MONOCLONAL GAMMOPATHIES AND RELATED DISORDERS 0889-8588/99 $8.00 + .OO
ACQUIRED FANCONI'S SYNDROME ASSOCIATED WITH
MONOCLONAL GAMMOPATHIES Martha Q. Lacy, MD, and Morie A. Gertz, MD
Guido Fanconi first described a syndrome in children characterized by renal glycosuria, generalized aminoaciduria, hypophosphatemia, polyuria, and rickets in the absence of azotemia. He postulated deficient renal tubular reabsorption of glucose, amino acids, calcium, and phosphate associated with normal rates of glomerular filtration.z8 At least two forms of inherited Fanconi's syndrome (FS) have been described.'O Subsequently, acquired forms of Fanconi's syndrome were described in adults.28 The differential diagnosis of acquired FS includes monoclonal gammopathies including multiple myeloma and primary systemic amyloidosis, Sjogren's syndrome, inherited enzyme disorders, heavy metal poi- sonings, and toxic drug reactions. This article reviews acquired FS associated with plasma cell dyscrasias.
RENAL COMPLICATIONS OF MONOCLONAL GAMMOPATHIES
Renal dysfunction is commonly associated with monoclonal gammopathies. Fanconi's syndrome is characterized by crystalline cytoplasmic inclusions in the plasma cells of the bone marrow and the renal tubular cells,2* in contrast with multiple myeloma (MM), which often causes renal failure through myeloma cast nephropathy or hypercalcemia. Myeloma casts are large, dense, and waxy and are found in the distal and collecting tubules. They are composed of monoclonal light chains with small amounts of albumin and Tamm-Horsfall protein (THP).l8
Supported in part by NIH Grant CA62242.
From the Division of Hematology and Internal Medicine, Mayo Clinic and Mayo Founda- tion, and Mayo Medical School, Rochester, Minnesota
HEMATOLOGY / ONCOLOGY CLINICS OF NORTH AMERICA ~~ ~
VOLUME 13 * NUMBER 6 DECEMBER 1999 1273

1274 LACY & GERTZ
Nephrotic syndrome is the most common renal manifestation of primary sys- temic amyloidosis. Amyloid deposition is found in mesangial or glomerular basement membranes.18 Light-chain deposition disease is characterized by depo- sition of monoclonal light chains in the renal glomerulus, leading to renal insufficiency and nephrotic syndrome.'*
PATHOLOGY AND PATHOGENESIS OF ACQUIRED FANCONI'S SYNDROME
Kidney biopsies viewed by light microscopy may reveal cytoplasmic crystals in proximal tubule cells7, 11, u, 3o or tubulointerstitial nephritis without glomerular lesions. Immunofluorescence studies have shown that the crystals stain strongly for monoclonal light chain. These findings have been confirmed by electron microscopy and by immunoelectron microscopic techniques.=, 30 Similar cyto- plasmic crystalline inclusions are also seen in bone marrow plasma cells and macrophages.7, 26
The critical role of the proximal renal tubule in the catabolism of light chains was shown in a rat model? Investigators were able to induce proximal tubular lesions in rats by the intraperitoneal injection of human K-type Bence Jones proteins. They found that approximately 80% of injected K-chains were reabsorbed by the proximal tubular cells, where they formed crystal-like struc- tures with phagolysosomes.
In an elegant series of investigations,l, 19, 24 Aucouturier et a1 showed that light-chain toxicity in FS is related to the resistance of the V domain to degrada- tion in lysosomes of the proximal tubular epithelial cells. Initially, they investi- gated light chains from a single patient with FS.' The sequence of the patient's monoclonal K-chain was determined by cloning the K complementary DNA (cDNA) sequences from bone marrow plasma cells. Analysis of tubular crystals by N-terminal sequencing and mass spectrometry showed that the crystals were composed primarily of the V domain of the K light chain together with small proportions of the entire light chain, suggesting posttranscriptional degradation in the lysosomes. Protease treatment of the K light chain yielded a fragment of the V domain that, in contrast with other K light chains, was completely resistant to further proteolytic degradation. In addition, the patient's light chain displayed an unusual self-avidity.
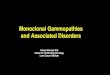
These studies prompted further investigations by the same group. They studied light chains from 4 patients with FS, 12 patients with cast nephropathy, and 4 control patients.19 All the light chains from patients with FS were of the K type. Kinetic studies of light-chain digestion by pepsin and cathepsin B showed generation of a protease-resistant 12-kDa fragment corresponding to the V do- main of the light chain. In contrast, digestion studies of the light chains obtained from patients with cast nephropathy had a variable pattern of protease resistance (Fig. 1). All the light chains from myeloma patients without cast nephropathies were completely digestible. In addition, light chains from patients with FS showed avidity for light chains but no reactivity with THP. The majority of the light chains from cast nephropathy patients bound to THP. Finally, the group demonstrated a preponderance of sequences of the V K ~ subgroup among patients with FS.24
These studies suggest that complete proteolysis of the K light chain cannot occur in vivo after endocytosis by the proximal tubule cells. As a result, the V fragment accumulates in the lysosomal compartment of the cells. Reactivity with light chains from normal polyclonal immunoglobulin G (IgG), which is

