Embed Size (px)
Citation preview
Zdravila , ki vplivajo na nastajanje trombov
Lovro Stanovnik
Možnosti vpliva na nastajanje trombusa
• Vpliv na koagulacijo krvi (tvorba fibrina)
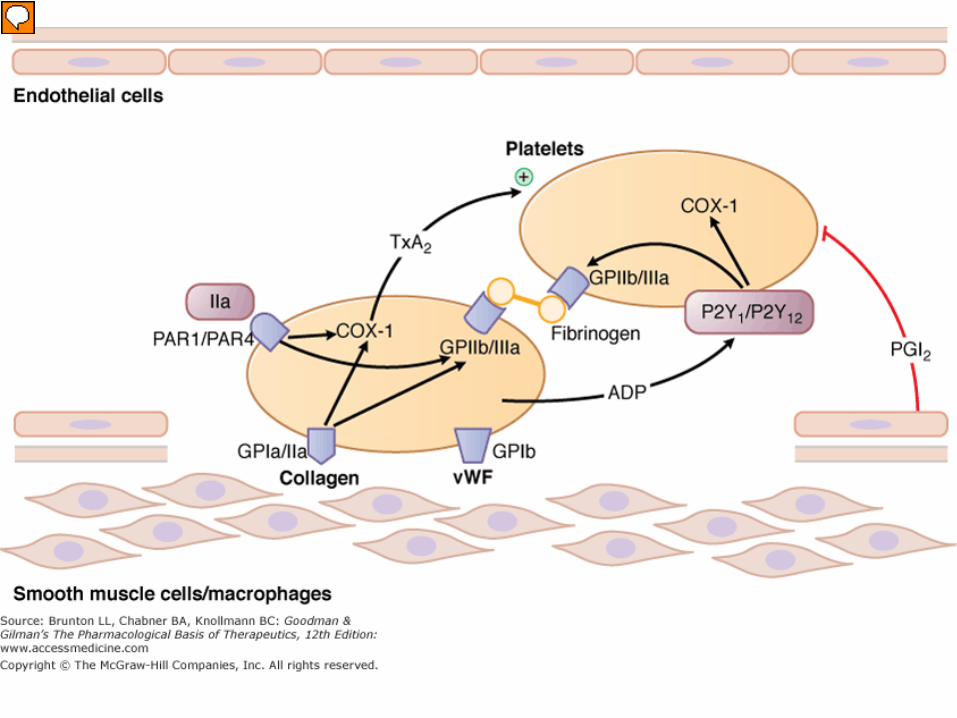
• Vpliv na delovanje trombocitov
• Odstranjevanje fibrina (fibrinoliza).
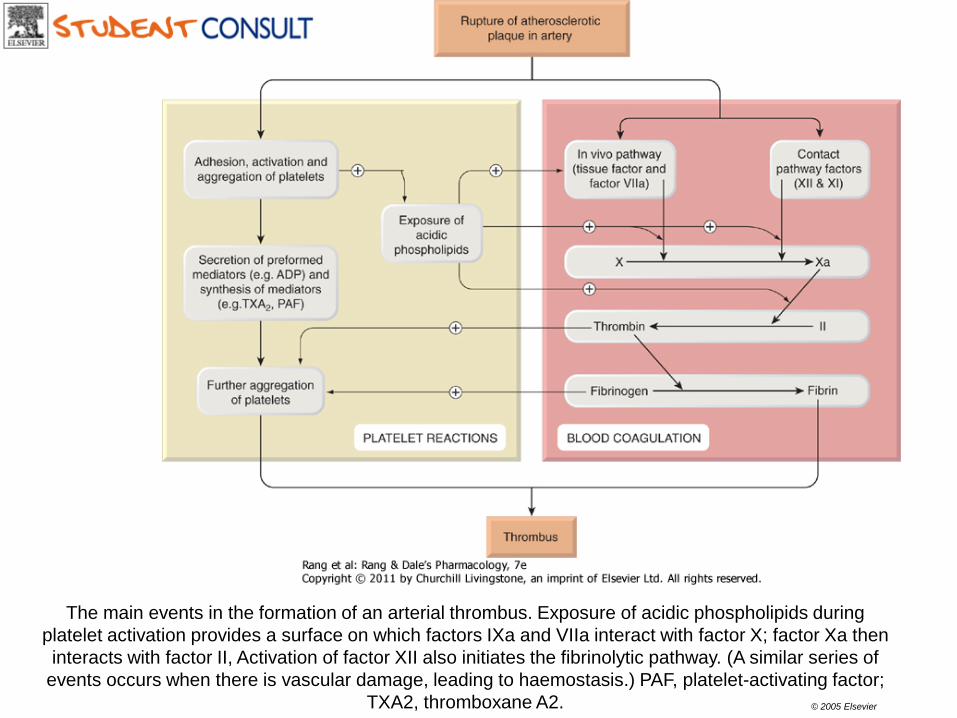
The main events in the formation of an arterial thrombus. Exposure of acidic phospholipids during platelet activation provides a surface on which factors IXa and VIIa interact with factor X; factor Xa then interacts with factor II, Activation of factor XII also initiates the fibrinolytic pathway. (A similar series of
