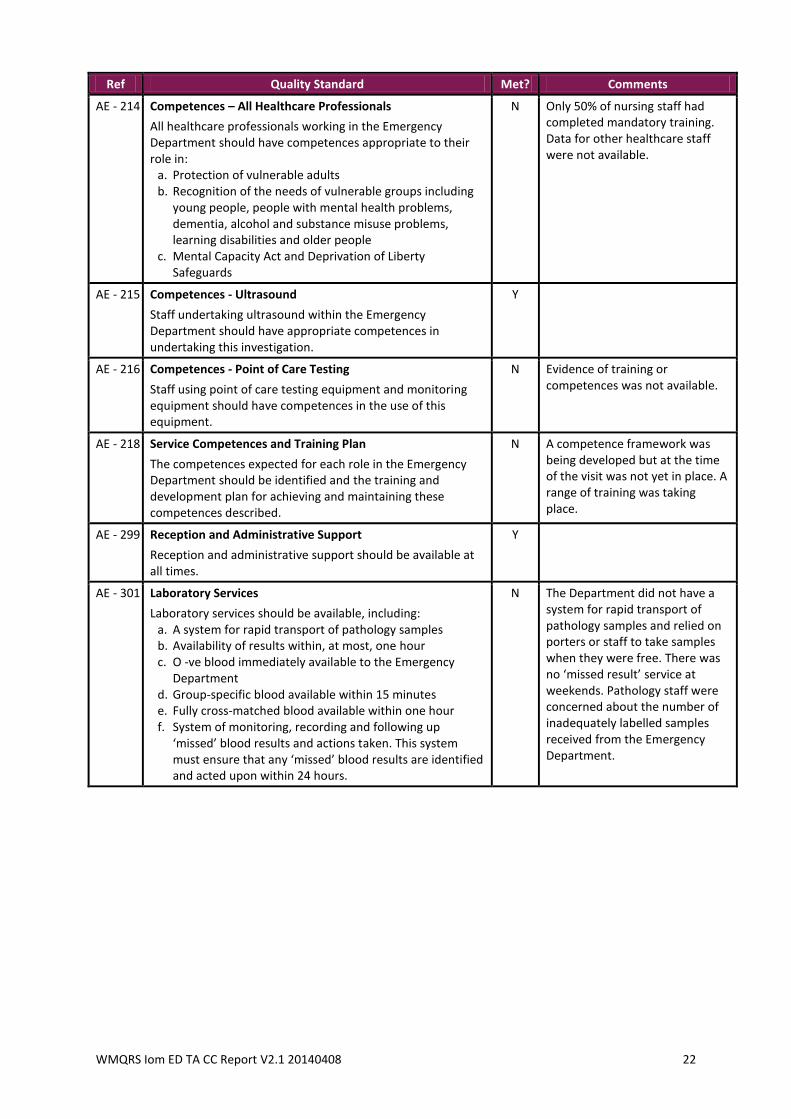
AE - 214 Competences – All Healthcare Professionals
All healthcare professionals working in the Emergency Department should have competences appropriate to their role in:
a. Protection of vulnerable adults b. Recognition of the needs of vulnerable groups including
young people, people with mental health problems, dementia, alcohol and substance misuse problems, learning disabilities and older people
c. Mental Capacity Act and Deprivation of Liberty Safeguards
N Only 50% of nursing staff had completed mandatory training. Data for other healthcare staff were not available.
AE - 215 Competences - Ultrasound
Staff undertaking ultrasound within the Emergency Department should have appropriate competences in undertaking this investigation.
Y
AE - 216 Competences - Point of Care Testing
Staff using point of care testing equipment and monitoring equipment should have competences in the use of this equipment.
N Evidence of training or competences was not available.
AE - 218 Service Competences and Training Plan
The competences expected for each role in the Emergency Department should be identified and the training and development plan for achieving and maintaining these competences described.
N A competence framework was being developed but at the time of the visit was not yet in place. A range of training was taking place.
AE - 299 Reception and Administrative Support
Reception and administrative support should be available at all times.
Y
AE - 301 Laboratory Services
Laboratory services should be available, including: a. A system for rapid transport of pathology samples b. Availability of results within, at most, one hour c. O -ve blood immediately available to the Emergency
Department d. Group-specific blood available within 15 minutes e. Fully cross-matched blood available within one hour f. System of monitoring, recording and following up
‘missed’ blood results and actions taken. This system must ensure that any ‘missed’ blood results are identified and acted upon within 24 hours.
N The Department did not have a system for rapid transport of pathology samples and relied on porters or staff to take samples when they were free. There was no ‘missed result’ service at weekends. Pathology staff were concerned about the number of inadequately labelled samples received from the Emergency Department.
WMQRS Iom ED TA CC Report V2.1 20140408 23
Ref Quality Standard Met? Comments
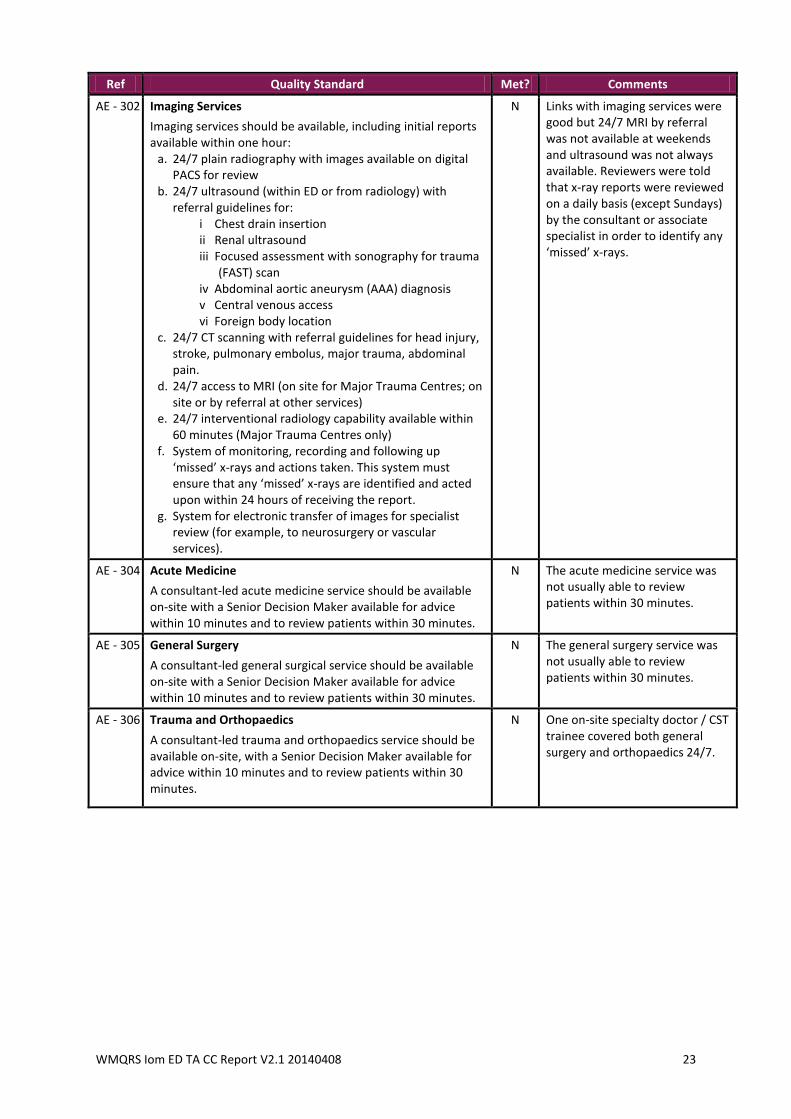
AE - 302 Imaging Services
Imaging services should be available, including initial reports available within one hour:
a. 24/7 plain radiography with images available on digital PACS for review
b. 24/7 ultrasound (within ED or from radiology) with referral guidelines for:
i Chest drain insertion ii Renal ultrasound iii Focused assessment with sonography for trauma
(FAST) scan iv Abdominal aortic aneurysm (AAA) diagnosis v Central venous access vi Foreign body location
c. 24/7 CT scanning with referral guidelines for head injury, stroke, pulmonary embolus, major trauma, abdominal pain.
d. 24/7 access to MRI (on site for Major Trauma Centres; on site or by referral at other services)
e. 24/7 interventional radiology capability available within 60 minutes (Major Trauma Centres only)
f. System of monitoring, recording and following up ‘missed’ x-rays and actions taken. This system must ensure that any ‘missed’ x-rays are identified and acted upon within 24 hours of receiving the report.
g. System for electronic transfer of images for specialist review (for example, to neurosurgery or vascular services).
N Links with imaging services were good but 24/7 MRI by referral was not available at weekends and ultrasound was not always available. Reviewers were told that x-ray reports were reviewed on a daily basis (except Sundays) by the consultant or associate specialist in order to identify any ‘missed’ x-rays.
AE - 304 Acute Medicine
A consultant-led acute medicine service should be available on-site with a Senior Decision Maker available for advice within 10 minutes and to review patients within 30 minutes.
N The acute medicine service was not usually able to review patients within 30 minutes.
AE - 305 General Surgery
A consultant-led general surgical service should be available on-site with a Senior Decision Maker available for advice within 10 minutes and to review patients within 30 minutes.
N The general surgery service was not usually able to review patients within 30 minutes.
AE - 306 Trauma and Orthopaedics
A consultant-led trauma and orthopaedics service should be available on-site, with a Senior Decision Maker available for advice within 10 minutes and to review patients within 30 minutes.
N One on-site specialty doctor / CST trainee covered both general surgery and orthopaedics 24/7.
WMQRS Iom ED TA CC Report V2.1 20140408 24
Ref Quality Standard Met? Comments
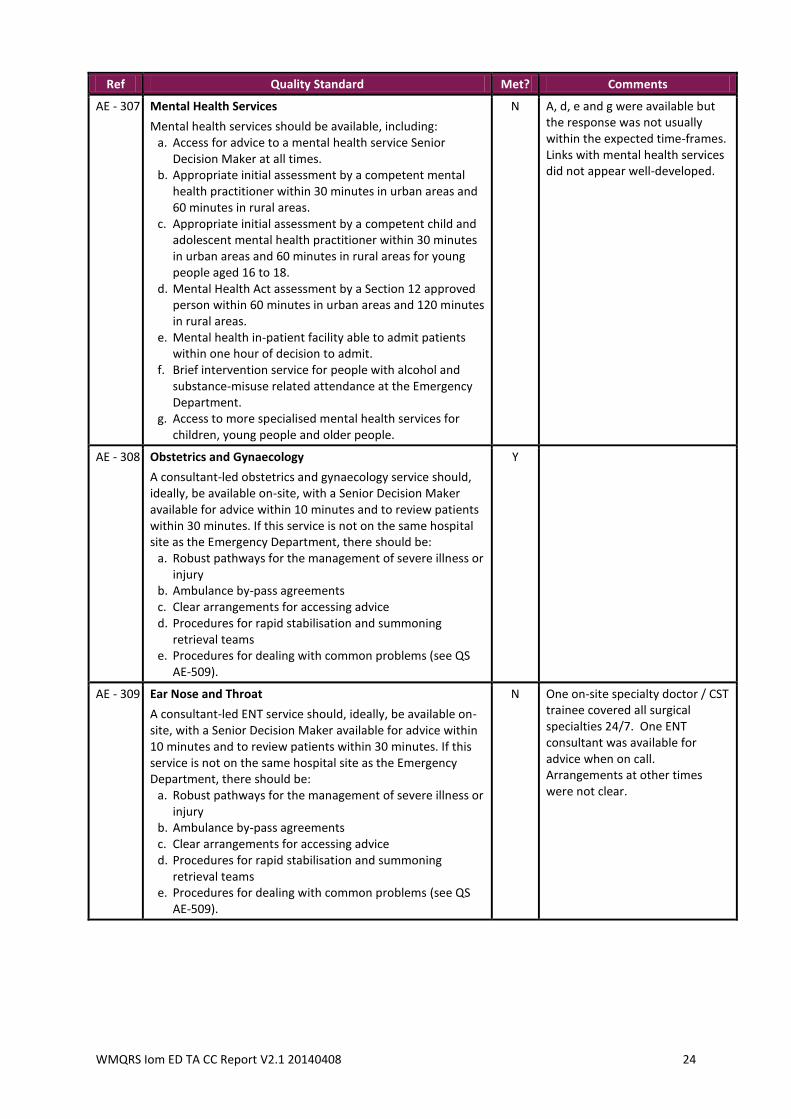
AE - 307 Mental Health Services
Mental health services should be available, including: a. Access for advice to a mental health service Senior
Decision Maker at all times. b. Appropriate initial assessment by a competent mental
health practitioner within 30 minutes in urban areas and 60 minutes in rural areas.
c. Appropriate initial assessment by a competent child and adolescent mental health practitioner within 30 minutes in urban areas and 60 minutes in rural areas for young people aged 16 to 18.
d. Mental Health Act assessment by a Section 12 approved person within 60 minutes in urban areas and 120 minutes in rural areas.
e. Mental health in-patient facility able to admit patients within one hour of decision to admit.
f. Brief intervention service for people with alcohol and substance-misuse related attendance at the Emergency Department.
g. Access to more specialised mental health services for children, young people and older people.
N A, d, e and g were available but the response was not usually within the expected time-frames. Links with mental health services did not appear well-developed.
AE - 308 Obstetrics and Gynaecology
A consultant-led obstetrics and gynaecology service should, ideally, be available on-site, with a Senior Decision Maker available for advice within 10 minutes and to review patients within 30 minutes. If this service is not on the same hospital site as the Emergency Department, there should be:
a. Robust pathways for the management of severe illness or injury
b. Ambulance by-pass agreements c. Clear arrangements for accessing advice d. Procedures for rapid stabilisation and summoning
retrieval teams e. Procedures for dealing with common problems (see QS
AE-509).
Y
AE - 309 Ear Nose and Throat
A consultant-led ENT service should, ideally, be available on-site, with a Senior Decision Maker available for advice within 10 minutes and to review patients within 30 minutes. If this service is not on the same hospital site as the Emergency Department, there should be:
a. Robust pathways for the management of severe illness or injury
b. Ambulance by-pass agreements c. Clear arrangements for accessing advice d. Procedures for rapid stabilisation and summoning
retrieval teams e. Procedures for dealing with common problems (see QS
AE-509).
N One on-site specialty doctor / CST trainee covered all surgical specialties 24/7. One ENT consultant was available for advice when on call. Arrangements at other times were not clear.
WMQRS Iom ED TA CC Report V2.1 20140408 25
Ref Quality Standard Met? Comments
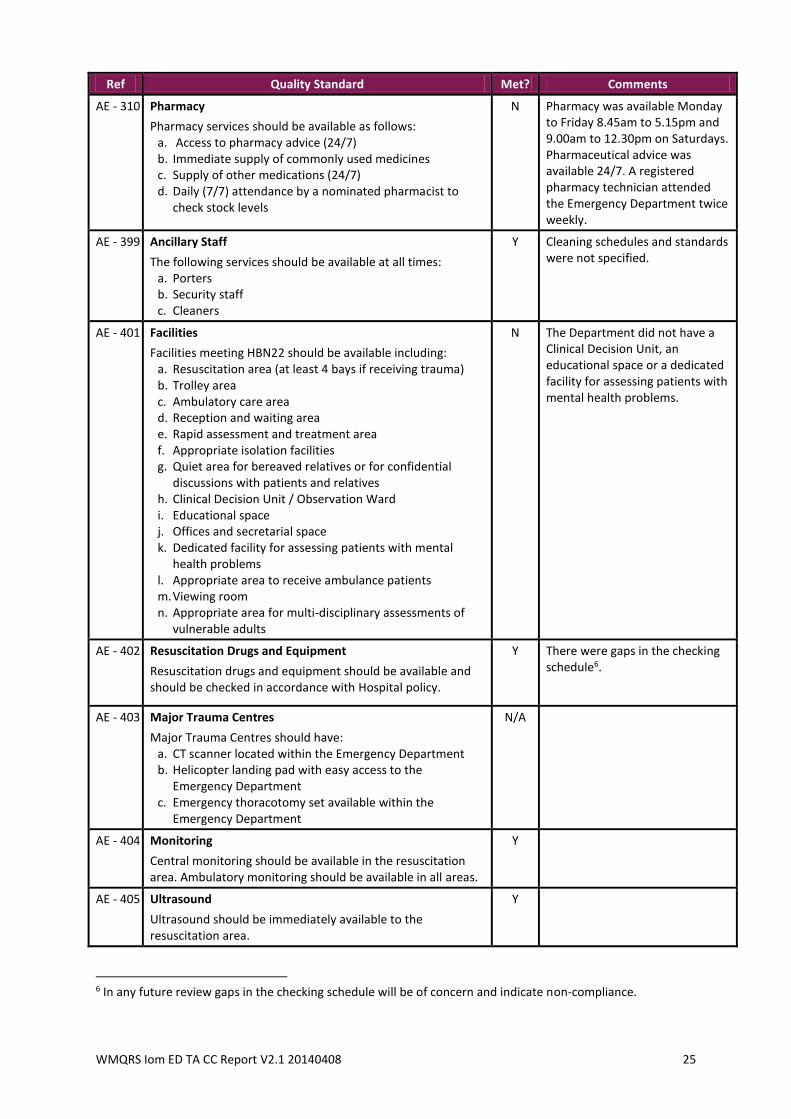
AE - 310 Pharmacy
Pharmacy services should be available as follows: a. Access to pharmacy advice (24/7) b. Immediate supply of commonly used medicines c. Supply of other medications (24/7) d. Daily (7/7) attendance by a nominated pharmacist to
check stock levels
N Pharmacy was available Monday to Friday 8.45am to 5.15pm and 9.00am to 12.30pm on Saturdays. Pharmaceutical advice was available 24/7. A registered pharmacy technician attended the Emergency Department twice weekly.
AE - 399 Ancillary Staff
The following services should be available at all times: a. Porters b. Security staff c. Cleaners
Y Cleaning schedules and standards were not specified.
AE - 401 Facilities
Facilities meeting HBN22 should be available including: a. Resuscitation area (at least 4 bays if receiving trauma) b. Trolley area c. Ambulatory care area d. Reception and waiting area e. Rapid assessment and treatment area f. Appropriate isolation facilities g. Quiet area for bereaved relatives or for confidential
discussions with patients and relatives h. Clinical Decision Unit / Observation Ward i. Educational space j. Offices and secretarial space k. Dedicated facility for assessing patients with mental
health problems l. Appropriate area to receive ambulance patients m. Viewing room n. Appropriate area for multi-disciplinary assessments of
vulnerable adults
N The Department did not have a Clinical Decision Unit, an educational space or a dedicated facility for assessing patients with mental health problems.
AE - 402 Resuscitation Drugs and Equipment
Resuscitation drugs and equipment should be available and should be checked in accordance with Hospital policy.
Y There were gaps in the checking schedule6.
AE - 403 Major Trauma Centres
Major Trauma Centres should have: a. CT scanner located within the Emergency Department b. Helicopter landing pad with easy access to the
Emergency Department c. Emergency thoracotomy set available within the
Emergency Department
N/A
AE - 404 Monitoring
Central monitoring should be available in the resuscitation area. Ambulatory monitoring should be available in all areas.
Y
AE - 405 Ultrasound
Ultrasound should be immediately available to the resuscitation area.
