Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
74 (2007) 145–158www.elsevier.com/locate/ymvre
Microvascular Research
Potential therapeutic strategies for lymphatic metastasis
Bernadette M.M. Zwaans, Diane R. Bielenberg ⁎
Program in Vascular Biology, Department of Surgery, Children's Hospital, Harvard Medical School, Boston, Massachusetts, USA
Received 21 March 2007; revised 24 August 2007; accepted 24 August 2007
Abstract
Physiologically, the lymphatic system regulates fluid volume in the interstitium and provides a conduit for immune cells to travel to lymphnodes, but pathologically, the lymphatic system serves as a primary escape route for cancer cells. Lymphatic capillaries have a thin discontinuousbasement membrane, lack pericyte coverage and often contain endothelial cell gaps that can be invaded by immune cells (or tumor cells). Inaddition, tumor cells and stromal cells in the tumor microenvironment secrete factors that stimulate lymphangiogenesis, the growth of lymphaticendothelial cells and the sprouting of lymphatic capillaries. As a result, many tumors are surrounded by large, hyperplastic, peri-tumoral lymphaticvessels and less frequently are invaded by intra-tumoral lymphatic vessels. Carcinoma cells commonly metastasize through these lymphaticvessels to regional lymph nodes. The presence of metastatic cells in the sentinel lymph node is a prognostic indicator for many types of cancer, andthe degree of dissemination determines the therapeutic course of action. Lymphangiogenesis is currently at the frontier of metastasis research.Recent strides in this field have uncovered numerous signaling pathways specific for lymphatic endothelial cells and vascular endothelial cells.This review will provide an overview of tumor lymphangiogenesis and current strategies aimed at inhibiting lymphatic metastasis. Noveltherapeutic approaches that target the tumor cells as well as the vascular and lymphatic endothelial compartments are discussed.© 2007 Elsevier Inc. All rights reserved.
Keywords: Metastasis; Angiogenesis; Lymphangiogenesis; VEGF-C; VEGFR-3; Theraphy; Inhibitors
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146The cutaneous lymphatic system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146The pathogenesis of a lymphatic metastasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 147
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 148The occurrence of lymph node metastasis in solid tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 148(Tumor-derived) stimulators of lymphangiogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 148Potential therapies and new possibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150Targeting lymphangiogenic ligands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151Inhibiting tumor lymphangiogenesis with soluble receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152Targeting receptors on lymphatic endothelium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152Other strategies to suppress lymphangiogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
Abbreviations: Ang, angiopoietins; COX-2, cyclooxygenase-2; EGF, epidermal growth factor; FGF-2, fibroblast growth factor-2, also called basic fibroblastgrowth factor; FGFR, fibroblast growth factor receptor; HGF, hepatocyte growth factor; IGF, insulin-like growth factor; IGFR, insulin-like growth factor receptor; IL-8, interleukin-8; LEC, lymphatic endothelial cell; NRP, neuropilin; PDGF, platelet-derived growth factor; PDGFR, platelet-derived growth factor receptor; SEMA3F,semaphorin 3F TSP-1-thrombospondin-1; VEC, vascular endothelial cell; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factorreceptor.⁎ Corresponding author. Department of Surgery, Children's Hospital, 12.211 Karp Family Research Laboratories, 1 Blackfan Circle, Boston, MA 02115, USA. Fax:
+1 617 730 0231.E-mail address: [email protected] (D.R. Bielenberg).
0026-2862/$ - see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.mvr.2007.08.006

146 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
Competitive ligands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153Endothelial inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153Inflammatory regulators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154Summary and perspective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
Introduction
The cutaneous lymphatic system
Although the vascular system and the lymphatic system areboth lined with endothelial cells, the two systems differ quitedramatically. The vascular system is a closed, circulatory sys-tem in which the heart pumps blood around the body througharteries, capillaries and veins. In contrast, the lymphatic systemis an open-ended, unidirectional system in which fluid flowsfrom tissues back to the blood stream (Rusznyak et al., 1967).The cutaneous lymphatic system is depicted in Fig. 1A. Initiallymphatics are blind-ended, finger-shaped vessels that protrudeinto the upper dermis near the epidermis. These lymphaticcapillaries are lined with a thin, single layer of endothelial cellsthat form interdigitating, overlapping and end-to-end-type junc-tions (Sauter et al., 1998). Terminal lymphatics drain the in-
Fig. 1. Structural diagram of the cutaneous lymphatic system under physiological andwide luminal capillaries (green color) that extend up near the epidermis (E, peach colextracellular matrix through anchoring filaments. Capillaries possess inter-endothecoverage. In the dermis (D, pink color), capillaries drain into lymphatic vessels calledline) and valves that prevent the reflux of lymph. At the border to the subcutis (Ssurrounded with smooth muscle cells or pericytes (denoted by blue line) that constric(dark brown color) is shown. Tumor cells metastasize through peri-tumoral and intincreased and tumor-associated lymphatic capillaries are dilated and hyperplastic. A feshown with lymphangiogenic vessels as well. Note: this diagram is not drawn exac
terstitial fluid and proteinous exudate that leaks from bloodcapillaries. Lymphatic endothelial cells (LEC) in the capillariesattach to collagen fibers in the dermal extracellular matrix viaanchoring filaments composed of elastic fibers. These fibers areresponsible for increasing luminal diameters of lymphatic ves-sels when interstitial fluid volumes are increased (Swartz andSkobe, 2001). In addition, lymphatic capillaries have an incom-plete basement membrane, lack pericyte coverage and containfrequent gaps between neighboring endothelial cells (Daróczy,1988; Sauter et al., 1998; Schacht et al., 2004). Immune cellssuch as Langerhans cells in the skin can invade these interen-dothelial openings (Stoitzner et al., 2002).
The superficial lymphatic plexus is located in the upperdermis (near the arterial plexus) and includes a network of valve-less, lymphatic capillaries that interconnect to ensure adequatedrainage even in the event that one becomes occluded (Haagen-sen et al., 1972). In general, veins outnumber lymphatics in the
pathological (tumor-bearing) conditions. (A) Interstitial fluid is drained throughor). Capillaries are composed of thin layers of endothelial cells connecting to thelial cell gaps, discontinuous basement membrane, no valves and no pericyteprecollectors that have a continuous basement membrane (denoted by dark greenC, yellow color), precollectors drain into collecting lymphatic vessels that aret to propel the lymph along to regional lymph nodes. (B) An invasive melanomaratumor lymphatic capillaries. Lymphatic capillary density around the tumor isw lymphatic capillaries have sprouted into the tumor. The sentinel lymph node istly to scale.

Table 1Lymphangiogenic factors
Growth factor/cytokine Selected references
VEGF• VEGF-A Nagy et al. (2002), Bjorndahl et al. (2005b),
Hirakawa et al. (2005)• VEGF-C Joukov et al. (1996), Jeltsch et al. (1997),
Skobe et al. (2001b)• VEGF-D Achen et al. (1998), Stacker et al. (2001),
Rissanen et al. (2003)PDGF Cao et al. (2004)HGF Jiang et al. (2005), Kajiya et al. (2005),
Cao et al. (2006)Ang-1 Morisada et al. (2005), Tammela et al. (2005b)Ang-2 Gale et al. (2002)IGF-1/2 Akagi et al. (1998), Bjorndahl et al. (2005a)FGF-2 (bFGF) Kubo et al. (2002), Chang et al. (2004)
147B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
skin, but in certain regions such as the fingers, palms, soles andpubic areas the density of lymphatic capillaries is abundant(Haagensen et al., 1972; Rusznyak et al., 1967). Lymphaticvessels are often found in close proximity to blood vessels, yetthe two systems never intermix within the skin (Rafii and Skobe,2003). In the dermis, lymphatic capillaries drain into largerlymphatic vessels called precollectors. The precollectors have acontinuous basal lamina and contain endothelial cell protrusionsinto the vessel lumen that function as valves to maintain theunidirectional flow of lymph and to protect against reflux. In theskin, valves are present every 2–3 mm (Daróczy, 1988).
A deeper lymphatic plexus is found at the cutis–subcutisboundary, where precollectors drain into thicker lymphatic ves-sels of varying caliber called collectors (Fig. 1A). Collectorshave a continuous membrane, valves, and are surrounded bysmooth muscle cells that contract to propel lymph toward af-ferent vessels of regional lymph nodes (Daróczy, 1988). Thesubcutaneous space contains no lymphatic capillaries, but thelarge collecting lymphatics in this region are found sparselydistributed and follow venous routes (Rusznyak et al., 1967).Lymphatic fluid enters the lymph node through several afferentvessels and usually exits via a single efferent vessel (Fig. 1A).After the lymph is filtered through several lymph nodes, it isdrained into larger lymphatic trunks that lead to the left lym-phatic duct (thoracic duct) or right lymphatic duct and then intothe subclavian veins. In this way, the lymphatic system helps toreturn approximately 10% of the fluid volume that escapes fromthe tissue capillary beds to the vascular system.
The pathogenesis of a lymphatic metastasis
Metastasis, the spread of tumor cells from the primary site todistant organ environments, is the leading cause of death fromcancer. Tumors are heterogeneous in that some tumor foci withinthe parent neoplasm havemore invasive and metastatic propertiesthan others (Fidler, 1990; Fidler, 2002). The metastatic cascadeinvolving the vascular system has been well established (Fidleret al., 2000). But in many solid tumors, metastasis via the lym-phatic system precedes metastasis via the vascular system.
Here, we outline our current understanding and the likely eventsin the pathogenesis of a lymphatic metastasis. Following trans-formation, a tumor cell continues to proliferate and receive itsnutrients and oxygen by diffusion until the nodule reaches appro-ximately 2mm in diameter. In order to grow further, the tumormustrecruit a newblood capillary network from the surrounding tissue, aprocess called angiogenesis (Folkman, 1971). Tumors promoteangiogenesis by secreting molecules from tumor cells and stromalcells that attract vascular capillaries and stimulate their sprouting.Many of the same molecules that induce vascular endothelial cell(VEC) growth also stimulate LEC growth (Table 1) (McColl et al.,2005; Van der Auwera et al., 2006). In some patients, tumor-derived factors stimulate intra-tumoral lymphatic vessels (Dadras etal., 2003;Maula et al., 2003;Kyzas et al., 2005b; Sipos et al., 2004),while most tumors induce hyperplastic peri-tumoral lymphaticvessels (depicted in Fig. 1B). The lymphatic capillaries surroundingthe tumor can reach sizes of 10–50 times that of a normal lymphaticcapillary. This increased lumen size may be the result of dilation,
LEC proliferation, high tumor-induced interstitial pressure, or theconsequence of tumor-secreted extracellular matrix molecules thatpull on the lymphatic focal adhesions keeping them in a constantstate of openness.
Tumor cells capable of invading the host stroma mayencounter these hyperplastic lymphatic capillaries as well asnormal lymphatic capillaries. Terminal lymphatics do not have acontinuous basement membrane and contain intercellular gapsthat allow for fluid drainage and the infiltration of immune cellssuch as dendritic cells and Langerhans cells. These structuralcharacteristics may make it easier for a tumor cell to enter thelymphatic system than the blood system (Sleeman, 2000). Thebasement membrane of tumor-associated lymphatic capillarieslacks laminin and collagen XVIII (Skobe et al., 2001b) and iscompletely lacking in some areas; therefore, tumor cells maynot require as many invasive properties to invade the lymphaticsystem. In addition, LEC secrete chemotactic agents that attractmalignant tumor cells toward areas of high lymphatic vesseldensity (Shields et al., 2007). Tumor cells must detach in orderto be carried away in the lymph fluid, likely as small emboli,toward the afferent vessels of the sentinel lymph node. Fewerthan 0.1% of tumor cells entering the blood circulation actuallyform metastases (Fidler, 1970), while dissemination throughthe lymphatic system appears much more efficient (Haagensenet al., 1972). The high flow rate and high serum concentrationsin the blood stream are often toxic to tumor cells, whereas therelatively passive, low shear stress of the lymph fluid may allowfor tumor cell survival (Sleeman, 2000).