events occurs when there is vascular damage, leading to haemostasis.) PAF, platelet-activating factor; TXA2, thromboxane A2. © 2005 Elsevier
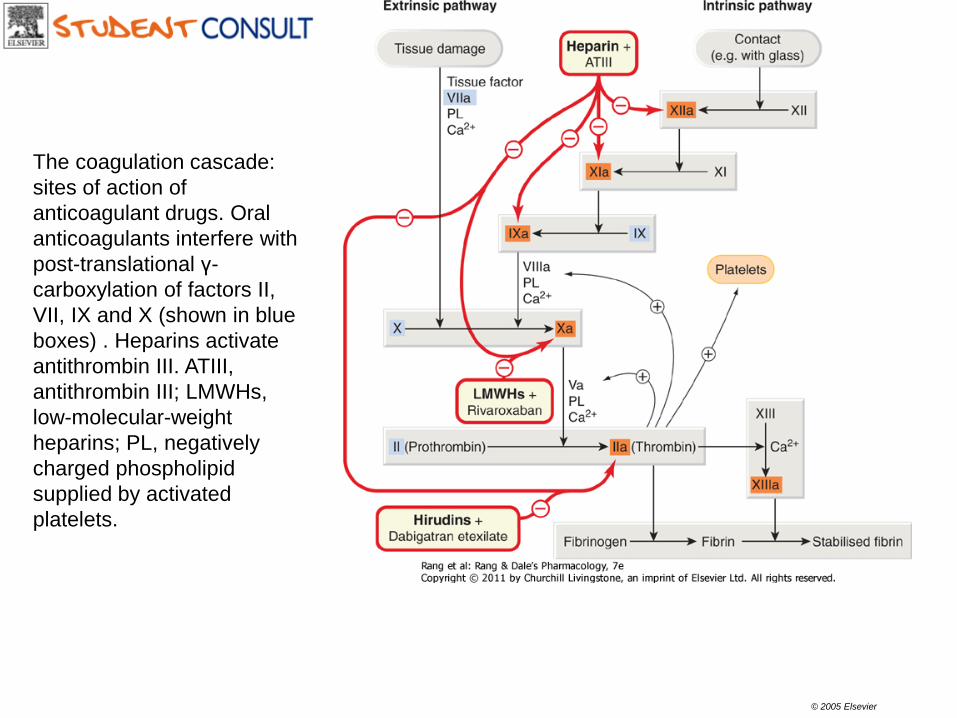
The coagulation cascade: sites of action of anticoagulant drugs. Oral anticoagulants interfere with post-translational γ-carboxylation of factors II, VII, IX and X (shown in blue boxes) . Heparins activate antithrombin III. ATIII, antithrombin III; LMWHs, low-molecular-weight heparins; PL, negatively charged phospholipid supplied by activated platelets.
© 2005 Elsevier
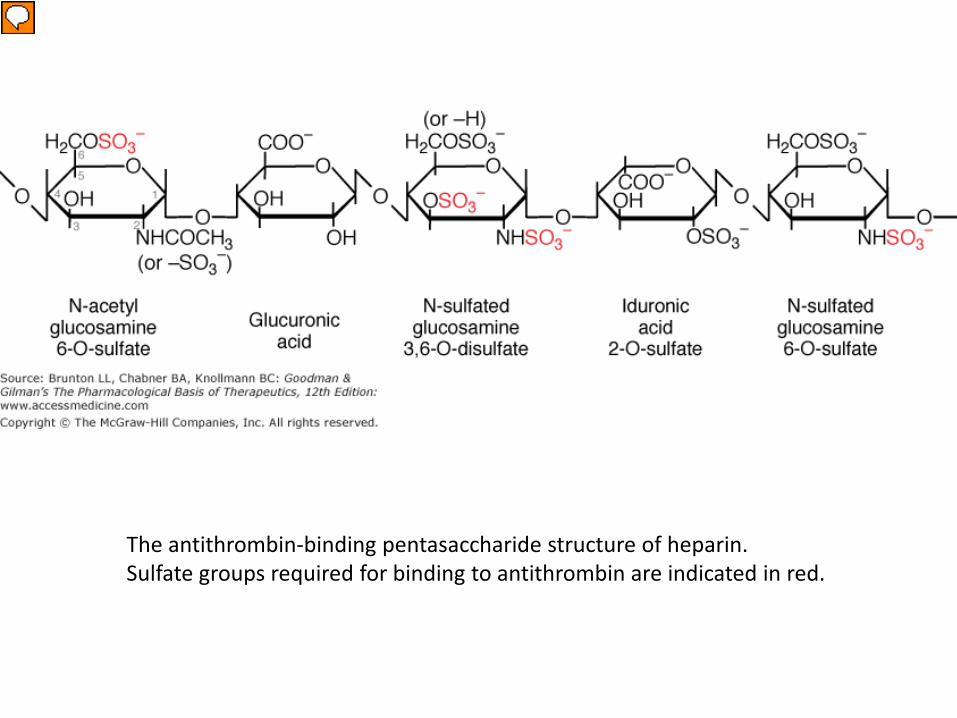
The antithrombin-binding pentasaccharide structure of heparin. Sulfate groups required for binding to antithrombin are indicated in red.
