From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
218
Appendix A-1
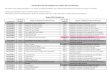
Seventh Characters by Code Category
Code Category Applicable 7th Characters
S00, S01, S03, S05, S06, S09, S10, S11, S12.8, S12.9, S13–S16, S20, S21, S24, S27, S30, S31, S33–S34, S36–S37, S39–S41, S43, S46, S50–S51, S53, S56, S59.8-, S60–S61, S63, S65–S67, S70–S71, S73, S76, S79.8, S80–S81, S83, S86, S89.8, S90–S91, S93, S96, S97, T15–T28, T36– T85, T88
A — initial encounterD — subsequent encounterS — sequela
Code Category Applicable 7th Characters
S02, S12.0–S12.6, S22, S32 A — initial encounter for closed fractureB — initial encounter for open fractureD — subsequent encounter for fracture with routine healingG — subsequent encounter for fracture with delayed healingK — subsequent encounter for fracture with nonunionS — sequela
Code Category Applicable 7th Characters
S42, S52, S62, S92 A — initial encounter for closed fractureB — initial encounter for open fractureD — subsequent encounter for fracture with routine healingG — subsequent encounter for fracture with delayed healingK — subsequent encounter for fracture with nonunionP — subsequent encounter for fracture with malunionS — sequela
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

219
Code Category Applicable 7th Characters
M80, M84.3–M84.6, S49, S59 (except S59.8-), S72.47, S79.0–S79.1, S82.16, S82.31, S82.81–S82.82-, S89.0–S89.3
A — initial encounter for closed fractureD — subsequent encounter for fracture with routine healingG — subsequent encounter for fracture with delayed healingK — subsequent encounter for fracture with nonunionP — subsequent encounter for fracture with malunionS — sequela
Code Category Applicable 7th Characters
S72 (except S72.47-), S82 (except S82.16-, S82.31-, S82.81 and S81.82)
A — initial encounter for closed fractureB — initial encounter for open fracture type I or II initial encounter for open fracture NOSD — subsequent encounter for closed fracture with routine healingE — subsequent encounter for open fracture type I or II with routine healingG — subsequent encounter for closed fracture with delayed healingH — subsequent encounter for open fracture type I or II with delayed healingK — subsequent encounter for closed fracture with nonunionM — subsequent encounter for open fracture type I or II with nonunionP — subsequent encounter for closed fracture with malunionQ — subsequent encounter for open fracture type I or II with malunionS — sequela
Injury/status codes to which no 7th characters are assigned
T07, T14, T30–T32, T86–T87, Y07, Y09, Y62–90, Y92–Y93, Y99
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

220
Category Description Related Terms Not Intractable Intractable
G40.0 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes w/ seizures of localized onset
Benign childhood epilepsy w/ centrotemporal EEG spikes
Childhood epilepsy w/ occipital EEG paroxysms
G40.001 Not intractable,w/ statusepilepticusG40.009 Not intractable,w/o statusepilepticus
G40.011Intractable, w/ statusepilepticusG40.019Intractable,w/o statusepilepticus
G40.1 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes w/ simple partial seizures
Attacks w/o alteration of consciousness
Epilepsia partialis continua [Kozhevnikof]
Simple partial seizures developing into secondarily generalized seizures
FocalBravais-
JacksonianSomatomotorSomatosensory
G40.101 Not intractable,w/ statusepilepticusG40.109 Not intractable,w/o statusepilepticus
G40.111Intractable,w/ statusepilepticusG40.119Intractable,w/o statusepilepticus
G40.2 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes w/ complex partial seizures
Attacks w/ alteration of consciousness, often w/ automatisms
Complex partial seizures developing into secondarily generalized seizures
G40.201 Not intractable,w/ statusepilepticusG40.209 Not intractable,w/o statusepilepticus
G40.211Intractable, w/ statusepilepticusG40.219Intractable,w/o statusepilepticus
Appendix A-2
ICD-10-CM Codes for Epilepsy by Type
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

221
Category Description Related Terms Not Intractable Intractable
G40.3 Generalized idiopathic epilepsy and epileptic syndromes
G40.301 Not intractable,w/ statusepilepticusG40.309 Not intractable,w/o statusepilepticus
G40.311Intractable, w/ statusepilepticusG40.319Intractable,w/o statusepilepticus
G40.A Absence epileptic syndrome
Childhood absence epilepsy [pyknolepsy]
Juvenile absence epilepsy
Absence epileptic syndrome, NOS
G40.A01 Not intractable,w/ statusepilepticusG40.A09 Not intractable,w/o statusepilepticus
G40.A11Intractable,w/ statusepilepticusG40.A19Intractable,w/o statusepilepticus
G40.B Juvenile myoclonic epilepsy [impulsive petit mal]
G40.B01 Not intractable,w/ statusepilepticusG40.B09 Not intractable,w/o statusepilepticus
G40.B11Intractable,w/ statusepilepticusG40.B19Intractable,w/o statusepilepticus
G40.4 Other generalized epilepsy and epileptic syndromes
Myoclonus, epileptic
Seizure, grand malSeizure, petit mal
G40.401 Not intractable,w/ statusepilepticusG40.409 Not intractable,w/o statusepilepticus
G40.411Intractable,w/ statusepilepticusG40.419Intractable,w/o statusepilepticus
(continued on page 222)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

222
Category Description Related Terms Not Intractable Intractable
G40.5 Epileptic seizures related to external causes
Epileptic seizures related to alcohol
Epileptic seizures related to drugs
Epileptic seizures related to hormonal changes
Epileptic seizures related to sleep deprivation
Epileptic seizures related to stress
G40.501 Not intractable,w/ statusepilepticusG40.509 Not intractable,w/o statusepilepticus
G40.80 Other epilepsy
Epilepsies and epileptic syndromes undetermined as to whether they are focal or generalized
Landau-Kleffner syndrome
G40.801 Not intractable,w/ statusepilepticusG40.802 Not intractable,w/o statusepilepticus
G40.803Intractable,w/ statusepilepticusG40.804Intractable,w/o statusepilepticus
G40.81 Lennox-Gastaut syndrome
G40.811 Not intractable,w/ statusepilepticusG40.812 Not intractable,w/o statusepilepticus
G40.813Intractable,w/ statusepilepticusG40.814Intractable,w/o statusepilepticus
G40.82 Epileptic spasms
Infantile spasmsSalaam attacksWest syndrome
G40.821 Not intractable,w/ statusepilepticusG40.822 Not intractable,w/o statusepilepticus
G40.823Intractable,w/ statusepilepticusG40.824Intractable,w/o statusepilepticus
Appendix A-2ICD-10-CM Codes for Epilepsy by Type (continued from page 221)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

223
Category Description Related Terms Not Intractable Intractable
G40.9 Epilepsy, unspecified
G40.909 Only Epilepsy
NOSEpileptic
convulsions NOS
Epileptic fits NOSEpileptic seizures
NOSRecurrent seizures
NOSSeizure disorder
NOS
G40.901 Not intractable,w/ statusepilepticusG40.909 Not intractable,w/o statusepilepticus
G40.911Intractable,w/ statusepilepticusG40.919Intractable,w/o statusepilepticus
From American Academy of Pediatrics. Principles of Pediatric ICD-10-CM Coding. 2013:255–257.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

224
W21 Striking against or struck by sports equipment Excludes1: assault with sports equipment (Y08.0-) striking against
or struck by sports equipment with subsequent fall (W18.01)
The appropriate 7th character is to be added to each code from category W21.A — initial encounterD — subsequent encounterS — sequela
W21.00X√ Struck by hit or thrown ball, unspecified typeW21.01X√ Struck by footballW21.02X√ Struck by soccer ballW21.03X√ Struck by baseballW21.04X√ Struck by golf ballW21.05X√ Struck by basketballW21.06X√ Struck by volleyballW21.07X√ Struck by softballW21.09X√ Struck by other hit or thrown ballW21.11X√ Struck by baseball batW21.12X√ Struck by tennis racquetW21.13X√ Struck by golf clubW21.19X√ Struck by other bat, racquet or clubW21.210√ Struck by ice hockey stickW21.211√ Struck by field hockey stickW21.220√ Struck by ice hockey puckW21.221√ Struck by field hockey puckW21.31X√ Struck by shoe cleats (Stepped on)W21.32X√ Struck by skate blades (Skated over)W21.39X√ Struck by other sports foot wearW21.4XX√ Striking against diving board
Use additional code for subsequent falling into water, if applicable (W16.-).W21.81X√ Striking against or struck by football helmetW21.89X√ Striking against or struck by other sports equipment
Appendix A-3
ICD-10-CM Codes to Identify Object in Injury Due to Striking/Struck By Sports Equipment
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

225
When International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) is released, guidelines for reporting on certain infectious and parasitic diseases will be found in Chapter 1 of the tabular list (codes A00–B99).
This article will provide an overview of those guidelines (with the exception of guidelines for reporting sepsis, which was reviewed in the November 2014 AAP Pediatric Coding Newsletter™). For this and other articles in the “Transitioning to 10” series, please see the Transitioning to 10 collection at http://coding.solutions.aap.org/transitioning.aspx.
HIV InfectionsCode B20, HIV disease, is reported as follows:
■■ Report B20 only for cases confirmed by a physician’s statement that the patient has symptomatic HIV, an HIV-related illness, or history of an HIV-related illness.
■■ Inconclusive laboratory evidence of HIV is reported with code R75.■■ Report first the code for HIV (B20) when the reason for the encounter is an HIV-
related condition. Related conditions are additionally reported. When an encounter for a patient with HIV disease is for unrelated conditions, report first the condition most responsible for the encounter followed by the code for HIV disease.
■■ Encounters for patients who are HIV-positive but without symptoms or documenta-tion of any HIV-related condition or history of an HIV-related condition are reported using code Z21, asymptomatic HIV infection status, rather than code B20.
Code Z11.4 is appropriate for reporting an encounter for screening for HIV. Additional codes identifying high-risk behavior may also be assigned. Counseling about HIV in the absence of a positive HIV result is reported with code Z71.7. For patients with a positive HIV result, report code Z21 or, if symptomatic, code B20.
Infectious Agents as the Cause of Diseases Classified to Other ChaptersCategories B95–B97 are used to report an identified infectious agent when a disease is classified in chapters other than Chapter 1 of the tabular list and the code descriptor does not include the infectious agent. An instruction at the code for the condition will typically instruct to also code any known infectious agent.
ExampleA child has a urinary tract infection with Escherichia coli identified as the infectious agent. The code for the urinary tract infection is listed first, followed by the code identifying the infectious agent.N39.0 Urinary tract infection, site not specifiedB96.20 Unspecified Escherichia coli [E coli] as the cause
of diseases classified elsewhere
Appendix B-1
Infection
(continued on page 226)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

226
Infections Resistant to AntibioticsSome code categories in ICD-10-CM include codes specifying antibiotic resistance. When antibiotic resistance has been identified but the appropriate code for the infection does not indicate resistance, report the code for the infection followed by code Z16, resistance to antimicrobial drugs.
ExamplesOnly one code is necessary to report methicillin-resistant Staphylococcus aureus (MRSA) infection. A49.02 Methicillin resistant Staphylococcus aureus infection, unspecified site
To identify penicillin resistance in a patient with an E coli infection of the urinary tract, 3 codes are reported.N39.0 Urinary tract infection, site not specifiedB96.20 Unspecified Escherichia coli [E coli] as the cause
of diseases classified elsewhereZ16.11 Resistance to penicillins
Methicillin-Resistant Staphylococcus aureus ConditionsCombination codes are included in ICD-10-CM to identify sepsis or pneumonia due to MRSA. When MRSA is identified as the cause of a condition for which no combination code is provided, code B95.62, MRSA infection as the cause of diseases classified else-where, is reported in addition to the code for the related condition. It is not necessary to also report resistance to penicillins (Z16.11) when reporting MRSA.
Examples Only one code is required to report pneumonia due to MRSA.J15.212 Pneumonia due to methicillin-resistant Staphylococcus aureus
Reporting cellulitis due to MRSA requires 2 codes.L03.115 Cellulitis of right lower limbB95.62 Methicillin-resistant Staphylococcus aureus as the cause of diseases
classified elsewhere
Colonization or positive screening for methicillin-susceptible Staphylococcus aureus or MRSA is reported with codes in category Z22.Z22.321 Carrier or suspected carrier of methicillin-susceptible Staphylococcus
aureusZ22.322 Carrier or suspected carrier of methicillin-resistant Staphylococcus aureus
For patients identified as having a history of MRSA infection, report code Z86.14.Z86.14 Personal history of methicillin-resistant Staphylococcus aureus infection
For full information on the ICD-10-CM guidelines for these and other conditions, see the ICD-10-CM Official Guidelines for Coding and Reporting 2015 in the ICD-10-CM manual or online at www.cdc.gov/nchs/icd/icd10cm.htm.
Appendix B-1Transitioning to 10: Infection (continued from page 225)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

