Embed Size (px)
Citation preview

Working together - a healthy partnershipKnox Improving
Chronic Care Project
The preparations required to implement an
effective chronic disease program
Kate Gilbert, Chronic Disease Project Manager

Knox Community Health Service
Working together - a healthy partnership
The Early Intervention in Chronic Disease Initiative

Working together - a healthy partnership
• Local systems and organisational development
– links with GPs (referral systems, care planning, team care arrangements)– internal: assessment tools, referral processes, prioritisation, self-management training– support neighbouring CHSs
• Service delivery– new clinical areas to respond to community – ‘key workers’/named contacts– self-management interventions/groups– psychosocial / psychology
• $400,000 per year recurrent + $167,000 establishment
Scope of EIiCD

Knox Community Health Service
Working together - a healthy partnership
Identifying target groups and priorities

Knox Community Health Service
Working together - a healthy partnership
Consultation Timeline
NOVEMBER
4 x Consumer Focus Groups Facilitated by Chronic Illness Alliance
DECEMBER
OCTOBER
Collect Data – Prevalence
Key Stakeholders’
Forum
GP Phone Interviews
Preliminary consultation local consumer groups
Convene Internal Reference Group
Internal Chronic Disease
Screening Exercise
Dental Service Chronic Disease Audit
Internal Client Sat.
Survey
Implem. Planning
Pres. to DHS
Client-specificInternalGPs and other external stakeholders
Implem-entation
Plan to DHS
Mapping self-management interventions
Consumer Focus Groups continued

Knox Community Health Service
Working together - a healthy partnership
• PHIDU - Population health profiles by Division of GP: www.publichealth.gov.au
• Department of Human Services (2006). Ambulatory Care sensitive conditions 2004-05 update – by Region.
• Burden of Disease - Disability Adjusted Life Years: http://www.aihw.gov.au/cdarf/index.cfm
• HARP – Local hospital admission data• Local Council, Social Researcher

Knox Community Health Service
Working together - a healthy partnership
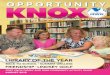
Number of people in Knox (estimated)
Reference: PHIDU. (2005) Population health profile of the Knox Division of General
Practice. Population Profile Series: No. 50. Public Health Information Development Unit (PHIDU), Adelaide.
0
10,000
20,000
30,000
40,000
50,000
CO
PD
an
d o
the
rch
ron
icre
spira
tory
(e
xa
sth
ma
)
Ch
ron
ic A
sth
ma
Oth
er
Ch
ron
icm
usc
ulo
ske
leta
l(e
x a
rth
ritis
)
Ch
ron
ic a
rth
ritis
He
art
failu
re a
nd
oth
er
CV
dis
ea
se (
exc
.Is
cha
em
ic &
stro
ke)
Dia
be
tes

Knox Community Health Service
Working together - a healthy partnership
SummaryMeasure Highest in Knox Higher than
comparison populations
Estimated number of people living with each chronic disease, 2001
• COPD & other Chronic Respiratory (exc. Asthma)
• COPD & other Chronic Respiratory (inc. Asthma)
Disability Adjusted Life Years (DALYs), 2001
• Cardiovascular Disease (inc. ischaemic & stroke)
All comparable
Premature mortality, 2000-02
• Heart failure and other CVD (exc. ischaemic & stroke)
• Diabetes• Respiratory diseases
Preventable Hospital admissions, 2004-05
• Diabetes • Cellulitis
Emergency department admissions, 2005-06
• Asthma State-wide data for 2005-06 not yet available

Knox Community Health Service
Working together - a healthy partnership
Chronic Disease in Knox
• Chronic Respiratory Diseases (COPD etc) - most prevalent chronic condition in Knox, even when asthma not counted
• Chronic Respiratory Diseases and Asthma - prevalence is >10% above Australian average rate in north of Knox, and 5-10% above in south Knox
When comparing chronic diseases:• Cardiovascular disease - greatest contributor
to premature mortality and DALYs • Diabetes - leading cause of preventable hospital
admissions (Ambulatory Care Sensitive Admissions Study)
• Asthma highest cause of ED admissions in Knox