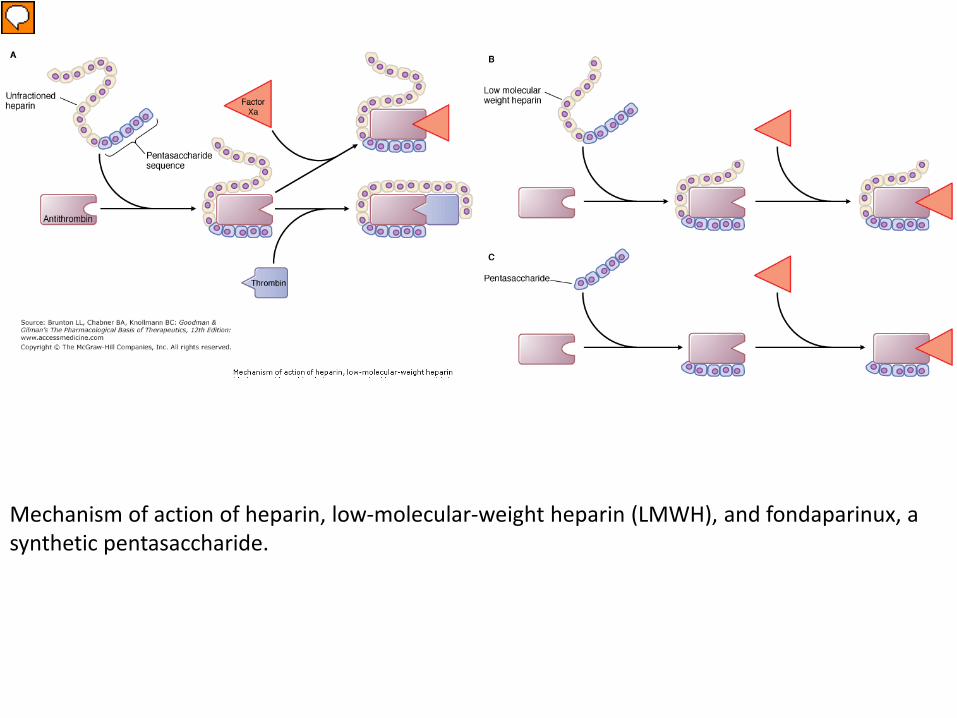
Mechanism of action of heparin, low-molecular-weight heparin (LMWH), and fondaparinux, a synthetic pentasaccharide.
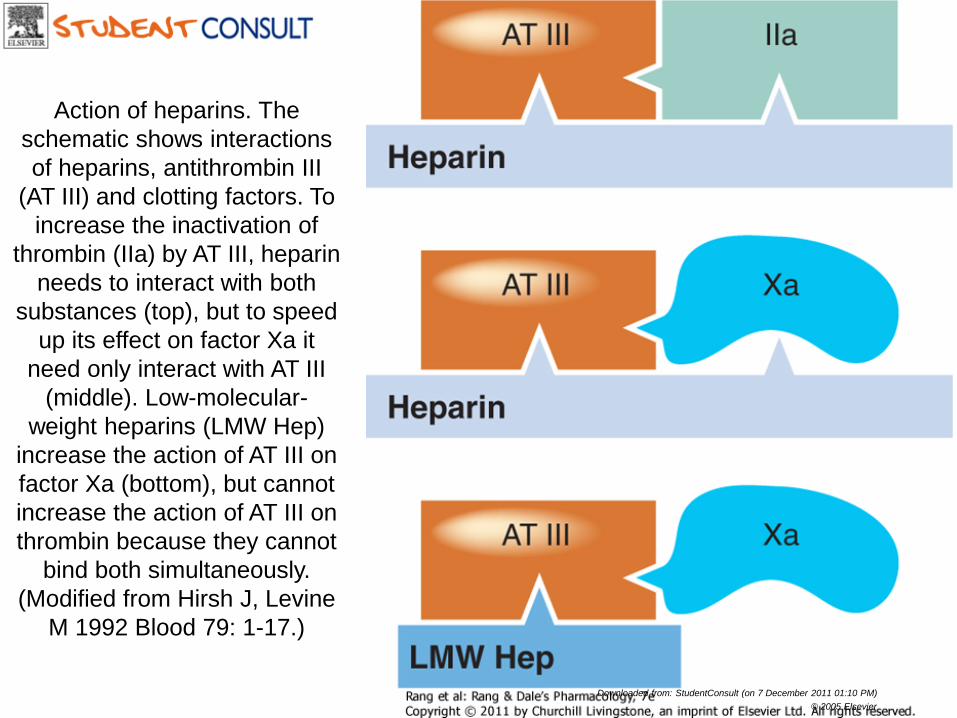
Action of heparins. The schematic shows interactions of heparins, antithrombin III
(AT III) and clotting factors. To increase the inactivation of
thrombin (IIa) by AT III, heparin needs to interact with both
substances (top), but to speed up its effect on factor Xa it
need only interact with AT III (middle). Low-molecular-
weight heparins (LMW Hep) increase the action of AT III on factor Xa (bottom), but cannot increase the action of AT III on thrombin because they cannot
bind both simultaneously. (Modified from Hirsh J, Levine
M 1992 Blood 79: 1-17.)