227
By now, you may know that the term for a late effect in International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) is sequela. In addition to changing the terminology for describing a late effect of a disease or injury, ICD-10-CM also approaches different types of sequelae in different ways.
In this article, we will review the guidelines for reporting sequelae and look at some examples of codes that are used to report them.
GuidelinesThe guidelines for ICD-10-CM instruct
■■ A sequela is the residual effect (condition produced) after the acute phase of an illness or injury has terminated.
■■ There is no time limit on when a sequela code can be used. The residual may be apparent early, such as in cerebral infarction, or it may occur months or years later, such as that caused by a previous injury.
■■ Coding of sequela generally requires 2 codes sequenced in the following order: The condition or nature of the sequela is sequenced first (ie, the patient’s residual condition or complication that represents the sequela is sequenced first). The sequela code is sequenced second.
■● This guideline applies except when the code for the sequela is followed by a manifestation code identified in the ICD-10-CM tabular list and title (eg, the tabular list instructs code first sequelae of traumatic intracranial injury codes S06.- when reporting pseudobulbar effect code F48.2) or the sequela code has been expanded to include the manifestation.
■■ The code for the acute phase of an illness or injury is not used in conjunction with a code for the sequela. (Exception: A current injury code is reported for a burn that is still in the acute phase of healing, while a sequela code may be reported at the same encounter related to effects of another healed burn.)
■■ The external cause-of-injury code with the seventh character S for sequela should be used with any report of a late effect or sequela resulting from a previous injury.
Some examples may help illustrate these guidelines.
Example 1Probably the most discussed approach to identifying an encounter to address a sequela is the use of seventh character S when reporting an injury, poisoning, or external cause of injury. Most categories of injury in ICD-10-CM include 3 choices for the seventh character appended to complete each code: A, initial encounter; D, subsequent encounter; or S, sequela.
Appendix B-2
Late Effects or Sequela
(continued on page 228)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

228
A child is diagnosed with partial physeal arrest as a late effect of a Salter-Harris type II physeal fracture of the distal right tibia caused by falling from his skateboard.
M89.166 Partial physeal arrest, right distal tibiaS89.121S Salter-Harris Type II physeal fracture of lower end of right tibiaV00.131S Fall from skateboard
Note: The sequence of codes begins with the nature of the sequela (partial physeal arrest), followed by codes describing the related injury and external cause of injury ending with seventh character S to indicate the first-listed condition is a sequela of this injury.
TIp: Be sure to include any placeholders (X) necessary to complete a code to the seventh character (eg, S02.2XXS is used to report sequela of fracture of nasal bones).
Example 2A girl who was hospitalized for viral encephalitis 3 months ago is evaluated for learning difficulties that have presented and persisted since the episode of encephalitis. Assessment is deficit of attention and concentration as a late effect of viral encephalitis with probable attention-deficit/hyperactivity disorder (ADHD).
R41.840 Attention and concentration deficitB94.1 Sequelae of viral encephalitis
Note: In this example, code B94.1 requires no additional character to identify a sequela of viral encephalitis. Codes in categories B90–B94 are used to report sequelae of infectious and parasitic diseases. An instruction at categories B90–B94 directs to code first the condition resulting from the sequela of the infectious or parasitic disease.
(Note: The “probable” or unconfirmed diagnosis of ADHD is not reported.) Similar codes for sequela are provided for other conditions. Examples include
E64.0 Sequelae of protein-calorie malnutrition (Does not include retarded development following protein-calorie malnutrition [E45]. Report E45 also when appropriate.)E68 Sequelae of hyperalimentationG09 Sequelae of inflammatory diseases of central nervous systemG65.0 Sequelae of Guillain-Barré syndromeG65.1 Sequelae of other inflammatory polyneuropathyG65.2 Sequelae of toxic polyneuropathyI69.31 Cognitive deficits following cerebral infarction
Locating CodesFor sequela of conditions other than injuries, always start with the term Sequelae in the alphabetic index of ICD-10-CM for reference to the correct code category and follow any further directions for reporting as provided in the tabular list. For injuries, see the type of injury (eg, burn, crushing injury) by site with seventh character S. External cause of injury is also indexed by cause and reported with the appropriate code appended with seventh character S.
Appendix B-2Transitioning to 10: Late Effects or Sequela (continued from page 227)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

229
As we approach October 1, 2013, and the last scheduled year of reporting diagnoses with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), there remains a good deal of misinformation about the soon to be adopted International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) code set. Often when ICD-10-CM is discussed, it is noted that unspecified codes may be denied when reporting diagnoses with ICD-10-CM. Likewise, it has been noted that the abun-dance of external cause codes available to describe circumstances related to injuries and conditions will greatly increase the number of codes reported. A statement released by the 4 cooperating parties (American Health Information Management Association, American Hospital Association, Centers for Medicare & Medicaid Services, National Center for Health Statistics) for ICD-10-CM/PCS (PCS is the inpatient procedural por-tion of ICD-10-CM) and ICD-9-CM in May 2013 offers important clarification on these topics. The statement, which can be found online at http://library.ahima.org/xpedio /groups/public/documents/government/bok1_050189.hcsp?dDocName=bok1_050189, should resolve some confusion and concerns about adoption of ICD-10-CM.
This article will focus on the clarifications of use of unspecified codes and codes for signs and symptoms. Clarification of external cause code use will be reviewed in a future issue of AAP Pediatric Coding Newsletter™.
The cooperating parties clearly state that unspecified codes have acceptable, even neces-sary uses. An unspecified code or codes for signs and symptoms may be reported when it would be inappropriate to assign a specific code not supported by medical record doc- umentation or when unnecessary diagnostic testing would determine a more specific code. Any reporting would need to be based on the information available in medical record documentation. Following are guidelines for reporting an unspecified code or signs and symptoms:
• Codes should reflect what is known about the patient’s condition at the time ofthe encounter.
• If no definitive diagnosis is determined at an encounter, codes for signs andsymptoms should be reported.
• It is appropriate to report an unspecified code when clinical information is notknown or not available for a diagnosed condition.
• For those categories for which an unspecified code is not provided, the “otherspecified” code may represent other and unspecified.
• When documentation lacks information that was likely known at the time of theencounter (eg, laterality), it is appropriate for a coder to query the physician orprovider for additional information to determine if a specific code may be assignedbased on an addendum to the record.
Appendix B-3
Important ICD-10-CM Clarification: Use of Unspecified Codes
(continued on page 230)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

230
Examples
Use of an Unspecified Code A child is seen for a sore throat. The strep test result is negative. Diagnosis is acute pharyngitis. In ICD-9-CM, code 462, acute pharyngitis, is reported. In ICD-10-CM, code J02.9, acute pharyngitis, unspecified, is reported. Like ICD-9-CM, ICD-10-CM includes codes for pharyngitis due to certain specified organisms (eg, Streptococcus, Coxsackie virus) that are reported when documented.
Query for Information to Assign a Specific Code Documentation indicates that a child is seen for initial evaluation of a superficial foreign body of the thumb with no significant wound and no signs of infection. This documen- tation supports a specific ICD-9-CM code, 915.6, superficial foreign body (splinter) without major open wound and without mention of infection. However, documenta- tion must include laterality for a specific code to be reported in ICD-10-CM. Code S60.369A, initial encounter for super-ficial foreign body of unspecified thumb, may be reported if the thumb is not documented as right or left. However, it would be more appropriate for the coder to query the physician or provider for the additional informa-tion necessary to choose a more specific code including laterality and request that an addendum to the medical record be used to document this (addendum must include current date and be signed by the provider prior to claim submission).
Reporting of Signs and SymptomsDocumentation for hospital care indicates that a 2-week-old was admitted with a diag- nosis of “rule out sepsis.” Sepsis is ruled out, and discharge diagnoses are fever of unknown origin and poor feeding. ICD-9-CM codes reported for the physician’s services are 778.4, other disturbances of temperature regulation of newborn, and 779.31, feeding problems in newborn. ICD-10-CM codes reported are p81.9, disturbance of temperature regulation of newborn, unspecified, and p92.9, feeding problem of newborn, unspecified. A code for sepsis is not reported because conditions documented with terms such as probable, suspected, or rule out are not reported in conjunction with physician charges.
Hopefully, the next year will bring more reassuring information about the adoption of ICD-10-CM. Until then, take note that while ICD-10-CM does require planning and changes in many areas of practice, it does not change everything. Most guidelines are similar to ICD-9-CM, and many physicians already document sufficiently to support the greater specificity of ICD-10-CM diagnoses such as asthma classification and laterality.
Appendix B-3Transitioning to 10: Important ICD-10-CM Clarification: Use of Unspecified Codes (continued from page 229)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

231
The revisions to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) guidelines in 2015 provide guidance on the appropriate reporting of initial or subsequent encounters for injuries. Previously, the guidelines instructed that an initial encounter was reported for active treatment, which included evaluation and treatment by a new physician. The revised guidelines clarify that seventh character A is appropriately reported for any encounter for active treatment of a fracture, injury, or complication of care. Per ICD-10-CM guidelines, examples of active treatment are surgical treatment, emergency department encounter, and evaluation and continuing treatment by the same or a different physician. Because the guidelines specify that a sub- sequent encounter addresses the recovery or healing phase, the active treatment required for an initial encounter may be considered to be the visits, interventions, and assessments that are applied during the initial course of the injury to establish a pattern conducive to healing and recovery. The following example illustrates encounters for injuries with active treatment and with routine care during the recovery or healing phase:
A teenaged girl presents to her pediatrician with wrist pain since falling from her bicycle 2 days ago. She notes that there is not much bruising and she can move her wrist but continues to have pain, especially at the base of her thumb. The pediatrician orders radiographs and finds no evidence of fracture but suspects a scaphoid fracture. A splint is applied and an appointment to return for a repeat radiograph is made for 2 weeks. Diagnosis is sprained right radiocarpal joint with possible scaphoid fracture.
The girl returns for repeat radiograph in 2 weeks. A non-displaced scaphoid fracture is now visualized. A cast is applied and the girl is scheduled for routine follow-up visits. Diagnosis is non-displaced right distal scaphoid fracture.
In this scenario, the same physician provides active treatment of the injury twice. The diagnosis at the end of the first encounter was sprained right radiocarpal joint, reported with code S63.521A. Seventh character A is appropriate for the active treatment of this injury. Although the second visit was with the same physician, there was active treat-ment of the right scaphoid fracture, so code S62.014A is reported. For both encounters, the cause of injury was a fall from a bicycle. Code V18.0XXA, pedal cycle driver injured in non-collision transport accident in non-traffic accident, is reported for each of the encounters for active treatment.
Note: Reporting of external cause-of-injury codes is recommended to provide accident information to the payer but is not a requirement of ICD-10-CM. State regulations may require reporting of external cause of injury in a facility setting.
Follow-up encounters during the healing phase of the scaphoid fracture will be reported with S62.014- appended with the appropriate seventh character to describe a subsequent encounter. Applicable seventh characters are
D, subsequent encounter for fracture with routine healingG, subsequent encounter for fracture with delayed healingK, subsequent encounter for fracture with nonunionp, subsequent encounter for fracture with malunion
Appendix B-4
Applying the 2015 ICD-10-CM Guidelines for Initial Encounters
(continued on page 232)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

232
Because an external cause code may be reported for the length of treatment, code V18.0XXD may also be reported, indicating a subsequent encounter. Applicable seventh characters for category V18 are
A, initial encounterD, subsequent encounterS, sequela
Were the patient in this example referred to an orthopedic physician for fracture care, the orthopedist would also report encounters for active treatment with seventh character A and all encounters during the healing phase with seventh character D.
Appendix B-4Transitioning to 10: Applying the 2015 ICD-10-CM Guidelines for Initial Encounters (continued from page 231)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

