-
8/8/2019 Zinc Diarrhea
1/13
DOI:10.1542/peds.2007-09212008;121;326-336Pediatrics
Marek Lukacik, Ronald L. Thomas and Jacob V. ArandaPersistent
Diarrhea
A Meta-analysis of the Effects of Oral Zinc in the Treatment of
Acute and
http://www.pediatrics.org/cgi/content/full/121/2/326located on
the World Wide Web at:
The online version of this article, along with updated
information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN:
1098-4275.Grove Village, Illinois, 60007. Copyright 2008 by the
American Academy of Pediatrics. Alland trademarked by the American
Academy of Pediatrics, 141 Northwest Point Boulevard,
Elkpublication, it has been published continuously since 1948.
PEDIATRICS is owned, published,PEDIATRICS is the official journal
of the American Academy of Pediatrics. A monthly
. Provided by Indonesia:AAP Sponsored on August 30,
2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/cgi/content/full/121/2/326http://www.pediatrics.org/cgi/content/full/121/2/326http://www.pediatrics.org/cgi/content/full/121/2/326http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/cgi/content/full/121/2/326
-
8/8/2019 Zinc Diarrhea
2/13
ARTICLE
A Meta-analysis of the Effects of Oral Zinc in the
Treatment of Acute and Persistent DiarrheaMarek Lukacik,MDa,
RonaldL. Thomas, PhDb, Jacob V.Aranda, MD, PhDb
aDepartment of Pediatrics, Childrens Medical Center, Medical
College of Georgia, Augusta, Georgia; bDepartment of Pediatrics,
Wayne State University School of
Medicine, and Childrens Hospital of Michigan, Detroit, Michigan,
and National Institute of Child Health and Human Development,
Pediatric Pharmacology
Research Unit Network, Wayne State University, Detroit,
Michigan
The authors have indicated they have no financial relationships
relevant to this article to disclose.
ABSTRACT
OBJECTIVE. Children in developing countries are at a high risk
for zinc deficiency.Supplemental zinc has previously been shown to
provide therapeutic benefits in
diarrhea. The objective of this study was to examine the
efficacy and safety ofsupplemental oral zinc therapy during
recovery from acute or persistent diarrhea.
METHODS. We conducted a meta-analysis of randomized, controlled
trials to comparethe efficacy and safety of supplementary oral zinc
with placebo in children with acuteand persistent diarrhea. Results
were reported using a pooled relative risk or aweighted mean
difference. A total of 22 studies were identified for inclusion:
16examined acute diarrhea (n 15 231), and 6 examined persistent
diarrhea (n 2968).
RESULTS. Mean duration of acute diarrhea and persistent diarrhea
was significantlylower for zinc compared with placebo. Presence of
diarrhea between zinc andplacebo at day 1 was not significantly
different in acute diarrhea or persistentdiarrhea trials. At day 3,
presence was significantly lower for zinc in persistent
diarrhea trials (n 221) but not in acute diarrhea trials.
Vomiting after therapy wassignificantly higher for zinc in 11 acute
diarrhea trials (n 4438) and 4 persistentdiarrhea trials (n 2969).
Those who received zinc gluconate in comparison withzinc
sulfate/acetate vomited more frequently. Overall, children who
received zincreported an 18.8% and 12.5% reduction in average stool
frequency, 15.0% and15.5% shortening of diarrhea duration, and a
17.9% and 18.0% probability ofreducing diarrhea over placebo in
acute and persistent trials, respectively.
CONCLUSIONS. Zinc supplementation reduces the duration and
severity of acute and persistent diarrhea; however, themechanisms
by which zinc exerts its antidiarrheal effect have not been fully
elucidated.
DIARRHEAL DISEASES POSE a significant public health problem on a
global scale and especially in developing
countries. It is estimated that there are 1.5 billion episodes
of diarrhea per year and that diarrheal diseaseaccounted for 21% of
all deaths in children who were younger than 5 years. This is
equivalent to 2.5 million deaths
in the same age group.1,2
This compares more favorably with the results of a previous
study from 1982 in which on the basis of a review
of active surveillance data from studies conducted in the 1950s,
1960s, and 1970s, it was estimated that 4.6 millionchildren died
annually from diarrhea.3 Newer data from the World Health
Organization (WHO) show that diarrhealdisease accounts for 18% of
the 10.6 million deaths in children who were younger than 5 years.