Downloaded from: StudentConsult (on 7 December 2011 01:10 PM) © 2005 Elsevier
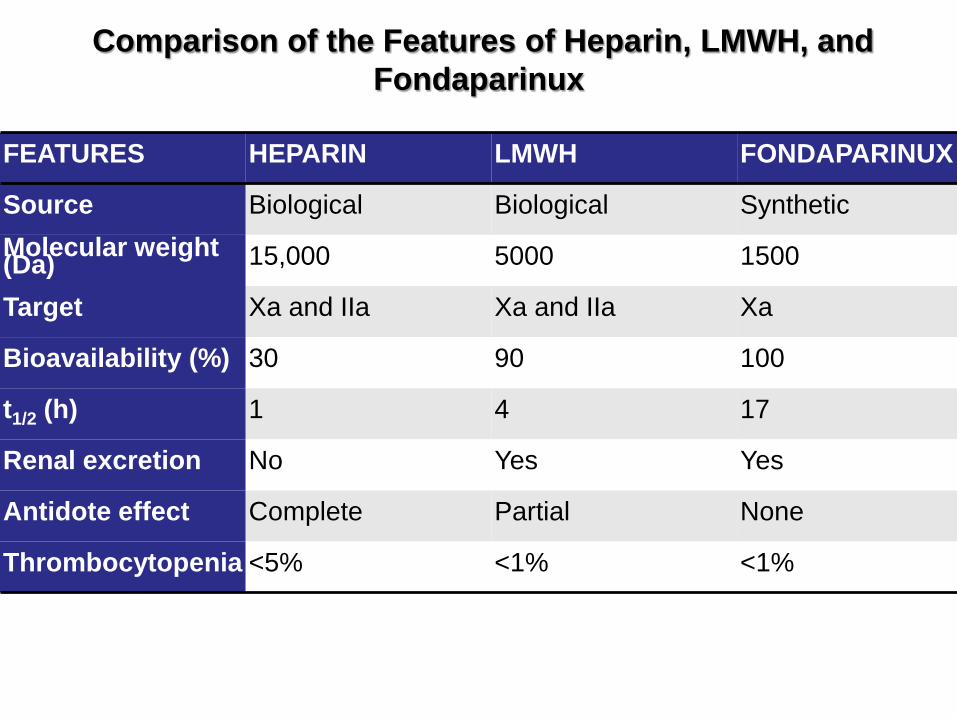
Comparison of the Features of Heparin, LMWH, and Fondaparinux
FEATURES HEPARIN LMWH FONDAPARINUX
Source Biological Biological Synthetic
Molecular weight (Da) 15,000 5000 1500
Target Xa and IIa Xa and IIa Xa
Bioavailability (%) 30 90 100
t1/2 (h) 1 4 17
Renal excretion No Yes Yes
Antidote effect Complete Partial None
Thrombocytopenia <5% <1% <1%
Varfarin • Oralni antikumarinski derivat • Inhibira podenoto C1 vitamin K epoksidne reduktaze
(VKORC1) • Prepreči sintezo koagulacijskih faktorjev, ki so odvisni od
vitamina K (faktorji II, VII, IX in X) in sintezo antikoagulantnih proteinov C in S.
• V visokem deležu se veže na plazemske beljakovine (cca 97%) – interakcije!
• Stereoselektivno se metabolizira s citohromi P-450 (CYP) v inaktivne hidroksilirane metabolite
• Pri metabolizmu varfarina so udeleženi naslednji CYP: 2C9, 2C19, 2C8, 2C18, 1A2 in 3A4.
• Ti izoencimi kažejo veliko genetsko variabilnost (teže predvidljiv učinek varfarina)
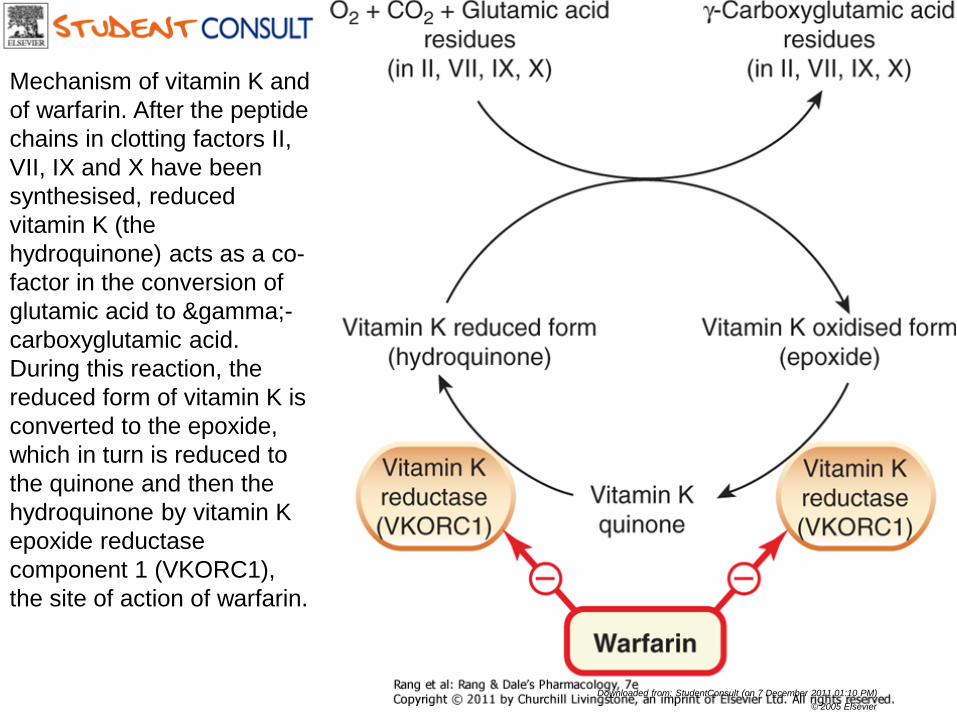
Mechanism of vitamin K and of warfarin. After the peptide chains in clotting factors II, VII, IX and X have been synthesised, reduced vitamin K (the hydroquinone) acts as a co-factor in the conversion of glutamic acid to γ-carboxyglutamic acid. During this reaction, the reduced form of vitamin K is converted to the epoxide, which in turn is reduced to the quinone and then the hydroquinone by vitamin K epoxide reductase component 1 (VKORC1), the site of action of warfarin.