233
Physicians and coders may be familiar with the codes and guidelines for reporting sepsis using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Reporting sepsis with International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) is different but perhaps simpler.
The following is a review of the ICD-10-CM codes and guidelines for reporting septicemia, sepsis, and systemic inflammatory response syndrome (SIRS).
ICD-9-CM ReviewICD-9-CM requires a minimum of 2 codes to report sepsis. The first code identifies the septicemia or systemic infection (eg, 038.9) and the second identifies the SIRS due to an infectious process such as sepsis (995.91) or severe sepsis (995.92). Likewise, for newborn sepsis, ICD-9-CM requires 2 codes. Code 771.81, septicemia (sepsis) of the newborn, is reported first, followed by a code from category 041 identifying a bacterial infection in conditions classified elsewhere and of unspecified site. When applicable, severe sepsis (995.92) and any acute organ dysfunction should be reported as additional diagnoses. SIRS due to a noninfectious process such as trauma is reported with a code for the underlying cause (eg, trauma) followed by a code for SIRS due to noninfectious process without organ failure (995.93) or with organ failure (995.94).
Moving to ICD-10-CMFirst, you will find that in the alphabetic index, the term septicemia is indexed to code A41.9 with an additional entry instructing to see the term sepsis if septicemia is intended to mean sepsis or SIRS due to an infectious process. Code A41.9 is used to report sepsis due to an unspecified organism. This is generally equivalent to ICD-9-CM code 038.9, unspecified septicemia.
CODING TIp: Clinical evidence of sepsis is sufficient to support a diagnosis of sepsis. Negative or inconclusive blood cultures do not prohibit reporting this diagnosis when clinically indicated by a physician or other qualified health care professional. Coders are instructed to consult the physician when documentation is unclear.
In ICD-10-CM, 2 codes are not always required. For instance, code A41.1 is used to report coagulase-negative staphylococcus sepsis. No additional code for SIRS due to infection is necessary. However, additional codes may be reported to identify severe sepsis with septic shock (R65.20) or without septic shock (R65.21), any organ failure, or a coexisting localized infection such as pneumonia.
CODING TIp: Acute organ dysfunction must be linked to the sepsis in the documentation for coders to assign a code for severe sepsis. When applicable, additional codes are used to identify severe sepsis (R65.2-) and any associated acute organ dysfunction. A code from subcategory R65.2, severe sepsis, should not be assigned unless severe sepsis or a sepsis- associated acute organ dysfunction is documented.
Appendix B-5
Coding for Sepsis
(continued on page 234)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

234
When reporting newborn sepsis, codes in category p36 are assigned. Combination codes may allow for reporting of newborn sepsis due to a specified organism with a single code such as p36.4, newborn sepsis due to Escherichia coli. However, when reporting conditions such as newborn sepsis due to Haemophilus influenzae, 2 codes are required. Code p36.8, other bacterial sepsis of newborn, is reported first, followed by code B96.3, H influenzae as the cause of diseases classified elsewhere. Codes in categories B95–B97 are used to identify the infecting organism when the infectious organism is not included in the code descriptor. It is not necessary to report codes from categories B95–B97 when the infec-tious organism is included in a code descriptor for the infection (eg, p36.8).
CODING TIp: If a neonate is documented as having sepsis without documentation of congenital or community acquired, the default is congenital and a code from category p36 should be assigned.
post-procedural SepsisAs with all post-procedural complications, code assignment is based on the physician’s documentation of the relationship between the infection and procedure. Post-procedural sepsis is reported with specific codes, with most requiring a seventh character to identify the episode of care. For instance, when a newborn is diagnosed with sepsis due to a central line–associated bloodstream infection, code T80.211A, initial encounter for bloodstream infection due to central venous catheter, would be reported first, followed by codes for sepsis (eg, A41.9) and, when applicable, severe sepsis (R65.2-).
Systemic Inflammatory Response Syndrome Due to Noninfectious process When SIRS occurs due to a noninfectious process with no subsequent infection noted, report first the underlying condition, such as injury or trauma, followed by codes for the SIRS without acute organ dysfunction (R65.10) or with acute organ dysfunction (R65.11). When reporting code R65.11, report also a code for the specific organ dysfunction (eg, respiratory failure).
When a noninfectious process leads to an infection and sepsis or severe sepsis, the codes reported are based on the focus of the encounter. For instance, when an infection and sepsis develop following a burn injury and the infectious conditions are chiefly responsible for the services provided at the encounter, list first the code for the systemic infection followed by codes for any localized infection, any associated severe sepsis with acute organ dysfunction, and the related burn injury.
CODING TIp: Only one code from category R65, symptoms and signs specifically associated with systemic inflammation and infection, should be assigned. Assign only the appropriate code from subcategory R65.2, severe sepsis, when severe sepsis results from a noninfectious condition (ie, do not report a code from subcategory R65.1).
The Table includes some of the ICD-10-CM codes that may be commonly reported in relation to sepsis in the newborn or pediatric patient. This list is not all inclusive, and it is recommended that the ICD-10-CM alphabetic index and tabular list be consulted for the most appropriate codes and sequencing instructions.
Appendix B-5Transitioning to 10: Coding for Sepsis (continued from page 233)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

235
ICD-10-CM Codes for Sepsis-Related Conditions
Conditiona Code and Associated Conditions (Instructions in italics are based on coding guidelines and conventions.)
Sepsis (not otherwise specified)
A41.9 Sepsis, unspecified organism
Due to specified organism (other than neonate)
A02.1 Salmonella sepsisA32.7 Listerial sepsisA39.2 Acute meningococcemiaA39.3 Chronic meningococcemiaA40.0 Sepsis due to streptococcus, group AA40.1 Sepsis due to streptococcus, group BA40.3 Sepsis due to Streptococcus pneumoniaeA41.01 Sepsis due to methicillin-susceptible Staphylococcus aureusA41.02 Sepsis due to methicillin-resistant Staphylococcus aureusA41.1 Sepsis due to other specified staphylococcusA41.51 Sepsis due to Escherichia coli
Newborn sepsis p36.0 Sepsis of newborn due to streptococcus, group Bp36.10 Sepsis of newborn due to unspecified streptococcip36.19 Sepsis of newborn due to other streptococcip36.2 Sepsis of newborn due to Staphylococcus aureusp36.30 Sepsis of newborn due to unspecified staphylococcip36.39 Sepsis of newborn due to other staphylococcip36.4 Sepsis of newborn due to Escherichia colip36.5 Sepsis of newborn due to anaerobesp36.8 Other bacterial sepsis of newborn (Use additional code from category B96 to identify infection.)
Sepsis with related organ dysfunction (severe sepsis)
Code first underlying systemic infection followed by R65.20 and a code to specify acute organ dysfunction.
acute kidney failure (N17.-)acute respiratory failure (J96.0-)critical illness myopathy (G72.81)critical illness polyneuropathy (G62.81)disseminated intravascular coagulopathy (D65)encephalopathy (metabolic) (septic) (G93.41)hepatic failure (K72.0-)
Sepsis with septic shock (See code T81.12 for post- procedural septic shock.)
Code first underlying systemic infection followed by R65.21 and a code to specify acute organ dysfunction.
Post-procedural sepsis T81.4 Use additional code to identify infection and, if applicable, severe sepsis.
Sepsis following infusion, transfusion, and thera- peutic injection
T80.2- (7 characters required for complete code) Use an additional code to identify sepsis and, if applicable, severe sepsis.
Urosepsis No code; see the conditions documented such as sepsis with localized urinary tract infection.
Abbreviation: ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification.aNot an all-inclusive listing. Please see ICD-10-CM alphabetic index for complete listing.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

236
JAMA: The Journal of the American Medical Association recently published research on the prevalence of diabetes mellitus types 1 and 2 among children and adolescents show-ing a 21% increase in type 1 and 30.5% increase in type 2 diabetes between 2001 and 2009.1 This increase in the number of children presenting with diabetes indicates that pediatricians are more frequently diagnosing and caring for children with diabetes. This is good reason to review the future of diagnosis coding for these conditions: International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM).
Most physicians are familiar with International Classification of Diseases, Ninth Revision, Clinical Modification codes in the 250 category that include diabetes mellitus types 1 and 2. The fourth and fifth digits of these codes identify manifestations, type of diabetes, and control status. ICD-10-CM addresses diabetes by type, identifying each type with a sepa-rate code category. For example, type 1 diabetes is reported with a code from category E10, while type 2 diabetes is reported with a code from category E11. Each category includes combination codes that identify the type of diabetes and a body system affected by manifestation of the disease. Additional codes may be required to further describe some manifestations.
Control status is only included in ICD-10-CM classification of diabetes when the condi-tion is documented with terms indicating poor control or lack of control. ICD-10-CM guidelines for reporting diabetes state that diabetes noted as poorly controlled or uncon-trolled are to be reported with the code for the type of diabetes with hyperglycemia (eg, E10.65, type 1 diabetes with hyperglycemia). This guideline applies to all types of diabetes. Hypo-glycemia in diabetes is reported with a combination code that identifies the type of diabetic hypoglycemia with or without coma (eg, E10.649, type 1 diabetes with hypoglyce-mia without coma).
ExamplesA teenager with type 1 diabetes diagnosed 6 years ago presents for regularly scheduled follow-up care. At an encounter 3 months prior, urine examination was positive for microalbuminuria. Repeat testing is again positive for microalbuminuria. The current hemoglobin A1c result is 8.5. The diagnoses are uncontrolled type 1 diabetes with nephro- pathy and microalbuminuria. ICD-10-CM codes reported are
E10.65 Type 1 diabetes mellitus with hyperglycemiaE10.21 Type 1 diabetes mellitus with diabetic nephropathy R80.9 Proteinuria, unspecified (includes microalbuminuria)
A teenaged girl with diabetes is seen in the physician office to follow up a recent emergency department visit for hypoglycemia. The girl states she has been busy with school activities and sports that distract from her normal routine, making it more difficult to manage her diabetes. She states she doesn’t feel the warning signs of hypoglycemia as she had
Appendix B-6
Documenting Diabetes Mellitus
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

237
There is currently no code specifying hypoglycemic unawareness. If the cause of the hypoglycemic unawareness is noted as diabetic autonomic neuropathy, code E10.43 (type 1 diabetes mellitus with diabetic autonomic [poly]neuropathy) may be reported in addition to code E10.649.
Coding Tip
Insulin use is assumed in type 1 diabetes, making it unnecessary to report an additional code. When the patient with another type of diabetes uses insulin (long term), code Z79.4 should be reported to indicate the long-term current use of insulin. Temporary administration of insulin during an encounter should not be separately reported. Prediabetes or other abnormal glucose without diagnosis of diabetes is reported with code R73.09. Dietary counseling and surveillance may be reported with code Z71.3.
Categories E08, E09, and E13 are used to report secondary diabetes. The ICD-10-CM tab-ular list provides instruction on sequencing of codes for these conditions. When diabetes is due to an underlying condition, the code for the underlying condition is reported first (eg, cystic fibrosis). Identified poisoning or adverse effect by drug or toxin should be reported in conjunction with the codes for drug- or chemical-induced diabetes (category E09). Sequencing of codes for drug- or chemical-induced diabetes is dependent on whether the patient experienced poisoning or an adverse effect of a properly administered substance. Category E13 includes postoperative diabetes and diabetes due to genetic defects of beta cell function or insulin action.
For patients who are pregnant and have preexisting or gestational diabetes, Chapter 15 of the ICD-10-CM tabular list (O codes) includes pregnancy codes specific to type of diabe-tes. Furthermore, like many ICD-10-CM pregnancy codes, conditions are also specified by trimester. For example, the code series O24.01X addresses preexisting type 1 diabetes specific to trimesters 1, 2, or 3, and the code series O24.11X addresses preexisting type 2 diabetes also specific to trimester. To these, one may add additional secondary codes to specify any additional diabetic manifestations (eg, codes from category E10 or E11). The O24.41X code series addresses gestational diabetes in pregnancy, but rather than being specific to trimester, gestational diabetes is referenced by diet or insulin control. Additional codes in category O24 are assigned for gestational diabetes in childbirth or the puerperium. ICD-10-CM also includes codes for reporting the syndrome of an infant of a mother with gestational (p70.0) or preexisting (p70.1) diabetes.
When documenting diabetes, key elements for code selection are type and manifestations. If the type of diabetes is not documented, a code for type 2 is reported. Type 1 and other types of diabetes should be documented accordingly. Codes for each manifestation of diabetes should be reported. Coders may not assume a relationship between diabetes and other documented conditions. For this reason, it is important that manifestations are clearly indicated in the record (eg, diabetic skin ulcer or neuropathy due to diabetes).
previously. The diagnosis is type 1 diabetes with hypoglycemia and hypoglycemic unawareness. The ICD-10-CM code reported is
E10.649 Type 1 diabetes mellitus with hypoglycemia without coma
(continued on page 238)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