Y
6 In any future review gaps in the checking schedule will be of concern and indicate non-compliance.
WMQRS Iom ED TA CC Report V2.1 20140408 26
Ref Quality Standard Met? Comments
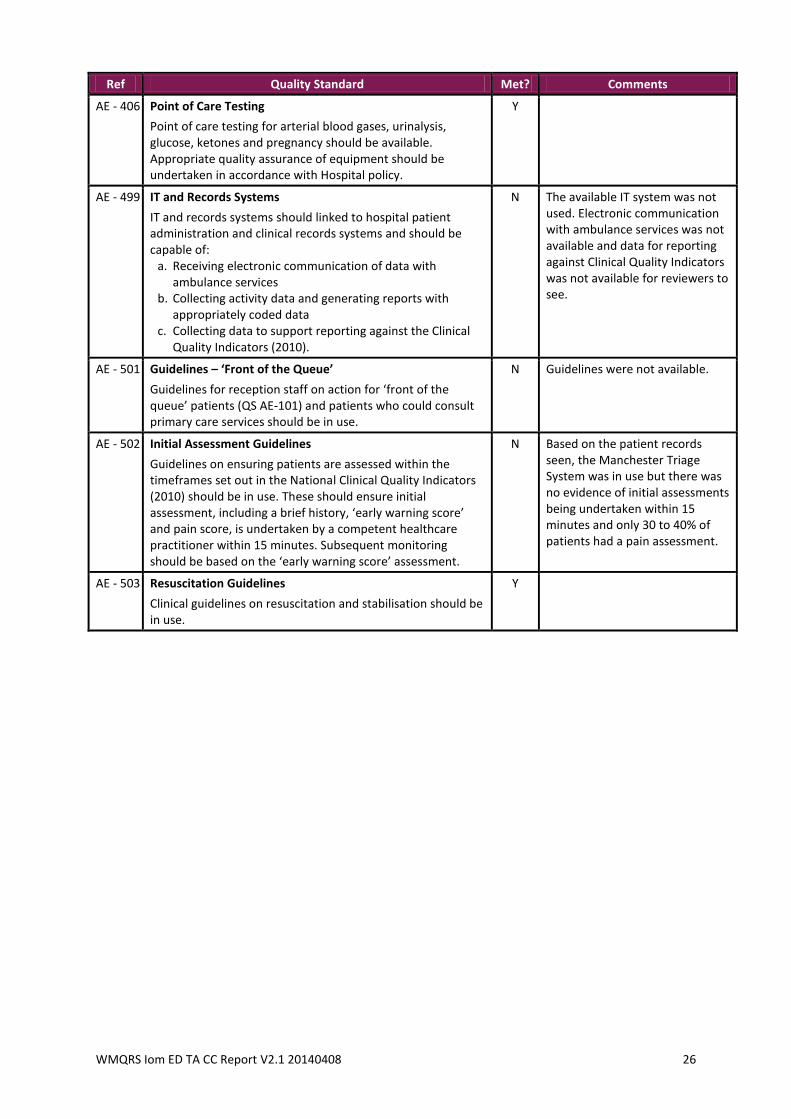
AE - 406 Point of Care Testing
Point of care testing for arterial blood gases, urinalysis, glucose, ketones and pregnancy should be available. Appropriate quality assurance of equipment should be undertaken in accordance with Hospital policy.
Y
AE - 499 IT and Records Systems
IT and records systems should linked to hospital patient administration and clinical records systems and should be capable of:
a. Receiving electronic communication of data with ambulance services
b. Collecting activity data and generating reports with appropriately coded data
c. Collecting data to support reporting against the Clinical Quality Indicators (2010).
N The available IT system was not used. Electronic communication with ambulance services was not available and data for reporting against Clinical Quality Indicators was not available for reviewers to see.
AE - 501 Guidelines – ‘Front of the Queue’
Guidelines for reception staff on action for ‘front of the queue’ patients (QS AE-101) and patients who could consult primary care services should be in use.
N Guidelines were not available.
AE - 502 Initial Assessment Guidelines
Guidelines on ensuring patients are assessed within the timeframes set out in the National Clinical Quality Indicators (2010) should be in use. These should ensure initial assessment, including a brief history, ‘early warning score’ and pain score, is undertaken by a competent healthcare practitioner within 15 minutes. Subsequent monitoring should be based on the ‘early warning score’ assessment.
N Based on the patient records seen, the Manchester Triage System was in use but there was no evidence of initial assessments being undertaken within 15 minutes and only 30 to 40% of patients had a pain assessment.
AE - 503 Resuscitation Guidelines
Clinical guidelines on resuscitation and stabilisation should be in use.
Y
WMQRS Iom ED TA CC Report V2.1 20140408 27
Ref Quality Standard Met? Comments
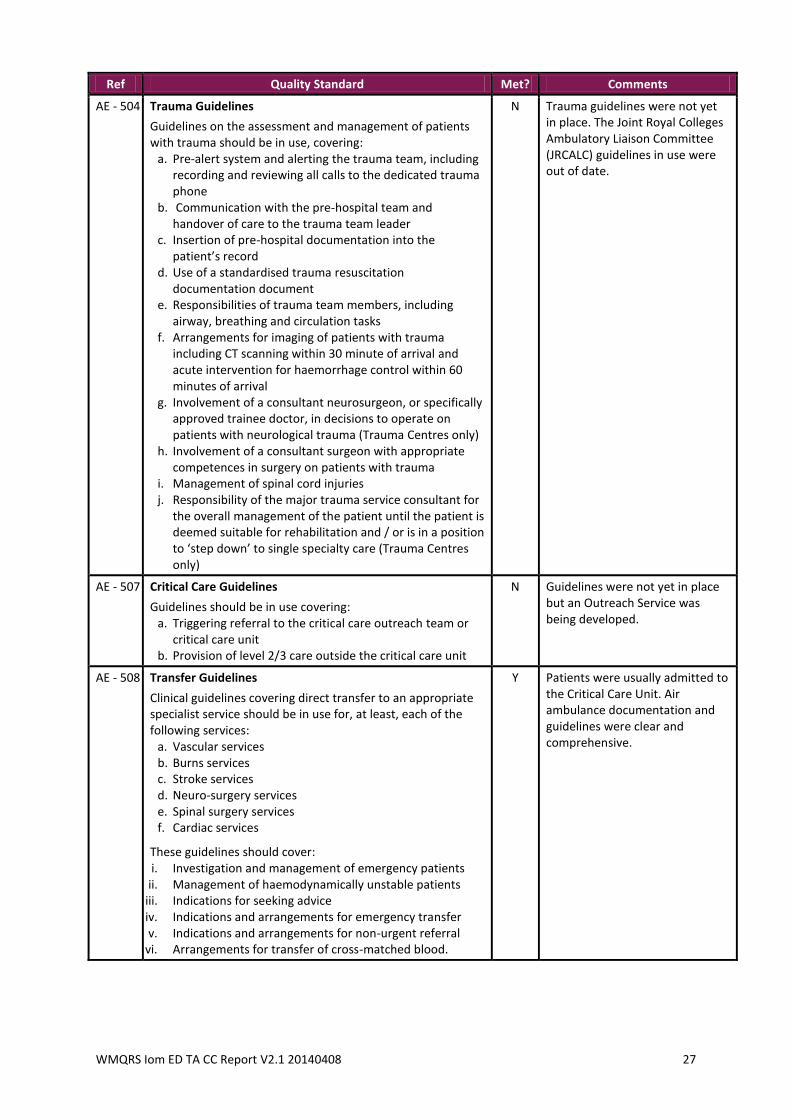
AE - 504 Trauma Guidelines
Guidelines on the assessment and management of patients with trauma should be in use, covering:
a. Pre-alert system and alerting the trauma team, including recording and reviewing all calls to the dedicated trauma phone
b. Communication with the pre-hospital team and handover of care to the trauma team leader
c. Insertion of pre-hospital documentation into the patient’s record
d. Use of a standardised trauma resuscitation documentation document
e. Responsibilities of trauma team members, including airway, breathing and circulation tasks
f. Arrangements for imaging of patients with trauma including CT scanning within 30 minute of arrival and acute intervention for haemorrhage control within 60 minutes of arrival
g. Involvement of a consultant neurosurgeon, or specifically approved trainee doctor, in decisions to operate on patients with neurological trauma (Trauma Centres only)
h. Involvement of a consultant surgeon with appropriate competences in surgery on patients with trauma
i. Management of spinal cord injuries j. Responsibility of the major trauma service consultant for
the overall management of the patient until the patient is deemed suitable for rehabilitation and / or is in a position to ‘step down’ to single specialty care (Trauma Centres only)
N Trauma guidelines were not yet in place. The Joint Royal Colleges Ambulatory Liaison Committee (JRCALC) guidelines in use were out of date.
AE - 507 Critical Care Guidelines
Guidelines should be in use covering: a. Triggering referral to the critical care outreach team or
critical care unit b. Provision of level 2/3 care outside the critical care unit
N Guidelines were not yet in place but an Outreach Service was being developed.
AE - 508 Transfer Guidelines
Clinical guidelines covering direct transfer to an appropriate specialist service should be in use for, at least, each of the following services:
a. Vascular services b. Burns services c. Stroke services d. Neuro-surgery services e. Spinal surgery services f. Cardiac services
These guidelines should cover: i. Investigation and management of emergency patients
ii. Management of haemodynamically unstable patients iii. Indications for seeking advice iv. Indications and arrangements for emergency transfer v. Indications and arrangements for non-urgent referral
vi. Arrangements for transfer of cross-matched blood.
Y Patients were usually admitted to the Critical Care Unit. Air ambulance documentation and guidelines were clear and comprehensive.
WMQRS Iom ED TA CC Report V2.1 20140408 28
Ref Quality Standard Met? Comments
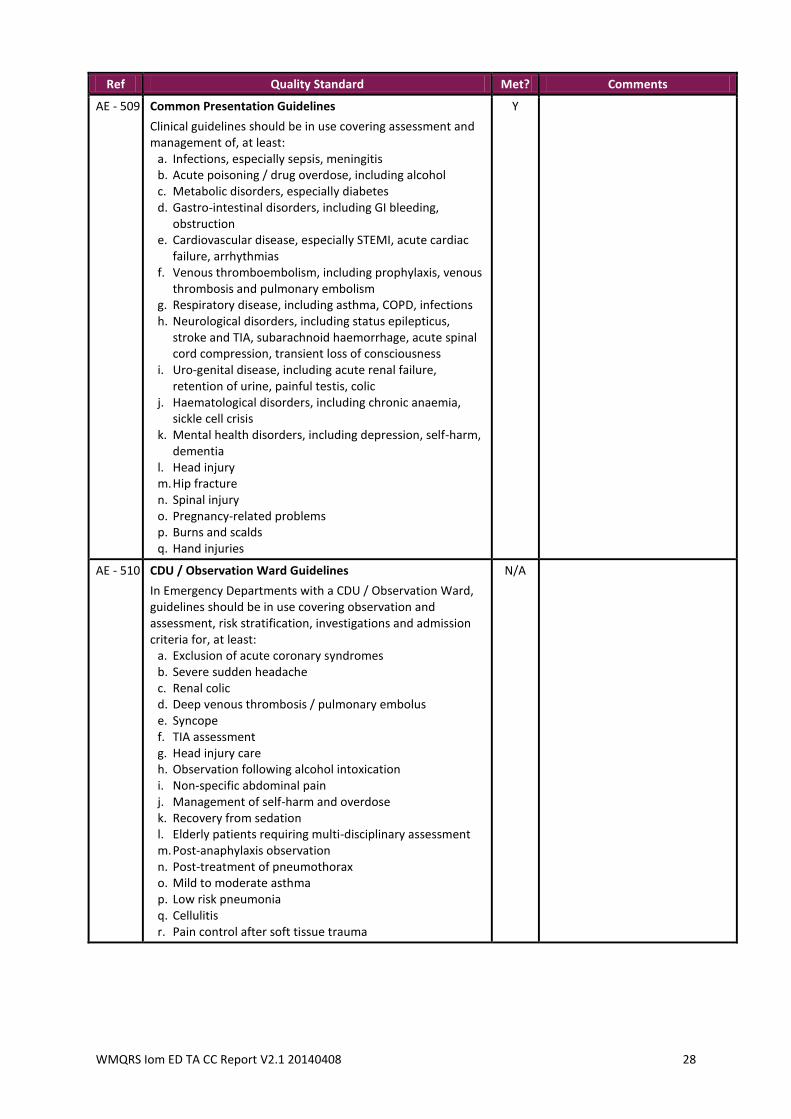
AE - 509 Common Presentation Guidelines
Clinical guidelines should be in use covering assessment and management of, at least:
a. Infections, especially sepsis, meningitis b. Acute poisoning / drug overdose, including alcohol c. Metabolic disorders, especially diabetes d. Gastro-intestinal disorders, including GI bleeding,
obstruction e. Cardiovascular disease, especially STEMI, acute cardiac
failure, arrhythmias f. Venous thromboembolism, including prophylaxis, venous
thrombosis and pulmonary embolism g. Respiratory disease, including asthma, COPD, infections h. Neurological disorders, including status epilepticus,
stroke and TIA, subarachnoid haemorrhage, acute spinal cord compression, transient loss of consciousness
i. Uro-genital disease, including acute renal failure, retention of urine, painful testis, colic
j. Haematological disorders, including chronic anaemia, sickle cell crisis
k. Mental health disorders, including depression, self-harm, dementia
l. Head injury m. Hip fracture n. Spinal injury o. Pregnancy-related problems p. Burns and scalds q. Hand injuries
Y
AE - 510 CDU / Observation Ward Guidelines
In Emergency Departments with a CDU / Observation Ward, guidelines should be in use covering observation and assessment, risk stratification, investigations and admission criteria for, at least:
a. Exclusion of acute coronary syndromes b. Severe sudden headache c. Renal colic d. Deep venous thrombosis / pulmonary embolus e. Syncope f. TIA assessment g. Head injury care h. Observation following alcohol intoxication i. Non-specific abdominal pain j. Management of self-harm and overdose k. Recovery from sedation l. Elderly patients requiring multi-disciplinary assessment m. Post-anaphylaxis observation n. Post-treatment of pneumothorax o. Mild to moderate asthma p. Low risk pneumonia q. Cellulitis r. Pain control after soft tissue trauma
N/A
WMQRS Iom ED TA CC Report V2.1 20140408 29
Ref Quality Standard Met? Comments
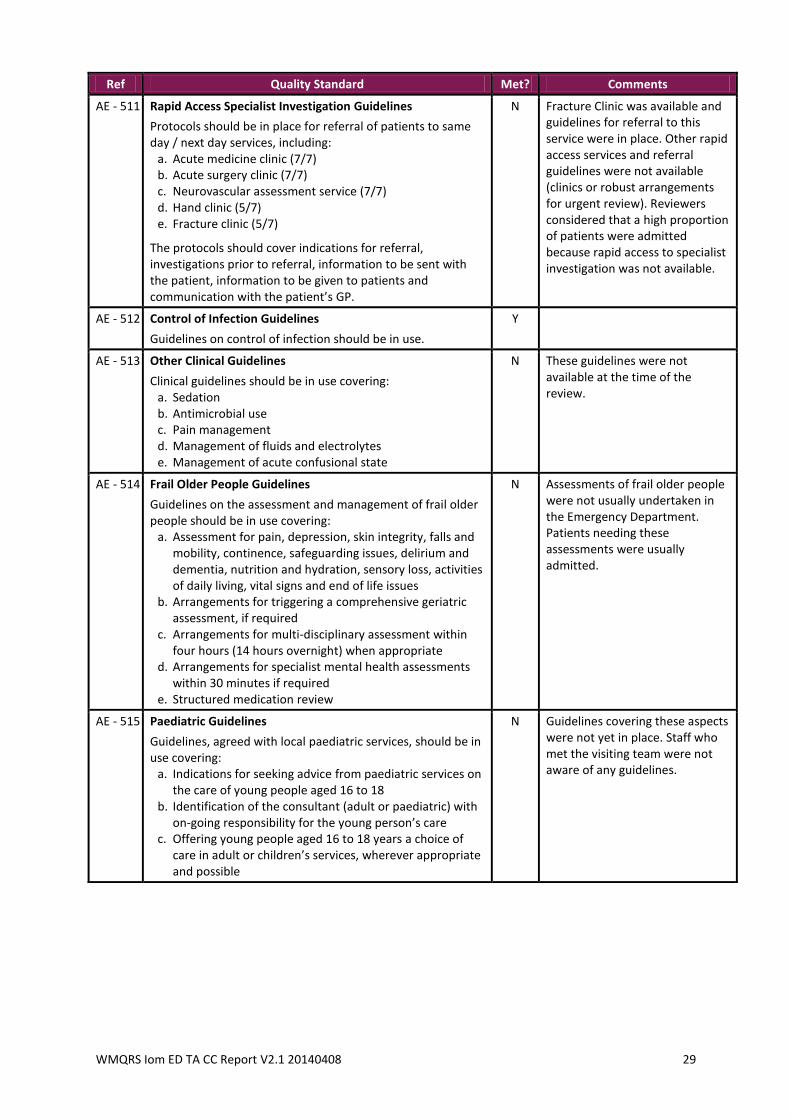
AE - 511 Rapid Access Specialist Investigation Guidelines
Protocols should be in place for referral of patients to same day / next day services, including:
a. Acute medicine clinic (7/7) b. Acute surgery clinic (7/7) c. Neurovascular assessment service (7/7) d. Hand clinic (5/7) e. Fracture clinic (5/7)
The protocols should cover indications for referral, investigations prior to referral, information to be sent with the patient, information to be given to patients and communication with the patient’s GP.
N Fracture Clinic was available and guidelines for referral to this service were in place. Other rapid access services and referral guidelines were not available (clinics or robust arrangements for urgent review). Reviewers considered that a high proportion of patients were admitted because rapid access to specialist investigation was not available.
AE - 512 Control of Infection Guidelines
Guidelines on control of infection should be in use.
Y
AE - 513 Other Clinical Guidelines
Clinical guidelines should be in use covering: a. Sedation b. Antimicrobial use c. Pain management d. Management of fluids and electrolytes e. Management of acute confusional state
N These guidelines were not available at the time of the review.
AE - 514 Frail Older People Guidelines
Guidelines on the assessment and management of frail older people should be in use covering:
a. Assessment for pain, depression, skin integrity, falls and mobility, continence, safeguarding issues, delirium and dementia, nutrition and hydration, sensory loss, activities of daily living, vital signs and end of life issues
b. Arrangements for triggering a comprehensive geriatric assessment, if required
c. Arrangements for multi-disciplinary assessment within four hours (14 hours overnight) when appropriate
d. Arrangements for specialist mental health assessments within 30 minutes if required
e. Structured medication review
N Assessments of frail older people were not usually undertaken in the Emergency Department. Patients needing these assessments were usually admitted.
AE - 515 Paediatric Guidelines
Guidelines, agreed with local paediatric services, should be in use covering:
a. Indications for seeking advice from paediatric services on the care of young people aged 16 to 18
b. Identification of the consultant (adult or paediatric) with on-going responsibility for the young person’s care
c. Offering young people aged 16 to 18 years a choice of care in adult or children’s services, wherever appropriate and possible
N Guidelines covering these aspects were not yet in place. Staff who met the visiting team were not aware of any guidelines.