Just as the lymph node acts as a filter for pathogens andimmune cells, it also filters tumor cells. This filter function mayinitially protect the patient and prevent the early disseminationof tumor cells throughout the body. Hematogenous metastasisrequires that the tumor cell extravasate through the vascularcapillary out into the new organ environment, while lymphaticmetastasis may not require such extravasation (Sleeman, 2000).The lymph node may simply concentrate all shed tumor cellsinto the same location in the reticular fibers of the marginalsinus where the emboli get trapped and subsequently proliferatein situ. The pooling of tumor cells in one site in the parenchyma

148 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
of the node likely promotes their survival and further growth.Eventually, the entire node may become replaced by tumor.Tumor cells may escape from the efferent vessels of the draininglymph node to the next lymph node or to the thoracic duct andinto the venous blood system for dissemination throughout thebody. Alternatively, tumor cells may invade the blood vesselswithin the lymph node itself and metastasize to distant organs(Haagensen et al., 1972; Tobler and Detmar, 2006).
Discussion
The occurrence of lymph node metastasis in solid tumors
Tumor cell metastasis to regional lymph nodes often marksthe first step in tumor cell progression (Table 2). In general,carcinomas metastasize through the lymphatic system moreoften than sarcomas. In fact, carcinoma in the large intestinemetastasizes almost exclusively via the lymphatics. Some car-cinomas also metastasize via the vascular system. In breastcancer, the metastases usually result from early lymphatic dis-semination followed by extensive spread into the vascular sys-tem in more advanced disease stages (Haagensen et al., 1972;Hess et al., 2006). Shortly after tumor formation, gastric carci-nomas metastasize through both routes. Even within a certaintype of cancer, location of the primary neoplasm can influencethe route of metastasis. For instance, squamous cell carcinoma(SCC) in the lung metastasizes early through both hematoge-nous and lymphogenous paths (Haagensen et al., 1972), whileSCC in the skin or cervix metastasizes late and mainly tosentinel lymph nodes (Weinberg et al., 2007).
Table 2Solid tumors that metastasize to lymph nodes
Tumor type Selected references
CommonBladder carcinoma Shariat et al. (2006), Jones et al. (2005)Breast carcinoma Chen et al. (2006), Hess et al. (2006)Cervical carcinoma Pandit-Taskar (2005)Colorectal carcinoma Chen et al. (2006), Hess et al. (2006)Endometrial carcinoma Sohaib et al. (2007)Esophageal carcinoma Hatakeyama et al. (2006)Head and Neck carcinomas Chen et al. (2006)Hepatocellular carcinoma Uka et al. (2007)Melanoma Chen et al. (2006), Lin et al. (2005)Non-small cell lungcarcinoma
Hess et al. (2006), Renyi-Vamos et al. (2005)
Ovarian carcinoma Onda et al. (1996)Pancreatic ductualadenocarcinoma
Sipos et al. (2005),Von Marschall et al. (2005)
Prostate carcinoma Morisawa et al. (2006)Thyroid carcinoma a Rodriguez et al. (2000), Scollo et al. (2003)
Less commonGastric Carcinoma Saito et al. (2007)Renal cell carcinoma Denzinger et al. (2007)Testicular carcinoma b Jones et al. (2000)a Papillary thyroid carcinoma, medullary thyroid carcinoma and anaplastic
thyroid carcinoma metastasize to sentinel lymph nodes.b Testicular carcinoma has a near 100% cure rate, but the primary site of
relapse is the para-aortic lymph node.
Head and neck carcinomas frequently metastasize to lymphnodes (Table 2). Whether this is due to the fact that these tumorsexpress high levels of lymphatic growth factors such as VEGF-Cor VEGF-D (discussed below) or whether this is partly due tostructural considerations since this region contains 300 lymphnodes is unclear. Conversely, liposarcoma, fibrosarcoma andosteosarcoma seldom metastasize to lymph nodes (Fong et al.,1993). Two possible explanations may account for the lack oflymphatic metastasis in sarcomas: their low expression of lym-phatic stimulators such as VEGF-C or their secretion of endo-genous lymphangiogenic inhibitors. In fact, T241 fibrosarcomacells growing subcutaneously in a syngeneic mouse could pre-vent lymphangiogenesis at a distant site (cornea) in that mouse,presumably by the production of a systemic inhibitor (Changet al., 2002). However, when T241 fibrosarcoma cells weretransfected with VEGF-C, this inhibition was overridden astumors readily metastasized to regional lymph nodes (Paderaet al., 2002).
Predicting the metastatic potential of a patient's tumor is achallenging task. Evidence of tumor cells in a lymph node isoften the first indicator of cancer spread. Lymph node meta-stasis is correlated with an increased risk of distant metastasisand a poor clinical outcome (Chen et al., 2006). For instance,75% of prostate cancer patients with lymph node metastasis atdiagnosis will possess bone metastasis in 5 years (Smith et al.,1983). According to the sentinel lymph node theory, tumor cellsinvade lymph nodes in sequence with the closest or draininglymph node (called the sentinel node) first, followed by the nextnode in line with the drainage flow, etc. (Schauer et al., 2005).Sentinel lymph node biopsy or lymphadenectomy is performedfor many cancers, and the absence of tumor cells in the sentinelnode predicts that other downstream nodes will likely be free ofmetastasis as well (Chen et al., 2006). Tumor foci in the lymphnode are categorized as micrometastases (0.2 mm to ≤2 mm) ormacrometastases (N2 mm). While isolated tumor cells (forexample, single keratin-positive tumor cells) in the lymph nodeare not currently considered as micrometastases, and theselymph nodes are usually designated as “tumor-free” (Chen et al.,2006). Metastasis to any lymph node other than the regionalnode is considered a distant metastasis.
(Tumor-derived) stimulators of lymphangiogenesis
Not all tumorsmetastasize to lymph nodes. Understanding themolecular cues that cause some tumors to induce lymphangio-genesis while others do not may result in the discovery andapplication of new strategies for disease prevention. For thisreason, it is important to study the factors that regulate lymphaticmetastasis (Table 1). The first proteins identified as stimulators oflymphangiogenesis were VEGF-C and VEGF-D (Joukov et al.,1996; Achen et al., 1998). Both aremembers of the VEGF familyand bind VEGFR-3, inducing proliferation and migration ofLECs. Knockout models for VEGF-C fail to form initial lym-phatic vessels during embryogenesis, indicating that VEGF-C isa vital factor in lymphatic development (Karkkainen et al., 2004).VEGF-D, on the other hand, is not required for lymphatic vesselformation during embryogenesis (Baldwin et al., 2005) but is the

149B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
strongest inducer of lymphangiogenesis in the adult when givenvia adenoviral delivery into mouse skeletal muscle (Rissanenet al., 2003).
VEGF-C or VEGF-D can stimulate tumor lymphangiogen-esis (Skobe et al., 2001a,b; Stacker et al., 2001; Karpanen et al.,2001; Mattila et al., 2002; He et al., 2002) and increase themetastatic spread of tumor cells to sentinel lymph nodes (Skobeet al., 2001b; Stacker et al., 2001; Mandriota et al., 2001; Mattilaet al., 2002; Krishnan et al., 2003). VEGF-D expression cor-relates with lymph node metastasis in many human cancersincluding invasive breast, ovarian, cervical, undifferentiatedgastric and lung adenocarcinoma (Renyi-Vamos et al., 2005;Tammela et al., 2005a; Hess et al., 2006). VEGF-C expressioncorrelates with lymphatic vessel invasion or lymph node meta-stasis in human breast, cervical, colon, prostate, endometrial,esophageal, gall bladder, ovarian, pancreatic and non-small celllung carcinomas (Ristimaki et al., 1998; Swartz and Skobe,2001; Stacker et al., 2002; Tammela et al., 2005a). On the otherhand, VEGF-C expression did not correlate with lymph nodemetastasis in neuroblastoma tumors, which typically lack lym-phatic vessels (Tammela et al., 2005a). VEGF-C expression alsocorrelates with poor prognosis or poor patient survival in manytumors, especially breast, cervical, esophageal and non-smallcell lung cancer (Tammela et al., 2005a).
In some tumors there appears to be a lymphangiogenic switch.Van Trappen and colleagues (2003) report that pre-cancerous cellsin the cervix (CIN-1 and CIN-2) seldom express VEGF-C andVEGF-D, but pre-invasive carcinoma in situ lesions (CIN-3)upregulate VEGF-C/D expression. Presumably, following thisswitch, tumor cells recruit and invade lymphatic capillaries andtravel to lymph nodes. The increase in lymph node metastasiscaused by VEGF-C may be due in part to its ability to stimulateLEC proliferation thereby increasing the size of tumor-associatedlymphatic vessels and increasing the chance that a tumor cell willcome in contact with a LEC. Other mechanisms may include theupregulation of chemokines by VEGF-C that attract immune cellsand tumor cells toward the lymphatic capillary (Shields et al.,2007). In addition, VEGF-C is a permeability factor that causesblood vessels to leak fluid thereby raising the interstitial pressure,dilating lymphatic capillaries and forcing a greater flow of fluid tolymph nodes (Hoshida et al., 2006). Tumor-secreted VEGF-C hasrecently been shown to act systemically by inducing lymphangio-genesis in the sentinel lymph node even prior to tumor cell invasion(Hirakawa et al., 2007). This may prepare the lymph node fordisseminated cells to come and may facilitate the further spread ofcells to other nodes (Tobler and Detmar, 2006; Harrell et al., 2007).
When fully processed, VEGF-C and VEGF-D, can also bind toVEGFR-2. VEGFR-2 is expressed on both VECs and LECs(Saaristo et al., 2002). In fact, high expression of VEGF-C orVEGF-D results in increased angiogenesis in addition to increasedlymphangiogenesis in some models (Skobe et al., 2001a; Robertset al., 2006; Achen et al., 2002). VEGF-C and VEGF-D also bindto a non-tyrosine kinase receptor called Neuropilin 2 (NRP2)(Karpanen et al., 2006a).NRP2 acts as a co-receptor withVEGFR-2 and VEGFR-3 (Soker et al., 1998; Favier et al., 2006). NRP2knockout mice have decreased numbers of lymphatic capillariesand veins, but surprisingly do not show edema (Yuan et al., 2002).
VEGF-A is a potent inducer of tumor angiogenesis. Recentstudies demonstrate that tumor-derived VEGF-A can also in-crease intra- and peri-tumoral lymphangiogenesis and increaselymphatic metastasis (Bjorndahl et al., 2005b; Hirakawa et al.,2005). However, in 293EBNA tumors VEGF-A over-expressionwas insufficient to induce lymphangiogenesis whereas VEGF-Deffectively stimulated lymphangiogenesis and lymph node me-tastasis (Stacker et al., 2001). Dramatic lymphangiogenesis isfound when VEGF-A (165 isoform) is delivered to mice usingadenoviral strategies. Surprisingly, the newly formed lymphaticsdo not regress for N1 year although the adenoviral VEGF-A isdepleted in approximately 2 weeks (Nagy et al., 2002). VEGF-Aalso induces lymphangiogenesis in other non-tumor murinemodels including adenoviral delivery to skeletal muscle, K14-VEGF-A transgenic skin, UV-B irradiation and corneal pelletmodels (Rissanen et al., 2003; Kunstfeld et al., 2004; Kajiyaet al., 2006; Rogers et al., 2003). The effects of VEGF-A onlymphangiogenesis may be direct through VEGFR-2 and NRP2expression on LECs or indirect as VEGF-A causes upregulationof VEGF-C/D in inflammatory cells (Cursiefen et al., 2004).
Most tumors express fibroblast growth factor-2 (FGF-2), alsocalled basic FGF (for reviewAbuharbeid et al., 2006). FGF-2 is apowerful mitogen for VECs and also stimulates the growth ofLECs (Chang et al., 2004). Although there are currently noreports linking tumor-derived FGF-2 with lymphangiogenesisand lymph node metastasis, injection of FGF-2 protein duringthe early phases of tumor progression stimulated neovascular-ization and metastasis (Tsunoda et al., 2007). In addition, mousecorneal lymphangiogenesis is strongly stimulated with FGF-2(Kubo et al., 2002; Chang et al., 2004). Interestingly, low-doseFGF-2 pellets can induce lymphatic vessel sprouting in theabsence of blood vessel sprouting (Chang et al., 2004, 2002).FGF-2 may directly affect the growth of lymphatic vessels sinceLEC express FGFR-3 (Shin et al., 2006). Alternately, FGF-2upregulates VEGF-C and VEGF-D in the cornea (Kubo et al.,2002; Chang et al., 2004) and upregulates VEGF-A in tumorstroma (Tsunoda et al., 2007).