238
Documentation Elements and ICD-10-CM Codes for Diabetes
Type of Diabetes and Affected System Manifestation Code
AssociatedConditions
Neonatal (transient) p70.2Prediabetes (abnormal glucose)
R73.09
Type 1 Without complication E10.9Type 1 with other specified compli-cations
With hyperglycemia (uncontrolled)
E10.65
Type 1 with skin complications
With diabetic dermatitis E10.620With foot ulcer E10.621 Identify site of ulcer.
L97.4-, L97.5-With other skin ulcer E10.622 Identify type and
site of ulcer.L97.1–L97.9, L98.41–L98.49
With other skin complications E10.628Type 1 with ketoacidosis
Without coma E10.10
With coma E10.11
Type 1 with ophthalmic complications
Unspecified diabetic retinopathy with macular edema
E10.311
Unspecified diabetic retinopathy without macular edema
E10.329
Mild nonproliferative diabetic retinopathy with macular edema
E10.321
Mild nonproliferative diabetic retinopathy without macular edema
E10.329
Type 1 diabetes mellitus with diabetic cataract
E10.36
With other diabetic ophthalmic complication
E10.39 Diabetic glaucoma (H40–H42) or other manifestation
Abbreviation: ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification.
Documentation elements that support ICD-10-CM coding of diabetes mellitus types 1 and 2 are illustrated in the Table. Not all codes for diabetes are included in the Table; please reference the ICD-10-CM code set for complete coding options and instructions.
Reference1. Dabelea D, Mayer-Davis EJ, Saydah S, et al. Prevalence of type 1 and type 2 diabetes among
children and adolescents from 2001 to 2009. JAMA. 2014;311(17):1778–1786
Appendix B-6Transitioning to 10: Documenting Diabetes Mellitus (continued from page 237)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

239
Documentation Elements and ICD-10-CM Codes for Diabetes (cont)
Type of Diabetes and Affected System Manifestation Code
AssociatedConditions
Type 2 Without complication E11.9 Identify any insulin use.Z79.4
Type 2 with other specified complications
With hyperglycemia (uncontrolled)
E11.65
With hypoglycemia with coma
E11.641
With hypoglycemia without coma
E11.649
Type 2 with hyperosmolarity
Without nonketotic hyperglycemic-hyperosmolar coma
E11.00 Identify any insulin use.Z79.4
With hyperosmolarity with coma
E11.01
Type 2 with kidney complications
With diabetic nephropathy E11.21 Identify any insulin use. Z79.4
With diabetic chronic kidney disease
E11.22 Identify stage of chronic kidney disease.N18.1–N18.6
With other diabetic kidney complication
E11.29
Abbreviation: ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

240
As 2014 draws to a close, we once again enter the year designated for implementation of International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). Barring another unexpected delay, it is likely that October 1, 2015, will be the imple- mentation date for ICD-10-CM.
In anticipation of this eventual implementation, “Transitioning to 10” articles have pro-vided information on transition preparation, ICD-10-CM codes common to pediatrics, and documentation tips to support reporting of specific diagnoses. This month, we will focus on anemia, but you may revisit previous “Transitioning to 10” articles anytime by visiting the online edition of the newsletter (http://coding.aap.org) and browsing our “Collections” page.
GuidelinesCurrently, no information is found for Chapter 3, Disease of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50–D89), in the guidelines for use of ICD-10-CM. However, anemia related to malignant neoplasms is addressed in the guidelines for Chapter 2. The related guidelines are
■■ When the admission/encounter is for management of an anemia associated with malignancy and the treatment is only for anemia, the appropriate code for the malignancy is sequenced as the principal or first-listed diagnosis, followed by the appropriate code for the anemia (eg, code D63.0, anemia in neoplastic disease).
■■ When the admission/encounter is for management of an anemia associated with an adverse effect of the administration of chemotherapy or immunotherapy and the only treatment is for the anemia, the anemia code is sequenced first, followed by the appropriate codes for the neoplasm and adverse effect (T45.1X5, adverse effect of anti-neoplastic and immunosuppressive drugs).
■■ When the admission/encounter is for management of an anemia associated with an adverse effect of radiotherapy, the anemia code should be sequenced first, followed by the appropriate neoplasm code and code Y84.2, radiological procedure and radiotherapy as the cause of abnormal reaction of the patient, or of later compli- cation, without mention of misadventure at the time of the procedure.
Common pediatric Anemias The Table includes codes for several types of pediatric anemia. Please note that this list is not comprehensive and the alphabetic index of ICD-10-CM should be consulted for terms not included in the table. As with most conditions presenting in the neonatal period, newborn anemia is reported with codes from Chapter 16 of the ICD-10-CM tabular list (codes beginning with p).
Appendix B-7
Pediatric Anemia
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

241
Documentation elements are fairly straightforward with most common terms included in the index, including various syndromes such as Blackfan-Diamond. When the under-lying cause of anemia is identified (eg, acute blood loss), documentation will support more specific coding. When documented, any associated fever (R50.81) is additionally reportable with sickle cell disorders. Codes indicating crisis are reported for dactylitis or vasoocclusive pain. Codes can further specify crisis with acute chest syndrome or splenic sequestration when indicated. Anemia without further specification is reported as anemia, unspecified (D64.9).
Coders should be careful to avoid coding for anemia when only deficiency or trait is documented. Iron deficiency without diagnosis of anemia is reported as a nutritional deficiency with code E61.1. Sickle cell trait is reported with code D57.3.
Screening for AnemiaIron deficiency is a concern in infants and young children due to potential effects on neurodevelopment. For this reason, screening is recommended in the presence of certain risk factors and at age 12 months. To report screening for iron deficiency anemia, use ICD-10-CM code Z13.0, encounter for screening for diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism. Code Z13.0 is also appropriate for reporting screening for sickle cell trait.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

242
Codes and reporting guidelines for epilepsy using International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) include familiar terminology carried over from International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
This article will review the similarities, differences, and documentation elements necessary for reporting epilepsy with ICD-10-CM.
As with ICD-9-CM, ICD-10-CM codes for epilepsy include specification of the type of epilepsy and status of the condition (eg, whether or not the condition is intractable). Intractable is assigned when documentation includes such terms as treatment resistant, poorly controlled, pharmacoresistant, or refractory. In addition, ICD-10-CM codes specify epilepsy with or without status epilepticus.
ExampleRefractory childhood absence epilepsy with status epilepticus is reported as follows using ICD-9-CM and ICD-10-CM:
ICD-9-CM345.01 Generalized nonconvulsive epilepsy, with intractable epilepsy
ICD-10-CMG40.A11 Absence epileptic syndrome, intractable, with status epilepticus
Note that ICD-9-CM code 345.01 does not specify status epilepticus. The differences in reporting epilepsy with or without status epilepticus may make it easier to code directly from the ICD-10-CM code set than crosswalking from ICD-9-CM. For instance, ICD-9-CM code 345.2 is used to report petit mal seizure. The ICD-10-CM index reference for petit mal seizure refers to other generalized epilepsy and epileptic syndromes, category G40.4. Four code options are included in category G40.4.
G40.401 Other generalized epilepsy and epileptic syndromes, not intractable, with status epilepticus
G40.409 Other generalized epilepsy and epileptic syndromes, not intractable, without status epilepticus
G40.411 Other generalized epilepsy and epileptic syndromes, intractable, with status epilepticus
G40.419 Other generalized epilepsy and epileptic syndromes, intractable, without status epilepticus
Appendix B-8
Epilepsy
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

243
Like petit mal seizures, ICD-10-CM does not include a specific code for grand mal seizure but directs again to category G40.4.
Categories of EpilepsyCategory G40 includes codes for epilepsy and recurrent seizures. Categories are further divided into subcategories for specific localization-related, generalized, and other specified forms of epilepsy. The subcategories are
G40.0 Localization-related (focal) (partial) idiopathic epilepsy and epileptic syndromes with seizures of localized onset (includes benign childhood epilepsy with centrotemporal EEG spikes)
G40.1 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with simple partial seizures (includes epilepsia partialis continua)
G40.2 Localization-related (focal) (partial) symptomatic epilepsy and epileptic syndromes with complex partial seizures
G40.3 Generalized idiopathic epilepsy and epileptic syndromes
G40.A Absence epileptic syndrome
G40.B Juvenile myoclonic epilepsy (impulsive petit mal)
G40.5 Epileptic seizures related to external causes
G40.8 Other epilepsy and recurrent seizures (includes Lennox-Gastaut and Landau-Kleffner syndromes)
G40.9 Epilepsy, unspecified
As previously noted, codes in each subcategory specify the epilepsy status as intractable or not intractable and with or without status epilepticus.
Convulsions and SeizuresConvulsions are classified as symptoms in ICD-10-CM except when further described as illustrated in the excerpt from the alphabetic index that follows. Note that febrile convulsions with status epilepticus are reported as unspecified epilepsy, not intractable, with status epilepticus (G40.901).
Convulsions (see also Seizure[s]) R56.9…- febrile R56.00- - with status epilepticus G40.901 - - complex R56.01- - - with status epilepticus G40.901- - simple R56.00 - hysterical F44.5- infantile p90- - epilepsy – see Epilepsy
(continued on page 244)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

244
Seizure disorder is reported as epilepsy per the alphabetic index instruction. However, a single seizure or seizure with identified cause such as fever or trauma is not reported asepilepsy unless status epilepticus is documented. As with convulsions, the alphabetic index provides direction to the correct codes for these seizures.
Seizure(s) (see also Convulsions) R56.9…- febrile (simple) R56.00- - with status epilepticus G40.901- - complex (atypical) (complicated) R56.01- - - with status epilepticus G40.901- post-traumatic R56.1
For seizure due to migraine headache, code first migraine with aura followed by the appropriate code for epilepsy (G40.-) or seizure (R56.9).
Documentation ElementsTo support correct ICD-10-CM coding of epilepsy and related syndromes, it is necessary to specify the type of epilepsy, wheth- er or not the condition is intractable (eg, fails to be controlled on antiepileptic medications), and, when indicated, status epilepticus. When documenting convulsions or seizures, the type (eg, febrile), severity (simple or complex), and, when indicated, status epilepticus will support the most specific code and best identify the complexity of the condition requiring diagnosis and management or treatment.
Appendix B-8Transitioning to 10: Epilepsy (continued from page 243)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

245
As preparations continue for the October 1, 2014, transition to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), some physicians and prac-tices may have concerns about how well current documentation practices will support code assignment in ICD-10-CM.
One option for implementing a documentation review and improvement project in rela-tion to ICD-10-CM is to start with a list of the physician’s or practice’s most frequently reported International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. To focus on documentation to support specific codes, it is necessary to determine the elements that support code selection for a specific condition. For instance, ICD-9-CM code 382.9 ranked third in the top 25 diagnosis codes reported by pediatricians for encounters with children up to age 18 years for the years 2008–2010. This code represents unspecified otitis media and could be more specifically reported in ICD-9-CM if documentation provides the necessary information. (See “Top 25 Pediatric Diagnoses Revisited” in the August 2013 issue of AAP Pediatric Coding Newsletter™ to learn how this code indicates a lack of specificity in documentation.) Once you have selected a condition to review, look carefully at the ICD-10-CM codes for that condition and create a list or table of the documentation elements that support code selection. The Table shows in 4 columns the documentation elements necessary to specifically identify otitis media using ICD-10-CM. A documentation element from each of the 4 columns is necessary to support specific code selection.
To take this a step further, note whether there is documentation of tobacco use or exposure, as this is reported in addition to otitis media when documented.
Alternatively, you can start dual coding for certain conditions now. This is a bit time con-suming because it involves assignment of ICD-9-CM and ICD-10-CM codes to current services (officially reporting only ICD-9-CM codes). However, this brings real-world ICD-10-CM coding experience to your practice prior to the date when these codes will actually be billed. This may help offset the expected October work delays related to the transition while clearly illustrating where documentation lacks information to assign specific codes. Documentation references such as the Table may be built and used as improvement tools as you find necessary during the project.
Whichever method you choose, these are exercises that offer opportunity now to not only prepare for ICD-10-CM but also to report the codes that most specifically describe the conditions managed and support the necessity of services provided. Who knows? You may be pleasantly surprised that documentation for ICD-10-CM is not so different from ICD-9-CM.
Appendix B-9
Documentation and Coding of Otitis Media
(continued on page 246)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