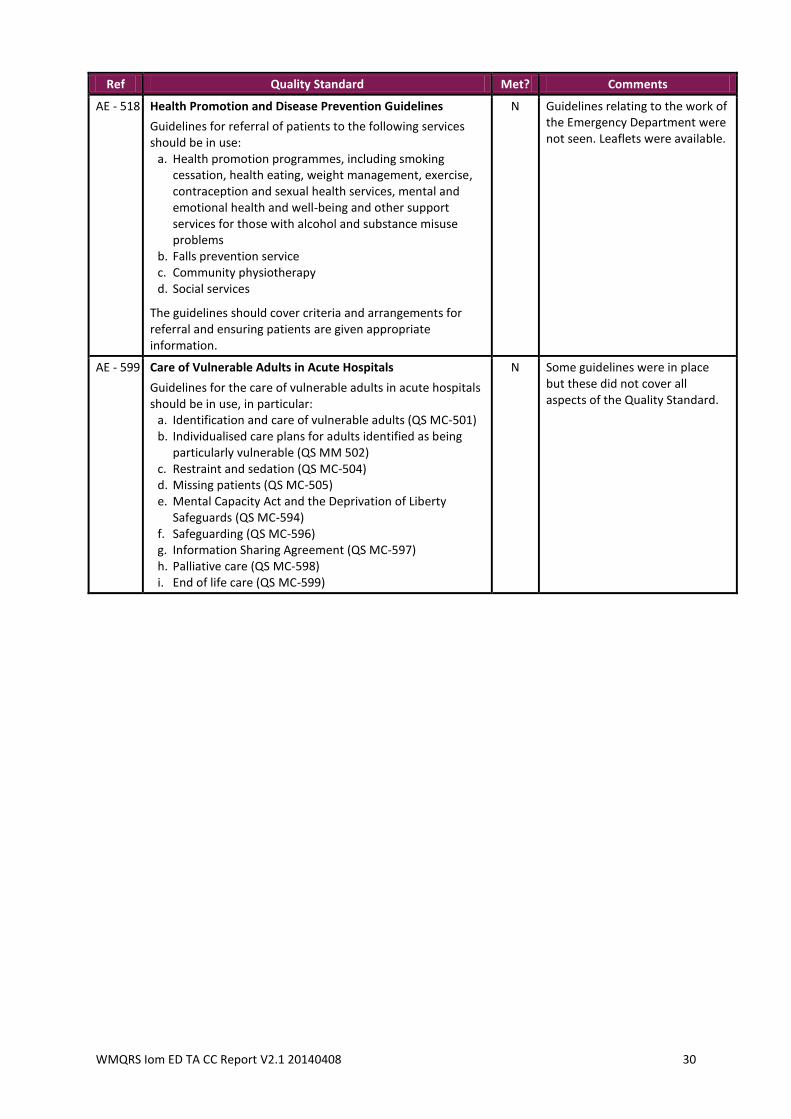
WMQRS Iom ED TA CC Report V2.1 20140408 30
Ref Quality Standard Met? Comments
AE - 518 Health Promotion and Disease Prevention Guidelines
Guidelines for referral of patients to the following services should be in use:
a. Health promotion programmes, including smoking cessation, health eating, weight management, exercise, contraception and sexual health services, mental and emotional health and well-being and other support services for those with alcohol and substance misuse problems
b. Falls prevention service c. Community physiotherapy d. Social services
The guidelines should cover criteria and arrangements for referral and ensuring patients are given appropriate information.
N Guidelines relating to the work of the Emergency Department were not seen. Leaflets were available.
AE - 599 Care of Vulnerable Adults in Acute Hospitals
Guidelines for the care of vulnerable adults in acute hospitals should be in use, in particular:
a. Identification and care of vulnerable adults (QS MC-501) b. Individualised care plans for adults identified as being
particularly vulnerable (QS MM 502) c. Restraint and sedation (QS MC-504) d. Missing patients (QS MC-505) e. Mental Capacity Act and the Deprivation of Liberty
Safeguards (QS MC-594) f. Safeguarding (QS MC-596) g. Information Sharing Agreement (QS MC-597) h. Palliative care (QS MC-598) i. End of life care (QS MC-599)
N Some guidelines were in place but these did not cover all aspects of the Quality Standard.
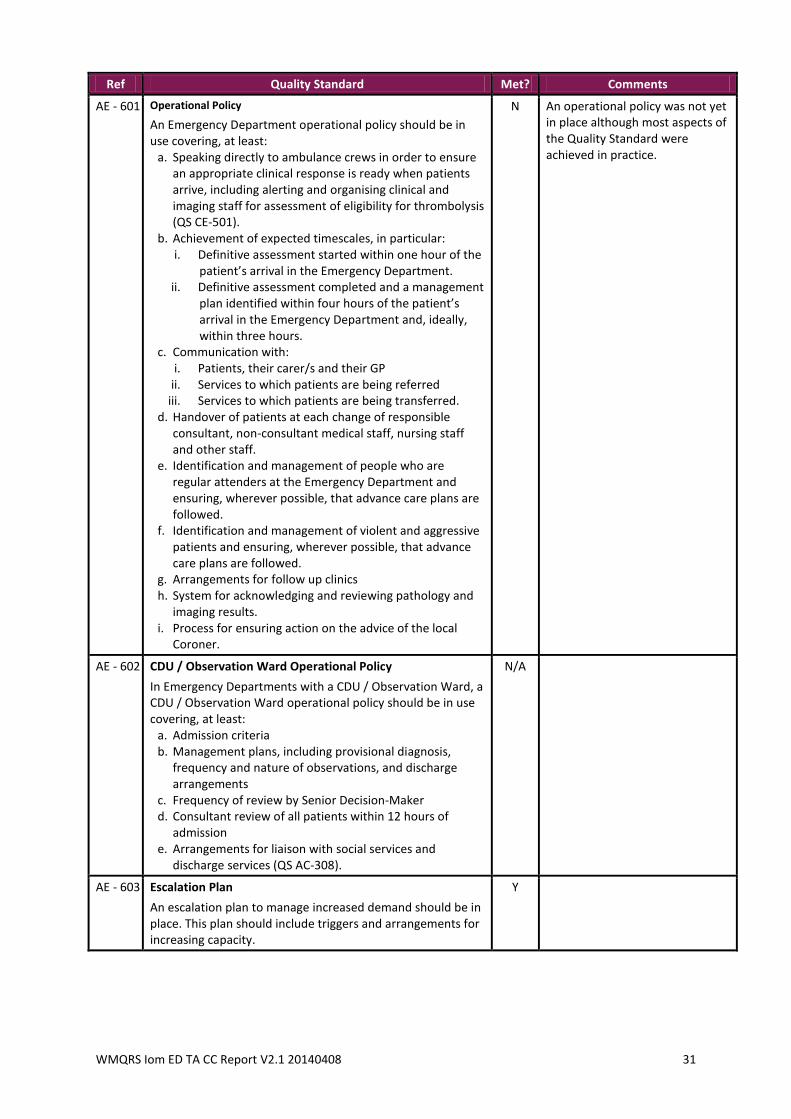
WMQRS Iom ED TA CC Report V2.1 20140408 31
Ref Quality Standard Met? Comments
AE - 601 Operational Policy
An Emergency Department operational policy should be in use covering, at least:
a. Speaking directly to ambulance crews in order to ensure an appropriate clinical response is ready when patients arrive, including alerting and organising clinical and imaging staff for assessment of eligibility for thrombolysis (QS CE-501).
b. Achievement of expected timescales, in particular: i. Definitive assessment started within one hour of the
patient’s arrival in the Emergency Department. ii. Definitive assessment completed and a management
plan identified within four hours of the patient’s arrival in the Emergency Department and, ideally, within three hours.
c. Communication with: i. Patients, their carer/s and their GP
ii. Services to which patients are being referred iii. Services to which patients are being transferred.
d. Handover of patients at each change of responsible consultant, non-consultant medical staff, nursing staff and other staff.
e. Identification and management of people who are regular attenders at the Emergency Department and ensuring, wherever possible, that advance care plans are followed.
f. Identification and management of violent and aggressive patients and ensuring, wherever possible, that advance care plans are followed.
g. Arrangements for follow up clinics h. System for acknowledging and reviewing pathology and
imaging results. i. Process for ensuring action on the advice of the local
Coroner.
N An operational policy was not yet in place although most aspects of the Quality Standard were achieved in practice.
AE - 602 CDU / Observation Ward Operational Policy
In Emergency Departments with a CDU / Observation Ward, a CDU / Observation Ward operational policy should be in use covering, at least:
a. Admission criteria b. Management plans, including provisional diagnosis,
frequency and nature of observations, and discharge arrangements
c. Frequency of review by Senior Decision-Maker d. Consultant review of all patients within 12 hours of
admission e. Arrangements for liaison with social services and
discharge services (QS AC-308).
N/A
AE - 603 Escalation Plan
An escalation plan to manage increased demand should be in place. This plan should include triggers and arrangements for increasing capacity.
Y
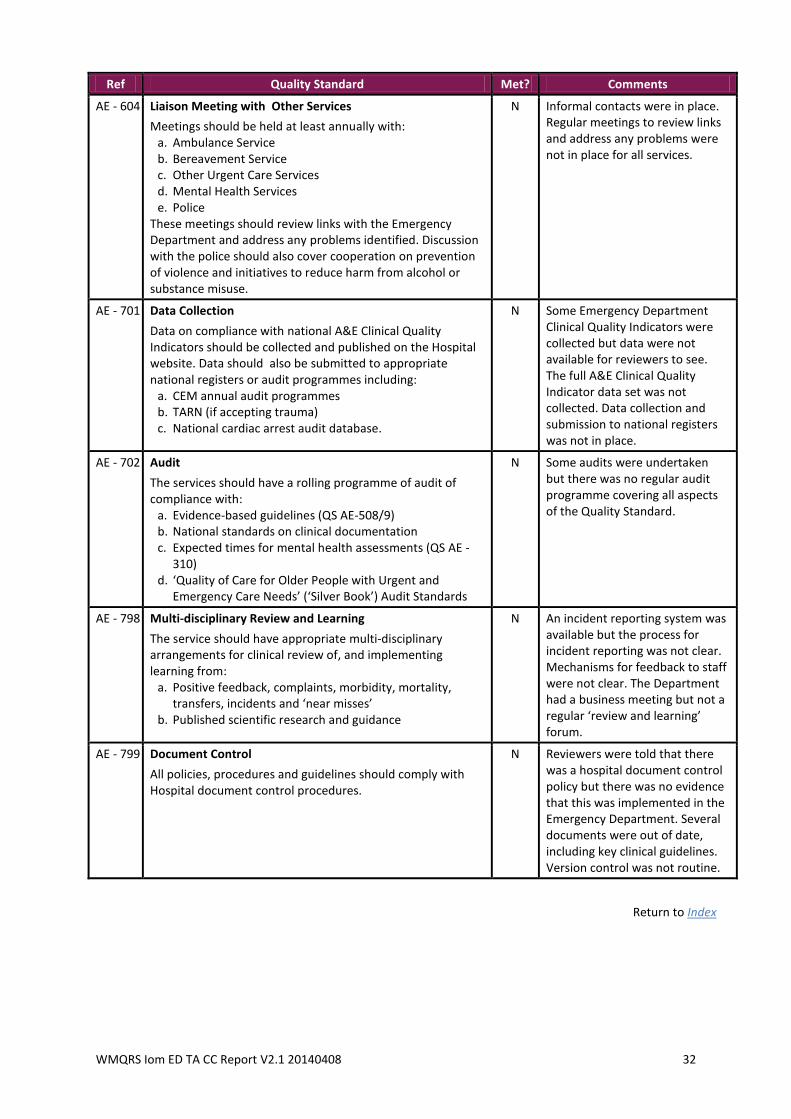
WMQRS Iom ED TA CC Report V2.1 20140408 32
Ref Quality Standard Met? Comments
AE - 604 Liaison Meeting with Other Services
Meetings should be held at least annually with: a. Ambulance Service b. Bereavement Service c. Other Urgent Care Services d. Mental Health Services e. Police
These meetings should review links with the Emergency Department and address any problems identified. Discussion with the police should also cover cooperation on prevention of violence and initiatives to reduce harm from alcohol or substance misuse.
N Informal contacts were in place. Regular meetings to review links and address any problems were not in place for all services.
AE - 701 Data Collection
Data on compliance with national A&E Clinical Quality Indicators should be collected and published on the Hospital website. Data should also be submitted to appropriate national registers or audit programmes including:
a. CEM annual audit programmes b. TARN (if accepting trauma) c. National cardiac arrest audit database.
N Some Emergency Department Clinical Quality Indicators were collected but data were not available for reviewers to see. The full A&E Clinical Quality Indicator data set was not collected. Data collection and submission to national registers was not in place.
AE - 702 Audit
The services should have a rolling programme of audit of compliance with:
a. Evidence-based guidelines (QS AE-508/9) b. National standards on clinical documentation c. Expected times for mental health assessments (QS AE -
310) d. ‘Quality of Care for Older People with Urgent and
Emergency Care Needs’ (‘Silver Book’) Audit Standards
N Some audits were undertaken but there was no regular audit programme covering all aspects of the Quality Standard.
AE - 798 Multi-disciplinary Review and Learning
The service should have appropriate multi-disciplinary arrangements for clinical review of, and implementing learning from:
a. Positive feedback, complaints, morbidity, mortality, transfers, incidents and ‘near misses’
b. Published scientific research and guidance
N An incident reporting system was available but the process for incident reporting was not clear. Mechanisms for feedback to staff were not clear. The Department had a business meeting but not a regular ‘review and learning’ forum.
AE - 799 Document Control
All policies, procedures and guidelines should comply with Hospital document control procedures.
N Reviewers were told that there was a hospital document control policy but there was no evidence that this was implemented in the Emergency Department. Several documents were out of date, including key clinical guidelines. Version control was not routine.
Return to Index
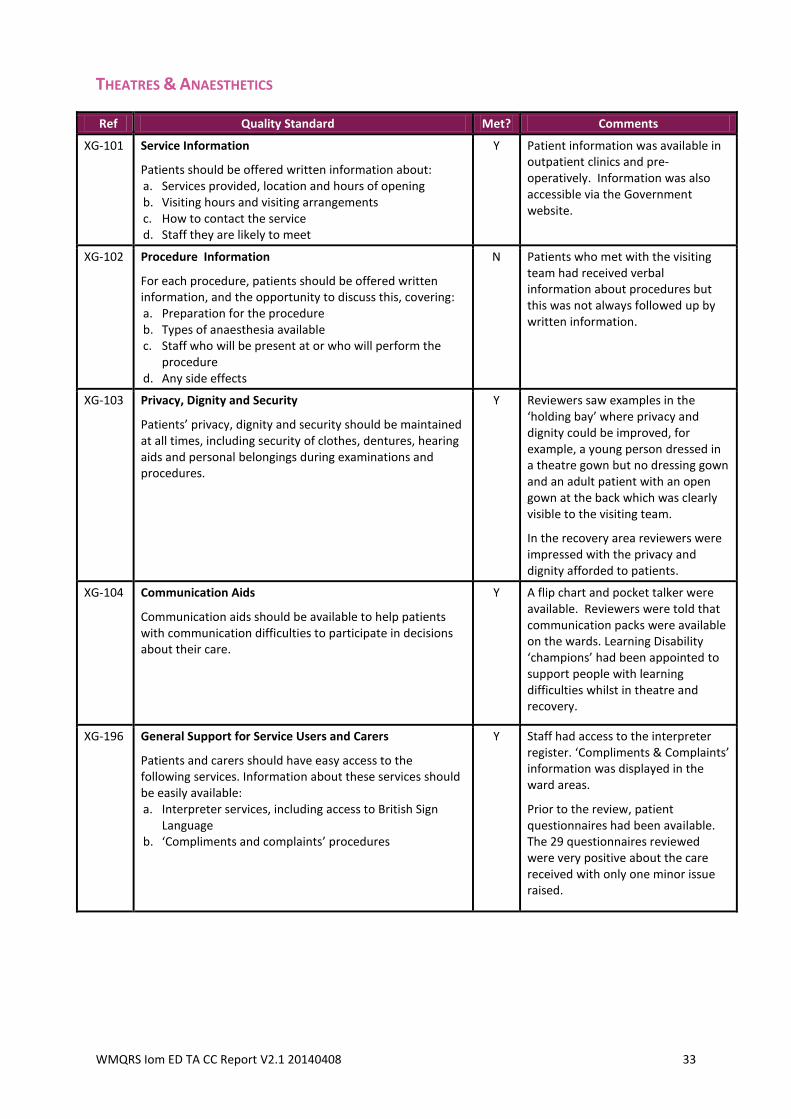
WMQRS Iom ED TA CC Report V2.1 20140408 33
THEATRES & ANAESTHETICS
Ref Quality Standard Met? Comments
XG-101
Service Information
Patients should be offered written information about: a. Services provided, location and hours of opening b. Visiting hours and visiting arrangements c. How to contact the service d. Staff they are likely to meet
Y Patient information was available in outpatient clinics and pre-operatively. Information was also accessible via the Government website.
XG-102 Procedure Information
For each procedure, patients should be offered written information, and the opportunity to discuss this, covering: a. Preparation for the procedure b. Types of anaesthesia available c. Staff who will be present at or who will perform the
procedure d. Any side effects
N Patients who met with the visiting team had received verbal information about procedures but this was not always followed up by written information.
XG-103 Privacy, Dignity and Security
Patients’ privacy, dignity and security should be maintained at all times, including security of clothes, dentures, hearing aids and personal belongings during examinations and procedures.
Y Reviewers saw examples in the ‘holding bay’ where privacy and dignity could be improved, for example, a young person dressed in a theatre gown but no dressing gown and an adult patient with an open gown at the back which was clearly visible to the visiting team.
In the recovery area reviewers were impressed with the privacy and dignity afforded to patients.
XG-104 Communication Aids
Communication aids should be available to help patients with communication difficulties to participate in decisions about their care.
Y A flip chart and pocket talker were available. Reviewers were told that communication packs were available on the wards. Learning Disability ‘champions’ had been appointed to support people with learning difficulties whilst in theatre and recovery.
XG-196 General Support for Service Users and Carers
Patients and carers should have easy access to the following services. Information about these services should be easily available: a. Interpreter services, including access to British Sign
Language b. ‘Compliments and complaints’ procedures
Y Staff had access to the interpreter register. ‘Compliments & Complaints’ information was displayed in the ward areas.
Prior to the review, patient questionnaires had been available. The 29 questionnaires reviewed were very positive about the care received with only one minor issue raised.