The angiopoietins (Ang) may also stimulate lymphaticspartly through VEGFR-3. Two angiopoietins are known, Ang-1and Ang-2, and both play a role in vascular development incombination with VEGF-A (Sato et al., 1995). Ang-1 (adeno-virus) promotes LEC proliferation, lymphatic vessel enlarge-ment and lymphatic vessel sprouting in vivo in adult mouse ears(Tammela et al., 2005b). Inhibitors of the VEGF-C/VEGFR-3pathway block Ang-1-stimulated lymphangiogenesis (Tammelaet al., 2005b). Alternatively, Ang may affect lymphangiogenesisdirectly since embryonic and adult LECs express the tyrosinekinase angiopoietin receptor, Tie2 (Morisada et al., 2005; Tam-mela et al., 2005b). Ang-1 protein stimulates the growth of LECin vitro and in vivo in a mouse corneal pocket model (Morisadaet al., 2005), and genetically engineered mice expressing Ang-1in basal keratinocytes have hyperplastic dermal lymphaticvessels (Tammela et al., 2005b). Transgenic mice deficient inAng-2 expression fail to form large collecting lymphatic vesselsand have defective patterning of small lymphatic capillaries,possibly indicating that Ang-2 functions in the maturation oflymphatic vessels (Gale et al., 2002). Although the majority of

150 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
tumors show an increase in Ang-1 and Ang-2 expression (forreview Tait and Jones, 2004), a direct correlation between eitherof these factors and tumor lymphangiogenesis is lacking.
Pathways other than the classical VEGF-C/VEGFR-3 signaltransduction can stimulate lymphangiogenesis as well. Theseinclude the platelet-derived growth factor (PDGF)/PDGFR path-way, the hepatocyte growth factor (HGF)/c-met pathway and theinsulin-like growth factor (IGF)/IGFR pathway. PDGF-AA,PDGF-AB and PDGF-BB induce mouse corneal lymphangio-genesis, with PDGF-AA being the least effective stimulator (Caoet al., 2004). Mouse fibrosarcoma-derived PDGF-BB inducedperi- and intra-tumoral lymphangiogenesis, possibly throughactivation of the PDGFR and promoted lymphatic metastasis(Cao et al., 2004). Recently, HGF was identified as a lymph-angiogenic factor. In vitro, HGF stimulates LEC to proliferate,migrate and form tube-like structures (Kajiya et al., 2005). HGFdid not upregulate VEGF-C or VEGF-D in LEC, and thereforethe effect of HGF was assumed to be directly through itsreceptor, c-met. On the other hand, corneal mouse models de-monstrate lymphangiogenesis toward HGF-releasing pellets, butthe neo-lymphatic vessels did not express c-met. This cornealHGF-stimulated lymphangiogenesis could be partially blockedwith soluble VEGFR-3, indicating an indirect effect of HGF(Cao et al., 2006). HGF was associated with tumor lymphangio-genesis in transgenic mammary tumors (Cao et al., 2006). In-
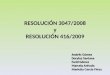
Fig. 2. Human melanoma (A, C) and human melanoma (A375SM) xenograft (B, D)and eosin. (C) Human podoplanin (D2-40 antibody, Signet Laboratories) staining (broD=dermis.
fusion of rhHGF into tumors or co-injection of a fibroblast cellline producing HGF with tumor cells resulted in increased tumorlymphangiogenesis (Jiang et al., 2005). IGF-1 and IGF-2 sti-mulate the proliferation and migration of primary LECs thatexpress IGFR-1 and IGFR-2 (Bjorndahl et al., 2005a). In vivo,IGF-1 and IGF-2 could both stimulate corneal lymphangiogen-esis independently (Bjorndahl et al., 2005a). Although the effectof IGF-1 on tumor lymphangiogenesis has yet to be shown,tumor-secreted IGF-1 may indirectly affect LEC by the upregu-lation of VEGF-A and activation of VEGFR-2 similarly to theway it affects VEC (Akagi et al., 1998).
Potential therapies and new possibilities
The tumor-associated lymphatic endothelium represents anovel target for cancer therapy. Metastasis to lymph nodesresults from tumor cell invasion into lymphatic capillaries.Lymphangiogenesis is documented in numerous animal modelsand in many human cancers as well. For many neoplasms, thelymphatic system is the primary and only route of metastasis.The existence and functionality of intra-tumoral lymphaticvessels has been vehemently debated (Padera et al., 2002;Schneider et al., 2006), but the fact that many tumors aresurrounded with grossly enlarged lymphatic vessels cannot bedenied (Fig. 2). Large peri-tumoral lymphatic vessels may result
are surrounded with large peri-tumoral lymphatics (arrows). (A, B) Hematoxylinwn color). (D) Murine podoplanin (Reliatech) staining (brown color). T= tumor,

Table 3Potential targets and therapeutic strategies for anti-lymphangiogenesis
Target Strategy Anti-
Angiogenesis Lymphangiogenesis Tumor
LigandsHGF Antibody to
HGFa+ + +
NK4 + + +VEGF-A Antibody to
VEGF-A++ +
SolubleVEGFR-2
++ + +/−
VEGF trap(Soluble R1/R2)
++ +
Soluble NRP1 + +Soluble NRP2 a + +Semaphorin 3F + + +
VEGF-C Antibody toVEGF-Ca
+ ++
SolubleVEGFR-3
+ ++
Soluble NRP2 a + ++Semaphorin 3F + + +
VEGF-D Antibody toVEGF-D
+ ++
SolubleVEGFR-3
+ ++
Soluble NRP2 a + ++Receptorsc-met Antibody to
c-met a+ ++
c-met kinaseinhibitors
+ ++
Neuropilin 2 Antibody toNRP2 a
+ +
Semophorin 3F + + +PDGFRα/β Antibody to
PDGFRa+ + ++
PDGFR kinaseinhibitors
+ + ++
VEGFR-3 Antibody toVEGFR-3
+ ++
VEGFR-3 kinaseinhibitors
+ ++
VEGFR-2 Antibody toVEGFR-2
++ + +
VEGFR-2 kinaseinhibitors
++ + +
Integrins Antibody tointegrin-α1/α2
+
OthersAngiostatin ++ +COX-2inhibitors
+ + +
Endostatin ++ +Glucocorticoids + +Interferon α/β ++ + ++Platelet-factor 4 ++ +Semaphorin 3F + + +
a These strategies have not yet been reported for anti-lymphangiogenesis.
151B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
from (1) pre-existing capillaries that become highly dilated dueto increased interstitial pressure, (2) pre-existing capillaries thathave increased their luminal diameter by proliferation of LECs(hyperplasia) and (3) neovascularization or sprouting of existingvessels toward a stimulus (tumor) that results in the increasedsize or density of vessels in the vicinity. Regardless of theorigin, these vessels represent an increased opportunity fortumor cells to enter the lymphatic system and the increasedchance of systemic dissemination. Therapies targeted towardthe tumor-associated lymphatic compartment may inhibit meta-stasis if given early and may prevent further spread of tumorcells even if given at later time points.
Angiogenesis inhibitors have been intensely studied over thelast decades. Currently, there are more than twenty-five anti-angiogenic drugs in clinical trials (Folkman, 2004; Morabitoet al., 2006). The recent FDA-approval of the first exclusivelyanti-angiogenic agent, bevacizumab (Avastin™), a humanizedmonoclonal antibody to VEGF-A to be used in combinationwith chemotherapy for the treatment of advanced stage coloncancer, has proven beneficial to patients and pivotal for the fieldof vascular biology (Slevin and Payne, 2004). This clinical“proof of concept” has paved the way for other novel anti-vascular strategies and opened a new frontier in cancer therapy(Folkman, 2004). Lymphangiogenesis research has lagged be-hind angiogenesis, but the discovery of new lymphatic markersand an increased understanding of the growth factor signalingpathways in LEC have poised scientists to begin testing manypotential anti-lymphangiogenic therapeutic strategies (Table 3).New trials will be needed to validate these pre-clinical studiesand determine their medicinal significance.
Targeting lymphangiogenic ligands
VEGF-A is a major tumor-derived angiogenic factor, whileVEGF-C is a major tumor-derived lymphangiogenic factor.Indeed, many other growth factors (FGF-2, Ang-1, VEGF-A,IGF-1, HGF) stimulate lymphangiogenesis indirectly throughVEGF-C. VEGF-C is secreted by other cells in the tumor mic-roenvironment besides neoplastic cells including fibroblasts,macrophages, platelets and keratinocytes (Skobe and Detmar,2000; Sleeman, 2006). VEGF-C not only induces the hyper-plasia of peri-tumoral vessels, but also increases the volumetricflow rate of fluid in lymphatics that results in the increaseddelivery of tumor cells to the lymph node (Hoshida et al.,2006). In fact, tumors over-expressing VEGF-C were found todeliver 200-fold more tumor cells to the regional lymph nodeand increase lymph node metastasis 4-fold (Hoshida et al.,2006). Since angiogenic inhibitors targeting VEGF-A (ie., anti-bodies, kinase inhibitors and soluble receptors) have proveneffective (for reviewManley et al., 2002), strategies targeting theVEGF-C pathway may prove equally effective against tumorlymphangiogenesis.
Most anti-lymphangiogenic pre-clinical studies to date havetargeted the VEGF-C/VEGF-D/VEGFR-3 signaling pathway(Table 3). These strategies have included antibodies to VEGF-D,knockdown of VEGF-C using RNAi and soluble receptors, allaimed to neutralize the effects of these ligands. VD1, a mono-
clonal VEGF-D antibody, inhibited binding of VEGF-D to bothVEGFR-2 and VEGFR-3 (Achen et al., 2000). This antibodyblocked lymphatic spread of VEGF-D over-expressing human293EBNA cells in immunocompromised mice (Stacker et al.,

152 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
2001). The down-modulation of VEGF-C with stable RNAitransfection in murine breast cancer cells results in reducedtumor lymphangiogenesis and lymph node metastasis (Chenet al., 2005). In a prostate cancer model, VEGF-C silencingcompletely abolished intra-tumoral lymphatic vessels when cellswere implanted subcutaneously, but reduced lymphatic vesseldensity by only 50% when implanted orthotopically (Wonget al., 2005). The reduction of lymphatic vessels in the orthotopicmodel was insufficient to inhibit the incidence of lymph nodemetastasis. These results may indicate that stromal cells ofdifferent organ environments may differ in their VEGF-C ex-pression. Additionally, peri-tumoral vessels may be sufficientfor tumor cell invasion and metastasis in some cases. It isimportant to note that RNAi strategies have not yet been ap-proved for clinical use in human patients.
Inhibiting tumor lymphangiogenesis with soluble receptors
Targeting an individual ligand (e.g.,VEGF-C) can neutralizeits effects on several receptors (e.g., VEGFR-3, VEGFR-2 andNRP2), but will not affect the ability of another ligand (e.g.,VEGF-D) to stimulate these same receptors. Targeting a specificreceptor (e.g., VEGFR-2) with a kinase inhibitor or blockingantibody will inhibit its activation by multiple ligands (e.g.,VEGF-C, VEGF-D or VEGF-A), but will not affect the abilityof these ligands to stimulate another receptor (such as NRP2 orVEGFR-3). Soluble receptors may prove more effective sincethey bind multiple ligands (for example, sVEGFR-2 bindsVEGF-A, VEGF-C and VEGF-D) and compete for bindingwith multiple receptors (for example, sVEGFR-2 may sequesterVEGF-C away from VEGFR-2, VEGFR-3 and NRP2).
sVEGFR-3 proteins and adenoviral constructs have been themost widely used strategy for targeting tumor lymphangiogen-esis. sVEGFR-3 globulin protein inhibited lymphangiogenesisand lymph node metastasis in rat and human breast cancermodels (Karpanen et al., 2001; Krishnan et al., 2003). sVEGFR-3protein was effective even when the tumor cells were engi-neered to express high levels of VEGF-C (Karpanen et al.,2001). Blocking lymph node metastasis in breast tumors withsVEGFR-3 protein inhibited subsequent distant lung metastasesas well (Krishnan et al., 2003). The same strategy did not inhibitdistant metastases in a lung carcinoma model (He et al., 2002).These results may indicate that sVEGFR-3 strategies may bemore useful in cancers like breast and prostate carcinomas thatinitially metastasize to lymph nodes and later to distant sites.