Downloaded from: StudentConsult (on 7 December 2011 01:10 PM) © 2005 Elsevier
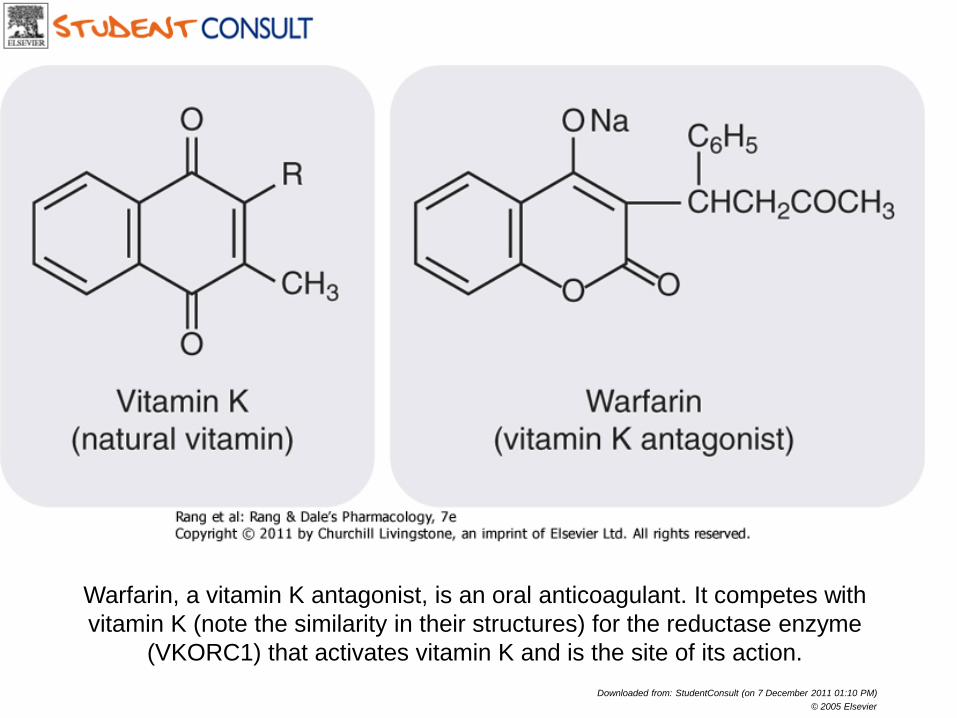
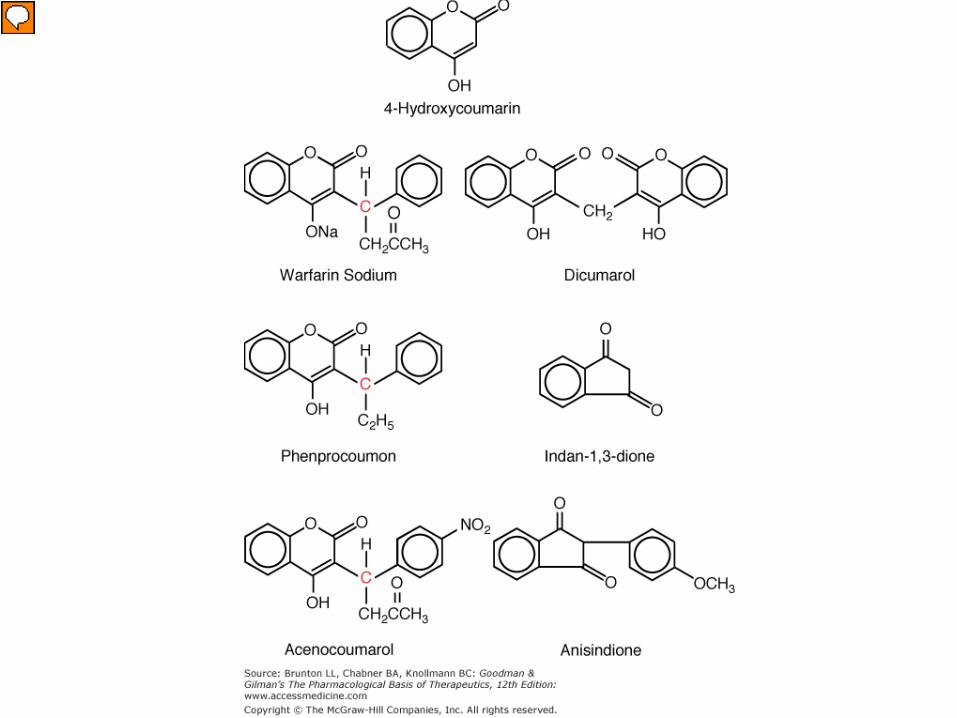
Warfarin, a vitamin K antagonist, is an oral anticoagulant. It competes with vitamin K (note the similarity in their structures) for the reductase enzyme
(VKORC1) that activates vitamin K and is the site of its action. Downloaded from: StudentConsult (on 7 December 2011 01:10 PM)
© 2005 Elsevier
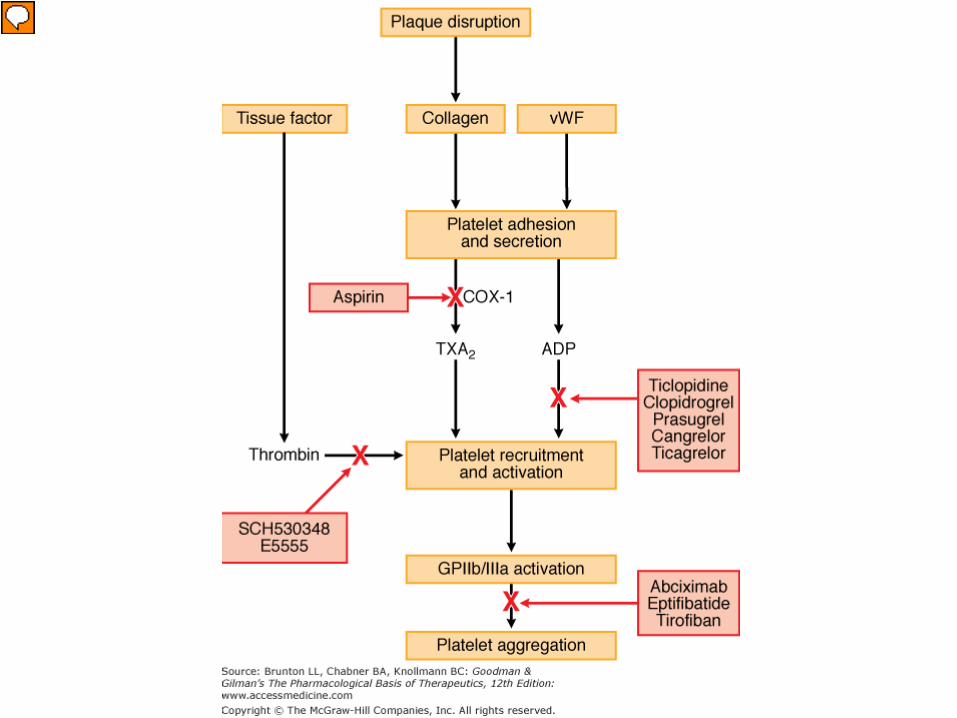
Klopidogrel • Antagonist adenozin difosfata(ADP) na trombocitnih
receptorjih P2Y12 ⇒ preprečena aktivacija glikoproteina GPIIb/IIIa
• Predzdravilo – aktivacija s CYP2C19, CYP3A4, CYP2B6 in CYP1A2
Indikacije • profilaksa arterijskih trombembolij • stabilna koronarna bolezen, pešanje srca, ateroskleroza