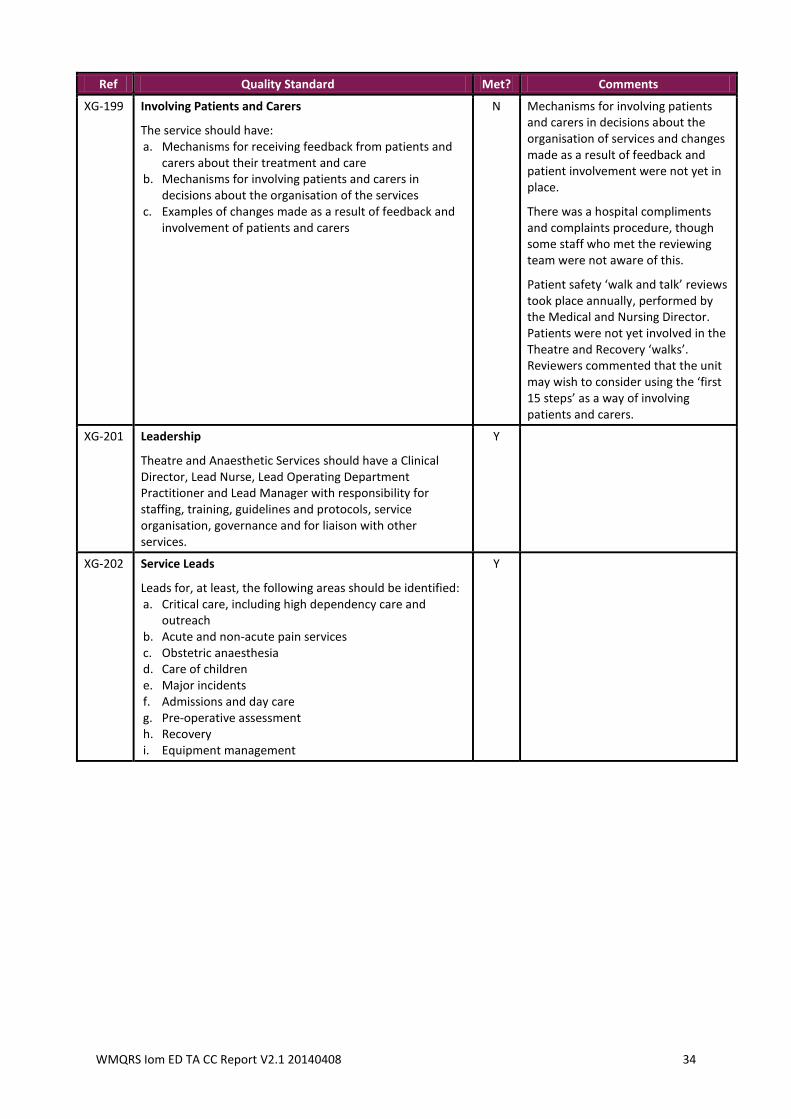
WMQRS Iom ED TA CC Report V2.1 20140408 34
Ref Quality Standard Met? Comments
XG-199 Involving Patients and Carers
The service should have: a. Mechanisms for receiving feedback from patients and
carers about their treatment and care b. Mechanisms for involving patients and carers in
decisions about the organisation of the services c. Examples of changes made as a result of feedback and
involvement of patients and carers
N Mechanisms for involving patients and carers in decisions about the organisation of services and changes made as a result of feedback and patient involvement were not yet in place.
There was a hospital compliments and complaints procedure, though some staff who met the reviewing team were not aware of this.
Patient safety ‘walk and talk’ reviews took place annually, performed by the Medical and Nursing Director. Patients were not yet involved in the Theatre and Recovery ‘walks’. Reviewers commented that the unit may wish to consider using the ‘first 15 steps’ as a way of involving patients and carers.
XG-201 Leadership
Theatre and Anaesthetic Services should have a Clinical Director, Lead Nurse, Lead Operating Department Practitioner and Lead Manager with responsibility for staffing, training, guidelines and protocols, service organisation, governance and for liaison with other services.
Y
XG-202 Service Leads
Leads for, at least, the following areas should be identified: a. Critical care, including high dependency care and
outreach b. Acute and non-acute pain services c. Obstetric anaesthesia d. Care of children e. Major incidents f. Admissions and day care g. Pre-operative assessment h. Recovery i. Equipment management
Y
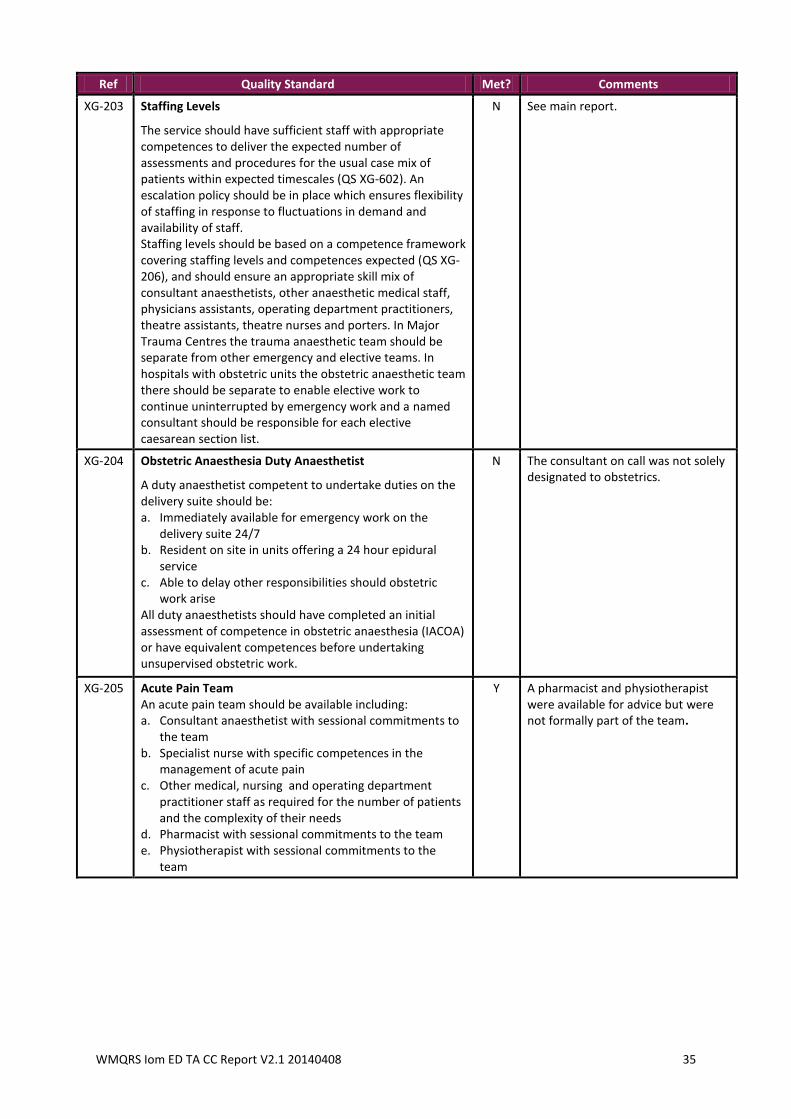
WMQRS Iom ED TA CC Report V2.1 20140408 35
Ref Quality Standard Met? Comments
XG-203 Staffing Levels
The service should have sufficient staff with appropriate competences to deliver the expected number of assessments and procedures for the usual case mix of patients within expected timescales (QS XG-602). An escalation policy should be in place which ensures flexibility of staffing in response to fluctuations in demand and availability of staff. Staffing levels should be based on a competence framework covering staffing levels and competences expected (QS XG-206), and should ensure an appropriate skill mix of consultant anaesthetists, other anaesthetic medical staff, physicians assistants, operating department practitioners, theatre assistants, theatre nurses and porters. In Major Trauma Centres the trauma anaesthetic team should be separate from other emergency and elective teams. In hospitals with obstetric units the obstetric anaesthetic team there should be separate to enable elective work to continue uninterrupted by emergency work and a named consultant should be responsible for each elective caesarean section list.
N See main report.
XG-204 Obstetric Anaesthesia Duty Anaesthetist
A duty anaesthetist competent to undertake duties on the delivery suite should be: a. Immediately available for emergency work on the
delivery suite 24/7 b. Resident on site in units offering a 24 hour epidural
service c. Able to delay other responsibilities should obstetric
work arise All duty anaesthetists should have completed an initial assessment of competence in obstetric anaesthesia (IACOA) or have equivalent competences before undertaking unsupervised obstetric work.
N The consultant on call was not solely designated to obstetrics.
XG-205 Acute Pain Team An acute pain team should be available including: a. Consultant anaesthetist with sessional commitments to
the team b. Specialist nurse with specific competences in the
management of acute pain c. Other medical, nursing and operating department
practitioner staff as required for the number of patients and the complexity of their needs
d. Pharmacist with sessional commitments to the team e. Physiotherapist with sessional commitments to the
team
Y A pharmacist and physiotherapist were available for advice but were not formally part of the team.
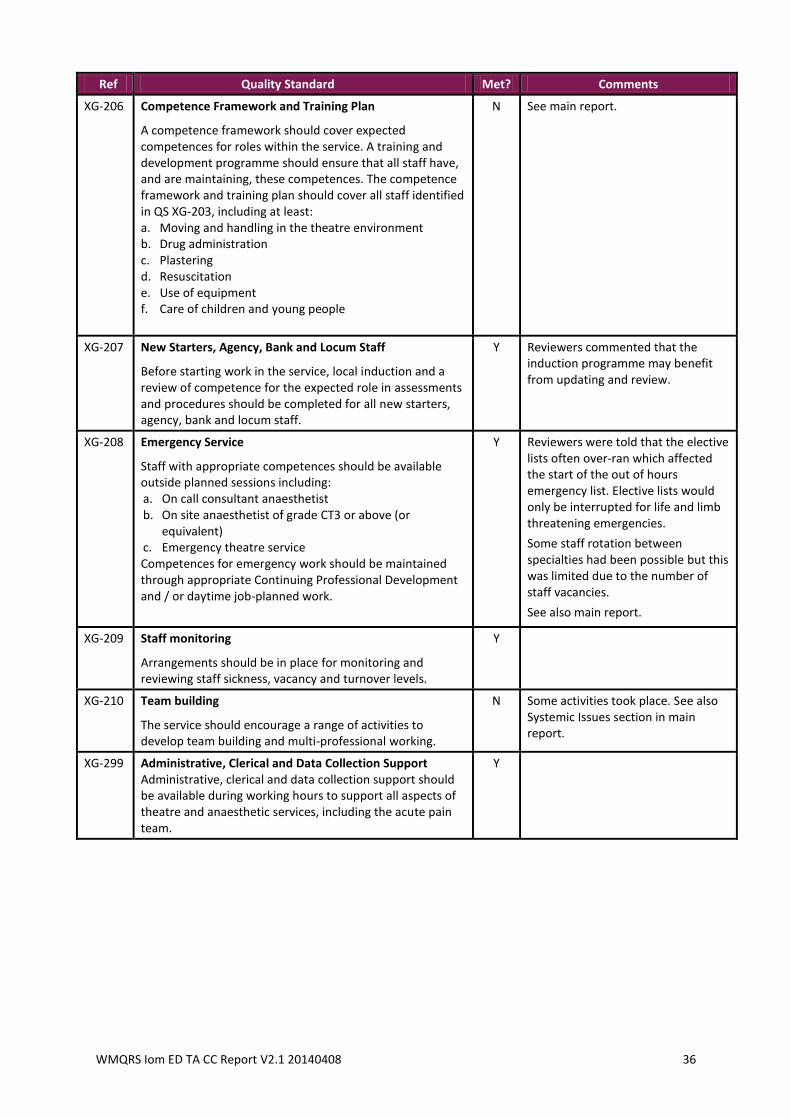
WMQRS Iom ED TA CC Report V2.1 20140408 36
Ref Quality Standard Met? Comments
XG-206 Competence Framework and Training Plan
A competence framework should cover expected competences for roles within the service. A training and development programme should ensure that all staff have, and are maintaining, these competences. The competence framework and training plan should cover all staff identified in QS XG-203, including at least: a. Moving and handling in the theatre environment b. Drug administration c. Plastering d. Resuscitation e. Use of equipment f. Care of children and young people
N See main report.
XG-207 New Starters, Agency, Bank and Locum Staff
Before starting work in the service, local induction and a review of competence for the expected role in assessments and procedures should be completed for all new starters, agency, bank and locum staff.
Y Reviewers commented that the induction programme may benefit from updating and review.
XG-208
Emergency Service
Staff with appropriate competences should be available outside planned sessions including: a. On call consultant anaesthetist b. On site anaesthetist of grade CT3 or above (or
equivalent) c. Emergency theatre service Competences for emergency work should be maintained through appropriate Continuing Professional Development and / or daytime job-planned work.
Y
Reviewers were told that the elective lists often over-ran which affected the start of the out of hours emergency list. Elective lists would only be interrupted for life and limb threatening emergencies.
Some staff rotation between specialties had been possible but this was limited due to the number of staff vacancies.
See also main report.
XG-209
Staff monitoring
Arrangements should be in place for monitoring and reviewing staff sickness, vacancy and turnover levels.
Y
XG-210
Team building
The service should encourage a range of activities to develop team building and multi-professional working.
N Some activities took place. See also Systemic Issues section in main report.
XG-299
Administrative, Clerical and Data Collection Support Administrative, clerical and data collection support should be available during working hours to support all aspects of theatre and anaesthetic services, including the acute pain team.
Y
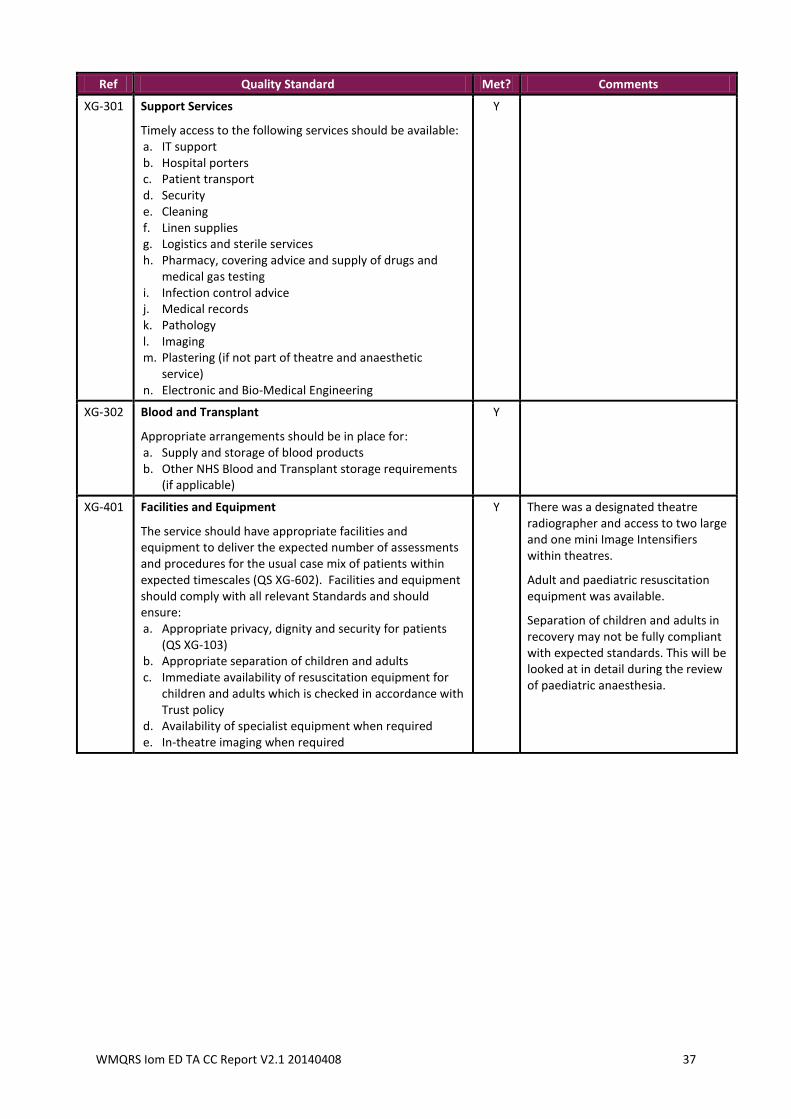
WMQRS Iom ED TA CC Report V2.1 20140408 37
Ref Quality Standard Met? Comments
XG-301
Support Services
Timely access to the following services should be available: a. IT support b. Hospital porters c. Patient transport d. Security e. Cleaning f. Linen supplies g. Logistics and sterile services h. Pharmacy, covering advice and supply of drugs and
medical gas testing i. Infection control advice j. Medical records k. Pathology l. Imaging m. Plastering (if not part of theatre and anaesthetic
service) n. Electronic and Bio-Medical Engineering
Y
XG-302
Blood and Transplant
Appropriate arrangements should be in place for: a. Supply and storage of blood products b. Other NHS Blood and Transplant storage requirements
(if applicable)
Y
XG-401
Facilities and Equipment
The service should have appropriate facilities and equipment to deliver the expected number of assessments and procedures for the usual case mix of patients within expected timescales (QS XG-602). Facilities and equipment should comply with all relevant Standards and should ensure: a. Appropriate privacy, dignity and security for patients
(QS XG-103) b. Appropriate separation of children and adults c. Immediate availability of resuscitation equipment for
children and adults which is checked in accordance with Trust policy
d. Availability of specialist equipment when required e. In-theatre imaging when required
Y There was a designated theatre radiographer and access to two large and one mini Image Intensifiers within theatres.
Adult and paediatric resuscitation equipment was available.
Separation of children and adults in recovery may not be fully compliant with expected standards. This will be looked at in detail during the review of paediatric anaesthesia.