The mode of delivery of sVEGFR-3 may influence its the-rapeutic potential. Tumor cells transfected with sVEGFR-3suppressed lymph node metastasis by 66% (from 12/12 lymphnode metastases in controls to 4/12 lymph node metastases intransfected mice), while sVEGFR-3 given systemically in anadenovirus completely inhibited lymph node metastasis (from11/14 metastases in Adeno-LacZ mice to 0/28 lymph nodemetastases in Adeno-sVEGFR-3 mice) (He et al., 2002). At thistime, transfection or viral therapies may not be desirable forhuman patients, but sVEGFR-3 given as a protein may be aviable strategy. sVEGFR-3 protein inhibits lymphangiogenesisin a dose-dependent manner with the most effective dose
depending on the VEGF-C levels in the tumor (Karpanen et al.,2001, 2006b; Krishnan et al., 2003; He et al., 2005). sVEGFR-3therapy can indirectly inhibit multiple stimulators of lymphan-giogenesis including HGF, FGF-2, IGF-1 and Ang-1, which areregulated by VEGF-C (Bjorndahl et al., 2005a; Cao et al., 2006;Chang et al., 2004; Tammela et al., 2005b).
The timing of sVEGFR-3 delivery is also quite important.When sVEGFR-3-Fc adenovirus or adeno-associated virus wasgiven prior to tumor cell inoculation or early in tumor prog-ression, lymphangiogenesis and lymph node metastasis couldbe suppressed in several tumor models including melanoma,prostate, renal cell and lung carcinoma (He et al., 2005; Linet al., 2005). When systemic sVEGFR-3 therapy was started toolate, tumor cells had already reached regional lymph nodes andmetastasis was not affected (He et al., 2005).
Targeting receptors on lymphatic endothelium
To date, nearly all attempts to target receptors on the lymphaticendothelium of tumors have been via VEGFR-3. VEGFR-3 wasthe first lymphatic-specific marker identified (Kaipainen et al.,1995). Blocking antibodies that target the ligand binding domainof murine VEGFR-3 inhibit tumor lymphangiogenesis (Shimizuet al., 2004; Hoshida et al., 2006; Pytowski et al., 2005; Robertset al., 2006; Laakkonen et al., 2007), FGF-2 induced corneallymphangiogenesis (Kubo et al., 2002), spontaneous corneallymphangiogenesis in corn1 mice (Cursiefen et al., 2005) andUV-B-induced (VEGF-A-mediated) lymphangiogenesis (Kajiyaet al., 2006). Early intervention (7 days after tumor cell injection)with VEGFR-3 antibodies reduced lymphatic vessel density andinhibited lymph node metastasis in highly metastatic gastriccarcinomas (Shimizu et al., 2004). Peri-tumoral lymphatic vesselhyperplasia was also reduced with VEGFR-3 antibodies. Thesmaller vessel area resulted in fewer GFP-labeled tumor cellsdelivered to regional lymph nodes (Hoshida et al., 2006; Robertset al., 2006).
VEGFR-3 is expressed by tumor-associated blood vessels aswell as lymphatic blood vessels (Clarijs et al., 2002; Partanenet al., 1999). VEGFR-3 antibodies inhibited tumor angiogenesisand therefore, primary tumor growth in some models (Kubo etal., 2000; Roberts et al., 2006; Laakkonen et al., 2007). Treatedtumors showed reduced microvessel density and in some casesmicro-hemorrhaging throughout the tumor. VEGF-C can inducetumor angiogenesis via VEGFR-2 as well as VEGFR-3 on tumorendothelial cells and a blocking antibody to VEGFR-2, calledDC101, was also effective at inhibiting VEGF-C-induced tumorangiogenesis (Kadambi et al., 2001; Roberts et al., 2006). LECsexpress VEGFR-2, although preferentially on peri-tumorallymphatics and less so on intra-tumoral lymphatics; andaccordingly, DC101 was able to decrease tumor lymphangio-genesis (Roberts et al., 2006). In addition, DC101 was found toinhibit lymphatic vessel regeneration in cutaneous wounds inK14-VEGF-A transgenic mice (Hong et al., 2004). Lymphan-giogenesis in cutaneous delayed-type hypersensitivity reactions,however, could not be inhibited with VEGFR-2 antibodies aloneand required the combination of both VEGFR-2 and VEGFR-1antibodies (Kunstfeld et al., 2004).

153B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
When comparing VEGFR-3 versus VEGFR-2 antibodies,VEGFR-3 antibodies were more effective at inhibitingregional lymphatic metastases and distant metastases thanVEGFR-2 antibodies (Roberts et al., 2006). VEGFR-2antibodies were more effective at inhibiting tumor growthand angiogenesis. Interestingly, even though tumor volumewas reduced by 84% and tumor blood vessel area wasdecreased by 71% in the anti-VEGFR-2 treated group, thesesmall weakly vascularized tumors still managed to metastasizeto regional lymph nodes in 8/10 mice compared with 10/10mice in the controls (Roberts et al., 2006). These resultsunderscore the importance of blocking lymphangiogenesis inaddition to angiogenesis. The combination of both antibodieswas even more effective at inhibiting metastasis than eitherantibody alone (Roberts et al., 2006). A diabody, a bi-specificantibody that recognizes both VEGFR-2 and VEGFR-3 andcan block the interaction of VEGF-C/VEGFR-2, VEGF-C/VEGFR-3 and VEGF-A/VEGFR-2, was recently produced byImclone (Jimenez et al., 2005), but the efficacy of thisantibody at inhibiting metastasis or prolonging survival hasnot been reported yet. Strategies such as these that utilizeboth anti-angiogenic and anti-lymphangiogenic approachesmay be the most potent methods for blocking the deadlyspread of cancer cells (see Table 3).
Using RNA microarray technology, investigators havecompared the expression profiles of VECs and LECs (Hirakawaet al., 2003; Podgrabinska et al., 2002). VECs express α5 andαv integrins, whereas cultured LECs express α 1 and α 2integrins (which partner with β1 subunits). Lymphatic capil-laries have an incomplete basement membrane and lie in closecontact to interstitial collagen. VEGF-A enhances the expres-sion of collagen type I binding subunits, α1 and α2, on culturedLECs (Hong et al., 2004; Senger et al., 1997). Monoclonalantibodies targeting α1 and α2, used in combination, inhibitedphysiologic lymphangiogenesis in a wound healing model andinhibited pathologic lymphangiogenesis in a skin tumor model(Hong et al., 2004).
Small compounds have been used to block the kinase do-mains of cell surface receptors. These kinase inhibitors gen-erally target one or more receptors specifically but can havenon-specific effects on other receptors. Many kinase inhibitorsare currently in clinical trials. Several compounds inhibit theactivities of VEGF receptors including Semaxanib (SU5416),Sumitnib (SU11248), Vatalanib (PTK/ZK), Sorafenib (BAY 43-9006), Recentin (AZD2171), SU6668, AG-013736, MAZ51and CEP-7055 (for a review, see Ahmed et al., 2004; Baka et al.,2006; Morabito et al., 2006). The relative effects of theseinhibitors on tumor lymphangiogenesis versus tumor angio-genesis are unclear. Kinase inhibitors targeting the c-met recep-tor, the PDGFR and the IGFR may target LECs in addition totumor cells (Table 3).
Other strategies to suppress lymphangiogenesis
Many different strategies are being explored to target tumorlymphangiogenesis and prevent lymphatic metastases. Thesepotential therapies include using competitive ligands of lym-
phangiogenic stimulators, inflammatory regulators and endoge-nous inhibitors of angiogenesis/lymphangiogenesis. A novelapproachmay be to select those inhibitors that target both vascularand lymphatic endothelial cells as well as tumor cells (Table 3).
Competitive ligands
Semaphorin 3F (SEMA3F) is a competitive ligand of VEGF-A and VEGF-C for Neuropilin 2 (NRP2). NRP2 is a co-receptorfor VEGF-A with VEGFR-2 and a co-receptor for VEGF-Cwith VEGFR-3. NRP2 is also a co-receptor for SEMA3F withplexins, a family of transmembrane receptors involved in neu-ronal guidance. In addition to competing for VEGF binding,SEMA3F induces repulsion of NRP2-expressing VECs andLECs (Bielenberg et al., 2004). Human melanoma cells over-expressing SEMA3F have reduced microvessel density and acomplete inhibition of lymph node metastasis and lung meta-stasis. SEMA3F-expressing tumors have no intra-tumoral lym-phatic vessels and reduced peri-tumoral lymphatic vessel area ascompared to control A375SM tumors that have large peri-tumoral lymphatic vessels (Fig. 2) and intra-tumoral lymphaticvessels (manuscript submitted, Bielenberg and Klagsbrun). TheSEMA3F chromosomal loci, 3p21.3, is often deleted in lungcancer (Roche et al., 1996; Sekido et al., 1996; Xiang et al.,1996) and therefore SEMA3F has been suggested to act as atumor suppressor. SEMA3F protein may be a novel therapycapable of inhibiting angiogenesis, lymphangiogenesis, tumor-igenicity and metastasis (Bielenberg et al., 2006).
NK4 is a competitive inhibitor of HGF binding to c-met andwas effective at inhibiting HGF-induced tumor angiogenesisand tumor lymphangiogenesis (Jiang et al., 2005; Kuba et al.,2000). NK4 may also reduce neovascularization independentlyof HGF as it decreased VEGF- and FGF-stimulated prolifera-tion and migration of EC in vitro as well (Kuba et al., 2000).
Endothelial inhibitors
Surprisingly few studies have compared the endogenous orclassical angiogenesis inhibitors in lymphangiogenesis models.Some in vitro studies do suggest that these compounds mayaffect both endothelial cell compartments. For example, Shaoand colleagues reported that angiostatin, endostatin and platelet-factor 4 could inhibit LEC proliferation (MTT assay) and mig-ration (scratch assay) in a dose-dependent manner (Shao andChi, 2005; Shao and Xie, 2005). On the other hand, thesecompounds need to be examined in vivo to truly establish theirpotency. For instance, thalidomide inhibited LEC growth in vitro(Shao and Xie, 2005) but was inefficient at inhibiting FGF-2induced corneal lymphangiogenesis (Chang et al., 2004).
Interferon (IFN) α and β have been shown to regress cuta-neous hemangiomas in children and to block tumor angiogen-esis and metastasis in murine models by down-regulating FGF-2and matrix metalloproteinases (Ezekowitz et al., 1992; Ezeko-witz et al., 1995; Dinney et al., 1998; Bielenberg et al., 1999;Dong et al., 1999). FGF-2 injection during the initial phase oftumorigenesis increases tumor growth and metastasis (Tsunodaet al., 2007). Tumor-secreted FGF-2 may also stimulate tumor

154 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
lymphangiogenesis. IFNα inhibits LEC growth and inducesapoptosis in vitro (Shao and Liu, 2006), but its effect on tumorlymphangiogenesis remains to be seen.
Thrombospondin-1 (TSP-1) is a competent angiogenesisinhibitor, and tumors resulting from chemical-induced carcino-genesis in K14-TSP-1 mice have reduced microvessel density(Hawighorst et al., 2002). Lymphangiogenesis and lymph nodemetastasis, on the other hand, was not diminished in tumors fromTSP-1 transgenic mice possibly due to the fact that cutaneouslymphatic capillaries lack CD36, one of the TSP-1 receptors.
Inflammatory regulators
Cyclooxygenase-2 (COX-2) expression correlates withVEGF-C expression and lymph node metastasis in numeroushuman cancers including lung adenocarcinoma, head and necksquamous cell carcinoma, esophageal carcinoma, gastric car-cinoma and colon carcinoma (Su et al., 2004; Kyzas et al.,2005a; von Rahden et al., 2005; Zhang et al., 2005; Soumaoroet al., 2006). COX-2 over-expression induces VEGF-C but notVEGF-D in human lung adenocarcinomas and correlates withlymphatic vessel density (Su et al., 2004). COX-2 inhibitorsdecrease VEGF-C levels (Timoshenko et al., 2006). Whenthree esophageal cell lines were treated in vitro with COX-2inhibitors such as diclofenac, rofecoxib and SC560, VEGF-Aand VEGF-C levels decreased (von Rahden et al., 2005). TheCOX-2 inhibitor, celecoxib (Celebrex, Pfizer), powerfullyblocked FGF-2 induced corneal lymphangiogenesis (Changet al., 2004). Celecoxib inhibited tumor angiogenesis and mic-rovessel density by causing apoptosis in tumor endothelial cells(Raut et al., 2004). Celecoxib also inhibits tumor lymphangio-genesis as assessed by Q-PCR and immunohistochemistry inMCF7 and MDAMB231 breast cancers (Barnes et al., 2007).