4
One of the major advances in the reduction of mortality from
diarrhea was the introduction of WHO oralrehydration solution
(ORS)5; however, WHO ORS does not significantly decrease stool
output and duration of
diarrhea, and therefore other approaches to add to or to enhance
the available ORS have been sought. Several newerapproaches have
included the addition of zinc to the treatment regimen. Zinc is an
essential micronutrient and
protects cell membranes from oxidative damage. Zinc is not
stored in the body, so the level of zinc is determined bythe
balance of dietary intake, absorption, and losses. A zinc
deficiency state may exist in children with acute diarrhea
www.pediatrics.org/cgi/doi/10.1542/peds.2007-0921
doi:10.1542/peds.2007-0921
KeyWords
diarrhea, zinc
Abbreviations
WHOWorld Health Organization
ORSoral rehydration solution
RRrelative risk
WMDweighted mean difference
CIconfidence interval
cAMP3,5-cyclic monophosphate
Kpotassium
Cacalcium
Accepted for publication Jul 24, 2007
Address correspondence to Marek Lukacik,MD, Childrens Medical
Center Department of
Pediatrics, Medical College of Georgia, 1120
15th St, Augusta, GA 30912. E-mail: mlukacik@
mcg.edu
PEDIATRICS (ISSNNumbers:Print, 0031-4005;
Online, 1098-4275). Copyright 2008by the
AmericanAcademy of Pediatrics
326 LUKACIK et al. Provided by Indonesia:AAP Sponsored on August
30, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
3/13
-
8/8/2019 Zinc Diarrhea
4/13
StatisticalAnalysesComprehensive Meta-Analysis,10 a stand-alone
program,was used to synthesize data that were obtained from the22
trials identified for inclusion: 16 acute and 6 persis-tent
diarrhea trials. Briefly, the analysis software pro-duces a Forrest
plot as a schematic description of themeta-analysis results. The
program is augmented usingaccepted computational algorithms. Where
appropriate,
results were reported using a pooled relative risk (RR).For
continuous outcomes, the weighted mean difference(WMD) was
calculated. The 95% confidence intervals(CIs) were reported around
the weighted effect size.
HeterogeneityGiven that studies that are selected for inclusion
in ameta-analysis will differ, the types of variability
(clinical,methodologic, and/or statistical) that may occur
amongstudies must be investigated. These various types of
vari-ability are termed heterogeneity. Meta-analysis should
be considered only when a group of trials is
sufficientlyhomogeneous (as indicated in the inclusion criteria)
in
terms of participants, interventions, and outcomes toprovide a
meaningful summary. Strict adherence to theinclusion criteria
listed, such as blinding and conceal-ment of allocation, help to
control for clinical/method-ologic heterogeneity. Still,
statistical heterogeneity canalso occur when variability in the
treatment effects beingevaluated in the different trials exists.
This results whenthe observed treatment effects are more different
fromeach other than would be expected as a result of randomerror
(chance) alone. Following convention, statisticalheterogeneity in
the results of this meta-analysis arereferred to simply as
heterogeneity.
Different approaches for identification and measure-
ment of heterogeneity were therefore undertaken toexamine the
extent to which the results of the studiesincluded were consistent.
CIs for the results of individualstudies (depicted graphically
using horizontal lines) wereexamined for poor overlap, a general
indication of pres-ence of statistical heterogeneity. Variability
(heterogene-ity) among the obtained effects sizes was formally
op-erationalized using a 2 test of significance. The formulafor
heterogeneity assesses the dispersion of individualoutcomes,
vis-a-vis the combined effect, and denotesthis value using a Q
statistic.11 A low P value (or a large2 statistic relative to its
degree of freedom) providesevidence of heterogeneity of treatment
effects (variationin effect estimates beyond chance).
Because some degree of clinical and methodologicdiversity always
occurs in a meta-analysis, some statis-tical heterogeneity is
inevitable; therefore, the test forheterogeneity is irrelevant to
the choice of analysis: het-erogeneity will always exist regardless
of whether it can
be detected using a statistical test. Still, methods have been
developed for quantifying inconsistency acrossstudies that move the
focus away from testing whetherheterogeneity is present to
assessing its impact on themeta-analysis. A useful statistic for
quantifying inconsis-tency is I2, the percentage of the variability
in effect sizeestimates that is attributable to heterogeneity
ratherthan sampling error (chance).12 A value 50% may be
considered substantial heterogeneity, and that percent-age
cutoff was adopted and examined also in our anal-yses.
GravityAnother more recent approach13 proposed jackknife
re-sampling to measure a concept termed gravity. In any
meta-analysis, arguments have focused on the inclusionor
exclusion of some studies, with debate on which onesshould be
included or excluded because studies are com-monly weighted
according to their sample size and/orinternal variability. Gee13
proposed that jackknife re-sampling could be used to examine study
influence anddetect outlier studies. The technique recomputes
themeta-analysis once for each of k studies, where eachstudy is
individually excluded. K results are then ob-tained. The difference
between the average of these kresults and each studys individual
result (when omit-ted) is taken as an index of raw gravity. This
differ-ence, divided by the SD of the k differences, is taken
as
a zscore, or standardized gravity, which can be used toestablish
which studies might be unusually influential.SPSS 15.014 was used
to calculate standardized gravityvalues.
Fixed- or Random-EffectsModelChoice of whether to interpret a
fixed-effects or ran-dom-effects model was considered thoroughly.