Fig
ure
1. K
appa
ligh
t cha
ins
are
endo
cyto
sed
by ly
soso
mes
. Und
er n
orm
al c
ondi
tions
, the
y ar
e co
mpl
etel
y deg
rade
d by
pro
teas
es in
clud
ing
peps
in a
nd c
athe
psin
D.
In p
atie
nts
with
Fan
coni
’s s
yndr
ome,
pro
teas
e-re
sist
ant 1
2 kD
a fra
gmen
ts c
orre
spon
ding
to t
he V
dom
ain
are
gene
rate
d. T
hese
frag
men
ts a
vidl
y bi
nd to
oth
er l
ight
cha
ins
and
serv
e as
a n
idus
for
crys
tal f
orm
atio
n.

1276 LACY & GERTZ
Tubule lumen
Crystal-laden lysosomes
Peritubule space
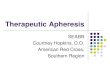
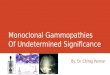
Figure 2. Crystal-laden lysosomes interfere with a broad range of apical membrane trans- porters.
continuously filtered by the glomerulus and reabsorbed in the proximal tubules, may serve as a nidus for crystal formation. The crystals interfere with a broad range of apical membrane transporters, including the sodium-hydrogen (Na-H) exchangers and sodium-linked symporters for glucose, phosphate, urate, and amino acids (Fig. 2).'QI9
CLINICAL MANIFESTATIONS OF ACQUIRED FANCONI'S SYNDROME
Patients with FS most often seek medical attention for back or bone pain, fatigue, or myalgias.zl, 25 Proximal muscle weakness is not uncommon. Symptoms are frequently confused with myeloma bone pain. Many patients with FS are asymptomatic, and the finding of glycosuria, proteinuria, electrolyte abnormali- ties, or renal insufficiency triggers the work-up. Unexplained hypouricemia may be the only clue to a diagnosis of FS.
Electrolyte and Renal Abnormalities
Mild and slowly progressive renal insufficiency is commonly seen in FS.21, 25
Renal failure often stabilizes or improves with ~hemotherapy.'~, 31, 32 Electrolyte abnormalities typically include hypokalemia, hypophosphatemia, and hypouri- cemia. The diagnosis is confirmed by the demonstration of aminoaciduria and

ACQUIRED FANCONI'S SYNDROME WITH MONOCLONAL GAMMOPATHIES 1277
glycosuria. The renal dysfunction is a constellation of proximal tubule transport defects resulting in broad failure of tubule reabsorption. The kaliuresis is not a direct effect but rather is a consequence of the delivery of large amounts of bicarbonate past the distal nephron under conditions that favor aldosterone secretion.'O
Bone Findings
Osteomalacia, with or without 1,25-dihydroxyvitamin D deficiency, has been seen in patients with acquired FS and is a result of prolonged hypophos- phatemia.5, 20, 23 Roentgenograms are often normal but may show demineraliza- tion, fractures, or pseudofractures." 21 Lytic lesions suggest fully developed multi- ple myeloma. When roentgenograms are normal, the presence of osteomalacia may be suggested by an elevated serum alkaline phosphatase?, 21, In the absence of overt myeloma, bone pain may be dramatically relieved by treatment with phosphorus (NeutraPhos), with or without calcitriol. Complete reversal of the osteomalacia has been demonstrated by repeat bone biopsies after treatment with phosphoru~.~~ Noninvasive methods of assessing treatment efficacy include following serum alkaline phosphatase and phosphate levels and 24-hour urine calcium excretion.
The primary cause of osteomalacia in FS is proximal renal tubular phosphate wasting? The degree of osteomalacia correlates with the duration and severity of the hypophosphatemia.2 Osteomalacia, however, may develop even in the face of normal serum phosphorus levels, because these patients invariably have high fractional excretions of phosphorus? This can eventually lead to secondary hyperparathyroidism. Parathyroid hormone levels (PTH) were elevated in two of nine FS patients with osteomalacia in one series? Low levels of 1,25-dihydroxy- vitamin D levels may be seen and are presumed to be caused by low serum phosphorus, which is a potent stimulus of renal la-hydroxylase. Chronic acido- sis is often seen in FS and may contribute to the osteomalacia by decreasing the conversion of amorphous calcium phosphate to hydroxyapatite?
Predominance of K Light Chains
Bence Jones proteinuria is usually present and is almost always of the K
type.2l. 25 Rare patients with FS associated with X-type Bence Jones proteinuria have been re~0rted. l~~ 29 The authors observed that 22 of 23 patients with FS (96%) had K-type Bence Jones pr~teinuria;~ and a monoclonal protein was found in the serum in 60% of patients.
Association with Malignant Disease
Fanconi's syndrome may be seen in association with overt hematologic malignant disease or may be associated with indolent processes such as mono- clonal gammopathy of undetermined significance (MGUS) or idiopathic Bence Jones proteinuria (IBJP). The most common associated malignancy is multiple myeloma.4, 7-9, 11, 1S17, 21-23, 2528, 3&33 F anconi's syndrome has also been associated with primary amyloidosis,lz, 27 Waldenstrom's macr~globulinemia,~~ and chronic lymphocytic leukemia.23 Like MGUS and IBJP, FS may predate a malignant diagnosis by many years. One report described FS that was present for 16.5