Glucocorticoids, including prednisone, hydrocortisone anddexamethasone, inhibit tumor angiogenesis by down-regulatingVEGF-A and IL-8 (Yano et al., 2006). Dexamethasone reducedVEGF-C expression in Du145 prostate tumors by 50% andinhibited tumor lymphangiogenesis (Yano et al., 2006).
Summary and perspective
Two safety concerns that arise when considering any therapyagainst lymphangiogenesis is whether the therapy will specif-ically target abnormal tumor lymphatic vessels and sparenormal lymphatic vessels or blood vessels and whether suchtherapy will result in lymphedema by reducing lymphatic flowand accumulating interstitial fluid (Gershenwald and Fidler,2002). Several recent studies have indirectly addressed theseconcerns. sVEGFR-3 in an adenoviral construct (which resultsin high expression) did not appear to affect normal lymphaticvessels once mice reached adolescence, approximately 4 weeksof age (Karpanen et al., 2006b). In addition, tumor studies inadult animals using sVEGFR-3 therapy have not reported nor-mal lymphatic vessel damage or non-specific effects on normalblood vessels (Karpanen et al., 2001, 2006b; Krishnan et al.,2003; He et al., 2005). Edema formation was not reported in anyof the anti-tumor lymphangiogenic studies using sVEGFR-3 but
was found in newborn transgenic mice. When mice were engi-neered to express sVEGFR-3-Ig under the keratin 14-promoter,which results in transgene expression in all basal keratinocytesof the skin, normal lymphatic vessels regressed and edemaresulted (Makinen et al., 2001). Using locally administeredprotein strategies (such as soluble receptors, antibodies or com-petitive inhibitors) instead of adenoviral or transgenic strategiesand appropriate dosing schedules may alleviate these unwantededema reactions.
Angiogenesis and lymphangiogenesis are both importantprocesses contributing to tumor progression and metastasis. Inorder to prevent the deadly spread of cancer cells, therapeuticstrategies combining inhibitors of both these endothelial com-partments may be necessary. Alternatively, single compoundsthat target both tumor-associated blood vessels and tumor-asso-ciated lymphatic vessels may decrease tumor size and decreasethe incidence of local and distant metastases (Table 3). Otherstrategies such as “low-dose chemotherapy” or “metronomicchemotherapy”may target the lymphatic endothelium as well asthe vascular endothelium (Gately and Kerbel, 2001; Kerbel andKamen, 2004; Kieran et al., 2005). Future studies will requirethe use of metastatic tumor models to elucidate the most ef-fective strategies of inhibiting tumor progression.
Acknowledgments
This work was supported by a Howard Temin Award (CA118732-01A1) from the National Cancer Institute and by theRobert Leet and Clara Guthrie Patterson Trust Award. Theauthors would like to acknowledge Ethan Bickford and KristinJohnson for illustrations and Ricardo Sanchez for histology.
References
Abuharbeid, S., Czubayko, F., Aigner, A., 2006. The fibroblast growth factor-binding protein FGF-BP. Int. J. Biochem. Cell Biol. 38, 1463–1468.
Achen, M.G., Jeltsch, M., Kukk, E., Makinen, T., Vitali, A., Wilks, A.F., Alitalo,K., Stacker, S.A., 1998. Vascular endothelial growth factor D (VEGF-D) is aligand for the tyrosine kinases VEGF receptor 2 (Flk1) and VEGF receptor 3(Flt4). Proc. Natl. Acad. Sci. U. S. A. 95, 548–553.
Achen, M.G., Roufail, S., Domagala, T., Catimel, B., Nice, E.C., Geleick, D.M.,Murphy, R., Scott, A.M., Caesar, C., Makinen, T., Alitalo, K., Stacker, S.A.,2000. Monoclonal antibodies to vascular endothelial growth factor-D blockits interactions with both VEGF receptor-2 and VEGF receptor-3. Eur. J.Biochem. 267, 2505–2515.
Achen, M.G., Williams, R.A., Baldwin, M.E., Lai, P., Roufail, S., Alitalo, K.,Stacker, S.A., 2002. The angiogenic and lymphangiogenic factor vascularendothelial growth factor-D exhibits a paracrine mode of action in cancer.Growth Factors 20, 99–107.
Ahmed, S.I., Thomas, A.L., Steward,W.P., 2004. Vascular endothelial growth factor(VEGF) inhibition by small molecules. J. Chemother. 16 (Suppl 4), 59–63.
Akagi, Y., Liu, W., Zebrowski, B., Xie, K., Ellis, L.M., 1998. Regulation ofvascular endothelial growth factor expression in human colon cancer byinsulin-like growth factor-I. Cancer Res. 58, 4008–4014.
Baka, S., Clamp, A.R., Jayson, G.C., 2006. A review of the latest clinicalcompounds to inhibit VEGF in pathological angiogenesis. Expert Opin.Ther. Targets 10, 867–876.
Baldwin, M.E., Halford, M.M., Roufail, S., Williams, R.A., Hibbs, M.L., Grail,D., Kubo, H., Stacker, S.A., Achen, M.G., 2005. Vascular endothelial growthfactor D is dispensable for development of the lymphatic system. Mol. Cell.Biol. 25, 2441–2449.

155B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
Barnes, N.L., Warnberg, F., Farnie, G., White, D., Jiang, W., Anderson, E.,Bundred, N.J., 2007. Cyclooxygenase-2 inhibition: effects on tumour growth,cell cycling and lymphangiogenesis in a xenograft model of breast cancer.Br. J. Cancer 96, 575–582.
Bielenberg, D.R., Bucana, C.D., Sanchez, R., Mulliken, J.B., Folkman, J.,Fidler, I.J., 1999. Progressive growth of infantile cutaneous hemangiomas isdirectly correlated with hyperplasia and angiogenesis of adjacent epidermisand inversely correlated with expression of the endogenous angiogenesisinhibitor, IFN-beta. Int. J. Oncol. 14, 401–408.
Bielenberg, D.R., Hida, Y., Shimizu, A., Kaipainen, A., Kreuter, M., Kim, C.C.,Klagsbrun, M., 2004. Semaphorin 3F, a chemorepulsant for endothelial cells,induces a poorly vascularized, encapsulated, nonmetastatic tumor phenotype.J. Clin. Invest. 114, 1260–1271.
Bielenberg, D.R., Pettaway, C.A., Takashima, S., Klagsbrun, M., 2006. Neuro-pilins in neoplasms: expression, regulation, and function. Exp. Cell Res.312, 584–593.
Bjorndahl, M., Cao, R., Nissen, L.J., Clasper, S., Johnson, L.A., Xue, Y., Zhou,Z., Jackson, D., Hansen, A.J., Cao, Y., 2005a. Insulin-like growth factors 1and 2 induce lymphangiogenesis in vivo. Proc. Natl. Acad. Sci. U. S. A. 102,15593–15598.
Bjorndahl, M.A., Cao, R., Burton, J.B., Brakenhielm, E., Religa, P., Galter, D.,Wu, L., Cao, Y., 2005b. Vascular endothelial growth factor-A promotesperitumoral lymphangiogenesis and lymphatic metastasis. Cancer Res. 65,9261–9268.
Cao, R., Bjorndahl, M.A., Religa, P., Clasper, S., Garvin, S., Galter, D., Meister,B., Ikomi, F., Tritsaris, K., Dissing, S., Ohhashi, T., Jackson, D.G., Cao, Y.,2004. PDGF-BB induces intratumoral lymphangiogenesis and promoteslymphatic metastasis. Cancer Cells 6, 333–345.
Cao, R., Bjorndahl, M.A., Gallego, M.I., Chen, S., Religa, P., Hansen, A.J., Cao,Y., 2006. Hepatocyte growth factor is a lymphangiogenic factor with anindirect mechanism of action. Blood 107, 3531–3536.
Chang, L., Kaipainen, A., Folkman, J., 2002. Lymphangiogenesis new mecha-nisms. Ann. N. Y. Acad. Sci. 979, 111–119.
Chang, L.K., Garcia-Cardena, G., Farnebo, F., Fannon, M., Chen, E.J., Butter-field, C., Moses, M.A., Mulligan, R.C., Folkman, J., Kaipainen, A., 2004.Dose-dependent response of FGF-2 for lymphangiogenesis. Proc. Natl.Acad. Sci. U. S. A. 101, 11658–11663.
Chen, Z., Varney, M.L., Backora, M.W., Cowan, K., Solheim, J.C., Talmadge,J.E., Singh, R.K., 2005. Down-regulation of vascular endothelial cell growthfactor-C expression using small interfering RNA vectors in mammary tu-mors inhibits tumor lymphangiogenesis and spontaneous metastasis andenhances survival. Cancer Res. 65, 9004–9011.
Chen, S.L., Iddings, D.M., Scheri, R.P., Bilchik, A.J., 2006. Lymphatic mappingand sentinel node analysis: current concepts and applications. CA CancerJ. Clin. 56, 292–309.
Clarijs, R., Schalkwijk, L., Hofmann, U.B., Ruiter, D.J., de Waal, R.M., 2002.Induction of vascular endothelial growth factor receptor-3 expression ontumor microvasculature as a new progression marker in human cutaneousmelanoma. Cancer Res. 62, 7059–7065.
Cursiefen, C., Chen, L., Borges, L.P., Jackson, D., Cao, J., Radziejewski, C.,D'Amore, P.A., Dana, M.R., Wiegand, S.J., Streilein, J.W., 2004. VEGF-Astimulates lymphangiogenesis and hemangiogenesis in inflammatory neo-vascularization via macrophage recruitment. J. Clin. Invest. 113, 1040–1050.
Cursiefen, C., Ikeda, S., Nishina, P.M., Smith, R.S., Ikeda, A., Jackson, D.,Mo, J.S., Chen, L., Dana, M.R., Pytowski, B., Kruse, F.E., Streilein, J.W.,2005. Spontaneous corneal hem- and lymphangiogenesis in mice withdestrin-mutation depend on VEGFR3 signaling. Am. J. Pathol. 166,1367–1377.
Dadras, S.S., Paul, T., Bertoncini, J., Brown, L.F., Muzikansky, A., Jackson,D.G., Ellwanger, U., Garbe, C., Mihm, M.C., Detmar, M., 2003. Tumorlymphangiogenesis: a novel prognostic indicator for cutaneous melanomametastasis and survival. Am. J. Pathol. 162, 1951–1960.
Daróczy, J., 1988. The Dermal Lymphatic Capillaries. Springer-Verlag, Berlin,p. 157.
Denzinger, S., Otto, W., Burger, M., Hammerschmied, C., Junker, K., Hartmann,A., Wieland, W.F., Walter, B., 2007. Sporadic renal cell carcinoma in youngand elderly patients: are there different clinicopathological features anddisease specific survival rates? World J. Surg. Oncol. 5, 16.
Dinney, C.P., Bielenberg, D.R., Perrotte, P., Reich, R., Eve, B.Y., Bucana, C.D.,Fidler, I.J., 1998. Inhibition of basic fibroblast growth factor expression,angiogenesis, and growth of human bladder carcinoma in mice by systemicinterferon-alpha administration. Cancer Res. 58, 808–814.
Dong, Z., Greene, G., Pettaway, C., Dinney, C.P., Eue, I., Lu, W., Bucana, C.D.,Balbay, M.D., Bielenberg, D., Fidler, I.J., 1999. Suppression of angiogen-esis, tumorigenicity, and metastasis by human prostate cancer cells engi-neered to produce interferon-beta. Cancer Res. 59, 872–879.
Ezekowitz, R.A.,Mulliken, J.B., Folkman, J., 1992. Interferon alfa-2a therapy forlife-threatening hemangiomas of infancy. N. Engl. J. Med. 326, 1456–1463.
Ezekowitz, A., Mulliken, J., Folkman, J., 1995. Additional corrections: inter-feron for hemangiomas of infancy. N. Engl. J. Med. 333, 595–596.
Favier, B., Alam, A., Barron, P., Bonnin, J., Laboudie, P., Fons, P., Mandron, M.,Herault, J.P., Neufeld, G., Savi, P., Herbert, J.M., Bono, F., 2006. Neuro-pilin-2 interacts with VEGFR-2 and VEGFR-3 and promotes human endo-thelial cell survival and migration. Blood 108, 1243–1250.