Fixed-effect meta-analyses ignore heterogeneity. The fixed-effect
estimate and its CI address the question, What isthe best estimate
of the treatment effect? The random-effects estimate and its CI
address the question, What is
the average treatment effect? The answers to thesequestions are
analogous when no heterogeneity ispresent or when the distribution
of the treatment effectsis roughly symmetrical. If they are not,
then the ran-dom-effects estimate may not reflect the actual effect
inany population being studied. In a fixed-effects meta-analysis, a
pooled-effect estimate is termed, generally, asthe best estimate of
the treatment effect. It is for thesereasons that we chose a
fixed-effects model for ourmeta-analysis, along with the various
stated approachesto examine heterogeneity if found.
RESULTS
The author, year, country, amount of zinc supplemen-tation and
type, sample size, and age for each of the 22studies selected for
inclusion in the meta-analysis arelisted in Tables 3 and 4.
Although all 22 studies wererandomly assigned clinical trials, it
seemed that 51519
were not double-blinded. Sixteen of these publishedstudies met
the definition for acute diarrhea and 6 forpersistent diarrhea.
Overall, 56.3% (9 of 16) of acute diarrhea trials wereconducted
in inpatient hospital settings, and 43.7% (7 of16) were conducted
in outpatient homes and commu-nities. Of the 6 persistent diarrhea
trials, 66.7% (4 of 6)were inpatient and 33.3% (2 of 6) were
outpatient.
328 LUKACIK et al. Provided by Indonesia:AAP Sponsored on August
30, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
5/13
MortalityMortality was originally a primary outcome in this
meta-analysis; however, of both acute and persistent trials,only
315,20,21 reported mortality outcome, making it diffi-cult to
compare across all included trials. Two of thesewere acute diarrhea
trials,15,20 and 1 was a persistentdiarrhea trial.21 In the largest
acute diarrhea outpatienttrial15 (n 8070), 33 children (0.008%; 33
of 3974) diedin the zinc-treated group and 37 (0.009%; 37 of
4096)died in the placebo group. Thirty deaths were attributedto
drowning, and the remaining were not injury related(ie, not
attributable to zinc intervention). When re-stricted to noninjury
deaths, there were 13 in the zinc-treated group and 27 in the
placebo group. The investi-gators attributed the lower noninjury
death rate in theintervention group almost entirely to fewer deaths
fromdiarrhea and acute lower respiratory infection. Diarrheaand
acute lower respiratory infection together accountedfor 10 deaths
in the zinc intervention group and 20deaths in the placebo group.
In the other acute diarrheatrial,20 2 children in the placebo group
died of septicemia.In the persistent diarrhea trial,21 the causes
of death weresepticemia with diarrhea in 3 children, septicemia in
1child, bronchopneumonia in 1 child, and continued di-arrhea in 1
child. Because acute and persistent diarrheaare, most likely,
distinct disease entities, the outcomes
obtained are presented initially for acute diarrhea (last-ing up
to 14 days) and followed by persistent diarrhea(lasting 14
days).
Results forAcuteDiarrhea Trials
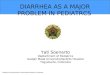
Duration of Acute DiarrheaIn 16 trials that examined the primary
measure of aver-age duration of acute diarrhea1517,19,20,2232 (n 15
231),those who received zinc experienced a significantlylower
average duration of diarrhea than those who re-ceived a placebo
(WMD: 0.24; SE: 0.02; 95% CI: 0.210.27; P .001; Table 5, Fig 1) but
also with the presenceof statistically significant heterogeneity (Q
95.58, de-grees of freedom [df]Q 15, P .001, I
2 84.3%).Figure 1 depicts a Forrest plot for these results, in
whichevery study is displayed as a point estimate with CIs.
Examination of significant heterogeneity in the acutediarrhea
trials revealed 5 trials17,19,20,25,30 with insignifi-cant
differences between zinc and placebo groups inaverage duration of
diarrhea. P values ranged from .478to nonsignificant in sample
sizes that ranged from 50 to215. Although those who received zinc
had a shorteraverage duration of diarrhea, the difference in 4
tri-als17,19,20,30 was very small, with an average difference
of0.18 0.18 days ranging from 0.04 to 0.40 days. One
TABLE 3 Characteristics of Acute Diarrhea Trials
Reference Country Zinc Supplement Zinc Dosage Zinc/Control
Group, N Age, mo
Sachdev et al17 (1988) India Sulfate 20 mg 25/25 618
Sazawal et al31 (1995) India Gluconate 20 mg 456/481 635
Roy et al30 (1997) Bangladesh Acetate 20 mg 57/54 324
Faruque et al27 (1999) Bangladesh Acetate 14/40 mg 343/341
623
Hidayat et al28 (1998) Indonesia Acetate 4/5 mg/kg 739/659
325
Dutta et al26 (2000) India Sulfate 40 mg 44/36 324
Strand et al32 (2002) Nepal Gluconate 15/30 mg 445/449 635
Bahl et al23 (2002)a India Gluconate 15/30 mg 404/401 635
Al-Sonboli et al22 (2003) Brazil Sulfate 22.5/45 mg 37/37
360
Polat et al29 (2003)b Turkey Sulfate 20 mg 92/90 229
Bhatnagar et al24 (2004) India Sulfate 15/30 mg 143/144 336
Valery et al19 (2005)c Australia Sulfate 20/40 mg 107/108 011,
1223,24
Patel et al20 (2005) India Sulfate/copper sulfate 40 mg/5 mg
102/98 659
Brooks et al25 (2005)d Bangladesh Acetate 20 mg 86/89 16
Baqui et al15 (2002) Bangladesh Acetate 20 mg 3974/4096 359
Fischer Walker et al16 (2006) Pakistan, Ethiopia, India Sulfate
10 mg 554/556 15
aThree study groups were examined (control, zinc syrup, and
zinc/ORS). We included only those who received zinc syrup or a
control.b Four study groups were examined: low/normal zinc in 2
intervention groups and low/normal zinc in 2 control groups. We
combined the groups into either intervention or control,
without
excluding those with low zinc levels.c Children up to 11 years
of age were included; however, 45.1% (97 of 215) were 0 to 11
months of age; 38.1% (82 of 215) were 12 to 23 months; and only
16.8% (36 of 215) were 24 months. All
study participants were included in our analyses.dThree groups
wereused (control,5 mgof zincacetate, and20 mgof zincacetate).We
examinedonly those whoused 20mg of zincversuscontrolsubjects.Brooks
etal enrolledonlymale children.