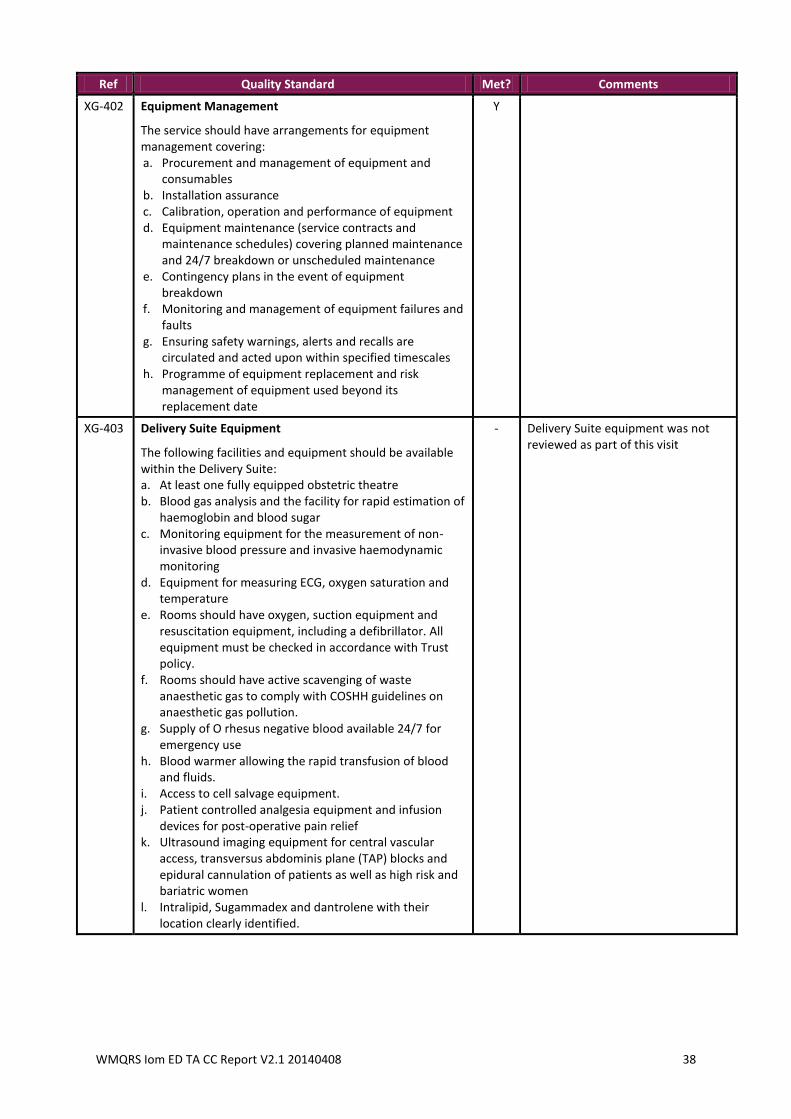
WMQRS Iom ED TA CC Report V2.1 20140408 38
Ref Quality Standard Met? Comments
XG-402
Equipment Management
The service should have arrangements for equipment management covering: a. Procurement and management of equipment and
consumables b. Installation assurance c. Calibration, operation and performance of equipment d. Equipment maintenance (service contracts and
maintenance schedules) covering planned maintenance and 24/7 breakdown or unscheduled maintenance
e. Contingency plans in the event of equipment breakdown
f. Monitoring and management of equipment failures and faults
g. Ensuring safety warnings, alerts and recalls are circulated and acted upon within specified timescales
h. Programme of equipment replacement and risk management of equipment used beyond its replacement date
Y
XG-403 Delivery Suite Equipment
The following facilities and equipment should be available within the Delivery Suite: a. At least one fully equipped obstetric theatre b. Blood gas analysis and the facility for rapid estimation of
haemoglobin and blood sugar c. Monitoring equipment for the measurement of non-
invasive blood pressure and invasive haemodynamic monitoring
d. Equipment for measuring ECG, oxygen saturation and temperature
e. Rooms should have oxygen, suction equipment and resuscitation equipment, including a defibrillator. All equipment must be checked in accordance with Trust policy.
f. Rooms should have active scavenging of waste anaesthetic gas to comply with COSHH guidelines on anaesthetic gas pollution.
g. Supply of O rhesus negative blood available 24/7 for emergency use
h. Blood warmer allowing the rapid transfusion of blood and fluids.
i. Access to cell salvage equipment. j. Patient controlled analgesia equipment and infusion
devices for post-operative pain relief k. Ultrasound imaging equipment for central vascular
access, transversus abdominis plane (TAP) blocks and epidural cannulation of patients as well as high risk and bariatric women
l. Intralipid, Sugammadex and dantrolene with their location clearly identified.
- Delivery Suite equipment was not reviewed as part of this visit
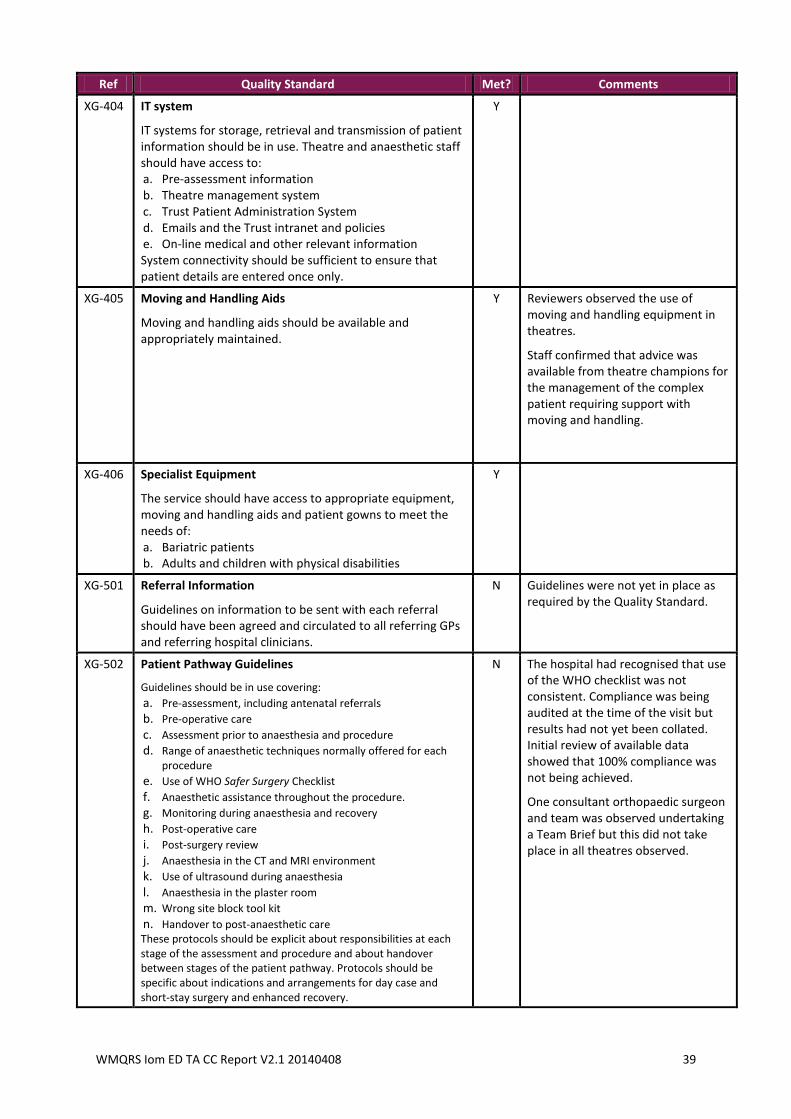
WMQRS Iom ED TA CC Report V2.1 20140408 39
Ref Quality Standard Met? Comments
XG-404
IT system
IT systems for storage, retrieval and transmission of patient information should be in use. Theatre and anaesthetic staff should have access to: a. Pre-assessment information b. Theatre management system c. Trust Patient Administration System d. Emails and the Trust intranet and policies e. On-line medical and other relevant information System connectivity should be sufficient to ensure that patient details are entered once only.
Y
XG-405
Moving and Handling Aids
Moving and handling aids should be available and appropriately maintained.
Y Reviewers observed the use of moving and handling equipment in theatres.
Staff confirmed that advice was available from theatre champions for the management of the complex patient requiring support with moving and handling.
XG-406
Specialist Equipment
The service should have access to appropriate equipment, moving and handling aids and patient gowns to meet the needs of: a. Bariatric patients b. Adults and children with physical disabilities
Y
XG-501
Referral Information
Guidelines on information to be sent with each referral should have been agreed and circulated to all referring GPs and referring hospital clinicians.
N Guidelines were not yet in place as required by the Quality Standard.
XG-502
Patient Pathway Guidelines
Guidelines should be in use covering:
a. Pre-assessment, including antenatal referrals
b. Pre-operative care
c. Assessment prior to anaesthesia and procedure
d. Range of anaesthetic techniques normally offered for each procedure
e. Use of WHO Safer Surgery Checklist
f. Anaesthetic assistance throughout the procedure.
g. Monitoring during anaesthesia and recovery
h. Post-operative care
i. Post-surgery review
j. Anaesthesia in the CT and MRI environment
k. Use of ultrasound during anaesthesia
l. Anaesthesia in the plaster room
m. Wrong site block tool kit
n. Handover to post-anaesthetic care These protocols should be explicit about responsibilities at each stage of the assessment and procedure and about handover between stages of the patient pathway. Protocols should be specific about indications and arrangements for day case and short-stay surgery and enhanced recovery.
N The hospital had recognised that use of the WHO checklist was not consistent. Compliance was being audited at the time of the visit but results had not yet been collated. Initial review of available data showed that 100% compliance was not being achieved.
One consultant orthopaedic surgeon and team was observed undertaking a Team Brief but this did not take place in all theatres observed.
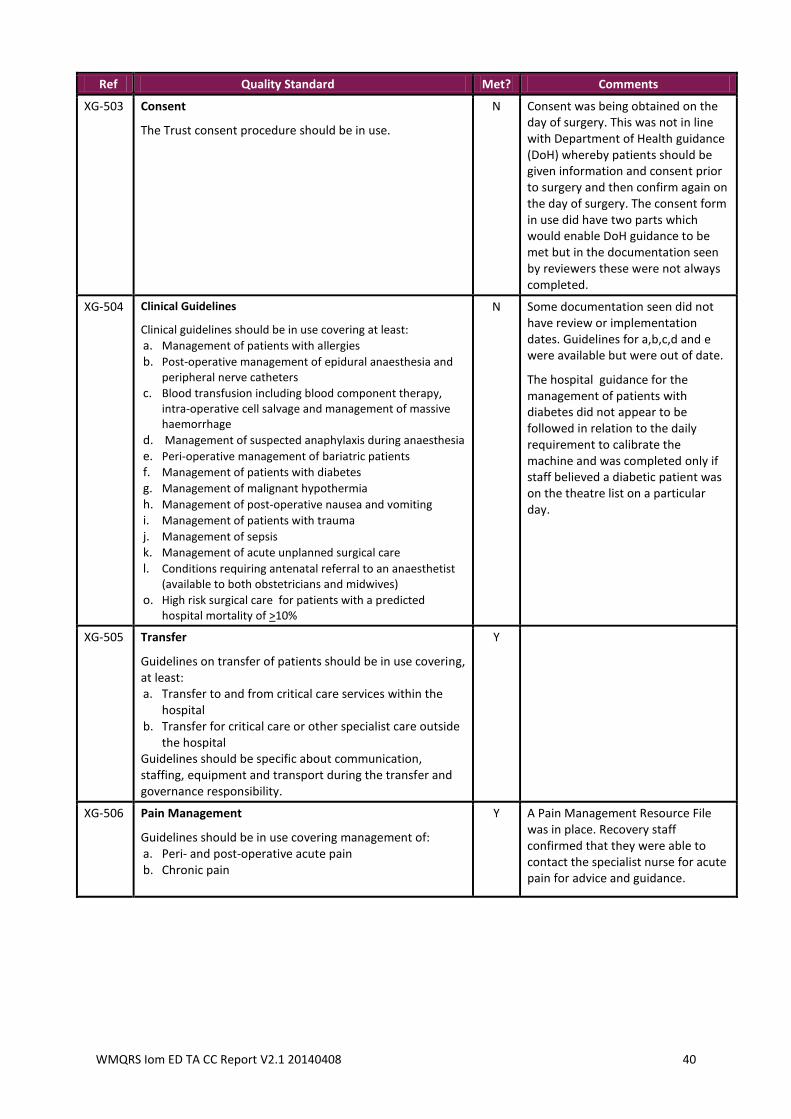
WMQRS Iom ED TA CC Report V2.1 20140408 40
Ref Quality Standard Met? Comments
XG-503
Consent
The Trust consent procedure should be in use.
N Consent was being obtained on the day of surgery. This was not in line with Department of Health guidance (DoH) whereby patients should be given information and consent prior to surgery and then confirm again on the day of surgery. The consent form in use did have two parts which would enable DoH guidance to be met but in the documentation seen by reviewers these were not always completed.
XG-504
Clinical Guidelines
Clinical guidelines should be in use covering at least:
a. Management of patients with allergies
b. Post-operative management of epidural anaesthesia and peripheral nerve catheters
c. Blood transfusion including blood component therapy, intra-operative cell salvage and management of massive haemorrhage
d. Management of suspected anaphylaxis during anaesthesia
e. Peri-operative management of bariatric patients
f. Management of patients with diabetes
g. Management of malignant hypothermia
h. Management of post-operative nausea and vomiting
i. Management of patients with trauma
j. Management of sepsis
k. Management of acute unplanned surgical care
l. Conditions requiring antenatal referral to an anaesthetist (available to both obstetricians and midwives)
o. High risk surgical care for patients with a predicted hospital mortality of >10%
N Some documentation seen did not have review or implementation dates. Guidelines for a,b,c,d and e were available but were out of date.
The hospital guidance for the management of patients with diabetes did not appear to be followed in relation to the daily requirement to calibrate the machine and was completed only if staff believed a diabetic patient was on the theatre list on a particular day.
XG-505
Transfer
Guidelines on transfer of patients should be in use covering, at least: a. Transfer to and from critical care services within the
hospital b. Transfer for critical care or other specialist care outside
the hospital Guidelines should be specific about communication, staffing, equipment and transport during the transfer and governance responsibility.
Y
XG-506
Pain Management
Guidelines should be in use covering management of: a. Peri- and post-operative acute pain b. Chronic pain
Y A Pain Management Resource File was in place. Recovery staff confirmed that they were able to contact the specialist nurse for acute pain for advice and guidance.
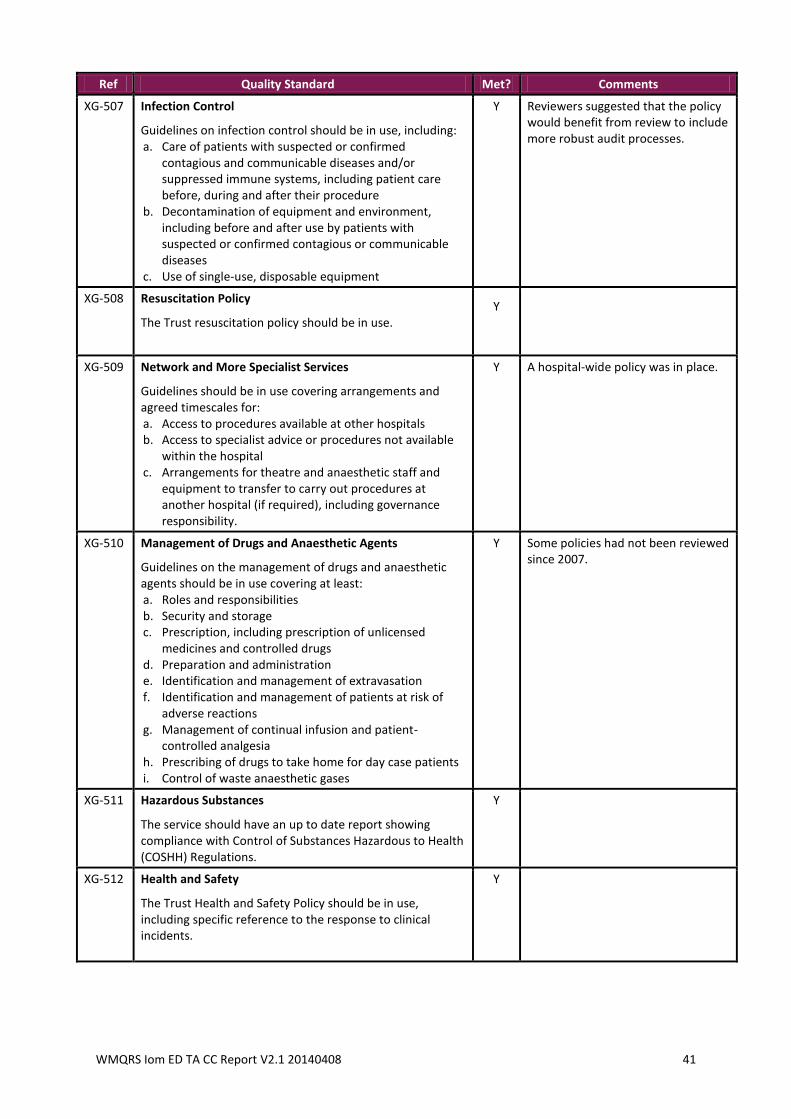
WMQRS Iom ED TA CC Report V2.1 20140408 41
Ref Quality Standard Met? Comments
XG-507
Infection Control
Guidelines on infection control should be in use, including: a. Care of patients with suspected or confirmed
contagious and communicable diseases and/or suppressed immune systems, including patient care before, during and after their procedure
b. Decontamination of equipment and environment, including before and after use by patients with suspected or confirmed contagious or communicable diseases
c. Use of single-use, disposable equipment
Y Reviewers suggested that the policy would benefit from review to include more robust audit processes.
XG-508
Resuscitation Policy
The Trust resuscitation policy should be in use. Y
XG-509
Network and More Specialist Services
Guidelines should be in use covering arrangements and agreed timescales for: a. Access to procedures available at other hospitals b. Access to specialist advice or procedures not available
within the hospital c. Arrangements for theatre and anaesthetic staff and
equipment to transfer to carry out procedures at another hospital (if required), including governance responsibility.
Y A hospital-wide policy was in place.
XG-510
Management of Drugs and Anaesthetic Agents
Guidelines on the management of drugs and anaesthetic agents should be in use covering at least: a. Roles and responsibilities b. Security and storage c. Prescription, including prescription of unlicensed
medicines and controlled drugs d. Preparation and administration e. Identification and management of extravasation f. Identification and management of patients at risk of
adverse reactions g. Management of continual infusion and patient-
controlled analgesia h. Prescribing of drugs to take home for day case patients i. Control of waste anaesthetic gases
Y Some policies had not been reviewed since 2007.
XG-511
Hazardous Substances
The service should have an up to date report showing compliance with Control of Substances Hazardous to Health (COSHH) Regulations.
Y
XG-512 Health and Safety
The Trust Health and Safety Policy should be in use, including specific reference to the response to clinical incidents.
Y
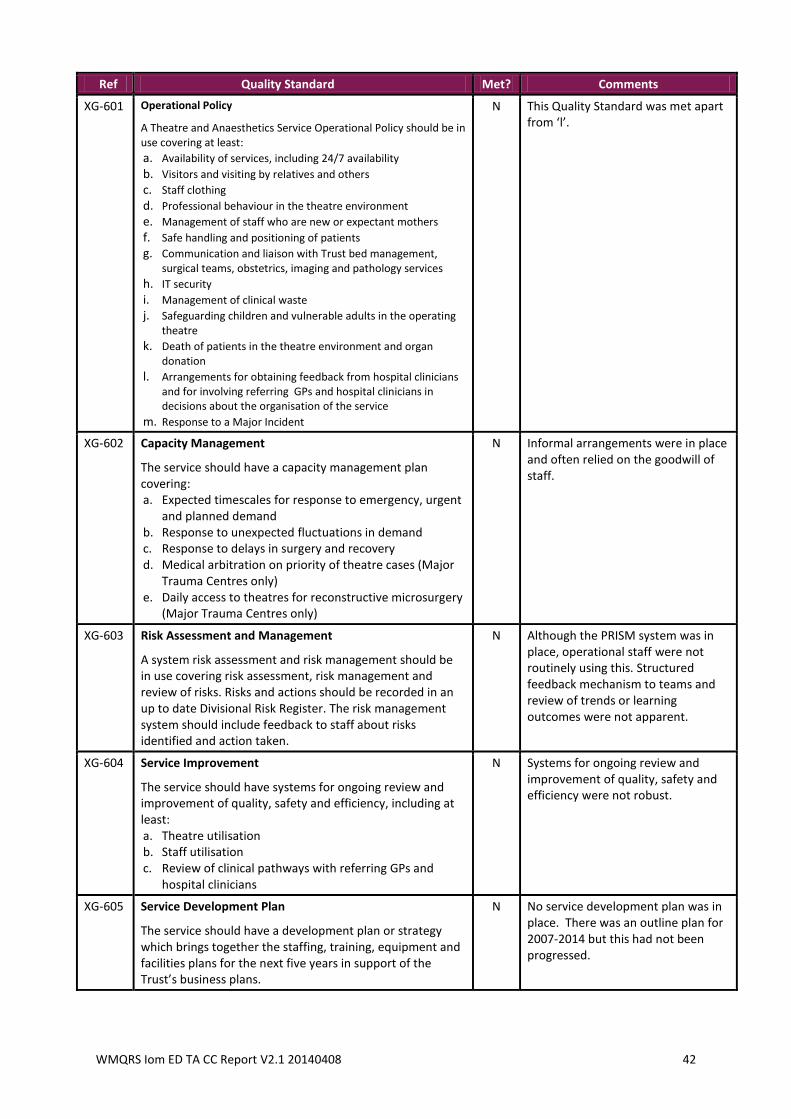
WMQRS Iom ED TA CC Report V2.1 20140408 42
Ref Quality Standard Met? Comments
XG-601
Operational Policy
A Theatre and Anaesthetics Service Operational Policy should be in use covering at least:
a. Availability of services, including 24/7 availability
b. Visitors and visiting by relatives and others
c. Staff clothing
d. Professional behaviour in the theatre environment
e. Management of staff who are new or expectant mothers
f. Safe handling and positioning of patients
g. Communication and liaison with Trust bed management, surgical teams, obstetrics, imaging and pathology services
h. IT security
i. Management of clinical waste
j. Safeguarding children and vulnerable adults in the operating theatre
k. Death of patients in the theatre environment and organ donation
l. Arrangements for obtaining feedback from hospital clinicians and for involving referring GPs and hospital clinicians in decisions about the organisation of the service
m. Response to a Major Incident
N This Quality Standard was met apart from ‘l’.