Fidler, I.J., 1970. Metastasis: quantitative analysis of distribution and fate oftumor emboli labeled with 125 I-5-iodo-2′-deoxyuridine. J. Natl. CancerInst. 45, 773–782.
Fidler, I.J., 1990. Critical factors in the biology of human cancer metastasis:twenty-eighth G.H.A. Clowes memorial award lecture. Cancer Res. 50,6130–6138.
Fidler, I.J., 2002. Critical determinants of metastasis. Semin. Cancer Biol. 12,89–96.
Fidler, I.J., Singh, R.K., Yoneda, J., Kumar, R., Xu, L., Dong, Z., Bielenberg,D.R., McCarty, M., Ellis, L.M., 2000. Critical determinants of neoplasticangiogenesis. Cancer J. 6 (Suppl 3), S225–S236.
Folkman, J., 1971. Tumor angiogenesis: therapeutic implications. N. Engl. J.Med. 285, 1182–1186.
Folkman, J., 2004. Endogenous angiogenesis inhibitors. APMIS 112, 496–507.Fong, Y., Coit, D.G., Woodruff, J.M., Brennan, M.F., 1993. Lymph node meta-
stasis from soft tissue sarcoma in adults. Analysis of data from a prospectivedatabase of 1772 sarcoma patients. Ann. Surg. 217, 72–77.
Gale, N.W., Thurston, G., Hackett, S.F., Renard, R., Wang, Q., McClain, J.,Martin, C., Witte, C., Witte, M.H., Jackson, D., Suri, C., Campochiaro, P.A.,Wiegand, S.J., Yancopoulos, G.D., 2002. Angiopoietin-2 is required forpostnatal angiogenesis and lymphatic patterning, and only the latter role isrescued by Angiopoietin-1. Dev. Cell 3, 411–423.
Gately, S., Kerbel, R., 2001. Antiangiogenic scheduling of lower dose cancerchemotherapy. Cancer J. 7, 427–436.
Gershenwald, J.E., Fidler, I.J., 2002. Cancer. Targeting lymphatic metastasis.Science 296, 1811–1812.
Haagensen, C.D., Feind, K.R., Herter, F.P., Slanets, C.A., Weinberg, J.A., 1972.The Lymphatics in Cancer. Saunders, Philadelphia, p. 583.
Harrell, M.I., Iritani, B.M., Ruddell, A., 2007. Tumor-induced sentinel lymphnode lymphangiogenesis and increased lymph flow precede melanoma meta-stasis. Am. J. Pathol. 170, 774–786.
Hatakeyama, H., Kondo, T., Fujii, K., Nakanishi, Y., Kato, H., Fukuda, S.,Hirohashi, S., 2006. Protein clusters associated with carcinogenesis, histo-logical differentiation and nodal metastasis in esophageal cancer. Proteomics6, 6300–6316.
Hawighorst, T., Oura, H., Streit, M., Janes, L., Nguyen, L., Brown, L.F.,Oliver, G., Jackson, D.G., Detmar, M., 2002. Thrombospondin-1selectively inhibits early-stage carcinogenesis and angiogenesis but nottumor lymphangiogenesis and lymphatic metastasis in transgenic mice.Oncogene 21, 7945–7956.
He, Y., Kozaki, K., Karpanen, T., Koshikawa, K., Yla-Herttuala, S., Takahashi,T., Alitalo, K., 2002. Suppression of tumor lymphangiogenesis and lymphnode metastasis by blocking vascular endothelial growth factor receptor 3signaling. J. Natl. Cancer Inst. 94, 819–825.
He, Y., Rajantie, I., Pajusola, K., Jeltsch, M., Holopainen, T., Yla-Herttuala, S.,Harding, T., Jooss, K., Takahashi, T., Alitalo, K., 2005. Vascular endothelialcell growth factor receptor 3-mediated activation of lymphatic endotheliumis crucial for tumor cell entry and spread via lymphatic vessels. Cancer Res.65, 4739–4746.
Hess, K.R., Varadhachary, G.R., Taylor, S.H., Wei, W., Raber, M.N., Lenzi, R.,Abbruzzese, J.L., 2006. Metastatic patterns in adenocarcinoma. Cancer 106,1624–1633.

156 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
Hirakawa, S., Hong, Y.K., Harvey, N., Schacht, V., Matsuda, K., Libermann, T.,Detmar, M., 2003. Identification of vascular lineage-specific genes by tran-scriptional profiling of isolated blood vascular and lymphatic endothelialcells. Am. J. Pathol. 162, 575–586.
Hirakawa, S., Kodama, S., Kunstfeld, R., Kajiya, K., Brown, L.F., Detmar, M.,2005. VEGF-A induces tumor and sentinel lymph node lymphangiogenesisand promotes lymphatic metastasis. J. Exp. Med. 201, 1089–1099.
Hirakawa, S., Brown, L.F., Kodama, S., Paavonen, K., Alitalo, K., Detmar, M.,2007. VEGF-C-induced lymphangiogenesis in sentinel lymph nodes pro-motes tumor metastasis to distant sites. Blood 109, 1010–1017.
Hong, Y.K., Lange-Asschenfeldt, B., Velasco, P., Hirakawa, S., Kunstfeld, R.,Brown, L.F., Bohlen, P., Senger, D.R., Detmar, M., 2004. VEGF-A pro-motes tissue repair-associated lymphatic vessel formation via VEGFR-2 andthe alpha1beta1 and alpha2beta1 integrins. FASEB J. 18, 1111–1113.
Hoshida, T., Isaka, N., Hagendoorn, J., di Tomaso, E., Chen, Y.L., Pytowski, B.,Fukumura, D., Padera, T.P., Jain, R.K., 2006. Imaging steps of lymphaticmetastasis reveals that vascular endothelial growth factor-C increases meta-stasis by increasing delivery of cancer cells to lymph nodes: therapeuticimplications. Cancer Res. 66, 8065–8075.
Jeltsch, M., Kaipainen, A., Joukov, V., Meng, X., Lakso, M., Rauvala, H.,Swartz, M., Fukumura, D., Jain, R.K., Alitalo, K., 1997. Hyperplasia oflymphatic vessels in VEGF-C transgenic mice. Science 276, 1423–1425.
Jiang, W.G., Davies, G., Martin, T.A., Parr, C., Watkins, G., Mansel, R.E.,Mason, M.D., 2005. The potential lymphangiogenic effects of hepatocytegrowth factor/scatter factor in vitro and in vivo. Int. J. Mol. Med. 16,723–728.
Jimenez, X., Lu, D., Brennan, L., Persaud, K., Liu, M., Miao, H., Witte, L., Zhu,Z., 2005. A recombinant, fully human, bispecific antibody neutralizes thebiological activities mediated by both vascular endothelial growth factorreceptors 2 and 3. Mol. Cancer Ther. 4, 427–434.
Jones, A., Fujiyama, C., Turner, K., Fuggle, S., Cranston, D., Turley, H., Valtola,R., Bicknell, R., Harris, A.L., 2000. Angiogenesis and lymphangiogenesis instage 1 germ cell tumours of the testis. BJU Int. 86, 80–86.
Jones, T.D., Carr, M.D., Eble, J.N., Wang, M., Lopez-Beltran, A., Cheng, L.,2005. Clonal origin of lymph node metastases in bladder carcinoma. Cancer104, 1901–1910.
Joukov, V., Pajusola, K., Kaipainen, A., Chilov, D., Lahtinen, I., Kukk, E.,Saksela, O., Kalkkinen, N., Alitalo, K., 1996. A novel vascularendothelial growth factor, VEGF-C, is a ligand for the Flt4 (VEGFR-3) and KDR (VEGFR-2) receptor tyrosine kinases. EMBO J. 15,290–298.
Kadambi, A., Mouta Carreira, C., Yun, C.O., Padera, T.P., Dolmans, D.E.,Carmeliet, P., Fukumura, D., Jain, R.K., 2001. Vascular endothelial growthfactor (VEGF)-C differentially affects tumor vascular function and leuko-cyte recruitment: role of VEGF-receptor 2 and host VEGF-A. Cancer Res.61, 2404–2408.
Kaipainen, A., Korhonen, J., Mustonen, T., van Hinsbergh, V.W., Fang, G.H.,Dumont, D., Breitman, M., Alitalo, K., 1995. Expression of the fms-liketyrosine kinase 4 gene becomes restricted to lymphatic endothelium duringdevelopment. Proc. Natl. Acad. Sci. U. S. A. 92, 3566–3570.
Kajiya, K., Hirakawa, S., Ma, B., Drinnenberg, I., Detmar, M., 2005. Hepa-tocyte growth factor promotes lymphatic vessel formation and function.EMBO J. 24, 2885–2895.
Kajiya, K., Hirakawa, S., Detmar, M., 2006. Vascular endothelial growth factor-A mediates ultraviolet B-induced impairment of lymphatic vessel function.Am. J. Pathol. 169, 1496–1503.
Karkkainen, M.J., Haiko, P., Sainio, K., Partanen, J., Taipale, J., Petrova, T.V.,Jeltsch, M., Jackson, D.G., Talikka, M., Rauvala, H., Betsholtz, C., Alitalo,K., 2004. Vascular endothelial growth factor C is required for sprouting ofthe first lymphatic vessels from embryonic veins. Nat. Immunol. 5, 74–80.
Karpanen, T., Egeblad, M., Karkkainen, M.J., Kubo, H., Yla-Herttuala, S.,Jaattela, M., Alitalo, K., 2001. Vascular endothelial growth factor C pro-motes tumor lymphangiogenesis and intralymphatic tumor growth. CancerRes. 61, 1786–1790.
Karpanen, T., Heckman, C.A., Keskitalo, S., Jeltsch, M., Ollila, H., Neufeld, G.,Tamagnone, L., Alitalo, K., 2006a. Functional interaction of VEGF-C andVEGF-D with neuropilin receptors. FASEB J. 20, 1462–1472.
Karpanen, T., Wirzenius, M., Makinen, T., Veikkola, T., Haisma, H.J., Achen,
M.G., Stacker, S.A., Pytowski, B., Yla-Herttuala, S., Alitalo, K., 2006b.Lymphangiogenic growth factor responsiveness is modulated by postnatallymphatic vessel maturation. Am. J. Pathol. 169, 708–718.
Kerbel, R.S., Kamen, B.A., 2004. The anti-angiogenic basis of metronomicchemotherapy. Nat. Rev., Cancer 4, 423–436.
Kieran, M.W., Turner, C.D., Rubin, J.B., Chi, S.N., Zimmerman, M.A., Chor-das, C., Klement, G., Laforme, A., Gordon, A., Thomas, A., Neuberg, D.,Browder, T., Folkman, J., 2005. A feasibility trial of antiangiogenic (metro-nomic) chemotherapy in pediatric patients with recurrent or progressivecancer. J. Pediatr. Hematol./Oncol. 27, 573–581.
Krishnan, J., Kirkin, V., Steffen, A., Hegen, M., Weih, D., Tomarev, S., Wilting,J., Sleeman, J.P., 2003. Differential in vivo and in vitro expression ofvascular endothelial growth factor (VEGF)-C and VEGF-D in tumors and itsrelationship to lymphatic metastasis in immunocompetent rats. Cancer Res.63, 713–722.
Kuba, K., Matsumoto, K., Date, K., Shimura, H., Tanaka, M., Nakamura, T.,2000. HGF/NK4, a four-kringle antagonist of hepatocyte growth factor, is anangiogenesis inhibitor that suppresses tumor growth and metastasis in mice.Cancer Res. 60, 6737–6743.
Kubo, H., Fujiwara, T., Jussila, L., Hashi, H., Ogawa, M., Shimizu, K., Awane,M., Sakai, Y., Takabayashi, A., Alitalo, K., Yamaoka, Y., Nishikawa, S.I.,2000. Involvement of vascular endothelial growth factor receptor-3 inmaintenance of integrity of endothelial cell lining during tumor angiogen-esis. Blood 96, 546–553.
Kubo, H., Cao, R., Brakenhielm, E., Makinen, T., Cao, Y., Alitalo, K., 2002.Blockade of vascular endothelial growth factor receptor-3 signaling inhibitsfibroblast growth factor-2-induced lymphangiogenesis in mouse cornea.Proc. Natl. Acad. Sci. U. S. A. 99, 8868–8873.