1278 LACY & GERTZ
years before the development of overt myeloma.*l In the experience at the Mayo Clinic, only one third of patients present with a malignant disease at the time FS is diagn~sed?~ Only one patient in the authors‘ series who did not have myeloma at the time of diagnosis of FS went on to develop overt myeloma, 37 months later. In the authors’ experiences FS is an indolent disorder with a median survival of 91 months. Patients rarely die of the disease. Causes of death include multiple myeloma, complications of chemotherapy, infections, and unrelated disea~es.2~
TREATMENT OF FANCONI’S SYNDROME
Franconi’s syndrome is an indolent disorder in patients without overt multi- ple myeloma. Complications such as renal insufficiency develop gradually. In the asymptomatic patient, it is appropriate to withhold potentially toxic chemo- therapy. Treatment with phosphorus, calcium, and calcitriol may improve bone pain and ameliorate osteomalacia. In the setting of progressive renal dysfunction or symptomatic malignant disease, chemotherapy such as melphalan and pred- nisone may be of benefit.l3? 31, 32
SUM MARY
Franconi’s syndrome is a rare complication of the monoclonal gammopa- thies characterized by diffuse failure in reabsorption at the level of the proximal renal tubule resulting in glycosuria, generalized aminoaciduria, and hypophos- phatemia. Current evidence suggests monoclonal light chains that are incom- pletely digested in renal tubule lysosomes cause renal injury. The light-chain fragments serve as a nidus for crystal formation, and the crystals interfere with a broad range of apical membrane transporters. Franconi’s syndrome is predominantly associated with monoclonal K in the urine, but rare instances of FS caused by A light chains have been described.
Overt hematologic malignancies such as multiple myeloma, Waldenstrom’s macroglobulinemia, or other lymphoproliferative disorders occur in one third of patients. Clinical manifestations include slowly progressive renal failure and bone pain caused by osteomalacia. The osteomalacia is caused by chronic hypo- phosphatemia and may be exacerbated by secondary hyperparathyroidism and renal tubular acidosis. Treatment consists of supplementation with phosphorus, calcium, and vitamin D. The osteomalacia is often completely reversible with mineral supplementation. Patients with an associated symptomatic malignancy or rapidly progressive renal failure may also benefit from chemotherapy. The prognosis is good in the absence of overt malignant disease.
References
1. Aucouturier P, Bauwens M, Khamlichi AA, et al: Monoclonal Ig L chain and L chain V domain fragment crystallization in myeloma-associated Fanconi’s syndrome. J Immunol 150:3561-3568, 1993
2. Bell NH: Osteomalacia and rickets. In Becker KL: Principles and Practice of Endocrinol- ogy. Philadelphia, J. 8. Lippincott, 1990
3. Bergeron M, Scriver CR Pathophysiology of renal hyperaminoacidurias and glucosu-