TABLE 4 Characteristics of Persistent Diarrhea Trials
Reference Country Zinc Supplement Zinc Dosage Zinc/Control
Group,N Age, mo
Sachdev et al18 (1990) India Sulfate 20 mg 20/20 618
Roy et al21 (1998) Bangladesh Acetate 20 mg 95/95 324
Khatun et al34 (2001) Bangladesh Acetate 20 mg 24/24 624
Bhutta et al33 (1999) Pakistan Sulfate 3 mg/kg 43/44 636
Penny et al35 (1999) Peru Gluconate 20 mg 139/136 635
Bhandari et al36 (2002) India Gluconate 10/20 mg 1228/1236
630
PEDIATRICS Volume 121, Number 2, February 2008 329. Provided by
Indonesia:AAP Sponsored on August 30,
2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
6/13
trial25 found no difference at all between treatmentgroups.
Participants in all 5 trials had been admitted fordehydration
secondary to diarrhea, although the sever-ity of dehydration
ranged. Four of the trials17,20,25,30 ad-ministered an ORS before
treatment assignment. Threetrials received zinc sulfate and 2
received acetate. Incontrast, all acute diarrhea trials23,31,32
that provided zincgluconate and not zinc sulfate had a shorter
duration ofdiarrhea than placebo (P .08). Two trials17,20
originatedfrom India, 225,30 from Bangladesh, and 119 from
Austra-lia. One trial15 in which average duration was
signifi-cantly lower (1.2 days lower) with zinc use also had a
tremendously higher sample size (n 8070) than all ofthe
others.
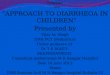
Table 6 shows the effect sizes, calculated raw gravityvalues,
standardized gravity values, and sample sizes foreach study when
removed. It is clear that 1 study15 hada great deal of impact on
the strength and direction ofthe estimated effect size value found
for average dura-tion of acute diarrhea among all studies. When
removed,the reaveraged effect size obtained (0.187) and
plottedstandardized gravity value (3.531; Fig 2) were consid-ered
outlying values in comparisons with all others. Thisis largely
attributed to the enormous sample size (n 8070) used in the trial,
because even very small differ-ences in mean duration of diarrhea
would be statisticallysignificant.
Occurrence of Diarrhea at Day 1Five acute diarrhea
trials16,19,20,27,32 reported the occur-rence of diarrhea at day 1
(n 3100). No statisticallysignificant difference in the occurrence
of acute diarrheaat day 1 was found (RR: 1.01; 95% CI: 0.991.03;
P0.30). Although the variability in effect sizes rangedfrom a low
of 0.968 to 1.695, significant heterogeneitydid occur (Q 10.60, dfQ
4, P .03, I
2 62.3%).
Occurrence of Diarrhea at Day 3Six acute diarrhea
trials16,19,20,23,27,32 collected data for oc-currence of diarrhea
at day 3. No statistically significantdifferences occurred between
treatment groups in occur-rence of diarrhea at day 3 (RR: 0.97; 95%
CI: 0.911.03;P .36); however, the occurrence of statistically
signif-icant heterogeneity was found (Q 10.880, dfQ 5, P0.05, I2
54.0%). Only 1 trial30 found a significantly(P .01) lower
occurrence of diarrhea at day 3 with zinc(27.4%) than placebo
(35.4%; effect size: 0.774); how-ever, the occurrence of
statistically significant heteroge-neity was found (Q 10.880, dfQ
5, P .05, I
2
54.0%).
FIGURE 1
Mean difference in duration of acute diarrhea. The effect size
index in this plot is the
standard mean difference, so a point estimate of 0.0 indicates
no effect. Values0.0
reflect a better outcome for the placebo group, and values 0.0
indicate a better out-
come forthe zincgroup. If thepointestimate andCI
fellabove0.0,then thestudywould
meet the criterion for statistical significance( .05). Ifthe CI
overlapped 0.0, thentheP
value would exceed .05 and the study would not be statistically
significant.