Kunstfeld, R., Hirakawa, S., Hong, Y.K., Schacht, V., Lange-Asschenfeldt, B.,Velasco, P., Lin, C., Fiebiger, E., Wei, X., Wu, Y., Hicklin, D., Bohlen, P.,Detmar, M., 2004. Induction of cutaneous delayed-type hypersensitivityreactions in VEGF-A transgenic mice results in chronic skin inflammationassociated with persistent lymphatic hyperplasia. Blood 104, 1048–1057.
Kyzas, P.A., Stefanou, D., Agnantis, N.J., 2005a. COX-2 expression correlateswith VEGF-C and lymph node metastases in patients with head and necksquamous cell carcinoma. Mod. Path 18, 153–160.
Kyzas, P.A., Geleff, S., Batistatou, A., Agnantis, N.J., Stefanou, D., 2005b.Evidence for lymphangiogenesis and its prognostic implications in head andneck squamous cell carcinoma. J. Pathol. 206, 170–177.
Laakkonen, P., Waltari, M., Holopainen, T., Takahashi, T., Pytowski, B., Steiner,P., Hicklin, D., Persaud, K., Tonra, J.R., Witte, L., Alitalo, K., 2007. Vascularendothelial growth factor receptor 3 is involved in tumor angiogenesis andgrowth. Cancer Res. 67, 593–599.
Lin, J., Lalani, A.S., Harding, T.C., Gonzalez, M., Wu, W.W., Luan, B., Tu,G.H., Koprivnikar, K., VanRoey, M.J., He, Y., Alitalo, K., Jooss, K., 2005.Inhibition of lymphogenous metastasis using adeno-associated virus-me-diated gene transfer of a soluble VEGFR-3 decoy receptor. Cancer Res. 65,6901–6909.
Makinen, T., Jussila, L., Veikkola, T., Karpanen, T., Kettunen, M.I., Pulkkanen,K.J., Kauppinen, R., Jackson, D.G., Kubo, H., Nishikawa, S., Yla-Herttuala,S., Alitalo, K., 2001. Inhibition of lymphangiogenesis with resultinglymphedema in transgenic mice expressing soluble VEGF receptor-3. Nat.Med. 7, 199–205.
Mandriota, S.J., Jussila, L., Jeltsch, M., Compagni, A., Baetens, D., Prevo, R.,Banerji, S., Huarte, J., Montesano, R., Jackson, D.G., Orci, L., Alitalo, K.,Christofori, G., Pepper, M.S., 2001. Vascular endothelial growth factor-C-mediated lymphangiogenesis promotes tumour metastasis. EMBO J. 20,672–682.
Manley, P.W., Martiny-Baron, G., Schlaeppi, J.M., Wood, J.M., 2002. Therapiesdirected at vascular endothelial growth factor. Expert Opin. Investig Drugs11, 1715–1736.
Mattila,M.M., Ruohola, J.K., Karpanen, T., Jackson,D.G., Alitalo, K., Harkonen,P.L., 2002. VEGF-C induced lymphangiogenesis is associated with lymphnode metastasis in orthotopic MCF-7 tumors. Int. J. Cancer 98, 946–951.
Maula, S.M., Luukkaa, M., Grenman, R., Jackson, D., Jalkanen, S., Ristamaki,R., 2003. Intratumoral lymphatics are essential for the metastatic spread andprognosis in squamous cell carcinomas of the head and neck region. CancerRes. 63, 1920–1926.

157B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
McColl, B.K., Loughran, S.J., Davydova, N., Stacker, S.A., Achen, M.G., 2005.Mechanisms of lymphangiogenesis: targets for blocking themetastatic spreadof cancer. Curr. Cancer Drug Targets 5, 561–571.
Morabito, A., De Maio, E., Di Maio, M., Normanno, N., Perrone, F., 2006.Tyrosine kinase inhibitors of vascular endothelial growth factor receptors inclinical trials: current status and future directions. Oncologist 11, 753–764.
Morisada, T., Oike, Y., Yamada, Y., Urano, T., Akao, M., Kubota, Y., Maekawa,H., Kimura, Y., Ohmura, M., Miyamoto, T., Nozawa, S., Koh, G.Y., Alitalo,K., Suda, T., 2005. Angiopoietin-1 promotes LYVE-1-positive lymphaticvessel formation. Blood 105, 4649–4656.
Morisawa, N., Koyama, T., Togashi, K., 2006. Metastatic lymph nodes inurogenital cancers: contribution of imaging findings. Abdom. Imaging 31,620–629.
Nagy, J.A., Vasile, E., Feng, D., Sundberg, C., Brown, L.F., Detmar, M.J.,Lawitts, J.A., Benjamin, L., Tan, X., Manseau, E.J., Dvorak, A.M., Dvorak,H.F., 2002. Vascular permeability factor/vascular endothelial growth factorinduces lymphangiogenesis as well as angiogenesis. J. Exp. Med. 196,1497–1506.
Onda, T., Yoshikawa, H., Yokota, H., Yasugi, T., Taketani, Y., 1996. Assessmentof metastases to aortic and pelvic lymph nodes in epithelial ovarian carci-noma. A proposal for essential sites for lymph node biopsy. Cancer 78,803–808.
Padera, T.P., Kadambi, A., di Tomaso, E., Carreira, C.M., Brown, E.B., Boucher,Y., Choi, N.C., Mathisen, D., Wain, J., Mark, E.J., Munn, L.L., Jain, R.K.,2002. Lymphatic metastasis in the absence of functional intratumor lym-phatics. Science 296, 1883–1886.
Pandit-Taskar, N., 2005. Oncologic imaging in gynecologic malignancies.J. Nucl. Med. 46, 1842–1850.
Partanen, T.A., Alitalo, K., Miettinen, M., 1999. Lack of lymphatic vascularspecificity of vascular endothelial growth factor receptor 3 in 185 vasculartumors. Cancer 86, 2406–2412.
Podgrabinska, S., Braun, P., Velasco, P., Kloos, B., Pepper, M.S., Skobe, M.,2002. Molecular characterization of lymphatic endothelial cells. Proc. Natl.Acad. Sci. U. S. A. 99, 16069–16074.
Pytowski, B., Goldman, J., Persaud, K., Wu, Y., Witte, L., Hicklin, D.J., Skobe,M., Boardman, K.C., Swartz, M.A., 2005. Complete and specific inhibitionof adult lymphatic regeneration by a novel VEGFR-3 neutralizing antibody.J. Natl. Cancer Inst. 97, 14–21.
Rafii, S., Skobe, M., 2003. Splitting vessels: keeping lymph apart from blood.Nat. Med. 9, 166–168.
Raut, C.P., Nawrocki, S., Lashinger, L.M., Davis, D.W., Khanbolooki, S.,Xiong, H., Ellis, L.M., McConkey, D.J., 2004. Celecoxib inhibits angio-genesis by inducing endothelial cell apoptosis in human pancreatic tumorxenografts. Cancer Biol. Ther. 3, 1217–1224.
Renyi-Vamos, F., Tovari, J., Fillinger, J., Timar, J., Paku, S., Kenessey, I.,Ostoros, G., Agocs, L., Soltesz, I., Dome, B., 2005. Lymphangiogenesiscorrelates with lymph node metastasis, prognosis, and angiogenic phenotypein human non-small cell lung cancer. Clin. Cancer Res. 11, 7344–7353.
Rissanen, T.T., Markkanen, J.E., Gruchala, M., Heikura, T., Puranen, A., Kettu-nen,M.I., Kholova, I., Kauppinen, R.A., Achen,M.G., Stacker, S.A., Alitalo,K., Yla-Herttuala, S., 2003. VEGF-D is the strongest angiogenic and lym-phangiogenic effector among VEGFs delivered into skeletal muscle viaadenoviruses. Circ. Res. 92, 1098–1106.
Ristimaki, A., Narko, K., Enholm, B., Joukov, V., Alitalo, K., 1998. Proinflam-matory cytokines regulate expression of the lymphatic endothelial mitogenvascular endothelial growth factor-C. J. Biol. Chem. 273, 8413–8418.
Roberts, N., Kloos, B., Cassella, M., Podgrabinska, S., Persaud, K., Wu, Y.,Pytowski, B., Skobe, M., 2006. Inhibition of VEGFR-3 activation with theantagonistic antibody more potently suppresses lymph node and distantmetastases than inactivation of VEGFR-2. Cancer Res. 66, 2650–2657.
Roche, J., Boldog, F., Robinson, M., Robinson, L., Varella-Garcia, M., Swanton,M., Waggoner, B., Fishel, R., Franklin, W., Gemmill, R., Drabkin, H., 1996.Distinct 3p21.3 deletions in lung cancer and identification of a new humansemaphorin. Oncogene 12, 1289–1297.
Rodriguez, J.M., Pinero, A., Ortiz, S., Moreno, A., Sola, J., Soria, T., Robles, R.,Parrilla, P., 2000. Clinical and histological differences in anaplastic thyroidcarcinoma. Eur. J. Surg. 166, 34–38.
Rogers,M.S., Rohan, R.M., Birsner, A.E., D'Amato, R.J., 2003. Genetic loci that
control vascular endothelial growth factor-induced angiogenesis. FASEB J.17, 2112–2114.
Rusznyak, I., Foldi, M., Szabo, G., 1967. Lymphatics and Lymph Circulation;Physiology and Pathology. In: Youlton, L. (Ed.), Pergamon Press, Oxford.
Saaristo, A., Veikkola, T., Tammela, T., Enholm, B., Karkkainen, M.J., Pajusola,K., Bueler, H., S.Alitalo, K., 2002. Lymphangiogenic gene therapy withminimal blood vascular side effects. J. Exp. Med. 196, 719–730.
Saito, H., Osaki, T., Murakami, D., Sakamoto, T., Kanaji, S., Ohro, S., Tatebe,S., Tsujitani, S., Ikeguchi, M., 2007. Prediction of sites of recurrence ingastric carcinoma using immunohistochemical parameters. J. Surg. Oncol.95, 123–128.
Sato, T.N., Tozawa, Y., Deutsch, U., Wolburg-Buchholz, K., Fujiwara, Y.,Gendron-Maguire, M., Gridley, T., Wolburg, H., Risau, W., Qin, Y., 1995.Distinct roles of the receptor tyrosine kinases Tie-1 and Tie-2 in blood vesselformation. Nature 376, 70–74.
Sauter, B., Foedinger, D., Sterniczky, B., Wolff, K., Rappersberger, K., 1998.Immunoelectron microscopic characterization of human dermal lymphaticmicrovascular endothelial cells: differential expression of CD31, CD34, andtype IV collagen with lymphatic endothelial cells vs blood capillary endo-thelial cells in normal human skin, lymphangioma, and hemangioma in situ.J. Histochem. Cytochem. 46, 165–176.
Schacht, V., von Rautenfeld, D.B., Abels, C., 2004. The lymphatic system in thedorsal skinfold chamber of the Syrian golden hamster in vivo. Arch. Der-matol. Res. 295, 542–548.
Schauer, A.J., Becker, W., Reiser, M., Possinger, K., 2005. The Sentinel LymphNode Concept. In: Heilmann, U. (Ed.), Springer-Verlag, Berlin, p. 565.
Schneider, M., Buchler, P., Giese, N., Giese, T., Wilting, J., Buchler, M.W.,Friess, H., 2006. Role of lymphangiogenesis and lymphangiogenic factorsduring pancreatic cancer progression and lymphatic spread. Int. J. Oncol. 28,883–890.
Scollo, C., Baudin, E., Travagli, J.P., Caillou, B., Bellon, N., Leboulleux, S.,Schlumberger, M., 2003. Rationale for central and bilateral lymph node dis-section in sporadic and hereditary medullary thyroid cancer. J. Clin. Endo-crinol. Metab. 88, 2070–2075.
Sekido, Y., Bader, S., Latif, F., Chen, J.Y., Duh, F.M., Wei, M.H., Albanesi, J.P.,Lee, C.C., Lerman, M.I., Minna, J.D., 1996. Human semaphorins A(V) andIVreside in the 3p21.3 small cell lung cancer deletion region and demonstratedistinct expression patterns. Proc. Natl. Acad. Sci. U. S. A. 93, 4120–4125.