XG-602
Capacity Management
The service should have a capacity management plan covering: a. Expected timescales for response to emergency, urgent
and planned demand b. Response to unexpected fluctuations in demand c. Response to delays in surgery and recovery d. Medical arbitration on priority of theatre cases (Major
Trauma Centres only) e. Daily access to theatres for reconstructive microsurgery
(Major Trauma Centres only)
N Informal arrangements were in place and often relied on the goodwill of staff.
XG-603
Risk Assessment and Management
A system risk assessment and risk management should be in use covering risk assessment, risk management and review of risks. Risks and actions should be recorded in an up to date Divisional Risk Register. The risk management system should include feedback to staff about risks identified and action taken.
N Although the PRISM system was in place, operational staff were not routinely using this. Structured feedback mechanism to teams and review of trends or learning outcomes were not apparent.
XG-604
Service Improvement
The service should have systems for ongoing review and improvement of quality, safety and efficiency, including at least: a. Theatre utilisation b. Staff utilisation c. Review of clinical pathways with referring GPs and
hospital clinicians
N Systems for ongoing review and improvement of quality, safety and efficiency were not robust.
XG-605
Service Development Plan
The service should have a development plan or strategy which brings together the staffing, training, equipment and facilities plans for the next five years in support of the Trust’s business plans.
N No service development plan was in place. There was an outline plan for 2007-2014 but this had not been progressed.
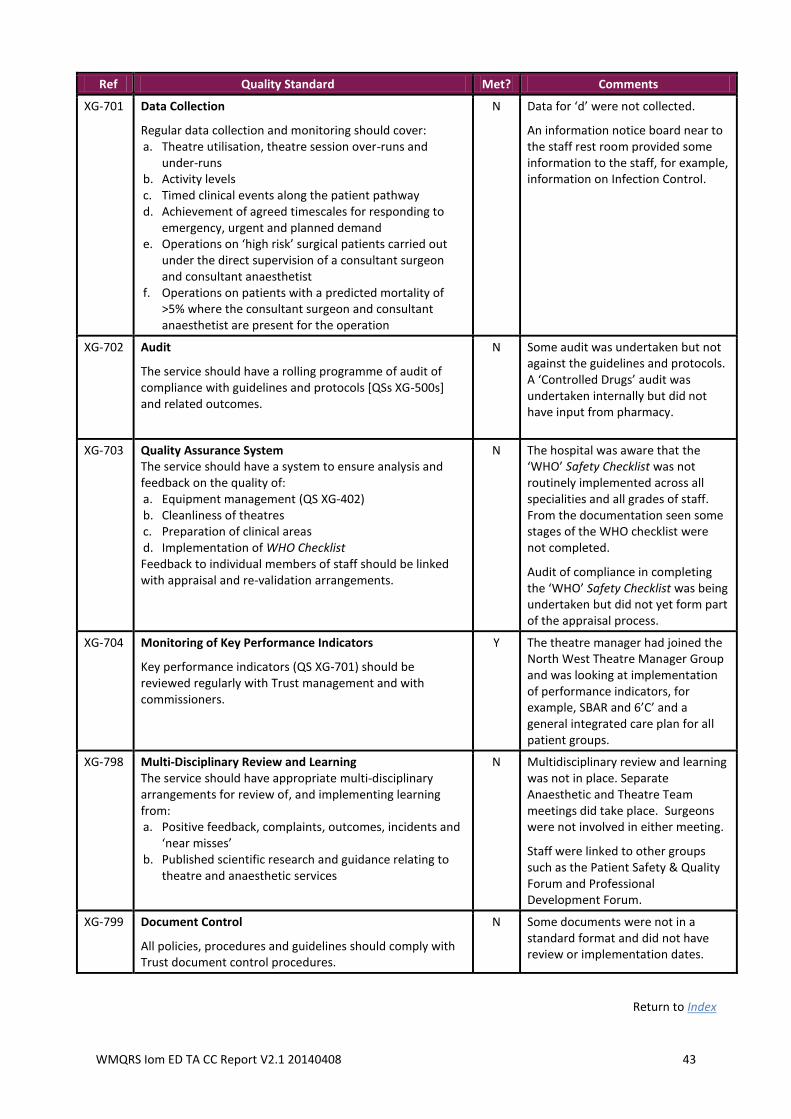
WMQRS Iom ED TA CC Report V2.1 20140408 43
Ref Quality Standard Met? Comments
XG-701
Data Collection
Regular data collection and monitoring should cover: a. Theatre utilisation, theatre session over-runs and
under-runs b. Activity levels c. Timed clinical events along the patient pathway d. Achievement of agreed timescales for responding to
emergency, urgent and planned demand e. Operations on ‘high risk’ surgical patients carried out
under the direct supervision of a consultant surgeon and consultant anaesthetist
f. Operations on patients with a predicted mortality of >5% where the consultant surgeon and consultant anaesthetist are present for the operation
N Data for ‘d’ were not collected.
An information notice board near to the staff rest room provided some information to the staff, for example, information on Infection Control.
XG-702
Audit
The service should have a rolling programme of audit of compliance with guidelines and protocols [QSs XG-500s] and related outcomes.
N Some audit was undertaken but not against the guidelines and protocols. A ‘Controlled Drugs’ audit was undertaken internally but did not have input from pharmacy.
XG-703
Quality Assurance System The service should have a system to ensure analysis and feedback on the quality of: a. Equipment management (QS XG-402) b. Cleanliness of theatres c. Preparation of clinical areas d. Implementation of WHO Checklist Feedback to individual members of staff should be linked with appraisal and re-validation arrangements.
N The hospital was aware that the ‘WHO’ Safety Checklist was not routinely implemented across all specialities and all grades of staff. From the documentation seen some stages of the WHO checklist were not completed.
Audit of compliance in completing the ‘WHO’ Safety Checklist was being undertaken but did not yet form part of the appraisal process.
XG-704
Monitoring of Key Performance Indicators
Key performance indicators (QS XG-701) should be reviewed regularly with Trust management and with commissioners.
Y The theatre manager had joined the North West Theatre Manager Group and was looking at implementation of performance indicators, for example, SBAR and 6’C’ and a general integrated care plan for all patient groups.
XG-798
Multi-Disciplinary Review and Learning The service should have appropriate multi-disciplinary arrangements for review of, and implementing learning from: a. Positive feedback, complaints, outcomes, incidents and
‘near misses’ b. Published scientific research and guidance relating to
theatre and anaesthetic services
N Multidisciplinary review and learning was not in place. Separate Anaesthetic and Theatre Team meetings did take place. Surgeons were not involved in either meeting.
Staff were linked to other groups such as the Patient Safety & Quality Forum and Professional Development Forum.
XG-799
Document Control
All policies, procedures and guidelines should comply with Trust document control procedures.
N Some documents were not in a standard format and did not have review or implementation dates.
Return to Index
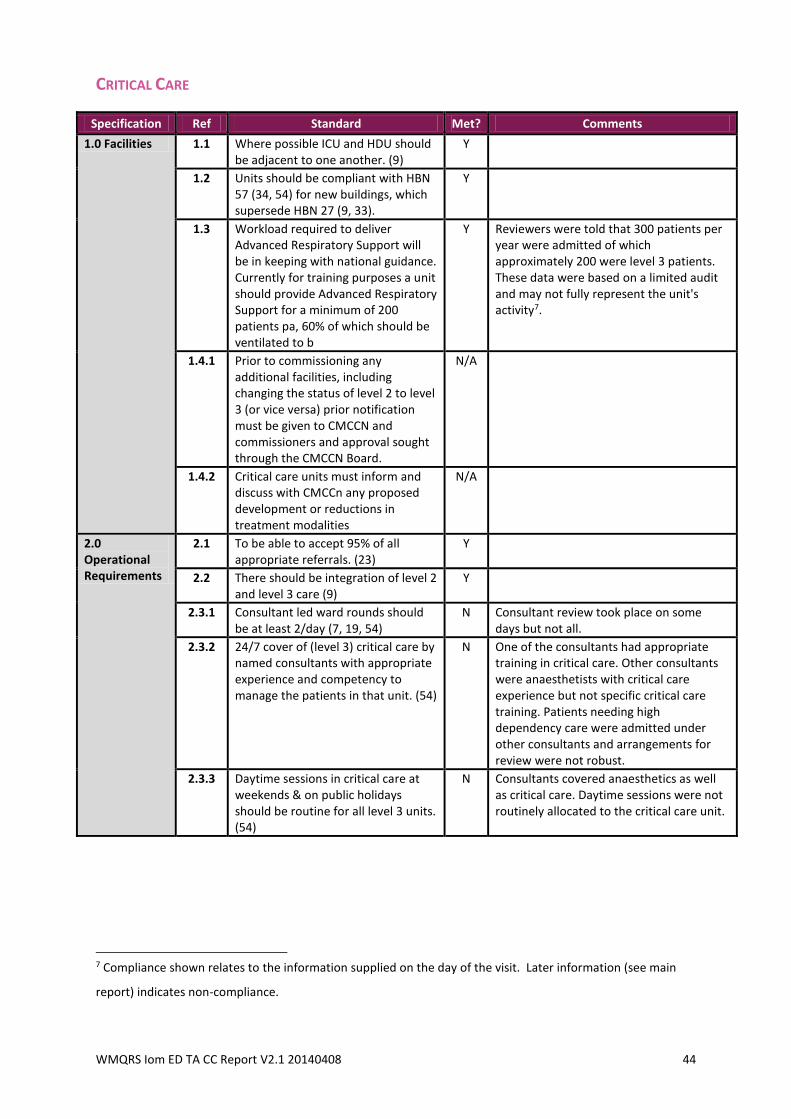
WMQRS Iom ED TA CC Report V2.1 20140408 44
CRITICAL CARE
Specification Ref Standard Met? Comments
1.0 Facilities 1.1 Where possible ICU and HDU should be adjacent to one another. (9)
Y
1.2 Units should be compliant with HBN 57 (34, 54) for new buildings, which supersede HBN 27 (9, 33).
Y
1.3 Workload required to deliver Advanced Respiratory Support will be in keeping with national guidance. Currently for training purposes a unit should provide Advanced Respiratory Support for a minimum of 200 patients pa, 60% of which should be ventilated to b
Y Reviewers were told that 300 patients per year were admitted of which approximately 200 were level 3 patients. These data were based on a limited audit and may not fully represent the unit's activity7.
1.4.1 Prior to commissioning any additional facilities, including changing the status of level 2 to level 3 (or vice versa) prior notification must be given to CMCCN and commissioners and approval sought through the CMCCN Board.
N/A
1.4.2 Critical care units must inform and discuss with CMCCn any proposed development or reductions in treatment modalities
N/A
2.0 Operational Requirements
2.1 To be able to accept 95% of all appropriate referrals. (23)
Y
2.2 There should be integration of level 2 and level 3 care (9)
Y
2.3.1 Consultant led ward rounds should be at least 2/day (7, 19, 54)
N Consultant review took place on some days but not all.
2.3.2 24/7 cover of (level 3) critical care by named consultants with appropriate experience and competency to manage the patients in that unit. (54)
N One of the consultants had appropriate training in critical care. Other consultants were anaesthetists with critical care experience but not specific critical care training. Patients needing high dependency care were admitted under other consultants and arrangements for review were not robust.
2.3.3 Daytime sessions in critical care at weekends & on public holidays should be routine for all level 3 units. (54)
N Consultants covered anaesthetics as well as critical care. Daytime sessions were not routinely allocated to the critical care unit.
7 Compliance shown relates to the information supplied on the day of the visit. Later information (see main
report) indicates non-compliance.
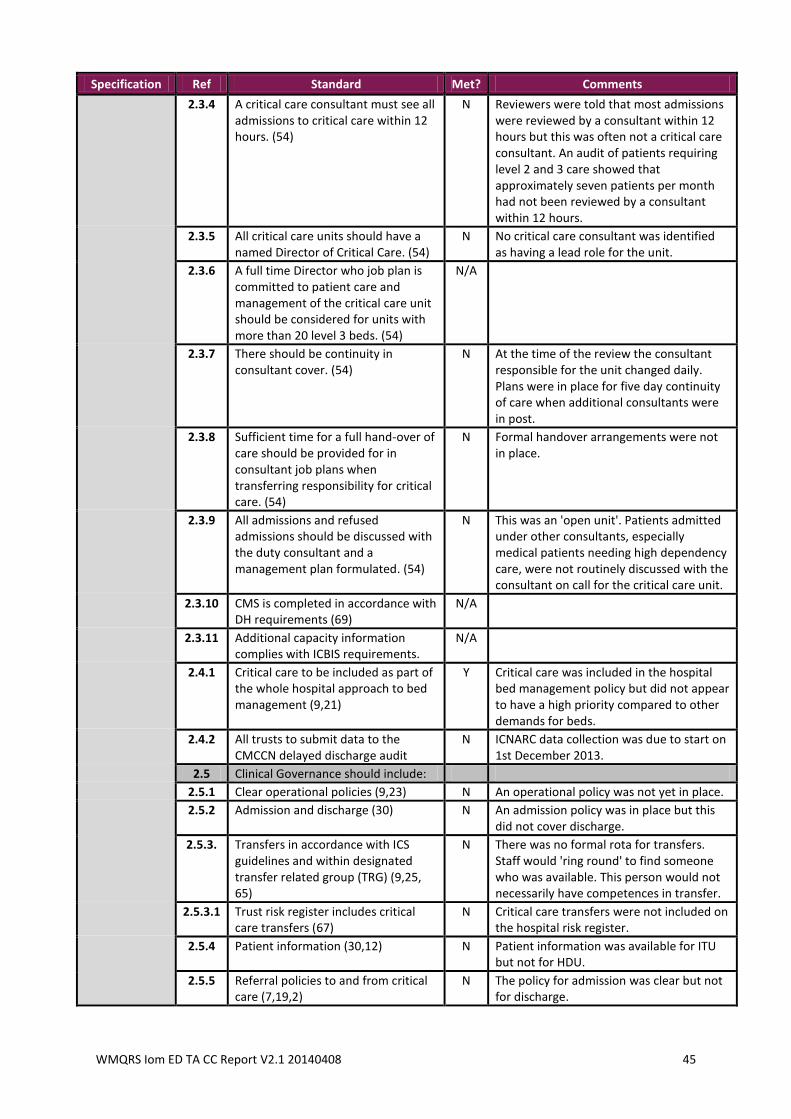
WMQRS Iom ED TA CC Report V2.1 20140408 45
Specification Ref Standard Met? Comments
2.3.4 A critical care consultant must see all admissions to critical care within 12 hours. (54)
N Reviewers were told that most admissions were reviewed by a consultant within 12 hours but this was often not a critical care consultant. An audit of patients requiring level 2 and 3 care showed that approximately seven patients per month had not been reviewed by a consultant within 12 hours.
2.3.5 All critical care units should have a named Director of Critical Care. (54)
N No critical care consultant was identified as having a lead role for the unit.
2.3.6 A full time Director who job plan is committed to patient care and management of the critical care unit should be considered for units with more than 20 level 3 beds. (54)
N/A
2.3.7 There should be continuity in consultant cover. (54)
N At the time of the review the consultant responsible for the unit changed daily. Plans were in place for five day continuity of care when additional consultants were in post.
2.3.8 Sufficient time for a full hand-over of care should be provided for in consultant job plans when transferring responsibility for critical care. (54)
N Formal handover arrangements were not in place.
2.3.9 All admissions and refused admissions should be discussed with the duty consultant and a management plan formulated. (54)
N This was an 'open unit'. Patients admitted under other consultants, especially medical patients needing high dependency care, were not routinely discussed with the consultant on call for the critical care unit.
2.3.10 CMS is completed in accordance with DH requirements (69)
N/A
2.3.11 Additional capacity information complies with ICBIS requirements.
N/A
2.4.1 Critical care to be included as part of the whole hospital approach to bed management (9,21)
Y Critical care was included in the hospital bed management policy but did not appear to have a high priority compared to other demands for beds.
2.4.2 All trusts to submit data to the CMCCN delayed discharge audit
N ICNARC data collection was due to start on 1st December 2013.
2.5 Clinical Governance should include:
2.5.1 Clear operational policies (9,23) N An operational policy was not yet in place.
2.5.2 Admission and discharge (30) N An admission policy was in place but this did not cover discharge.
2.5.3. Transfers in accordance with ICS guidelines and within designated transfer related group (TRG) (9,25, 65)
N There was no formal rota for transfers. Staff would 'ring round' to find someone who was available. This person would not necessarily have competences in transfer.
2.5.3.1 Trust risk register includes critical care transfers (67)
N Critical care transfers were not included on the hospital risk register.
2.5.4 Patient information (30,12) N Patient information was available for ITU but not for HDU.
2.5.5 Referral policies to and from critical care (7,19,2)
N The policy for admission was clear but not for discharge.