TABLE 5 MeanDurationof AcuteDiarrhea
Reference N1 N2 Lower Upper Effect SE P
Sachdev et al17 (1988) 25 25 .371 .769 .199 .284 .478
Sazawal et al31 (1995) 456 481 .128 .386 .257 .066 .000
Roy et al30 (1997) 37 37 .312 .616 .152 .233 .511
Hidayat et al28 (1998) 738 659 .015 .225 .120 .054 .025
Faruque et al27 (1999) 341 340 .045 .347 .196 .077 .011
Dutta et al26 (2000) 44 36 1.811 2.995 2.403 .297 .000
Strand et al32 (2002) 445 449 .052 .315 .184 .067 .006
Baqui et al15 (2002) 3974 4096 .243 .331 .287 .022 .000
Bahl et al23 (2002) 404 401 .016 .261 .122 .071 .083
Polat et al29 (2003) 92 90 .425 1.030 .727 .153 .000
Al-Sonboli et al22 (2003) 37 37 .435 1.412 .924 .245 .000
Bhatnagar et al24 (2004) 143 144 .025 .441 .208 .118 .079
Patel et al20 (2005) 102 98 .246 .312 .033 .141 .817
Valery et al19 (2005) 107 108 .260 .278 .009 .136 .946
Brooks et al25 (2005) 86 89 .298 .298 .000 .151 NS
Fischer Walker et al16 (2006) 554 556 .006 .242 .124 .060
.039
Fixed combined (16) 7585 7646 .208 .272 .240 .016 .000
N1 indicates sample size for zinc group; N2, sample size for the
placebo group; Lower, lower limit of the 95% CI for the standard
difference;
Upper, upper limit of the 95% CI for the standard difference;
Effect, standard difference; NS, nonsignificant.
330 LUKACIK et al. Provided by Indonesia:AAP Sponsored on August
30, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
7/13
Occurrence of Diarrhea at Day 5Similarly, in the same 6 acute
diarrhea trials, 16,19,20,23,27,32
no statistically significant differences occurred between
treatment groups in occurrence of diarrhea at day 5 (RR:0.94;
95% CI: 0.84 1.05; P .26). Similar to day 3results, the occurrence
of statistically significant hetero-
FIGURE 2
Standardized gravity results.
TABLE 6 AcuteDiarrhea:Gravity Values forDurationofDiarrhea
Reference Effect Size Raw Gravity Standardized Gravity Sample
Size
Valery et al19 (2005) 0.243 0.00481 0.332 215
Strand et al32 (2002) 0.243 0.00481 0.332 894
Sazawal et al31 (1995) 0.239 0.00081 0.056 937
Sachdev et al17 (1988) 0.240 0.00181 0.125 50
Roy et al30 (1997) 0.240 0.00181 0.125 74
Polat et al29 (2003) 0.234 0.00419 0.289 182
Patel et al20 (2005) 0.243 0.00481 0.332 200
Hidayat et al28 (1998) 0.252 0.01381 0.953 1397
Fischer Walker et al16 (2006) 0.249 0.01081 0.746 1110
Faruque et al27 (1999) 0.242 0.00381 0.263 681
Dutta et al26 (2000) 0.233 0.00519 0.358 80
Brooks et al25 (2005) 0.243 0.00481 0.332 175
Bhatnagar et al24 (2004) 0.240 0.00181 0.125 287
Baqui et al15 (2002) 0.187 0.05119 3.531 8070
Bahl et al23 (2002) 0.246 0.00781 0.539 805
Al-Sonboli et al22 (2003) 0.237 0.00119 0.082 74
PEDIATRICS Volume 121, Number 2, February 2008 331. Provided by
Indonesia:AAP Sponsored on August 30,
2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
8/13
geneity was found (Q 18.957, dfQ 5, P .002, I2
73.6%).
VomitingIn 11 acute diarrhea trials16,17,19,2225,2932 (n 4438),
theproportion of participants who vomited after the initialdose was
significantly higher with zinc (278 [12.7%] of2196) use than with
placebo (171 [7.6%] of 2242; RR:1.55; 95% CI: 1.301.84; P 0.001%; Q
25.54, P.004).
Vomiting After Administration of Zinc Sulfate or GluconateIn 3
acute diarrhea trials,23,31,32 a significantly higherproportion of
patients who received zinc gluconate vom-ited (160 [14.6%] of 1095)
than zinc sulfate/acetatetherapy16,17,19,22,24,25,29,30 (118
[10.7%] of 1101; RR: 1.18;95% CI: 1.051.31; P .006).
Shortening of Diarrhea DurationEight trials of acute
diarrhea1517,20,25,26,29,31 found an av-erage shortening of
diarrhea duration of 15.0% for thosewho received zinc in comparison
with placebo (Table 7).