Senger, D.R., Claffey, K.P., Benes, J.E., Perruzzi, C.A., Sergiou, A.P., Detmar,M., 1997. Angiogenesis promoted by vascular endothelial growth factor:regulation through alpha1beta1 and alpha2beta1 integrins. Proc. Natl. Acad.Sci. U. S. A. 94, 13612–13617.
Shao, X.J., Chi, X.Y., 2005. Influence of angiostatin and thalidomide on lym-phangiogenesis. Lymphology 38, 146–155.
Shao, X., Liu, C., 2006. Influence of IFN-alpha and IFN-gamma on lym-phangiogenesis. J. Interferon Cytokine Res. 26, 568–574.
Shao, X.J., Xie, F.M., 2005. Influence of angiogenesis inhibitors, endostatin andPF-4, on lymphangiogenesis. Lymphology 38, 1–8.
Shariat, S.F., Karakiewicz, P.I., Palapattu, G.S., Lotan, Y., Rogers, C.G.,Amiel, G.E., Vazina, A., Gupta, A., Bastian, P.J., Sagalowsky, A.I.,Schoenberg, M.P., Lerner, S.P., 2006. Outcomes of radical cystectomy fortransitional cell carcinoma of the bladder: a contemporary series from theBladder Cancer Research Consortium. J. Urol. 176, 2414–2422 (discus-sion 2422).
Shields, J.D., Emmett, M.S., Dunn, D.B., Joory, K.D., Sage, L.M., Rigby, H.,Mortimer, P.S., Orlando, A., Levick, J.R., Bates, D.O., 2007. Chemokine-mediated migration of melanoma cells towards lymphatics—a mechanismcontributing to metastasis. Oncogene 26, 2997–3005.
Shimizu, K., Kubo, H., Yamaguchi, K., Kawashima, K., Ueda, Y., Matsuo, K.,Awane, M., Shimahara, Y., Takabayashi, A., Yamaoka, Y., Satoh, S., 2004.Suppression of VEGFR-3 signaling inhibits lymph node metastasis in gas-tric cancer. Cancer Sci. 95, 328–333.
Shin, J.W.,Min,M., Larrieu-Lahargue, F., Canron, X., Kunstfeld, R., Nguyen, L.,Henderson, J.E., Bikfalvi, A., Detmar,M., Hong,Y.K., 2006. Prox1 promoteslineage-specific expression of fibroblast growth factor (FGF) receptor-3 inlymphatic endothelium: a role for FGF signaling in lymphangiogenesis. Mol.Biol. Cell 17, 576–584.
Sipos, B., Klapper, W., Kruse, M.L., Kalthoff, H., Kerjaschki, D., Kloppel, G.,

158 B.M.M. Zwaans, D.R. Bielenberg / Microvascular Research 74 (2007) 145–158
2004. Expression of lymphangiogenic factors and evidence of intratumorallymphangiogenesis in pancreatic endocrine tumors. Am. J. Pathol. 165,1187–1197.
Sipos, B., Kojima, M., Tiemann, K., Klapper, W., Kruse, M.L., Kalthoff, H.,Schniewind, B., Tepel, J., Weich, H., Kerjaschki, D., Kloppel, G., 2005.Lymphatic spread of ductal pancreatic adenocarcinoma is independent oflymphangiogenesis. J. Pathol. 207, 301–312.
Skobe, M., Detmar, M., 2000. Structure, function, and molecular control of theskin lymphatic system. J. Investig. Dermatol. Symp. Proc. 5, 14–19.
Skobe,M., Hamberg, L.M., Hawighorst, T., Schirner, M.,Wolf, G.L., Alitalo, K.,Detmar, M., 2001a. Concurrent induction of lymphangiogenesis, angio-genesis, andmacrophage recruitment by vascular endothelial growth factor-Cin melanoma. Am. J. Pathol. 159, 893–903.
Skobe, M., Hawighorst, T., Jackson, D.G., Prevo, R., Janes, L., Velasco, P.,Riccardi, L., Alitalo, K., Claffey, K., Detmar, M., 2001b. Induction of tumorlymphangiogenesis by VEGF-C promotes breast cancer metastasis. Nat.Med. 7, 192–198.
Sleeman, J.P., 2000. The lymph node as a bridgehead in the metastatic disse-mination of tumors. In: Schlag, P.M., Veronesi, U. (Eds.), Lymphatic Me-tastasis and Sentinel Lymphonodectomy. Springer-Verlag, Berlin, p. 309.
Sleeman, J.P., 2006. The relationship between tumors and the lymphatics: whatmore is there to know? Lymphology 39, 62–68.
Slevin,M., Payne, S., 2004. New treatments for colon cancer. BMJ 329, 124–126.Smith Jr., J.A., Seaman, J.P., Gleidman, J.B., Middleton, R.G., 1983. Pelvic
lymph node metastasis from prostatic cancer: influence of tumor grade andstage in 452 consecutive patients. J. Urol. 130, 290–292.
Sohaib, S.A., Houghton, S.L., Meroni, R., Rockall, A.G., Blake, P., Reznek,R.H., 2007. Recurrent endometrial cancer: patterns of recurrent disease andassessment of prognosis. Clin. Radiol. 62, 28–34 (discussion 35-6).
Soker, S., Takashima, S., Miao, H.Q., Neufeld, G., Klagsbrun, M., 1998.Neuropilin-1 is expressed by endothelial and tumor cells as an isoform-specific receptor for vascular endothelial growth factor. Cell 92, 735–745.
Soumaoro, L.T., Uetake, H., Takagi, Y., Iida, S., Higuchi, T., Yasuno, M.,Enomoto, M., Sugihara, K., 2006. Coexpression of VEGF-C and Cox-2 inhuman colorectal cancer and its association with lymph node metastasis.Dis. Colon Rectum 49, 392–398.
Stacker, S.A., Caesar, C., Baldwin, M.E., Thornton, G.E., Williams, R.A., Prevo,R., Jackson, D.G., Nishikawa, S., Kubo, H., Achen, M.G., 2001. VEGF-Dpromotes the metastatic spread of tumor cells via the lymphatics. Nat.Med. 7,186–191.
Stacker, S.A., Achen, M.G., Jussila, L., Baldwin, M.E., Alitalo, K., 2002.Lymphangiogenesis and cancer metastasis. Nat. Rev., Cancer 2, 573–583.
Stoitzner, P., Pfaller, K., Stossel, H., Romani, N., 2002. A close-up view ofmigrating Langerhans cells in the skin. J. Invest. Dermatol. 118, 117–125.
Su, J.L., Shih, J.Y., Yen, M.L., Jeng, Y.M., Chang, C.C., Hsieh, C.Y., Wei, L.H.,Yang, P.C., Kuo, M.L., 2004. Cyclooxygenase-2 induces EP1- and HER-2/Neu-dependent vascular endothelial growth factor-C up-regulation: a novelmechanism of lymphangiogenesis in lung adenocarcinoma. Cancer Res. 64,554–564.
Swartz, M.A., Skobe, M., 2001. Lymphatic function, lymphangiogenesis, andcancer metastasis. Microsc. Res. Tech. 55, 92–99.
Tait, C.R., Jones, P.F., 2004. Angiopoietins in tumours: the angiogenic switch.J. Pathol. 204, 1–10.
Tammela, T., Heckman, C.A., Alitalo, K., 2005a. Lymphangiogenesis andmetastasis. American Association for Cancer Research Educational Book,pp. 67–73.
Tammela, T., Saaristo, A., Lohela, M., Morisada, T., Tornberg, J., Norrmen, C.,Oike, Y., Pajusola, K., Thurston, G., Suda, T., Yla-Herttuala, S., Alitalo, K.,2005b. Angiopoietin-1 promotes lymphatic sprouting and hyperplasia. Blood105, 4642–4648.
Timoshenko, A.V., Chakraborty, C., Wagner, G.F., Lala, P.K., 2006. COX-2-mediated stimulation of the lymphangiogenic factor VEGF-C in humanbreast cancer. Br. J. Cancer 94, 1154–1163.
Tobler, N.E., Detmar, M., 2006. Tumor and lymph node lymphangiogenesis-impact on cancer metastasis. J. Leukoc. Biol. 80, 691–696.
Tsunoda, S., Nakamura, T., Sakurai, H., Saiki, I., 2007. Fibroblast growth factor-2-induced host stroma reaction during initial tumor growth promotes pro-gression of mouse melanoma via vascular endothelial growth factor A-dependent neovascularization. Cancer Sci. 98, 541–548.
Uka, K., Aikata, H., Takaki, S., Shirakawa, H., Jeong, S.C., Yamashina, K.,Hiramatsu, A., Kodama, H., Takahashi, S., Chayama, K., 2007. Clinicalfeatures and prognosis of patients with extrahepatic metastases from hepato-cellular carcinoma. World J. Gastroenterol. 13, 414–420.
Van der Auwera, I., Cao, Y., Tille, J.C., Pepper, M.S., Jackson, D.G., Fox, S.B.,Harris, A.L., Dirix, L.Y., Vermeulen, P.B., 2006. First international consen-sus on the methodology of lymphangiogenesis quantification in solid humantumours. Br. J. Cancer 95, 1611–1625.
Van Trappen, P.O., Steele, D., Lowe, D.G., Baithun, S., Beasley, N., Thiele, W.,Weich, H., Krishnan, J., Shepherd, J.H., Pepper, M.S., Jackson, D.G.,Sleeman, J.P., Jacobs, I.J., 2003. Expression of vascular endothelial growthfactor (VEGF)-C and VEGF-D, and their receptor VEGFR-3, during dif-ferent stages of cervical carcinogenesis. J. Pathol. 201, 544–554.
VonMarschall, Z., Scholz, A., Stacker, S.A., Achen,M.G., Jackson, D.G., Alves,F., Schirner, M., Haberey, M., Thierauch, K.H., Wiedenmann, B., Rosewicz,S., 2005. Vascular endothelial growth factor-D induces lymphangiogenesisand lymphatic metastasis in models of ductal pancreatic cancer. Int. J. Oncol.27, 669–679.
von Rahden, B.H., Stein, H.J., Puhringer, F., Koch, I., Langer, R., Piontek, G.,Siewert, J.R., Hofler, H., Sarbia, M., 2005. Coexpression of cycloox-ygenases (COX-1, COX-2) and vascular endothelial growth factors(VEGF-A, VEGF-C) in esophageal adenocarcinoma. Cancer Res. 65,5038–5044.
Weinberg, A.S., Ogle, C.A., Shim, E.K., 2007. Metastatic cutaneous squamouscell carcinoma: an update. Dermatol. Surg. 33, 885–899.
Wong, S.Y., Haack, H., Crowley, D., Barry, M., Bronson, R.T., Hynes, R.O.,2005. Tumor-secreted vascular endothelial growth factor-C is necessary forprostate cancer lymphangiogenesis, but lymphangiogenesis is unnecessaryfor lymph node metastasis. Cancer Res. 65, 9789–9798.
Xiang, R.H., Hensel, C.H., Garcia, D.K., Carlson, H.C., Kok, K., Daly, M.C.,Kerbacher, K., van den Berg, A., Veldhuis, P., Buys, C.H., Naylor, S.L., 1996.Isolation of the human semaphorin III/F gene (SEMA3F) at chromosome3p21, a region deleted in lung cancer. Genomics 32, 39–48.
Yano, A., Fujii, Y., Iwai, A., Kawakami, S., Kageyama, Y., Kihara, K., 2006.Glucocorticoids suppress tumor lymphangiogenesis of prostate cancer cells.Clin. Cancer Res. 12, 6012–6017.
Yuan, L., Moyon, D., Pardanaud, L., Breant, C., Karkkainen, M.J., Alitalo, K.,Eichmann, A., 2002. Abnormal lymphatic vessel development in neuropilin2 mutant mice. Development 129, 4797–4806.
Zhang, J., Ji, J., Yuan, F., Zhu, L., Yan, C., Yu, Y.Y., Liu, B.Y., Zhu, Z.G., Lin,Y.Z., 2005. Cyclooxygenase-2 expression is associated with VEGF-C andlymph node metastases in gastric cancer patients. Biomed. Pharmacother.59 (Suppl 2), S285–S288.
























![[insert cool codename here] Ames Bielenberg David Saltzman](https://img.pdfslide.net/doc/110x75/56649d2d5503460f94a0457c/insert-cool-codename-here-ames-bielenberg-david-saltzman.jpg)