ACQUIRED FANCONI'S SYNDROME WITH MONOCLONAL GAMMOPATHIES 1279
ria. In Seldin DW: The Kidney: Physiology and Pathophysiology. New York, Raven Press, 1992
4. Chan KW, Ho FCS, Chan MK Adult Fanconi syndrome in K light chain myeloma. Arch Pathol Lab Med 111:139-142, 1987
5. Clarke BL, Wynne AG, Wilson DM, et al: Osteomalacia associated with adult Fanconi's syndrome: Clinical and diagnostic features. Clin Endocrinol (Oxf) 43:479490, 1995
6. Clyne DH, Brendstrup L, First MR, et al: Renal effects of intraperitoneal kappa chain injection. Lab Invest 31:131-142, 1974
7. Costanza DJ, Smoller M: Multiple myeloma with the Fanconi syndrome. Am J Med 34:125-133, 1963
8. Dedmon RE, West JH: The adult Fanconi syndrome: Report of two cases, one with multiple myeloma. Med Clin North Am 47191-206, 1963
9. Dragsted PJ, Hjorth N: The association of the Fanconi syndrome with malignant disease. Dan Med Bull 3:177-179, 1956
10. Eiam-Ong S, Laski ME, Kurtzman NA: Diseases of renal adenosine triphosphatase [review]. Am J Med Sci 309:13-25, 1995
11. Engle RL, Wallis LA: Multiple myeloma and the adult Fanconi syndrome. Am J Med 22523, 1957
12. Finkel PN, Kronenberg K, Pesce AJ, et al: Adult Fanconi syndrome, amyloidosis and marked K-light chain proteinuria. Nephron 101-24, 1973
13. Gailani S, Seon B-K, Henderson ES: K light chain-myeloma associated with adult Fanconi syndrome: Response of the nephropathy to treatment of myeloma. Med Pediatr Oncol4141-147, 1978
14. Harrison JF, Blainey JD: Adult Fanconi syndrome with monoclonal abnormality of immunoglobulin light chain. J Clin Pathol 20:4248, 1967
15. Headley RN, King JS, Cooper MR, et al: Multiple myeloma presenting as adult Fanconi syndrome. Clin Chem 18293-295, 1972
16. Horn ME, Knapp MS, Page FT, et al: Adult Fanconi syndrome and multiple myeloma- tosis. J Clin Pathol 22:414-416, 1969
17. Isobe T, Kametani F, Shinoda T V-domain deposition of lambda Bence Jones protein in the renal tubular epithelial cells in a patient with the adult Fanconi syndrome with myeloma. Amyloid 5:117-120, 1998
18. Kyle RA: Monoclonal proteins and renal disease. Annu Rev Med 45:71-77, 1994 19. Leboulleux M, Lelongt B, Mougenot B, et al: Protease resistance and binding of Ig
light chains in myeloma-associated tubulopathies. Kidney Int 48:72-79, 1995 20. Lee DBN, Drinkard JP, Rosen VJ, et al: The adult Fanconi syndrome: Observations on
etiology, renal function, and mineral metabolism in three patients. Medicine (Baltimore)
21. Maldonado JE, Velosa JA, Kyle RA, et al: Fanconi syndrome in adults. A manifestation of a latent form of myeloma. Am J Med 583356364, 1975
22. Orfila C, Lepert J-C, Modesto A, et al: Fanconi's Syndrome, kappa light-chain myeloma, non-amyloid fibrils and cytoplasmic crystals in renal tubular epithelium. Am J Nephrol 11:345-349, 1991
23. Rao DS, Parfitt AM, Villanueva AR, et al: Hypophosphatemic osteomalacia and adult Fanconi syndrome due to light-chain nephropathy: Another form of oncogenous osteo- malacia. Am J Med 82333-338, 1987
24. Rocca A, Khamlichi AA, Touchard G, et al: Sequences of V kappa L subgroup light chains in Fanconi's syndrome. Light chain V region gene usage restriction and peculiar- ities in myeloma-associated Fanconi's syndrome. J Immunol 155:3245-3252, 1995
25. Rompala JF, Lacy MQ, Rajkumar SV, et al: Acquired Fanconi's syndrome is an indolent disorder in the absence of overt multiple myeloma [abstract 41601. Blood 92:269b, 1998
26. Sewell RL, Dorreen M S Adult Fanconi syndrome progressing to multiple myeloma. J Clin Pathol371256-1258, 1984
27. Short IA, Smith JP: Myelomatosis associated with glycosuria and aminoaciduria. Scott Med J 489-93, 1959
28. Sirota JH, Hamerman D: Renal function studies in an adult subject with the Fanconi syndrome. Am J Med 16:138-152, 1954
51~107-138, 1972

1280 LACY & GERTZ
29. Thomer PS, Bedard YC, Femandes BJ: A-light-chain nephropathy with Fanconi's syn- drome. Arch Pathol Lab Med 107654657, 1983
30. Truong LD, Mawad J, Cagle P, et al: Cytoplasmic crystals in multiple myeloma- associated Fanconi's syndrome. Arch Pathol Lab Med 113:781-785, 1989
31. Uchida S, Matsuda 0, Yokota T, et al: Adult Fanconi syndrome secondary to K-light chain myeloma: Improvement of tubular functions after treatment for myeloma. Nephron 55:332-335, 1990
32. von Scheele C: Light chain myeloma with features of the adult Fanconi syndrome: Six years remission following one course of melphalan. Acta Medica Scandinavica 199:533-537, 1976
33. Yonemura K, Matsushima H, Kato A, et al: Acquired Fanconi syndrome associated with IgG kappa multiple myeloma: Observations on the mechanisms of impaired renal acid excretion. Nephrol Dial Transplant 12:1251-1253, 1997
Address reprint requests to Martha Q. Lacy, MD
The Mayo Clinic 200 First Street, SW
Rochester, MN 55905
Recommended