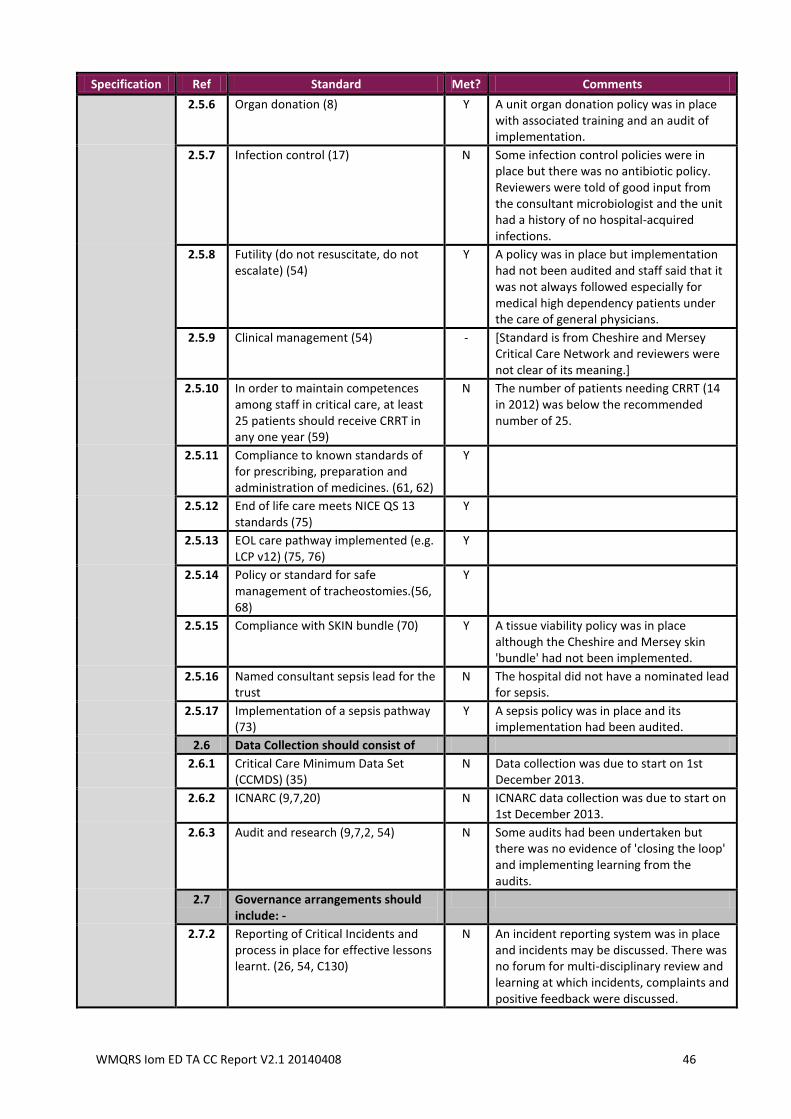
WMQRS Iom ED TA CC Report V2.1 20140408 46
Specification Ref Standard Met? Comments
2.5.6 Organ donation (8) Y A unit organ donation policy was in place with associated training and an audit of implementation.
2.5.7 Infection control (17) N Some infection control policies were in place but there was no antibiotic policy. Reviewers were told of good input from the consultant microbiologist and the unit had a history of no hospital-acquired infections.
2.5.8 Futility (do not resuscitate, do not escalate) (54)
Y A policy was in place but implementation had not been audited and staff said that it was not always followed especially for medical high dependency patients under the care of general physicians.
2.5.9 Clinical management (54) - [Standard is from Cheshire and Mersey Critical Care Network and reviewers were not clear of its meaning.]
2.5.10 In order to maintain competences among staff in critical care, at least 25 patients should receive CRRT in any one year (59)
N The number of patients needing CRRT (14 in 2012) was below the recommended number of 25.
2.5.11 Compliance to known standards of for prescribing, preparation and administration of medicines. (61, 62)
Y
2.5.12 End of life care meets NICE QS 13 standards (75)
Y
2.5.13 EOL care pathway implemented (e.g. LCP v12) (75, 76)
Y
2.5.14 Policy or standard for safe management of tracheostomies.(56, 68)
Y
2.5.15 Compliance with SKIN bundle (70) Y A tissue viability policy was in place although the Cheshire and Mersey skin 'bundle' had not been implemented.
2.5.16 Named consultant sepsis lead for the trust
N The hospital did not have a nominated lead for sepsis.
2.5.17 Implementation of a sepsis pathway (73)
Y A sepsis policy was in place and its implementation had been audited.
2.6 Data Collection should consist of
2.6.1 Critical Care Minimum Data Set (CCMDS) (35)
N Data collection was due to start on 1st December 2013.
2.6.2 ICNARC (9,7,20) N ICNARC data collection was due to start on 1st December 2013.
2.6.3 Audit and research (9,7,2, 54) N Some audits had been undertaken but there was no evidence of 'closing the loop' and implementing learning from the audits.
2.7 Governance arrangements should include: -
2.7.2 Reporting of Critical Incidents and process in place for effective lessons learnt. (26, 54, C130)
N An incident reporting system was in place and incidents may be discussed. There was no forum for multi-disciplinary review and learning at which incidents, complaints and positive feedback were discussed.
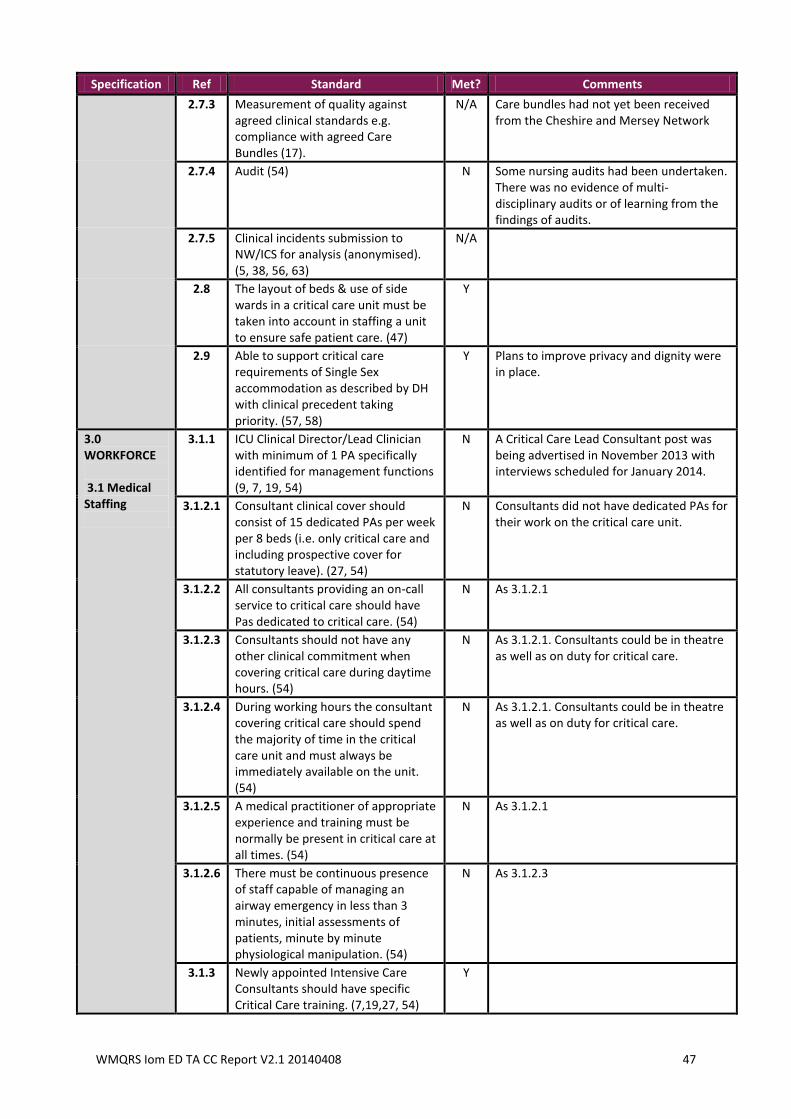
WMQRS Iom ED TA CC Report V2.1 20140408 47
Specification Ref Standard Met? Comments
2.7.3 Measurement of quality against agreed clinical standards e.g. compliance with agreed Care Bundles (17).
N/A Care bundles had not yet been received from the Cheshire and Mersey Network
2.7.4 Audit (54) N Some nursing audits had been undertaken. There was no evidence of multi-disciplinary audits or of learning from the findings of audits.
2.7.5 Clinical incidents submission to NW/ICS for analysis (anonymised). (5, 38, 56, 63)
N/A
2.8 The layout of beds & use of side wards in a critical care unit must be taken into account in staffing a unit to ensure safe patient care. (47)
Y
2.9 Able to support critical care requirements of Single Sex accommodation as described by DH with clinical precedent taking priority. (57, 58)
Y Plans to improve privacy and dignity were in place.
3.0 WORKFORCE 3.1 Medical Staffing
3.1.1 ICU Clinical Director/Lead Clinician with minimum of 1 PA specifically identified for management functions (9, 7, 19, 54)
N A Critical Care Lead Consultant post was being advertised in November 2013 with interviews scheduled for January 2014.
3.1.2.1 Consultant clinical cover should consist of 15 dedicated PAs per week per 8 beds (i.e. only critical care and including prospective cover for statutory leave). (27, 54)
N Consultants did not have dedicated PAs for their work on the critical care unit.
3.1.2.2 All consultants providing an on-call service to critical care should have Pas dedicated to critical care. (54)
N As 3.1.2.1
3.1.2.3 Consultants should not have any other clinical commitment when covering critical care during daytime hours. (54)
N As 3.1.2.1. Consultants could be in theatre as well as on duty for critical care.
3.1.2.4 During working hours the consultant covering critical care should spend the majority of time in the critical care unit and must always be immediately available on the unit. (54)
N As 3.1.2.1. Consultants could be in theatre as well as on duty for critical care.
3.1.2.5 A medical practitioner of appropriate experience and training must be normally be present in critical care at all times. (54)
N As 3.1.2.1
3.1.2.6 There must be continuous presence of staff capable of managing an airway emergency in less than 3 minutes, initial assessments of patients, minute by minute physiological manipulation. (54)
N As 3.1.2.3
3.1.3 Newly appointed Intensive Care Consultants should have specific Critical Care training. (7,19,27, 54)
Y
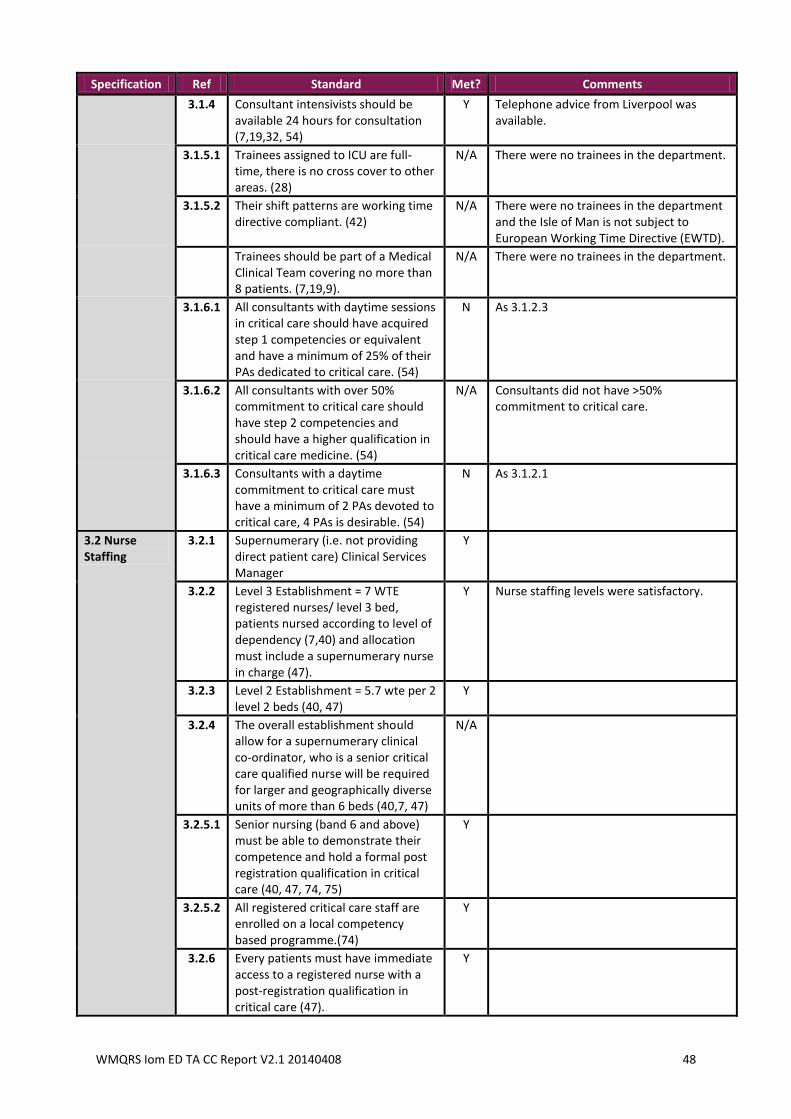
WMQRS Iom ED TA CC Report V2.1 20140408 48
Specification Ref Standard Met? Comments
3.1.4 Consultant intensivists should be available 24 hours for consultation (7,19,32, 54)
Y Telephone advice from Liverpool was available.
3.1.5.1 Trainees assigned to ICU are full-time, there is no cross cover to other areas. (28)
N/A There were no trainees in the department.
3.1.5.2 Their shift patterns are working time directive compliant. (42)
N/A There were no trainees in the department and the Isle of Man is not subject to European Working Time Directive (EWTD).
Trainees should be part of a Medical Clinical Team covering no more than 8 patients. (7,19,9).
N/A There were no trainees in the department.
3.1.6.1 All consultants with daytime sessions in critical care should have acquired step 1 competencies or equivalent and have a minimum of 25% of their PAs dedicated to critical care. (54)
N As 3.1.2.3
3.1.6.2 All consultants with over 50% commitment to critical care should have step 2 competencies and should have a higher qualification in critical care medicine. (54)
N/A Consultants did not have >50% commitment to critical care.
3.1.6.3 Consultants with a daytime commitment to critical care must have a minimum of 2 PAs devoted to critical care, 4 PAs is desirable. (54)
N As 3.1.2.1
3.2 Nurse Staffing
3.2.1 Supernumerary (i.e. not providing direct patient care) Clinical Services Manager
Y
3.2.2 Level 3 Establishment = 7 WTE registered nurses/ level 3 bed, patients nursed according to level of dependency (7,40) and allocation must include a supernumerary nurse in charge (47).
Y Nurse staffing levels were satisfactory.
3.2.3 Level 2 Establishment = 5.7 wte per 2 level 2 beds (40, 47)
Y
3.2.4 The overall establishment should allow for a supernumerary clinical co-ordinator, who is a senior critical care qualified nurse will be required for larger and geographically diverse units of more than 6 beds (40,7, 47)
N/A
3.2.5.1 Senior nursing (band 6 and above) must be able to demonstrate their competence and hold a formal post registration qualification in critical care (40, 47, 74, 75)
Y
3.2.5.2 All registered critical care staff are enrolled on a local competency based programme.(74)
Y
3.2.6 Every patients must have immediate access to a registered nurse with a post-registration qualification in critical care (47).
Y
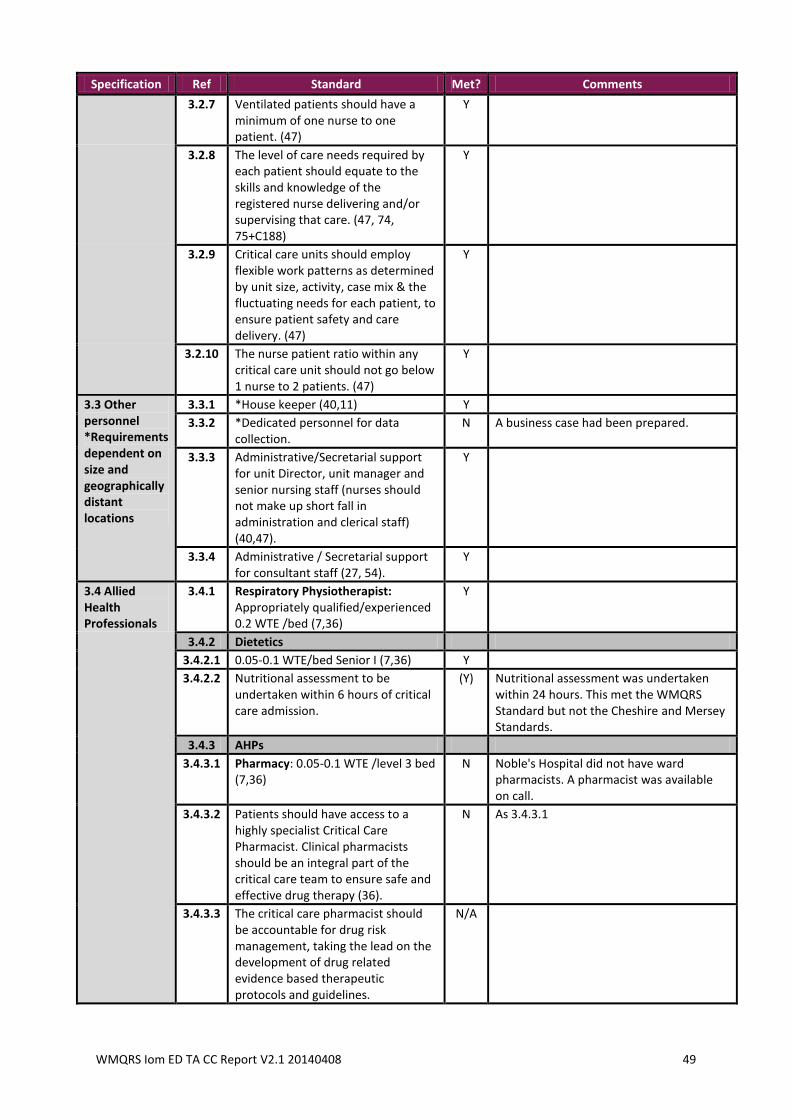
WMQRS Iom ED TA CC Report V2.1 20140408 49
Specification Ref Standard Met? Comments
3.2.7 Ventilated patients should have a minimum of one nurse to one patient. (47)
Y
3.2.8 The level of care needs required by each patient should equate to the skills and knowledge of the registered nurse delivering and/or supervising that care. (47, 74, 75+C188)
Y
3.2.9 Critical care units should employ flexible work patterns as determined by unit size, activity, case mix & the fluctuating needs for each patient, to ensure patient safety and care delivery. (47)
Y
3.2.10 The nurse patient ratio within any critical care unit should not go below 1 nurse to 2 patients. (47)
Y
3.3 Other personnel *Requirements dependent on size and geographically distant locations
3.3.1 *House keeper (40,11) Y
3.3.2 *Dedicated personnel for data collection.
N A business case had been prepared.
3.3.3 Administrative/Secretarial support for unit Director, unit manager and senior nursing staff (nurses should not make up short fall in administration and clerical staff) (40,47).
Y
3.3.4 Administrative / Secretarial support for consultant staff (27, 54).
Y
3.4 Allied Health Professionals
3.4.1 Respiratory Physiotherapist: Appropriately qualified/experienced 0.2 WTE /bed (7,36)
Y
3.4.2 Dietetics
3.4.2.1 0.05-0.1 WTE/bed Senior I (7,36) Y
3.4.2.2 Nutritional assessment to be undertaken within 6 hours of critical care admission.
(Y) Nutritional assessment was undertaken within 24 hours. This met the WMQRS Standard but not the Cheshire and Mersey Standards.
3.4.3 AHPs
3.4.3.1 Pharmacy: 0.05-0.1 WTE /level 3 bed (7,36)
N Noble's Hospital did not have ward pharmacists. A pharmacist was available on call.
3.4.3.2 Patients should have access to a highly specialist Critical Care Pharmacist. Clinical pharmacists should be an integral part of the critical care team to ensure safe and effective drug therapy (36).
N As 3.4.3.1
3.4.3.3 The critical care pharmacist should be accountable for drug risk management, taking the lead on the development of drug related evidence based therapeutic protocols and guidelines.