z dokazano kapjo • svež miokardni infarkt • akutni koronarni sindrom • miokardni infarkt z dvignjenim ST-segmentom • po operacijah na srcu
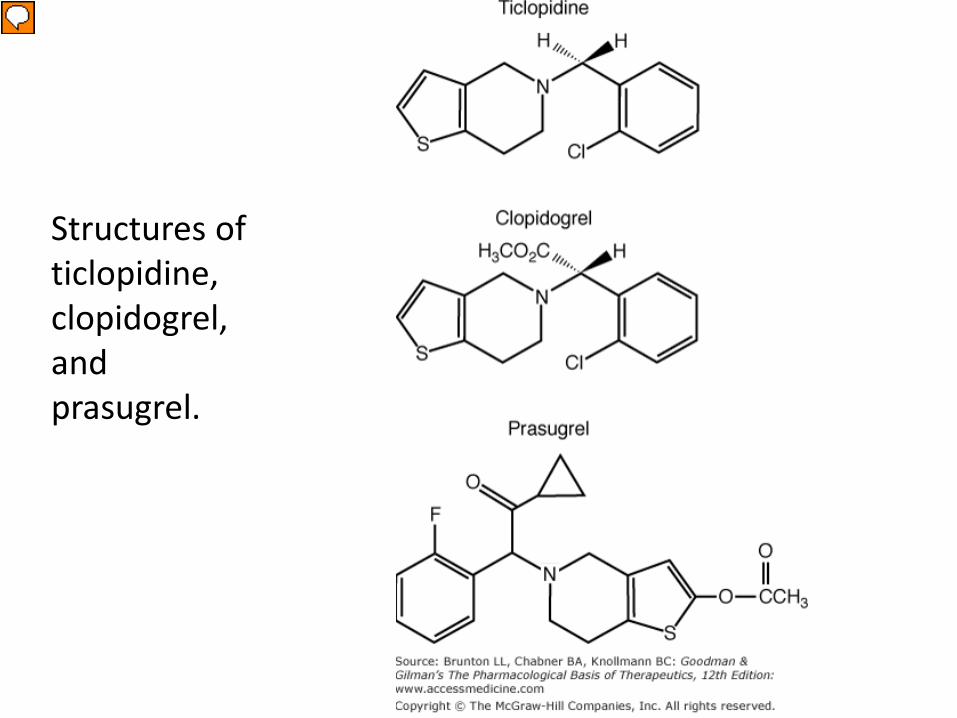
Structures of ticlopidine, clopidogrel, and prasugrel.
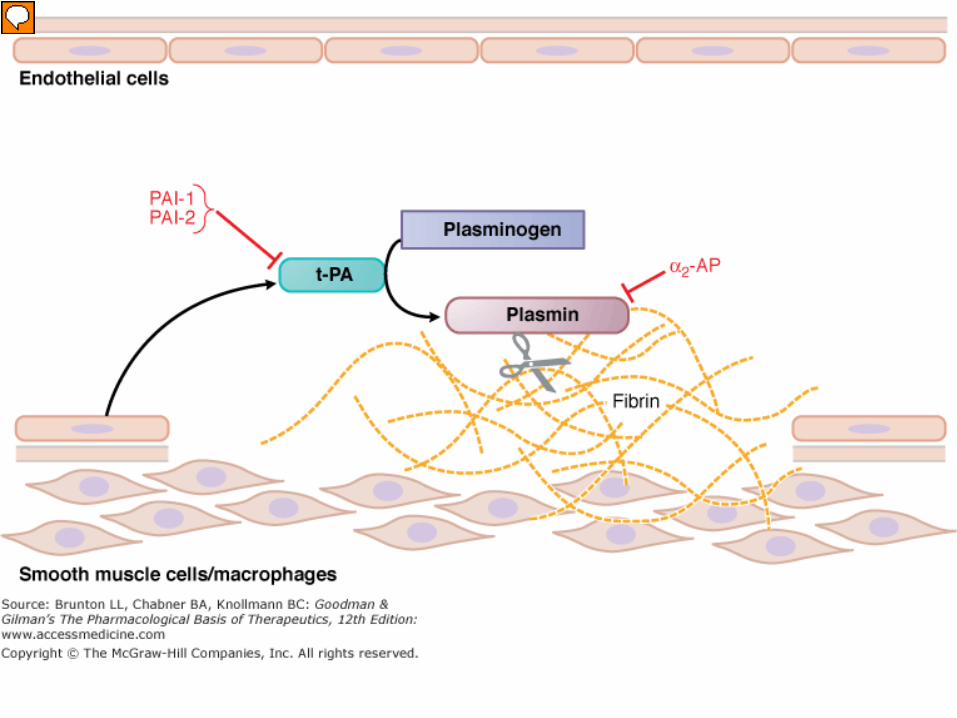
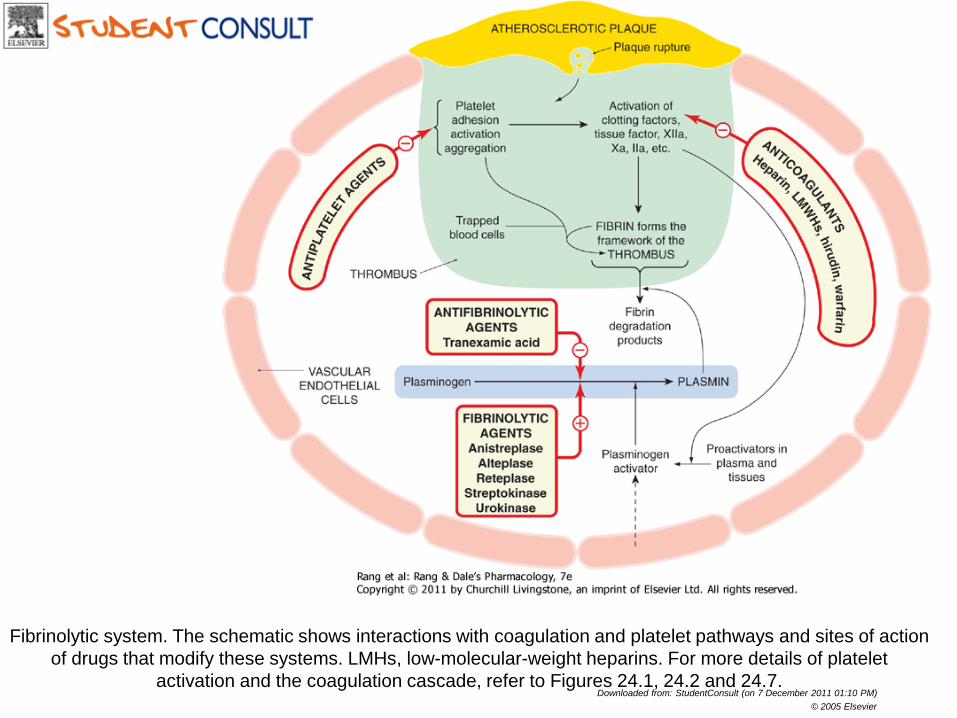
Fibrinolytic system. The schematic shows interactions with coagulation and platelet pathways and sites of action of drugs that modify these systems. LMHs, low-molecular-weight heparins. For more details of platelet
activation and the coagulation cascade, refer to Figures 24.1, 24.2 and 24.7. Downloaded from: StudentConsult (on 7 December 2011 01:10 PM)
© 2005 Elsevier