Reduction in Stool FrequencySeven trials of acute
diarrhea17,22,23,25,29,31,32 found an av-erage reduction in stool
frequency of 22.1% with zinctherapy in comparison with placebo. One
single trial16
found a 5.0% higher stool frequency using zinc thanplacebo.
Stool OutputThree trials of acute diarrhea24,26,30 found an
averagelowering of stool output of 30.3%.
Probability of Diarrhea ReductionEight acute diarrhea
trials20,2325,27,28,30,32 measured theprobability of diarrhea
reduction and found a 17.9%reduction using zinc compared with
placebo.
Results forPersistent Diarrhea Trials
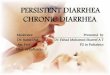
Duration of Persistent DiarrheaIn 5 persistent diarrhea
trials18,21,3335 (n 489), thosewho received zinc also experienced a
significantly loweraverage duration of diarrhea than the placebo
group(WMD: 0.30; SE: 0.09; 95% CI: 0.120.48; P .001;Table 8) but
without significant heterogeneity (Q 3.08,
TABLE 7 Effects of Zinc Therapy of AcuteDiarrhea
Reference Country Stool Frequency Reduction Probability of
Diarrhea Continuation
Sachdev et al17 (1988) India 18% lower frequency 9% shorter
duration
Sazawal et al31 (1995) India 39% lower frequency 19% shorter
duration
Roy et al30 (1997) Bangladesh 28% lower stool output 14%
reduction in probability
Faruque et al27 (1999) Bangladesh Not reported 20% reduction in
probability
Hidayat et al28 (1998) Indonesia Not reported 11% reduction in
probability
Dutta et al26 (2000) India 38% lower stool output 32% shorter
duration
Strand et al32 (2002) Nepal 8% lower frequency 26% reduction in
probability
Bahl et al23 (2002) India 17% lower frequency 11% reduction in
probability
Al-Sonboli et al22 (2003) Brazil 59% lower frequency Not
reported
Polat et al29 (2003) Turkey 14% lower frequency 20% shorter
duration
Bhatnagar et al24 (2004) India 25% lower stool output 30%
reduction in probability
Valery et al19 (2005) Australia Not reported Not reported
Brooks et al25 (2005) India Not reported 19% reduction in
probability, 7% shorter duration
Brooks et al25 (2005) Bangladesh 0% lower frequency 12%
reduction in probability, 0% shorter duration
Baqui et al15 (2002) Bangladesh Not reported 24% shorter
duration
Fischer Walker et al16 (2006) Pakistan, Ethiopia, India 5%
higher frequency 9% shorter duration
Average stool frequency reduction 18.8%; average lowering of
stool output 30.3%; average shortening of duration 15.0%; average
probability of diarrhea reduction 17.9%. Variances in
datareporting of outcome measures:For thismeta-analysis,
shortening of diarrheaduration wasdefinedas thepercentage ratioof
themean number of daysof diarrheain eachstudygroup. It was
then reported as a shorter percentage of time with diarrhea for
one group or the other. Probability of diarrhea duration was
calculated by authors using various statistical approaches, such as
the
odds ratio, risk ratio, or hazards ratio. This difference in
statistic negated a comparison in the meta-analysis. Stool
frequency reduction was calculated by taking a ratio of the average
diarrhea
frequency in some studies per 24 hours or by the risk ratio of
the mean number of stools in the first 4 days of another study.
Lower stool output was calculated, in 2 studies, by taking a ratio
of the
totalstoolweightper kilogramof bodyweightandreporting themedian.
Theratioof themedianwasthen taken. Theresultingpercentagewas
interpreted asa loweringof stooloutputin onegroup
or the other. In another study, it was reported as the total
stool output until the last first formed stool, measured in grams
per kilogram for each group. The geometric mean was then taken and
a
ratio between groups obtained. The group with the lower
percentage was interpreted as a lowering of stool output in one
group or another.
TABLE 8 MeanDurationof Persistent Diarrhea
Reference N1 N2 Lower Upper Effect SE P
Sachdev et al18 (1990) 20 20 0.123 1.182 0.530 0.322 .096
Roy et al21 (1998) 73 68 0.201 0.466 0.133 0.169 .430
Penny et al35 (1999) 87 86 0.134 0.742 0.438 0.154 .004
Bhutta et al33 (1999) 43 44 0.295 0.558 0.132 0.215 .537
Khatun et al34 (2001) 24 24 0.167 1.010 0.422 0.292 .144
Fixed combined (5) 247 242 0.120 0.478 0.299 0.091 .001
332 LUKACIK et al. Provided by Indonesia:AAP Sponsored on August
30, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
9/13
dfQ 4, P .544, I2 29.9%). Figure 3 depicts the
Forrest plot for these results.
Occurrence of Diarrhea at Day 1In 2 trials of persistent
diarrhea34,35 (n 221), no statis-tically significant differences
occurred between treat-ment groups in occurrence of diarrhea at day
1 (RR:1.00; 95% CI: 0.931.08; P .98), and no
statisticallysignificant variability occurred among the effect
sizes(Q 0.01, dfQ 1, P .93).