246
Documentation Elements of Otitis Media
Laterality Incidence
Type (Suppurative and nonsuppurative are less specific than other terms.)
TympanicMembraneStatus
RightLeftBilateral
Acute/subacuteAcute recurrentChronicIn disease classified elsewherea (eg, influenza)
SerousAllergic (includes otitis media stated as allergic and mucoid, sanguineous, or serous)MucoidGlue earExudativeSecretorySanguineousSeromucinousTransudativeNonsuppurative/with effusion/catarrhal Suppurative/purulentAtticoantralTubotympanicBenign chronic suppurative
With associated perforationWithout associated perforation
aType is not designated in codes for otitis media in disease classified elsewhere.
Appendix B-9Transitioning to 10: Documentation and Coding of Otitis Media (continued from page 245)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

247
The following Table provides a sample of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes for congenital cardiac and cardiovascular malformations and personal history of corrected malformations of the heart and circulatory system.
Diagnosis Codes for Congenital Malformations of the Heart and Circulatory System
ICD-9-CM ICD-10-CM
V13.65 Personal history of (corrected) congenital malformations of heart and circulatory system
Z87.74 Personal history of (corrected) congenital malformations of heart and circulatory system
745.4 Ventricular septal defect Q21.0 Ventricular septal defect
745.5 Ostium secundum type atrial septal defect
Q21.1 Atrial septal defect (includes patent foramen ovale)
745.2 Tetralogy of Fallot Q21.3 Tetralogy of Fallot
747.10 Coarctation of aorta (preductal) (postductal)
747.11 Interruption of aortic arch
747.22 Atresia and stenosis of aorta
Q25.1 Coarctation of aorta
Q25.2 Atresia of aorta
Q25.3 Supravalvular aortic stenosis
746.7 Hypoplastic left heart syndrome
Q23.4 Hypoplastic left heart syndrome
745.10 Complete transposition of great vessels
745.11 Double outlet right ventricle
745.12 Corrected transposition of great vessels
Q20.3 Discordant ventriculoarterial connection
Q20.1 Double outlet right ventricle
Q20.5 Discordant atrioventricular connection
745.0 Common truncus Q20.0 Common arterial trunk (Persistent truncus arteriosus)
747.41 Total anomalous pulmonary venous connection
Q26.2 Total anomalous pulmonary venous connection
Appendix B-10
Congenital Malformations of the Circulatory System
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

248
During the winter months, patients may present with symptoms ranging from the common cold to influenza. International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) offers a full range of codes for these conditions.
Starting with the common cold, J00, acute upper respiratory infections are reported with codes in categories J00–J06. However, an acute upper respiratory infection as a manifestation of influenza is typically reported with codes for influenza. For instance, when a patient with upper respiratory symptoms is diagnosed by her physician with influenza type B, it would be unnecessary to report a code for the upper respiratory symptoms. ICD-10-CM provides combination code J10.1 for reporting influenza due to other identified influenza virus with other respiratory manifestations. The identified type B influenza is an “other identified” influenza to differentiate from a novel influenza A virus that would be reported as “certain identified” influenza viruses with codes in category J09. Code J10.1 includes manifestations such as pharyngitis, laryngitis, and other upper respiratory symptoms. However, acute sinusitis associated with influenza would be separately reported with a code from category J01. Other codes for influenza include manifestations such as pneumonia, gastrointestinal symptoms, and otitis media.
Hopefully, upper respiratory symptoms will not often be associated with influenza because patients will have been previously assigned code Z23, encounter for immunization, on receipt of an influenza vaccination. When not associated with influenza, conditions represented by codes in categories J00–J06 include acute forms of sinusitis, pharyngitis, tonsillitis, laryngitis, and tracheitis.
Acute sinusitis is reported with codes in category J01 and an additional code from categories B95–B97 to identify the infectious agent when identified. Categories B95–B97 include codes specifying certain bacterial and viral infectious agents as the cause of condi-tions classified elsewhere (eg, B95.3, Streptococcus pneumoniae as the cause of diseases classified elsewhere). Codes in category J01 are not reported for chronic sinusitis (J32.0–J32.8), though acute and chronic sinusitis may be reported when applicable. Codes for acute sinusitis specify the type of sinusitis (eg, maxillary) and when applicable, recurrence of the condition. If sinusitis is not documented as acute or chronic, code J32.9 is used to report unspecified sinusitis.
Acute pharyngitis without an identified causal organism is reported with code J02.9. Streptococcal pharyngitis has a combination code, J02.0, that includes the causal organ-ism. Acute pharyngitis due to other specified organisms will require reporting of 2 codes. Code J02.8 specifies the pharyngitis due to other specified organisms, and a code from categories B95–B97 should be additionally reported to indicate the infectious agent.
Codes for acute tonsillitis may be reported with codes in category J03 when tonsillitis is due to streptococcal infection. Streptococcal tonsillitis is reported as acute or acute recurrent (J03.00–J03.01). Acute or recurrent acute tonsillitis codes J03.80–J03.81 are reported when the condition is due to other specified organisms classified in categories
Appendix B-11
Sniffling, Coughing, Aching All Over
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

249
B95–B97. Be aware of the “excludes1” note directing that several types of tonsillitis are classified according to the type of infectious agent involved (eg, herpesviral pharyngo- tonsillitis, B00.2). In ICD-10-CM, an “excludes1” note prohibits reporting of certain codes with the code above the note. An “excludes2” note indicates codes for conditions not reported with the code above the note but additionally reportable when the conditionspresent at the same encounter. When the infectious agent is not specified, acute tonsillitis is reported with code J03.9, which includes follicular, ulcerative, and gangrenous tonsillitis. Hypertrophy and chronic infection of the tonsils and adenoid are reported with codes in category J35.
Acute laryngitis (J04.0) does not include croup or acute obstructive laryngitis (J05.0). Acute tracheitis is reported with obstruction (J04.11) or without obstruction (J04.10). Acute laryngotracheitis is reported with code J04.2 except when with obstruction (J05.0). Codes for supraglottitis (J04.30–J04.31) and epiglottitis (J05.10–J05.22) also specify with or without obstruction.
Category J06 provides codes for acute respiratory infection of multiple and unspecified sites, with code J06.0 for acute laryngopharyngitis and code J06.9 for acute upper respiratory infection, unspecified.
There is one instruction that applies to all diseases in the respiratory system. Use an addi-tional code, where applicable, to identify
• Exposure to environmental tobacco smoke (Z77.22)• Exposure to tobacco smoke in the perinatal period (p96.81)• History of tobacco use (Z87.891)• Occupational exposure to environmental tobacco smoke (Z57.31)• Tobacco dependence (F17.-)• Tobacco use (Z72.0)
Wouldn’t it be great if by October 1, 2014, codes Z77.22 and p96.81 were obsolete? Here’s hoping that these codes seldom apply and that the extra time allotted for transition to ICD-10-CM allows you to breathe a little easier as well.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

250
Appendix B-12
Allergies
This article continues the “Transitioning to 10” series providing pediatric-specific information on the transition to and use of International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). The focus this month is allergies. This article provides a mapping of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) to ICD-10-CM codes for allergy-related conditions. For information on reporting allergic dermatitis, please see “Transitioning to 10: Documenting Dermatitis” in the “Transitioning to 10” collection of AAP Pediatric Coding Newsletter™ (http://coding.solutions.aap.org/transitioning.aspx).
Allergic RhinitisCodes for allergic rhinitis are found in category J30 in ICD-10-CM. Table 1 provides a crosswalk from ICD-9-CM to ICD-10-CM codes for allergic rhinitis.
Table 1. Diagnosis Codes for Allergic Rhinitis
Allergic Rhinitis ICD-9-CM ICD-10-CM
Due to animal hair and dander (cat) (dog)
477.2 J30.81
Due to food 477.1 J30.5
Due to pollen 477.0 J30.1
Perennial 477.9 J30.89
Seasonal 477.9 J30.2
Vasomotor 477.9 J30.0
Allergic ReactionA diagnosis of allergic reaction without further specification is reported with code 995.3 in ICD-9-CM. Code T78.40 is used to report an unspecified allergic reaction using ICD-10-CM. Personal history of anaphylaxis is reported with code V13.81 in ICD-9-CM and Z87.892 in ICD-10-CM. When reporting personal history of anaphylaxis, also report the allergy status. For diagnostic skin and sensitization tests, report ICD-9-CM code V72.7 or, after transition to ICD-10-CM, Z01.82.
Insect AllergiesAllergy to insects and arachnids is reported with ICD-9-CM code V15.06. ICD-10-CM includes separate codes for bee allergy status (Z91.030) and other insect allergy status (Z91.038). For anaphylactic shock due to insect sting, ICD-9-CM code 989.5 is reported. After transition to ICD-10-CM, for anaphylactic shock due to venomous sting, including that with allergic or anaphylactic shock, see the table of drugs and chemicals, by animal or substance, poisoning.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

251
Food AllergiesTable 2 provides a crosswalk from ICD-9-CM to ICD-10-CM codes for personal history or allergy status without reaction and for anaphylaxis due to food or food additives. All T78 codes require a seventh character to define the encounter.
Table 2. Diagnosis Codes for Allergic Reaction to Food
Diagnosis ICD-9-CM ICD-10-CM
Anaphylactic reaction due to unspecified food 995.60 T78.00-
Allergy to foods other than peanuts, seafood, milk products, eggs (status)
V15.05 Z91.018
Anaphylactic reaction due to peanuts 995.61 T78.01-
Allergy to peanuts (status) V15.01 Z91.010
Anaphylactic reaction due to shellfish (crustaceans) 995.62 T78.02-
Anaphylactic reaction due to other fish 995.65 T78.03-
Allergy to seafood (status) V15.04 Z91.013
Anaphylactic reaction due to fruits and vegetables 995.63 T78.04-
Anaphylactic reaction due to tree nuts and seeds (other than peanuts)
995.64 T78.05-
Anaphylactic reaction due to milk and dairy products 995.67 T78.07-
Allergy to milk products (not reported for lactose intolerance, E73.-)
V15.02 Z91.011
Anaphylactic reaction due to eggs 995.68 T78.08-
Allergy to eggs (status) V15.03 Z91.012
Anaphylactic reaction due to other food products 995.69 T78.09-
Anaphylactic reaction due to food additives 995.66 T78.06-
Allergy food additives (status) V15.05 Z91.02
(continued on page 252)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

252
Appendix B-12Transitioning to 10: Allergies (continued from page 251)
Drug and Medicinal AllergyTable 3 includes codes for allergic reactions to drugs and medicinal substances, including vaccines. When vaccination is not carried out because of allergy to a vaccine or a vaccine component, ICD-9-CM code V64.04 is reported. Following transition to ICD-10-CM, immunization not carried out because of patient allergy to a vaccine or component is reported with code Z28.04. Codes T88.6- and T80.52- require a seventh character to define the encounter.
Table 3. Diagnosis Codes for Reaction to Drugs or Medicinal Substances
Diagnosis ICD-9-CM ICD-10-CM
Anaphylactic reaction to drug or medicinal substance (correctly administered) (Use additional code to specify adverse effect of specified drug or medicinal substance)
995.0 T88.6-
Allergy to drug or medicinal substance (status) (see code set for complete codes)
V87.4- Z88.-
Anaphylactic reaction due to vaccination 999.42 T80.52-
Allergy to serum and vaccine (status) 999.59 Z88.7
Radiographic dye allergy (status) V15.08 Z91.041
Latex allergy status V15.07 Z91.040
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

253
This article is a continuation of a series started in 2011 to help prepare AAP Pediatric Coding Newsletter™ subscribers for the transition to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) on October 1, 2014. This series has in- cluded articles introducing ICD-10-CM code structure, conventions, and guidelines and codes for specific conditions frequently managed by pediatricians. You can find past articles of this column at http://coding.aap.org by clicking on “Browse All Transitioning to 10” in the “Newsletter Features” box near the bottom of the page. With 6 months left to prepare for the transition, we hope that physicians and coders are beginning to have a familiarity with this code set. Many physicians and practices are now assessing their documentation to determine if current documentation is sufficient to support accurate ICD-10-CM code assignment. A first step in this process is to identify the elements of documentation necessary to support code assignment for a selected condition. For this article, we will focus on the documentation elements necessary to support assignment of codes for asthma.
ICD-10-CM classifies asthma according to severity classification as described by the National Heart, Lung, and Blood Institute: intermittent, mild persistent, moderate per-sistent, and severe persistent (www.nhlbi.nih.gov/guidelines/asthma/04_sec3_comp.pdf). For each level of severity, codes may also indicate acute exacerbation or status asthmaticus.
ICD-10-CM guidelines instruct that an acute exacerbation of asthma is a worsening or decompensation of the chronic condition. An acute exacerbation is not equivalent to an infection superimposed on asthma, but an infection could trigger an acute exacerbation, making it necessary to report a code for asthma with acute exacerbation and a code for the related infection.
Tip
The Table on page 5 shows the elements of documentation that will support selection of specific ICD-10-CM codes to report asthma. If documentation does not indicate the severity and status of asthma, code J45.909 must be reported indicating uncomplicated, unspecified asthma. Documentation of reactive airway disease without further specifica-tion would also result in assignment of code J45.909 because ICD-10-CM cross-references this term to asthma. Note that the Table is not used for exercise-induced asthma (J45.990) or cough variant asthma (J45.991).
Coders assign codes for asthma with status asthmaticus only if this condition is specifically documented by the physician.
Tip
Appendix B-13
Documentation of Asthma
(continued on page 254)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