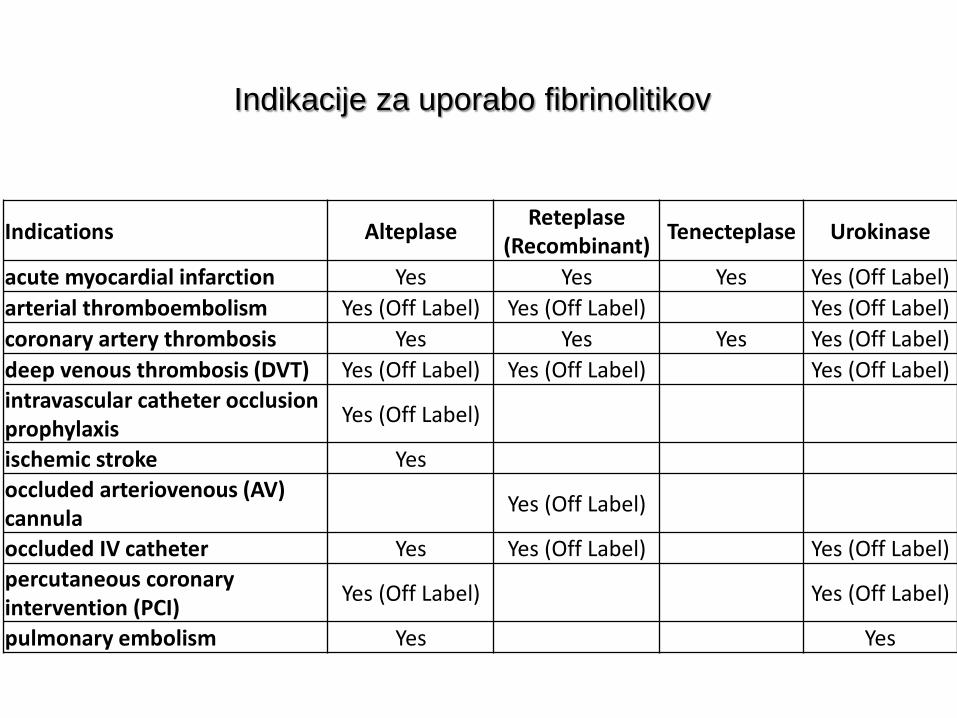
Indikacije za uporabo fibrinolitikov
Indications Alteplase Reteplase (Recombinant) Tenecteplase Urokinase
acute myocardial infarction Yes Yes Yes Yes (Off Label) arterial thromboembolism Yes (Off Label) Yes (Off Label) Yes (Off Label) coronary artery thrombosis Yes Yes Yes Yes (Off Label) deep venous thrombosis (DVT) Yes (Off Label) Yes (Off Label) Yes (Off Label) intravascular catheter occlusion prophylaxis Yes (Off Label)
ischemic stroke Yes occluded arteriovenous (AV) cannula Yes (Off Label)
occluded IV catheter Yes Yes (Off Label) Yes (Off Label) percutaneous coronary intervention (PCI) Yes (Off Label) Yes (Off Label)
pulmonary embolism Yes Yes
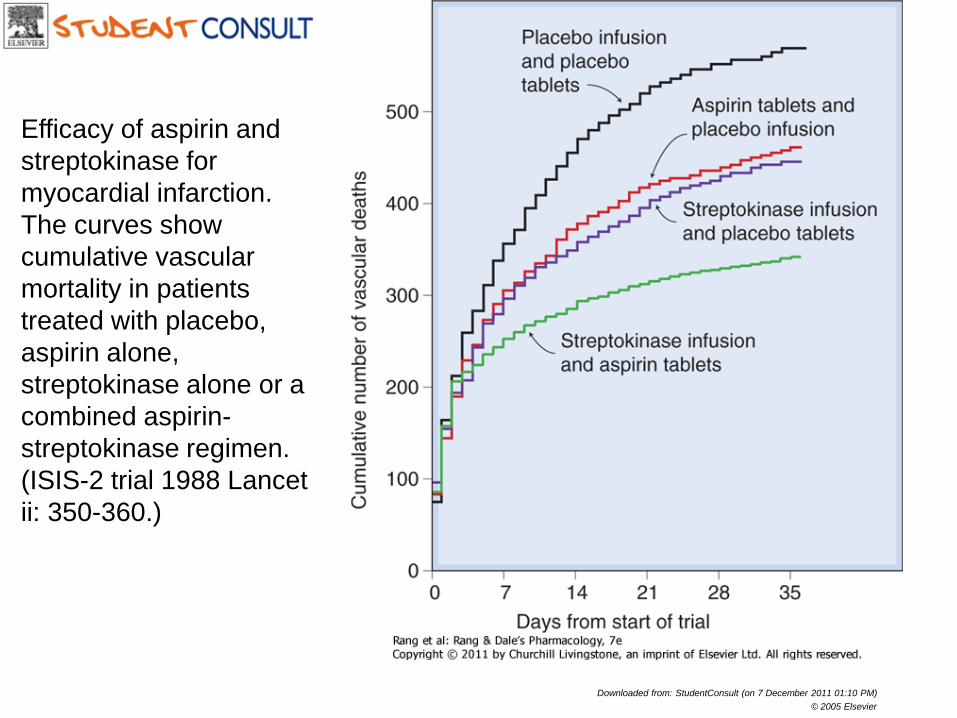