Occurrence of Diarrhea at Day 3In 2 trials of persistent
diarrhea34,35 (n 221), a signifi-cantly lower occurrence of
diarrhea at day 3 occurred inthose who were treated with zinc in
comparison withplacebo (RR: 0.70; 95% CI: 0.510.94; P .02).
Nostatistically significant variability occurred among the
effect sizes (Q 0.33, dfQ 1, P .56).
Occurrence of Diarrhea at Day 5This was not examined; fewer than
2 studies reported.
VomitingIn 4 persistent diarrhea trials18,21,35,36 (n 2969), a
sig-nificantly higher proportion vomited on zinc (41 [2.8%]of 1482)
than with placebo (2 [0.001%] of 1487; RR:3.64; 95% CI: 1.0213.02;
P .047; Q 5.91, P .116).
Vomiting After Zinc Sulfate or GluconateIn 4 persistent diarrhea
trials,18,21,35,36 those who received
zinc gluconate35,36 vomited more frequently (41 [3%] of1367)
than did those who received zinc sulfate/acetate(0 [0%] of 115; RR:
1.09; 95% CI: 0.941.09; P .07).
Shortening of Diarrhea DurationIn 4 persistent diarrhea
trials,18,21,34,35 those who receivedzinc experienced a 15.5%
average shortening of diarrheaduration than those who got a placebo
(Table 9).
Reduction in Stool FrequencyFour trials of persistent diarrhea
found that those whoreceived zinc also experienced an average of
9.8% re-duction in frequency.
Stool OutputStool output was not measured in the persistent
trials.
Probability of Diarrhea ReductionTwo persistent diarrhea
trials33,36 that measured theprobability of diarrhea reduction
found an 18.0% reduc-tion when zinc was used over placebo.
DISCUSSION
On the basis of these findings, which now add to thelarge body
of previously published clinical data and up-date previous
meta-analyses and systematic reviews,8,37
zinc therapy is useful for treating both acute and persis-tent
diarrhea and for their prophylaxis. Still, as exten-sively
addressed in a recent systematic review,6 muchinformation is
lacking relative to the mechanisms bywhich zinc physiologically
exerts its antidiarrheal effect.In this meta-analysis, 5 (31.3%) of
16 acute diarrheastudies17,19,20,25,30 found no statistically
significant differ-
ences between zinc and placebo on the average durationof
diarrhea (at least a P .48). Similarly, 2 (40.0%) of 5persistent
diarrhea studies21,33 also found no statisticallysignificant
differences in average duration of diarrhea
between treatments (at least a P .43). Still, the averagestool
frequency reductions, shortening of diarrhea dura-tions, and
probabilities of a shortening of diarrhea dura-tion reported were
higher in studies with zinc therapy incomparison with placebo.
To the majority of individuals, diarrhea means anincreased
frequency or decreased consistency of bowelmovements. In many
developed countries, the averagenumber of bowel movements is 3 per
day; however,
diarrhea is associated with an increase in stool weight,mainly
as a result of excess water, which normallymakes up a large
percentage of fecal matter. Given this,diarrhea is distinguished
from diseases that cause onlyan increase in the number of bowel
movements or fecalincontinence.
Determining the exact causes of diarrhea can be dif-ficult
because there are many different diarrheal agents,with such a
variety of infectious agents, including bac-teria, parasites, and
viruses. Identification of specific di-arrheal agents is
complicated by the lack of access tolaboratory tests in many
developing countries. Viral gas-troenteritis caused by rotavirus is
the primary cause ofdiarrhea among infants worldwide. Other causes
include
bacterial pathogens such as Vibrio cholerae, Shigella,
andSalmonella. Protozoa such as Cryptosporidium parvum andGiardia
lamblia are 2 of the most common protozoandiarrheal agents. The
primary symptoms of rotavirusinfection are fever and vomiting for
several days, fol-lowed by nonbloody diarrhea. Although not
normallyfatal, the diarrhea caused by the virus can be quitesevere,
leading to potentially life-threatening dehydra-tion. Although
easily treated with intravenous fluids indeveloped nations, these
supplies are often unavailablein the developing world, and the
dehydration that iscaused by rotavirus is a significant cause of
mortality.
In fact, conclusions from these randomized trials for
FIGURE 3
Mean difference in duration of persistent diarrhea. The effect
size index in this plot is the
standard mean difference, so a point estimate of 0.0 indicates
no effect. Values0.0
reflect a better outcome for the placebo group, and values 0.0
indicate a better out-
come forthe zincgroup. If thepointestimate andCI
fellabove0.0,then thestudywould
meet the criterion for statistical significance( .05). Ifthe CI
overlapped 0.0, thentheP
value would exceed .05 and the study would not be statistically
significant.