254
The tabular list instructs that physicians should report any use of or exposure to tobacco when reporting asthma. The third column of the Table includes the types of tobacco exposure or use that may be reported.
Once you have the documentation elements of severity and status, code selection is fairly straightforward despite the number of codes. Each code is found in category J45. The fourth characters 2 through 5 in codes J45.20–J45.52 represent the asthma severity classification, while fifth characters 0 through 2 identify the condition status as uncomplicated, with acute exacerbation, or with status asthmaticus. Codes in subcategory J45.9 include 6 characters to identify unspecified or other asthma. The codes in category J45 are as follows:
Appendix B-13Transitioning to 10: Documentation of Asthma (continued from page 253)
J45.20 Mild intermittent asthma, uncomplicated
J45.21 Mild intermittent asthma with (acute) exacerbation
J45.22 Mild intermittent asthma with status asthmaticus
J45.30 Mild persistent asthma, uncomplicated
J45.31 Mild persistent asthma with (acute) exacerbation
J45.32 Mild persistent asthma with status asthmaticus
J45.40 Moderate persistent asthma, uncomplicated
J45.41 Moderate persistent asthma with (acute) exacerbation
J45.42 Moderate persistent asthma with status asthmaticus
J45.50 Severe persistent asthma, uncomplicated
J45.51 Severe persistent asthma with (acute) exacerbation
J45.52 Severe persistent asthma with status asthmaticus
J45.901 Unspecified asthma with (acute) exacerbation
J45.902 Unspecified asthma with status asthmaticus
J45.909 Unspecified asthma, uncomplicatedJ45.990 Exercise-induced bronchospasmJ45.991 Cough variant asthmaJ45.998 Other asthma
Asthma Documentation Elements
Severity Status Tobacco Use/Exposure
IntermittentMild persistentModerate persistentSevere persistent
Uncomplicated or not otherwise specifiedWith acute exacerbationWith status asthmaticus
Exposure to environmental tobacco smoke (Z77.22)Exposure to tobacco smoke in the perinatal period (p96.81)History of tobacco use (Z87.891)Occupational exposure to environmental tobacco smoke (Z57.31)Tobacco use (Z72.0)Nicotine dependence, cigarettes (F17.21-; sixth character required to indicate uncomplicated [0], in remission [1], with withdrawal [3], with other nicotine-induced disorder [8], or with unspecified nicotine-induced disorder [9])
Development of an asthma visit documentation template capturing asthma severity classification and status at the time of an encounter may help support more complete documentation and specific coding. More specific code assignment may also better support medical necessity of the services provided and contribute to data used to influence public and private payer health initiatives.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

255
In our continuing series aimed at assisting readers with the transition to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), this article will discuss documentation elements that support ICD-10-CM code selection for sinusitis.
As with many conditions, sinusitis was frequently reported with nonspecific codes when reported with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Code 473.9, unspecified chronic sinusitis, ranked eighth in the American Academy of Pediatrics analysis of the National Ambulatory Medical Care Survey for the years 2008 through 2010.
ICD-10-CM codes for sinusitis are not significantly different from ICD-9-CM in that each code set provides for specificity for the condition in acute (J01.-) or chronic (J32.-) occur-rence and the involved sinus (eg, maxillary). One change in ICD-10-CM is the ability to capture recurrence of acute sinusitis. This presents an opportunity to better characterize the nature of the patient presentation and the medical necessity of services provided or referrals for additional workup.
Certain combination codes identify the condition and under-lying infection. Sinusitis occurring in influenza should be reported using the combination code for the type of influenza with respiratory manifestations (eg, J11.1, influenza due to unidentified influ-enza virus with other respiratory manifestations). For sinusitis in tuberculosis, see code A15.8, other respiratory tuberculosis. When reporting sinusitis due to other identified infectious agents, codes from categories B95–B97 are reported in addition to codes for sinusitis if known during the encounter.
No additional code is indicated to specify purulent and non-purulent sinusitis or sinus perforation because these conditions are referenced to the codes for acute or chronic sinusitis. Note, though, that a diagnosis of allergic sinusitis is reported with a code for allergic rhinitis (J30.-).
When acute and chronic sinusitis are diagnosed at the same encounter, codes for each condition are reported. The “excludes2” notes at categories J01 and J32 indicate each category excludes codes for conditions represented by the other but when present, each condition is separately reported.
Coding Tip
Table 1 provides the documentation elements necessary to support specific code selection for acute or chronic sinusitis. Note that occurrence and type are the key elements of docu-mentation necessary for specific code assignment. A diagnosis of sinusitis without indica- tion of occurrence will default to codes for chronic sinusitis. The type of sinusitis refers to inflamed sinus except in cases of allergic sinusitis or sinusitis in influenza or tuberculosis.
Appendix B-14
Documentation of Sinusitis
(continued on page 256)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

256
Table 1. ICD-10-CM Documentation Elements for Sinusitis
Occurrence Type Related Diagnoses (Code also)
Acute Acute recurrentChronic
Allergic (See rhinitis, allergic, J30.-.)EthmoidFrontalMaxillary (includes perforated antrum)Multiple sinuses, other than pansinusitisPansinusitisSphenoidTuberculous (A15.8)With influenza (See J09–J11, influenza by type with respiratory manifestation.)
Infectious agent (When known; see B95–B97.)Exposure to environmental tobacco smoke (Z77.22)Exposure to tobacco smoke in the perinatal period (p96.81)History of tobacco use (Z87.891)Occupational exposure to environmental tobacco smoke (Z57.31)Tobacco dependence (F17.-)Tobacco use (Z72.0)
Table 2. ICD-10-CM Codes for Acute and Chronic Sinusitis by Location
Location Acute Acute Recurrent Chronic
Ethmoid J01.20 J01.21 J32.2
Frontal J01.10 J01.11 J32.1
Involving more than one sinus, other than pansinusitis
J01.80 J01.81 J32.8
Maxillary J01.00 J01.01 J32.0
Pansinusitis J01.40 J01.41 J32.4
Sphenoid J01.30 J01.31 J32.3
Codes for acute and chronic sinusitis (not including codes for an identified infectious agent) are shown in Table 2.
Appendix B-14Transitioning to 10: Documentation of Sinusitis (continued from page 255)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

257
This article continues our focus on diagnoses commonly reported in pediatrics and the elements of documentation that support code selection using International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). Although the transition to use of the ICD-10-CM code set has been delayed beyond the previously published date of October 1, 2014, to no earlier than October 1, 2015, it is important to take advantage of the extended opportunity to prepare for this pending transition.
This article focuses on the classification of abdominal and pelvic pain. These symptoms have often been reported with nonspecific International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes (eg, code 789.00 is reported for abdominal pain even though a specific site of pain has been identified), and it may be helpful to review the elements of documentation that support specific code selection for abdominal pain and tenderness.
Chapter 18 of ICD-10-CM includes codes R00–R99 for signs and symptoms. The ICD-10-CM Official Guidelines for Coding and Reporting provide specific instruction for reporting symptoms such as abdominal pain.
• Codes for signs and symptoms are reported when no related definitive diagnosis has been established at the time of an encounter.
• A sign or symptom that is routinely associated with a diagnosed condition is not separately reported.
• A symptom that is not routinely associated with a definitive diagnosis may be separately reported. Sequence the definitive diagnosis code first.
ExampleA patient with pain in the right lower quadrant is seen at an urgent care clinic. The phy- sician documents rebound tenderness, right lower quadrant, possible appendicitis. The patient is sent to the emergency department for further workup. The same physician (or a physician of the same group and specialty) does not provide care at the hospital. The diagnosis at the time of the clinic encounter (eg, rebound tenderness of the right lower quadrant) is reported in conjunction with the appropriate procedure code for the evaluation and management (E/M) service. (Appendicitis documented as possible would not be reported because the guidelines for ICD-10-CM do not allow reporting of uncertain diagnoses for physician services.) If, however, the same physician or a physician of the same group and specialty provides observation or hospital care on the same date and it is established that the abdominal tenderness is a symptom of a more specific diag-nosis, only the code for the definitive diagnosis would be reported in conjunction with the procedure code representing the combined E/M services provided on that date.
Appendix B-15
Documenting Abdominal Pain or Tenderness
(continued on page 258)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

258
Like ICD-9-CM, ICD-10-CM includes separate codes for abdominal pain and abdomi-nal tenderness. In addition, rebound tenderness is separately classified in ICD-10-CM, allowing for a more specific description of the patient’s symptoms and, in some cases, better depicting the necessity of additional workup. Pain, tenderness, and rebound tenderness are further characterized by the generalized or localized site of discomfort. The Table shows ICD-10-CM codes for pain and tenderness by site.
2014 ICD-10-CM Codes for Abdominal pain and Tenderness
Site pain NOS TendernessRebound
Tenderness
Epigastric R10.13 R10.816 R10.826
Generalized, severe (acute abdomen) R10.0 See pain See pain
Generalized, not severe R10.84 R10.817 R10.827
Left upper quadrant R10.12 R10.812 R10.822
Left lower quadrant R10.32 R10.814 R10.824
Pelvic and perineal R10.2 See pain See pain
Periumbilical R10.33 R10.815 R10.825
Right upper quadrant R10.11 R10.811 R10.821
Right lower quadrant R10.31 R10.813 R10.823
Abbreviation: NOS, not otherwise specified.
Appendix B-15Transitioning to 10: Documenting Abdominal pain or Tenderness (continued from page 257)
Note: Colic is reported based on the age of the patient. A documentation of colic in an adult or child older than 12 months is reported as generalized abdominal pain. Colic in an infant is reported with code R10.83, colic. A diagnosis of renal colic is reported with code N23.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

259
Our recent “Transitioning to 10” articles have focused on elements of documentation that support assignment of specific International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes. This article will focus on elements of documentation to support coding of dermatitis.
In ICD-10-CM, categories L20–L30 and the terms dermatitis and eczema are used synonymously and interchangeably. However, in conditions such as dermatitis of the eyelid, the term eczematous or eczematoid is used as a descriptor to differentiate atopic from allergic contact dermatitis.
Coding Tip
High on the list of commonly reported diagnoses in pediatric ambulatory care is the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code for unspecified contact dermatitis, 692.9. ICD-10-CM code L23.9, allergic contact dermatitis with unspecified cause, is generally equivalent to 629.9. However, as noted in the August 2013 AAP Pediatric Coding Newsletter™, more specific codes should be reported when the cause of dermatitis is known. Codes for contact dermatitis may specify allergic contact or irritant contact dermatitis (when diagnosed) in addition to identifying the causative agent. For example, code L23.7 specifies allergic contact dermatitis due to nonfood plants, making this the appropriate code for reporting dermatitis due to poison ivy, oak, or sumac.
The differentiation between allergic and irritant contact dermatitis and identification of the causative substance are often based on history and presentation. When contact dermatitis is not distinguished as allergic or contact during an encounter, codes in category L25 are used to report unspecified contact dermatitis. When the causative agent is undetermined, it is appropriate to report code a code for contact dermatitis with unspecified cause (L23.9, L24.9, or L25.9).
Coding Tip
Codes for dermatitis of certain areas are specific to the site of the dermatitis. This includes diaper dermatitis, dermatitis of the eyelid, and dermatitis of the external ear.To arrive at a specific code for contact dermatitis using ICD-10-CM, the documentation elements shown in Table 1 are necessary. Documentation elements include the type of dermatitis and location or specified cause (when known). Incorporation of these terms in documentation will allow for more specific diagnosis assignment and may better support the necessity of services provided.
Appendix B-16
Documenting Dermatitis
(continued on page 260)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