Knox Community Health Service
Working together - a healthy partnership
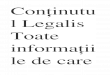
One Day Snapshot Dental Clients
Which chronic conditions did the clients have?
Blood pressure,
27%
Arthritis, 26%Heart
disease, 15%
Diabetes, 9%
Stroke, 9%
Asthma, 2%
Brain tumours, 2%
Fits, 2%Hep C, 2%

Knox Community Health Service
Working together - a healthy partnership
1 week – 252 clients, 95 with chronic disease
Asthma, 33%
Blood pressure,
31%
Heart disease,
26%
Diabetes, 17%
Arthritis, 33%
Stroke, 9%
Emphysema, 3%
Epilepsy/Fits, 4%
Hep B, 1%Parkinsons,
1%Hep C, 6%

Knox Community Health Service
Working together - a healthy partnership
Is there anything we can do in …. arthritis?

Knox Community Health Service
Working together - a healthy partnershipKnox – Target Groups
1. Respiratory Disease > Newly-diagnosed COPD
2. Diabetes> Type 2 diabetes Insulin Initiation
3. Musculoskeletal > Osteoarthritis Pathway
4. Heart Disease > Cardiac Rehabilitation

Knox Community Health Service
Working together - a healthy partnership
Further findings – after target
groups determined

Knox Community Health Service
Working together - a healthy partnership
Overview of Knox population
Mapping self-management interventions in the Outer East

Knox Community Health Service
Working together - a healthy partnershipNature
• Generic/Evidence-based/Stanford model/ Better Health Self-Management – 2
• Disease-specific:– MSK – 8– Cardiac – 5– Pulmonary rehabilitation – 3– Diabetes education – 5– Cancer – 2– Multiple sclerosis – 1– Weight loss – 2

Knox Community Health Service
Working together - a healthy partnership

Knox Community Health Service
Working together - a healthy partnership
KCHS Screening Exercise November 2006
Dental File Audit November 2006
PHIDU Population Estimates for Knox
Arthritis 57% 33% 16,160
Heart disease 26% 26% 20,137
Type 2 Diabetes 25% 17% 2,468
Asthma 21% 33% 18,396
Stroke 7% 9%
Lung/Respiratory
5 % 3% 29,078
Type 1 Diabetes 3% 840

Knox Community Health Service
Working together - a healthy partnershipConsumer involvement
• Focus Groups – CIA• Client Satisfaction Survey – piggy back• Reference Group – consumer reps
Community resources and linkages:• Informal – local support groups• Establishing partnership arrangements• Delegated ‘Community expert’ on staff• Pathways – ongoing support

Working together - a healthy partnership
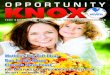
Cardiac RehabPhase 3
Newly-diagnosed COPD
Type 2 DiabetesInsulin Initiation
OsteoarthritisHip or Knee
Spirometry services / GPsAngliss Rehab , HARP
GPs (existing referral stream)
KCHS Case-finding and internal referral
Angliss Hospital and GPs(existing referrals)
KCHS INTAKE: 1. SCTT 2. CDM introduction 3. Key Worker identification
Assessment: inc. Partners in Health Scale, Baseline Evaluation
Allocate to Key worker
Individualised Care Plan:Flinders Goal Setting & Evidence Based Pathways
Follow-up: Telephone coaching or individual consults
Individual servicesDental, Physio, OT, Podiatry,
Psychology, CounsellingDiabetes Ed
Community linkagesPhysical Activity, Socialisation support,
Lifestyle management, Psychosocial support, Self-help groups
Group programsStanford course, Pulmonary rehab, DAFNE
Diabetes education, Falls prevention, Tai-Chi for arthritis, CVD Phase 3, etc.
Psychologist case reviewand treat directly or extra support to key worker
Mental health condition identified
Scheduled Recall and Review & 6-monthly evaluation surveys
GP: Intro & Clinical data for
evaluation
GP: Detail Care Plan
Patient-held record
GP: Revisions to Care
Plan or 6 months
Tar
get G
roup
s &
Ref
erra
l Sou
rces
1s
YE
AR EI Referrals to HARP
Eastern HARP ACCESS
Review assessments already completed to avoid duplication Assume
existing clients already had SCTT etc