PEDIATRICS Volume 121, Number 2, February 2008 333. Provided by
Indonesia:AAP Sponsored on August 30,
2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
10/13
-
8/8/2019 Zinc Diarrhea
11/13
-
8/8/2019 Zinc Diarrhea
12/13
40. Fenwick PK, Aggett PJ, Macdonald DC, Huber C, Wakelin D.
Zinc deprivation and zinc repletion: effect on the response
of
rats to infection with Strongyloides ratti. Am J Clin Nutr.
1990;
52(1):173177
41. Hoque KM, Rajendran VM, Binder HJ. Zinc inhibits cAMP-
stimulated Cl secretion via basolateral K-channel blockade
in
rat ileum. Am J Physiol Gastrointest Liver Physiol.
2005;288(5):
G956G963
42. Canani RB, Cirillo P, Buccigrossi V, et al. Zinc inhibits
cholera
toxin-induced, but not Escherichia coli heat-stable entero-
toxin-induced, ion secretion in human enterocytes. J Infect
Dis.
2005;191(7):10721077
43. Hershfinkel M, Moran A, Grossman N, Sekler I. A zinc-
sensing receptor triggers the release of intracellular Ca2
and regulates ion transport. Proc Natl Acad Sci USA. 2001;
98(20):1174911754
HIGH-STAKESFLIMFLAM
Its time to rein in the test zealots who have gotten such a
stranglehold on
the public schools in the US. Politicians and others have
promoted high-
stakes testing as a panacea that would bring accountability to
teaching and
substantially boost the classroom performance of students.
Measuring, said
President Bush, in a discussion of his No Child Left Behind law,
is the
gateway to success. Not only has high-stakes testing largely
failed to magi-
cally swing open the gates to successful learning, it is
questionable in many
cases whether the tests themselves are anything more than a
shell game.
Daniel Koretz, a professor at Harvards Graduate School of
Education, told me
in a recent interview that its important to ask whether you can
trust
improvements in test scores when you are holding people
accountable for the
tests. The short answer, he said, is no. If teachers,
administrators, politicians
and others have a stake in raising the test scores of studentsas
opposed to
improving student learning, which is not the same thingthere are
all kinds
of incentives to raise those scores by any means necessary. Weve
now had
four or five different waves of educational reform, said Dr.
Koretz, that were
based on the idea that if we can just get a good test in place
and beat people
up to raise scores, kids will learn more. Thats really what No
Child Left
Behind is. The problem is that you can raise scores the hard way
by teaching
more effectively and getting the students to work harder, or you
can take
shortcuts and start figuring out ways, as Dr. Koretz put it, to
game the
system. Guess whats been happening? Weve had high-stakes
testing, really,
since the 1970s in some states, said Dr. Koretz. Weve had maybe
six good
studies that ask: If the scores go up, can we believe them? Or
are people
taking shortcuts? And all of those studies found really
substantial inflation oftest scores.
Herbert B.New York Times. October 9, 2007
Noted by JFL, MD
336 LUKACIK et al. Provided by Indonesia:AAP Sponsored on August
30, 2010www.pediatrics.orgDownloaded from
http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/
-
8/8/2019 Zinc Diarrhea
13/13
DOI:10.1542/peds.2007-09212008;121;326-336Pediatrics
Marek Lukacik, Ronald L. Thomas and Jacob V. ArandaPersistent
Diarrhea
A Meta-analysis of the Effects of Oral Zinc in the Treatment of
Acute and
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/121/2/326including
high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/121/2/326#BIBLat:This
article cites 39 articles, 8 of which you can access for free
Citations
shttp://www.pediatrics.org/cgi/content/full/121/2/326#otherarticleThis
article has been cited by 3 HighWire-hosted articles:
Subspecialty Collections
http://www.pediatrics.org/cgi/collection/infectious_diseaseInfectious
Disease & Immunity
following collection(s):This article, along with others on
similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in
its entirety can be found online at:Information about reproducing
this article in parts (figures,
Reprintshttp://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
id d b d i ddi il d d f
http://www.pediatrics.org/cgi/content/full/121/2/326http://www.pediatrics.org/cgi/content/full/121/2/326http://www.pediatrics.org/cgi/content/full/121/2/326http://www.pediatrics.org/cgi/content/full/121/2/326#BIBLhttp://www.pediatrics.org/cgi/content/full/121/2/326#BIBLhttp://www.pediatrics.org/cgi/content/full/121/2/326#otherarticleshttp://www.pediatrics.org/cgi/content/full/121/2/326#otherarticleshttp://www.pediatrics.org/cgi/collection/infectious_diseasehttp://www.pediatrics.org/cgi/collection/infectious_diseasehttp://www.pediatrics.org/cgi/collection/infectious_diseasehttp://www.pediatrics.org/cgi/collection/infectious_diseasehttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/http://www.pediatrics.org/misc/reprints.shtmlhttp://www.pediatrics.org/misc/Permissions.shtmlhttp://www.pediatrics.org/cgi/collection/infectious_diseasehttp://www.pediatrics.org/cgi/content/full/121/2/326#otherarticleshttp://www.pediatrics.org/cgi/content/full/121/2/326#BIBLhttp://www.pediatrics.org/cgi/content/full/121/2/326