260
Table 1. Documentation Elements Supporting Contact Dermatitis Code Selection
Contact—Allergic Contact—Irritant Contact—Not Specified as Allergic or Irritant
Due toAdhesives L23.1Cement L23.5Chemical products NEC L23.5Cosmetics L23.2Dander (cat) (dog) L23.81Drugs in contact
with skin L23.3a
Dyes L23.4Food in contact
with skin L23.6Hair (cat) (dog) L23.81Insecticide L23.5Metals (eg, chromium,
nickel) L23.0Plants, nonfood
(eg, poison ivy) L23.7Plastic L23.5Rubber L23.5Specified agent
(NECa) L23.89Unspecified cause L23.9
Ear (acute contact otitis externa)Right ear H60.531Left ear H60.532Bilateral H60.533
EyelidRight upper lid H01.111Right lower lid H01.112Left upper lid H01.114Left lower lid H01.115
Due toCement L25.3Chemical products
NEC L24.5Cosmetics L24.3Detergents L24.0Drugs in contact
with skin L24.4a Dyes L24.89Food in contact
with skin L24.6Insecticide L24.5Metals (eg, chromium,
nickel) L24.81Oils and greases L24.1Plants, nonfood L24.7Plastic L24.5Rubber L24.5Solvents L24.2Specified agent NEC
L24.89Unspecified cause L24.9
Due to Cement L25.3Chemical products NEC L25.3Cosmetics L25.0Dander (cat) (dog)
L23.81Drugs in contact
with skin L25.1a
Dyes L25.2Food in contact
with skin L25.4Hair (cat) (dog) L23.81Insecticide L25.3Plants, nonfood L25.5Specified agent
NEC L25.8Unspecified cause L25.9
Abbreviation: NEC, not elsewhere classified.aUse additional code for adverse effect, if applicable, to identify drug (T36–T50 with fifth or sixth character 5).
Documentation elements for other types of dermatitis (eg, atopic) are included in Table 2. For each specified type of dermatitis in the first column, the second column of the same row includes documentation elements that lead to more specific code assignment.
Codes are included in the tables for quick reference. See the ICD-10-CM code set for further coding instruction, including inclusion and exclusion notes that may guide to more accurate coding.
Appendix B-16Transitioning to 10: Documenting Dermatitis (continued from page 259)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

261
Table 2. Documentation Elements of Dermatitis Other Than Contact
Type Specified as
Atopic/eczematous
Ear (acute eczematoid otitis externa) Right ear H60.541 Left ear H60.542 Bilateral H60.543
Eyelid Right upper lid H01.131 Right lower lid H01.132 Left upper lid H01.134 Left lower lid H01.135
Flexural eczema L20.82Infantile (acute) (chronic) eczema L20.83Intrinsic (allergic) eczema L20.84Other atopic dermatitis L20.89
Dermatitis due to substances taken internally
Drugs and medicaments taken internally, generalized skin eruption L27.0a
Drugs and medicaments taken internally, localized skin eruption L27.1a
Ingested food L27.2Other substances taken internally L27.8Unspecified substance taken internally L27.9
Diaper Diaper or napkin rash L22Diaper dermatitis L22Diaper erythema L22Psoriasiform diaper rash L22
Dry skin Dry skin dermatitis L85.3Xerosis cutis L85.3Xeroderma of right upper eyelid H01.141Xeroderma of right lower eyelid H01.142Xeroderma of left upper eyelid H01.144Xeroderma of left lower eyelid H01.145
Seborrheic Cradle cap L21.0Seborrheic infantile dermatitis L21.1Other seborrheic L21.8
aUse additional code for adverse effect, if applicable, to identify drug (T36–T50 with fifth or sixth character 5).
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

262
Children with congenital heart disease may undergo procedures to repair or compensate for anomalies very early in life or be monitored until a defect is resolved without inter-vention. These children may have related health concerns into adulthood. So do you continue to report the congenital condition that is affecting the child’s health after the repair or closure? The guidelines for International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) provide the answers. These answers also apply to other types of anomalies.
When congenital anomalies are diagnosed during birth admission, ICD-9-CM and ICD-10-CM direct to report first the appropriate code for the live-born neonate and then codes describing congenital anomalies. The guidelines also instruct to report additional codes for manifestations that are not an inherent component of the malformation. Manifestations that are inherent to a malformation are not separately reported.
Following birth admission, congenital anomalies are reported at the time of diagnosis and until corrected.
ICD-9-CM: Codes from Chapter 14 may be used throughout the life of the patient. If a congenital anomaly has been corrected, a personal history code should be used to identify the history of the anomaly. Although present at birth, a congenital anomaly may not be identified until later in life. Whenever the condition is diag-nosed by the physician, it is appropriate to assign a code from codes 740–759.
ICD-10-CM: Whenever the condition is diagnosed by the physician, it is appro- priate to assign a code from codes Q00–Q99. Codes from Chapter 17 may be used throughout the life of the patient. If a congenital malformation or deformity has been corrected, a personal history code should be used to identify the history of the malformation or deformity. Although present at birth, malformation/deformation or chromosomal abnormality may not be identified until later in life.
Note that both guidelines include an instruction to report a personal history code when a patient has undergone correction of a congenital malformation or deformity. ICD-9-CM guidelines also provide definition of personal history but add an exception note for corrected congenital malformations indicating these are lifelong conditions.
Personal history codes explain a patient’s past medical condition that no longer exists and is not receiving any treatment, but that has the potential for recurrence, and therefore may require continued monitoring.
V13 Personal history of other diseases
Except: V13.4, Personal history of arthritis, and subcategory V13.6, Personal history of congenital (corrected) malformations. These conditions are life-long so are not true history codes.
Appendix B-17
Is This History? Coding Congenital Heart Disease
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

263
ICD-10-CM provides the same definition of personal history codes but does not include the same exception note. Instead, the ICD-10-CM tabular list provides the following inclusion and exclusion notes to guide coding of personal history of corrected congenital conditions:
Inclusion note: Conditions classifiable to Q00–Q89 that have been repaired or corrected
Excludes1:Congenital malformations that have been partially corrected or repaired but which still require medical treatment—code to condition
Excludes2:Other postprocedural states (Z98.-)Personal history of medical treatment (Z92.-)Presence of cardiac and vascular implants and grafts (Z95.-)Presence of other devices (Z97.-)Presence of other functional implants (Z96.-)Transplanted organ and tissue status (Z94.-)
The excludes1 note prohibits reporting of personal history of corrected congenital malformations when the malformation has been partially corrected or repaired but still requires medical treatment and also instructs to continue reporting the code for the congenital condition. This recognizes that surgery is not curative for all congenital conditions. If in doubt about whether a surgery was curative, coders should consult the physician.
The excludes2 note indicates conditions that are not represented by the personal history of corrected congenital deformity codes but that may be additionally reported when applicable.
ExamplesA child with a secundum atrial defect underwent minimally invasive repair with no residual defect. The device used is relatively new and all patients receiving it will require long-term monitoring.
ICD-9-CM: V13.65 Personal history of (corrected) congenital malformations of heart and circulatory system V45.09 Other specified cardiac device
ICD-10-CM: Z87.74 Personal history of (corrected) congenital malformations of heart and circulatory system Z95.818 Presence of other cardiac implants and grafts
(continued on page 264)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

264
A child with a small ventricular septal defect is seen in follow-up. The child is asymptomatic, but echocardiogram shows the defect has not yet completely closed.
ICD-9-CM: 745.4 Ventricular septal defectICD-10-CM: Q21.0 Ventricular septal defect
The following points review what the guidelines have instructed concerning reporting of congenital malformations:
• When diagnosed during birth hospitalization, congenital malformations are reported secondary to the code for live birth.
• Codes for congenital malformation should be reported when diagnosed and as often as indicated until a complete repair has been accomplished and the condition no longer requires active medical treatment.
• Report only manifestations that are not inherent to the malformation.• Personal history of corrected congenital malformation should be reported following
curative repair of the congenital condition. Codes for personal history of corrected congenital malformation represent a lifelong health condition that may alter health management and treatment.
Following these guidelines will help you correctly assign codes for congenital conditions and history of congenital conditions.
Appendix B-17Is This History? Coding Congenital Heart Disease (continued from page 263)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

265
Certain conditions originating in the perinatal period are reported with codes begin- ning with the letter P in International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM); these codes are found in Chapter 16 of the ICD-10-CM tabular list. Guidelines for reporting conditions found in ICD-10-CM Chapter 16 are similar to those in Chapter 15 of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). However, there are a few substantial differences. The Table on page 5 provides a comparison of the guidelines.
Chapter 16 of the tabular list for ICD-10-CM includes more helpful instructions for reporting conditions originating in the perinatal period.
• An inclusion note repeats the instruction from the guidelines.
Includes: conditions that have their origin in the fetal or perinatal period (before birth through the first 28 days after birth) even if morbidity occurs later
• Exclusion notes advise of conditions that are not included in the chapter but may be reported in addition to conditions reported with codes in Chapter 16 when coexisting.
Excludes 2: congenital malformations, deformations and chromosomal abnormalities (Q00–Q99)endocrine, nutritional and metabolic diseases (E00–E88)injury, poisoning and certain other consequences of external causes (S00–T88)neoplasms (C00–D49)tetanus neonatorum (A33)
• Codes for newborns affected by maternal factors and complications of pregnancy, labor, and delivery (p00–p04) are reported for newborns who are suspected of having an abnormal condition resulting from exposure from the mother or the birth process.
Note: These codes are for use when the listed maternal conditions are specified as the cause of confirmed morbidity or potential morbidity which have their origin in the perinatal period (before birth through the first 28 days after birth). Codes from these categories are also for use for newborns who are suspected of having an abnormal condition resulting from exposure from the mother or the birth process, but without signs or symptoms, and, which after examination and observation, is found not to exist. These codes may be used even if treatment is begun for a suspected condition that is ruled out [emphasis added].
Appendix B-18
Guidelines for Chapter 16
(continued on page 266)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

266
• Codes for extremely low birth weight, low birth weight, extreme immaturity, and preterm birth are found in category p07, disorders of newborn related to short gestation and low birth weight, not elsewhere classified. The first 2 instructions the follow also apply to codes in category p08, used to report long gestation and high birth weight. The exclusion note (Excludes 1) indicates that codes in category p07 are never reported in conjunction with codes in category p05.
Note: When both birth weight and gestational age of the newborn are available, both should be coded with birth weight sequenced before gestational age
Includes: the listed conditions, without further specification, as the cause of morbidity or additional care, in newborn
Excludes 1: low birth weight due to slow fetal growth and fetal malnutrition (p05.-)
Beyond the guidelines and instructions of the tabular list for perinatal conditions are other differences, such as the absence of ICD-10-CM codes for the following conditions:• Light for dates without mention of fetal malnutrition, 2,500 g and over• Light for dates with signs of fetal malnutrition, 2,500 g and over• Thirty seven or more completed weeks of gestation
This aligns ICD-10-CM codes with current definitions of prematurity and low birth weight that do not include these conditions.
These are the most significant differences in the guidelines and instructions for reporting conditions that originate in the perinatal period with ICD-10-CM. For information on ICD-10-CM codes for live-born infants, see “Crosswalking ICD-9-CM to ICD-10-CM: Coding for Live-born Neonates,” an online-exclusive article in the February 2012 AAP Pediatric Coding Newsletter™, at www.coding.aap.org/content.aspx?aid=11683. Note: The American Academy of Pediatrics has submitted a code proposal to the ICD Coordination and Maintenance Committee to consider adding in codes that more appropriately crosswalk over from ICD-9-CM code category V29. Currently, there is no way to report suspected and subsequently ruled out perinatal conditions. If approved, on October 1, 2015, there will be new codes for observation for suspected conditions in the perinatal period.
Appendix B-18Transitioning to 10: Guidelines for Chapter 16 (continued from page 265)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

267
Pediatricians will probably be remembering many International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for years to come, well after they are no longer reported. And of these, probably none will be more memorable than the most common reason for visits, the V20 diagnosis codes associated with well-child visits. For International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), the preventive medicine codes have been expanded to include 6 characters beginning with the letter Z (Table 1).
The ICD-10-CM tabular list instructs that codes for an abnormal finding at the well- newborn or well-child encounter are also reported. Additional diagnosis codes for abnormal findings may be reported when applicable, even when the problem does not require significant evaluation and management (E/M) in addition to the preventive medicine service provided.
Codes from category p07, disorders of newborn related to short gestation and low birth weight, not elsewhere classified, are for use for a child or an adult who was premature or had a low birth weight as a newborn and this is affecting the patient’s current health status (Table 2).
The following list is a translation of the ICD-9-CM codes for diagnoses included in the American Academy of Pediatrics coding guidance, “Supporting Breastfeeding and Lactation: The Primary Care Pediatrician’s Guide to Getting Paid” (www2.aap.org /breastfeeding/files/pdf/coding.pdf). Codes in this list describe many conditions common to the newborn and infant. The list also includes codes for conditions of the mother when associated with lactation. (This list is not all-inclusive; please check an ICD-10-CM coding manual or online reference for additional information when reporting these conditions.)
Table 1. Well-Newborn Diagnosis Codes
ICD-9-CM ICD-10-CM
V20.31 Health supervision for newborn under 8 days old
Z00.110 Health examination for newborn under 8 days old
V20.32 Health supervision for newborn 8 to 28 days old
Z00.111 Health examination for newborn 8 to 28 days old
V20.2 Routine infant or child health check
Z00.121 Encounter for routine child health examination with abnormal findings
Z00.129 Encounter for routine child health examination without abnormal findings
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification.
Appendix B-19
Newborn and Infant Visits
(continued on page 268)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