Efficacy of aspirin and streptokinase for myocardial infarction. The curves show cumulative vascular mortality in patients treated with placebo, aspirin alone, streptokinase alone or a combined aspirin-streptokinase regimen. (ISIS-2 trial 1988 Lancet ii: 350-360.)
Downloaded from: StudentConsult (on 7 December 2011 01:10 PM) © 2005 Elsevier
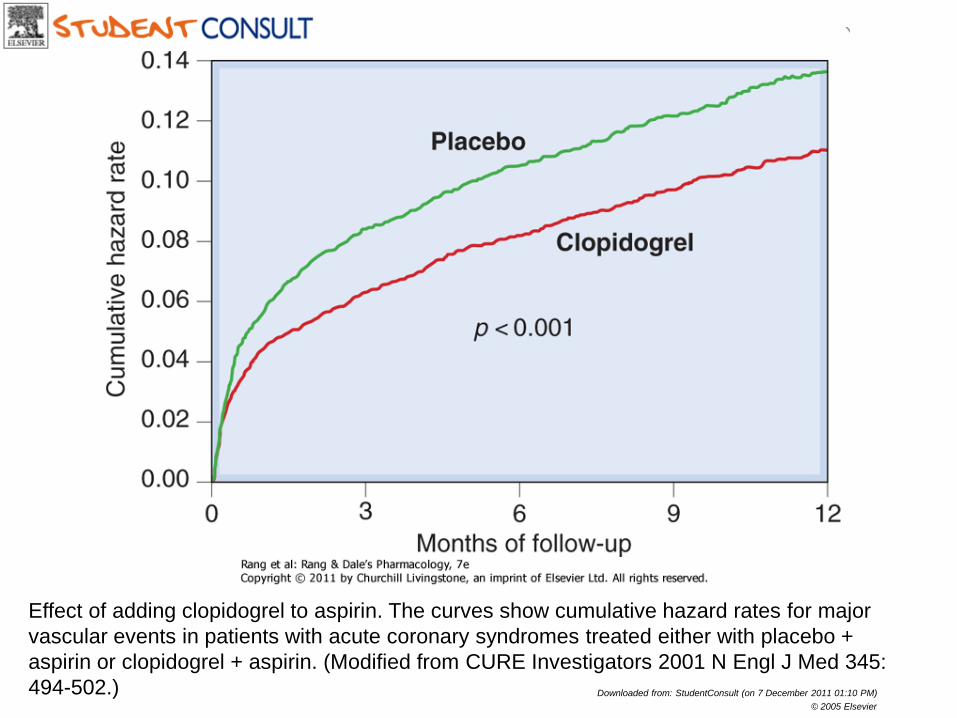
Effect of adding clopidogrel to aspirin. The curves show cumulative hazard rates for major vascular events in patients with acute coronary syndromes treated either with placebo + aspirin or clopidogrel + aspirin. (Modified from CURE Investigators 2001 N Engl J Med 345: 494-502.) Downloaded from: StudentConsult (on 7 December 2011 01:10 PM)
© 2005 Elsevier





