N/A
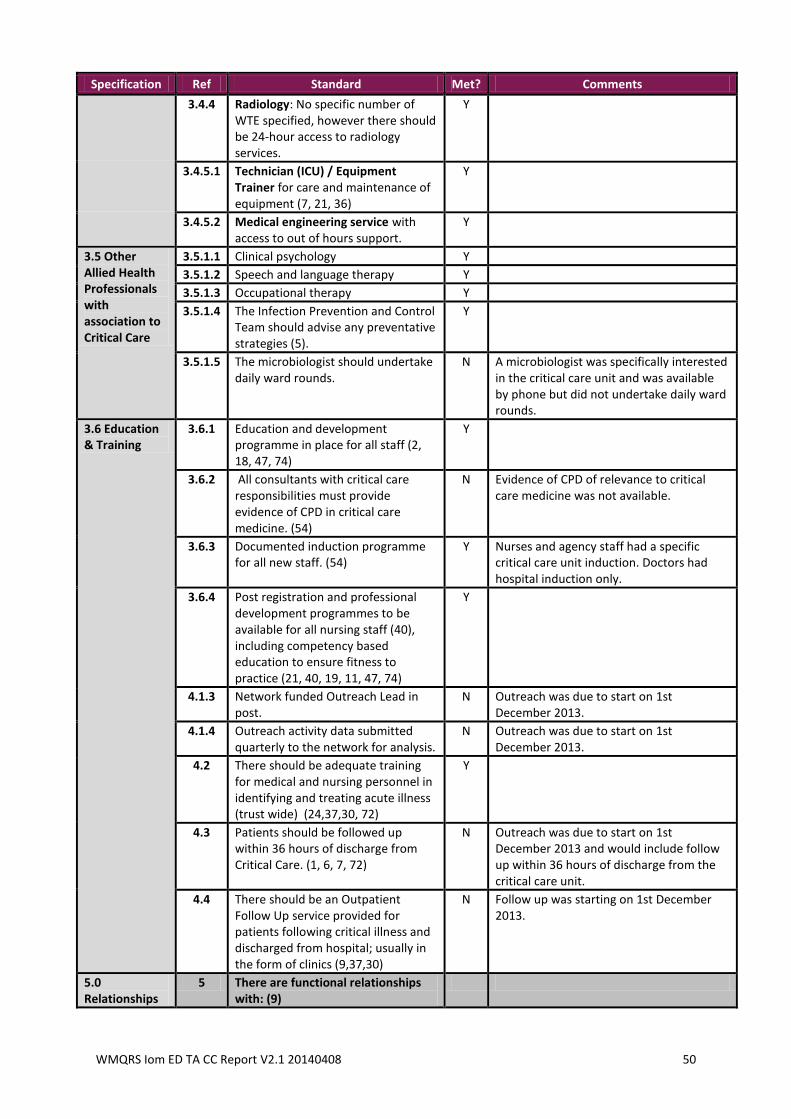
WMQRS Iom ED TA CC Report V2.1 20140408 50
Specification Ref Standard Met? Comments
3.4.4 Radiology: No specific number of WTE specified, however there should be 24-hour access to radiology services.
Y
3.4.5.1 Technician (ICU) / Equipment Trainer for care and maintenance of equipment (7, 21, 36)
Y
3.4.5.2 Medical engineering service with access to out of hours support.
Y
3.5 Other Allied Health Professionals with association to Critical Care
3.5.1.1 Clinical psychology Y
3.5.1.2 Speech and language therapy Y
3.5.1.3 Occupational therapy Y
3.5.1.4 The Infection Prevention and Control Team should advise any preventative strategies (5).
Y
3.5.1.5 The microbiologist should undertake daily ward rounds.
N A microbiologist was specifically interested in the critical care unit and was available by phone but did not undertake daily ward rounds.
3.6 Education & Training
3.6.1 Education and development programme in place for all staff (2, 18, 47, 74)
Y
3.6.2 All consultants with critical care responsibilities must provide evidence of CPD in critical care medicine. (54)
N Evidence of CPD of relevance to critical care medicine was not available.
3.6.3 Documented induction programme for all new staff. (54)
Y Nurses and agency staff had a specific critical care unit induction. Doctors had hospital induction only.
3.6.4 Post registration and professional development programmes to be available for all nursing staff (40), including competency based education to ensure fitness to practice (21, 40, 19, 11, 47, 74)
Y
4.1.3 Network funded Outreach Lead in post.
N Outreach was due to start on 1st December 2013.
4.1.4 Outreach activity data submitted quarterly to the network for analysis.
N Outreach was due to start on 1st December 2013.
4.2 There should be adequate training for medical and nursing personnel in identifying and treating acute illness (trust wide) (24,37,30, 72)
Y
4.3 Patients should be followed up within 36 hours of discharge from Critical Care. (1, 6, 7, 72)
N Outreach was due to start on 1st December 2013 and would include follow up within 36 hours of discharge from the critical care unit.
4.4 There should be an Outpatient Follow Up service provided for patients following critical illness and discharged from hospital; usually in the form of clinics (9,37,30)
N Follow up was starting on 1st December 2013.
5.0 Relationships
5 There are functional relationships with: (9)
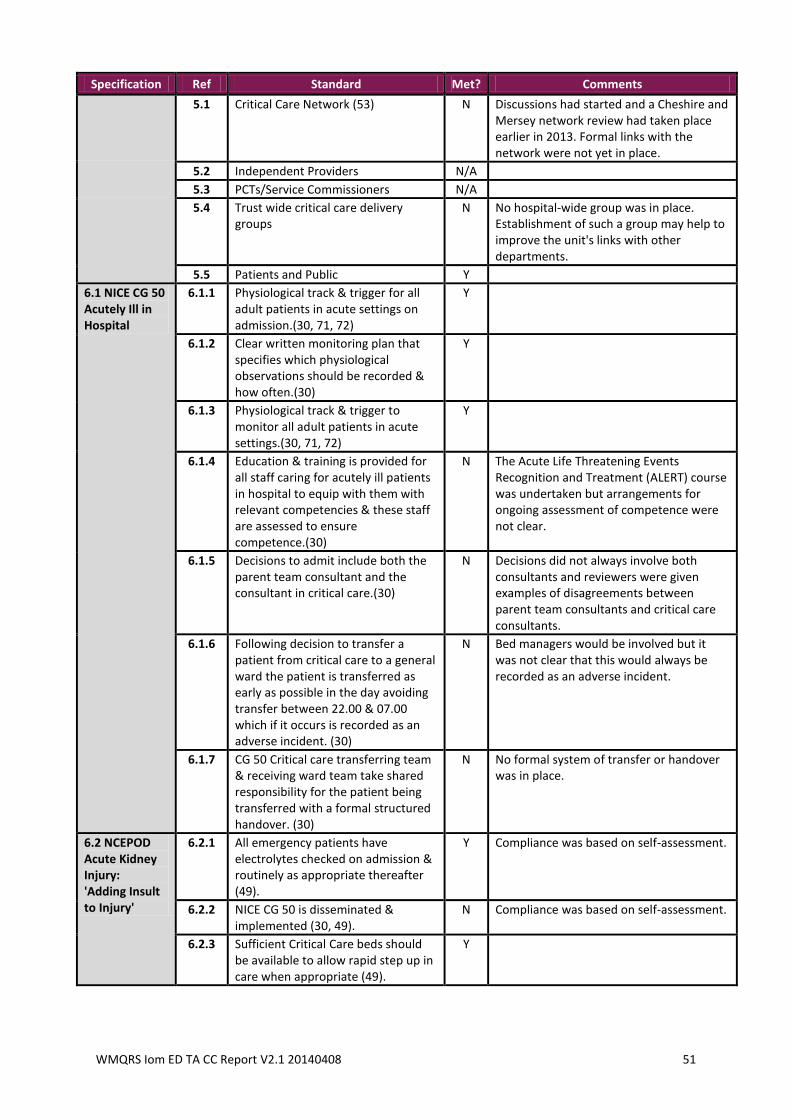
WMQRS Iom ED TA CC Report V2.1 20140408 51
Specification Ref Standard Met? Comments
5.1 Critical Care Network (53) N Discussions had started and a Cheshire and Mersey network review had taken place earlier in 2013. Formal links with the network were not yet in place.
5.2 Independent Providers N/A
5.3 PCTs/Service Commissioners N/A
5.4 Trust wide critical care delivery groups
N No hospital-wide group was in place. Establishment of such a group may help to improve the unit's links with other departments.
5.5 Patients and Public Y
6.1 NICE CG 50 Acutely Ill in Hospital
6.1.1 Physiological track & trigger for all adult patients in acute settings on admission.(30, 71, 72)
Y
6.1.2 Clear written monitoring plan that specifies which physiological observations should be recorded & how often.(30)
Y
6.1.3 Physiological track & trigger to monitor all adult patients in acute settings.(30, 71, 72)
Y
6.1.4 Education & training is provided for all staff caring for acutely ill patients in hospital to equip with them with relevant competencies & these staff are assessed to ensure competence.(30)
N The Acute Life Threatening Events Recognition and Treatment (ALERT) course was undertaken but arrangements for ongoing assessment of competence were not clear.
6.1.5 Decisions to admit include both the parent team consultant and the consultant in critical care.(30)
N Decisions did not always involve both consultants and reviewers were given examples of disagreements between parent team consultants and critical care consultants.
6.1.6 Following decision to transfer a patient from critical care to a general ward the patient is transferred as early as possible in the day avoiding transfer between 22.00 & 07.00 which if it occurs is recorded as an adverse incident. (30)
N Bed managers would be involved but it was not clear that this would always be recorded as an adverse incident.
6.1.7 CG 50 Critical care transferring team & receiving ward team take shared responsibility for the patient being transferred with a formal structured handover. (30)
N No formal system of transfer or handover was in place.
6.2 NCEPOD Acute Kidney Injury: 'Adding Insult to Injury'
6.2.1 All emergency patients have electrolytes checked on admission & routinely as appropriate thereafter (49).
Y Compliance was based on self-assessment.
6.2.2 NICE CG 50 is disseminated & implemented (30, 49).
N Compliance was based on self-assessment.
6.2.3 Sufficient Critical Care beds should be available to allow rapid step up in care when appropriate (49).
Y
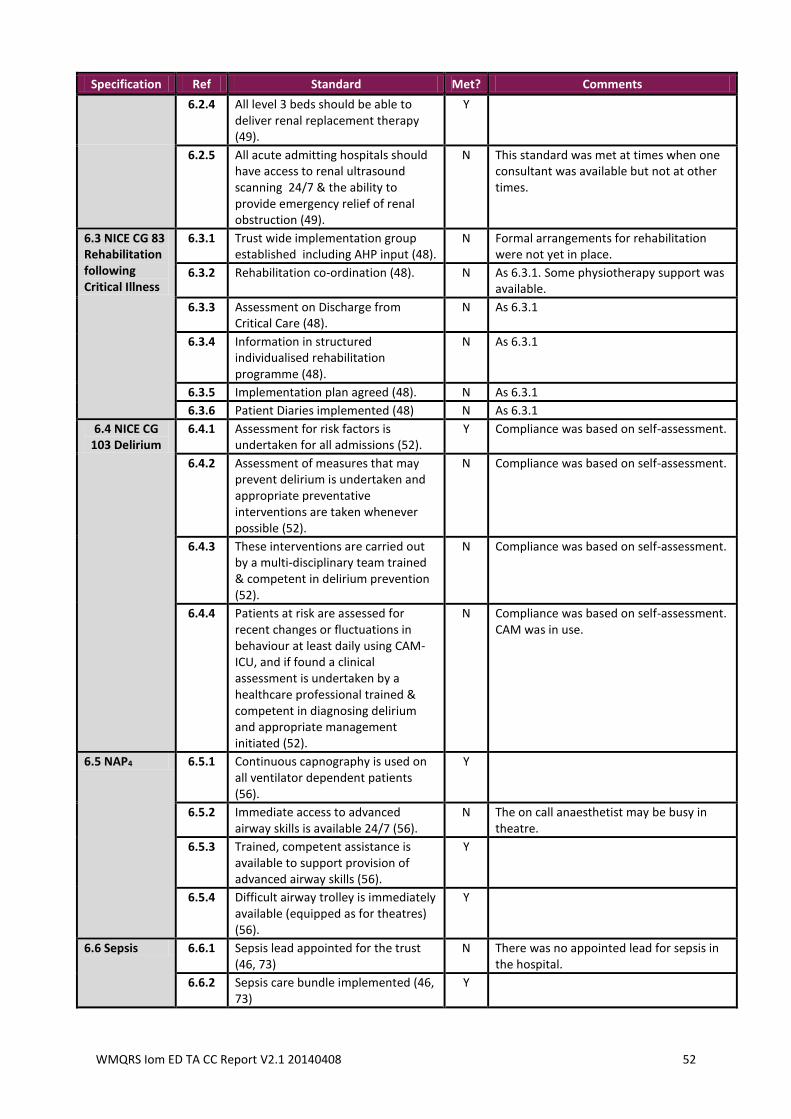
WMQRS Iom ED TA CC Report V2.1 20140408 52
Specification Ref Standard Met? Comments
6.2.4 All level 3 beds should be able to deliver renal replacement therapy (49).
Y
6.2.5 All acute admitting hospitals should have access to renal ultrasound scanning 24/7 & the ability to provide emergency relief of renal obstruction (49).
N This standard was met at times when one consultant was available but not at other times.
6.3 NICE CG 83 Rehabilitation following Critical Illness
6.3.1 Trust wide implementation group established including AHP input (48).
N Formal arrangements for rehabilitation were not yet in place.
6.3.2 Rehabilitation co-ordination (48). N As 6.3.1. Some physiotherapy support was available.
6.3.3 Assessment on Discharge from Critical Care (48).
N As 6.3.1
6.3.4 Information in structured individualised rehabilitation programme (48).
N As 6.3.1
6.3.5 Implementation plan agreed (48). N As 6.3.1
6.3.6 Patient Diaries implemented (48) N As 6.3.1
6.4 NICE CG 103 Delirium
6.4.1 Assessment for risk factors is undertaken for all admissions (52).
Y Compliance was based on self-assessment.
6.4.2 Assessment of measures that may prevent delirium is undertaken and appropriate preventative interventions are taken whenever possible (52).
N Compliance was based on self-assessment.
6.4.3 These interventions are carried out by a multi-disciplinary team trained & competent in delirium prevention (52).
N Compliance was based on self-assessment.
6.4.4 Patients at risk are assessed for recent changes or fluctuations in behaviour at least daily using CAM-ICU, and if found a clinical assessment is undertaken by a healthcare professional trained & competent in diagnosing delirium and appropriate management initiated (52).
N Compliance was based on self-assessment. CAM was in use.
6.5 NAP4 6.5.1 Continuous capnography is used on all ventilator dependent patients (56).
Y
6.5.2 Immediate access to advanced airway skills is available 24/7 (56).
N The on call anaesthetist may be busy in theatre.
6.5.3 Trained, competent assistance is available to support provision of advanced airway skills (56).
Y
6.5.4 Difficult airway trolley is immediately available (equipped as for theatres) (56).
Y
6.6 Sepsis 6.6.1 Sepsis lead appointed for the trust (46, 73)
N There was no appointed lead for sepsis in the hospital.
6.6.2 Sepsis care bundle implemented (46, 73)
Y
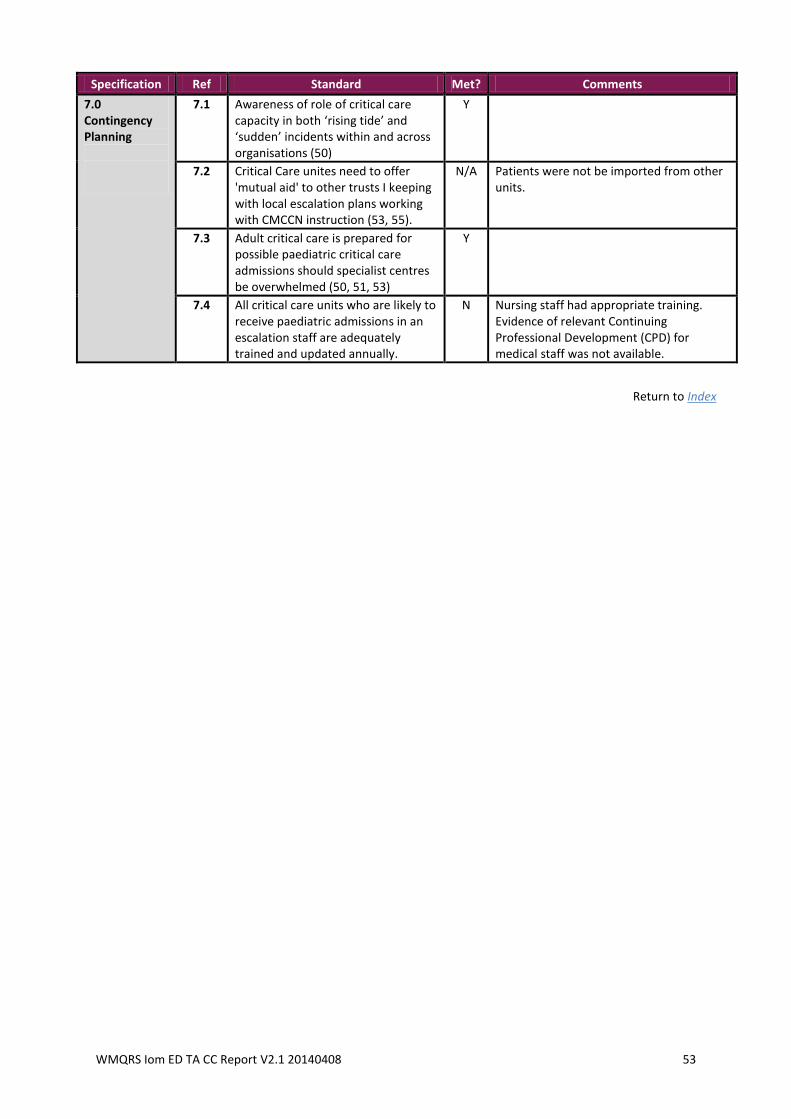
WMQRS Iom ED TA CC Report V2.1 20140408 53
Specification Ref Standard Met? Comments
7.0 Contingency Planning
7.1 Awareness of role of critical care capacity in both ‘rising tide’ and ‘sudden’ incidents within and across organisations (50)
Y
7.2 Critical Care unites need to offer 'mutual aid' to other trusts I keeping with local escalation plans working with CMCCN instruction (53, 55).
N/A Patients were not be imported from other units.
7.3 Adult critical care is prepared for possible paediatric critical care admissions should specialist centres be overwhelmed (50, 51, 53)
Y
7.4 All critical care units who are likely to receive paediatric admissions in an escalation staff are adequately trained and updated annually.
N Nursing staff had appropriate training. Evidence of relevant Continuing Professional Development (CPD) for medical staff was not available.
Return to Index



















![20140408 digital newspapers collections [idlc kuala lumpur]](https://img.pdfslide.net/doc/110x75/53fea18e8d7f72835c8b4595/20140408-digital-newspapers-collections-idlc-kuala-lumpur.jpg)


![20140408 toetsing protocol begeleiding [samen voor elkaar]](https://img.pdfslide.net/doc/110x75/54974d9fb47959794d8b51ff/20140408-toetsing-protocol-begeleiding-samen-voor-elkaar.jpg)