268
Table 2. Birth Weight and Gestational Agea
Low Birth Weight(LBW), 1,000–2,499 g
Extremely Low Birth Weight (ELBW), ≤999 g
Preterm Newborn, 28–37 Completed Weeks’ Gestation
Extreme Immaturity of Newborn (EIN), <28 Completed Weeks’ Gestation
p07.10 LBW newborn, unspecified weight
p07.00 ELBW newborn, unspecified weight
p07.30 Preterm newborn, unspecified weeks of gestation
p07.20 EIN, unspecified weeks of gestation
p07.14 LBW newborn, 1,000–1,249 g
p07.01 ELBW newborn, <500 g
p07.31 Preterm newborn, 28 weeks, 0–6 days
p07.21 EIN, <23 weeks, 0 days
p07.15 LBW newborn, 1,250–1,499 g
p07.02 ELBW newborn, 500–749 g
p07.32 Preterm newborn, 29 weeks, 0–6 days
p07.22 EIN, 23 weeks, 0–6 days
p07.16 LBW newborn, 1,500–1,749 g
p07.03 ELBW newborn, 750–999 g
p07.33 Preterm newborn, 30 weeks, 0–6 days
p07.23 EIN, 24 weeks, 0–6 days
p07.17 LBW newborn, 1,750–1,999 g
p07.34 Preterm newborn, 31 weeks, 0–6 days
p07.24 EIN, 25 weeks, 0–6 days
p07.18 LBW newborn, 2,000–2,499 g
p07.35 Preterm newborn, 32 weeks, 0–6 days
p07.25 EIN, 26 weeks, 0–6 days
p07.36 Preterm newborn, 33 weeks, 0–6 days
p07.26 EIN, 27 weeks, 0–6 days
p07.37 Preterm newborn, 34 weeks, 0–6 days
p07.38 Preterm newborn, 35 weeks, 0–6 days
p07.39 Preterm newborn, 36 weeks, 0–6 days
aIncludes the listed conditions, without further specification, as the cause of morbidity or additional care, in newborn; excludes low birth weight due to slow fetal growth and fetal malnutrition (p05.-); weight is sequenced before gestational age when both area available.
Appendix B-19Transitioning to 10: Newborn and Infants Visits (continued from page 267)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

269
FEEDING pROBLEMS ICD-10-CM
Neonatal difficulty in feeding at breast
p92.5
Slow feeding, newborn p92.2
Regurgitation and rumination of newborn
p92.1
Other specified feeding problems of newborn
p92.8
Bilious vomiting in newborn p92.01
Other vomiting in newborn p92.09
Feeding problem, infant (>28 days)
R63.3
Vomiting, infant (>28 days) R11.10
Projectile vomiting, infant (>28 days)
R11.12
JAUNDICE ICD-10-CM
Neonatal jaundice from breast milk inhibitor
p59.3
Neonatal jaundice, unspecified
p59.9
Neonatal jaundice associ-ated with preterm delivery
p59.0
WEIGHT AND HYDRATION ICD-10-CM
Dehydration, neonatal p74.1
Failure to thrive (FTT), newborn
p92.6
Weight loss R63.4
Underweight R63.6
Slow weight gain (FTT), infant (>28 days)
R62.51
Abnormal weight gain R63.5
See also the diagnoses associated with size and maturity included in Table 2.
Neonate/Infant
INFANT DISTRESS ICD-10-CM
Fussy infant/baby R68.12
Excessive crying, infant R68.11
Infantile colic (age ≤12 months)
R10.83
GASTROINTESTINAL ISSUES
ICD-10-CM
Abnormal stools R19.5
Neonatal diarrhea p78.3
Diarrhea, unspecified (>28 days)
R19.7
Change in bowel habits R19.4
MOUTH ICD-10-CM
Ankyloglossia Q38.1
High arched palate Q38.5
OTHER ICD-10-CM
Follow-up after completed treatment other than malignant neoplasm
Z09
When the original reason for visit has resolved, report also codes in categories Z86–Z87 to indicate personal history of disease.
(continued on page 270)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

270
Appendix B-19Transitioning to 10: Newborn and Infants Visits (continued from page 269)
LACTATION-ASSOCIATED BREAST AND NIppLE ICD-10-CM
Abscess, breast/mastitis, infective O91.13
Blocked milk duct/mastitis, interstitial O91.23
Mastitis in adoptive mother N61
Breast engorgement, ductal O92.79
Breast engorgement in adoptive mother N64.59
Burning pains, hyperesthesia of breast in lactation O92.79
Galactocele O92.79
Other specified nipple/breast infection associated with lactation O91.23
Impetigo (staph), nipple O91.03, L01.00
Candidiasis, nipple or breast O91.03, B37.89
Nipple infection O91.03
Nipple, cracks or fissures O92.13
Nipple, sore O92.79
Retracted nipple O92.03
Ectopic or axillary breast tissue Q83.8
Other specified nipple/breast anomaly Q83.8
Mother’s Healtha
a ICD-10-CM O codes represent conditions of the mother in pregnancy, childbirth, and the puerperium and are reported only on claims for care of the mother. E/M of conditions of the mother should be separately documented outside the newborn record and reported only on claims for services to the mother (ie, not the newborn).
Lactation ICD-10-CM
Agalactia, failure to lactate O92.3
Hypogalactia O92.4
Lactation, delayed O92.79
Lactation, suppressed (elective, secondary, therapeutic) O92.5
Other specified disorders of lactation O92.79
Supervision of lactation Z39.1
CONSTITUTIONAL ICD-10-CM
Disrupted sleep cycle G47.20
Fatigue R53.83
OTHER ICD-10-CM
Follow-up after completed treatment other than malignant neoplasm Z09
When the original reason for visit has resolved, report also codes in categories Z86–Z87 to indicate personal history of disease.
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

271
“For accurate reporting of ICD-10-CM diagnosis codes, the documentation should describe the patient’s condition, using terminology which includes specific diagnoses as well as symptoms, problems, or reasons for the encounter. There are ICD-10-CM codes to describe all of these.”
This quote is from the official guidelines for reporting diagnoses with International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). This is the overarching instruction for reporting diagnoses, but throughout the remaining guide-lines, more specific instructions can be found. These instructions advise what and what not to report and the order in which multiple conditions should be listed. Although there is little change from the guidelines for reporting ICD-9-CM, a brief review would be valuable as the transition to ICD-10-CM nears.
How Many Diagnoses to ReportThe guideline instructions for reporting multiple conditions noted in an encounter are as follows:
■■ Code all documented conditions that coexist at the time of the encounter/visit and require or affect patient care treatment or management.
■■ Do not code conditions that were previously treated and no longer exist. However, history codes (categories Z80–Z87) may be used as secondary codes if the historical condition or family history has an effect on current care or influences treatment.
■■ Signs and symptoms that are associated routinely with a disease process should not be assigned as additional codes unless otherwise instructed by the classification. Additional signs and symptoms that may not be associated routinely with a disease process should be coded when present.
■■ Manifestations due to an underlying etiology should be reported in addition to the underlying condition.
The first bullet in this list may have the greatest effect on diagnosis reporting. It is helpful to think of this guideline in an abbreviated fashion as “Code all documented conditions that require or affect patient care treatment or management at this encounter.” This statement can inform decisions on what elements of the patient’s medical history and which signs and symptoms merit reporting. If the answer to the question, “Did this condition require or affect patient care at this encounter?” is yes, the condition should be reported. This may apply to a sign or symptom that is routinely associated with a condition but by its presence affects treatment or management options (eg, clinical guidelines indicate different management based on presence or absence of a specific symptom).
Likewise, manifestations of disease may reflect the state of a patient’s chronic condition (eg, severity, level of control) and should be reported when care is affected.
Appendix B-20
Signs, Symptoms, and Manifestations
(continued on page 272)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

272
Sequencing Diagnosis CodesThe guidelines instruct physicians and other health care professionals to list first the diagnosis, condition, problem, or other reason chiefly responsible for the services pro-vided at an encounter. Note that the guidelines do not instruct to report first the patient’s chief complaint, as this may not be the condition chiefly responsible for the services pro-vided at an encounter. Sequencing diagnoses according to the guidelines can help place emphasis on underlying conditions and overall patient presentation at an encounter.
Listing first applies to the documentation of the encounter and in the linking of diagnosis codes to the services reported on the claim. While this is reasonably simple, there are additional guidelines that support appropriate reporting. One such guideline defines use of the word with in ICD-10-CM. It should be interpreted to mean “associated with” or “due to” when it appears in a code title, the alphabetic index, or an instruction of the tabular list. The term with is found immediately following some main terms in the alphabetic index. (Also watch for the term due to included alphabetically under some main terms.)
Here is a list of other sequencing guidelines.
■■ Etiology/manifestation: In most cases, the title of manifestation codes will include “in diseases classified elsewhere.” This code title indicates that it is a manifestation code. “In diseases classified elsewhere” codes are never permitted to be used as first-listed diagnosis codes. They must be used in conjunction with an underlying condition code and must be listed following the underlying condition. (Keep these codes together when included in a longer list of codes.)
■■ “Code first” and “Use additional code” notes are also used as sequencing rules in ICD-10-CM for certain codes that are not part of an etiology/manifestation com- bination. When there is a “code first” note and an underlying condition is present, the underlying condition should be sequenced first.
■■ “Code, if applicable, any causal condition first” notes indicate that this code may be assigned as a first-listed diagnosis when the causal condition is unknown or not applicable. If a causal condition is known, the code for that condition should be sequenced as the principal or first-listed diagnosis.
■■ A “code also” note instructs that 2 codes may be required to fully describe a condi-tion, but this note does not provide sequencing direction. Report first the condition that most affected treatment or management during the encounter.
This guidance on what to report and the sequencing of conditions could get overlooked as physicians and coders focus on other aspects of transitioning to ICD-10-CM. However, it is important to recognize that the diagnosis codes included on your claim are indica-tors of the reason for each service and the necessity for the level of service provided. Including and properly listing all conditions that coexist and require or affect patient management in an encounter better reflects the service provided.
Appendix B-20Transitioning to 10: Signs, Symptoms, and Manifestations (continued from page 271)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

273
Chapter-specific coding guidelines for physician coding and reporting are provided in Section IV of International Classification of Diseases, Ninth Revision, Clinical Modi-fication (ICD-9-CM) and International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). It is important that these guidelines be reviewed carefully prior to implementation of ICD-10-CM because they are considerably different from ICD-9-CM coding guidelines for fracture care and aftercare.
ICD-10-CM Chapter 19: Injury, poisoning, and Certain Other Consequences of External Causes (S00–T88)
Coding Traumatic Fractures• Theprinciplesofmultiplecodingofinjuriesshouldbefollowedincodingfractures.• Fracturesofspecifiedsitesarecodedindividuallybysiteinaccordancewithprovisions
within categories of ICD-10-CM codes and supporting documentation in the medical record.
Appendix B-21
Coding for Traumatic Fractures
– S02 (fracture of skull and facial bones) – S12 (fracture of cervical vertebra
and other parts of the neck) – S22 (fracture of rib, sternum, and
thoracic spine) – S32 (fracture of lumbar spine and pelvis) – S42 (fracture of shoulder and upper arm) – S49 (other and unspecified injuries
of shoulder and upper arm) – S52 (fracture of forearm)
– S59 (other and unspecified injuries of elbow and forearm)
– S62 (fracture at wrist and hand level) – S72 (fracture of femur) – S79 (other and unspecified injuries of hip
and thigh) – S82 (fracture of lower leg and ankle) – S89 (other and unspecified injuries
of lower leg) – S92 (fracture of foot and toe, except ankle)
• Afracturethatisnotdocumentedasopenorclosedshouldbecodedasaclosedfracture.• Afracturethatisnotdocumentedasdisplacedornotdisplacedcannotbecoded
as displaced.• Codesformultiplefracturesaresequencedinaccordancewiththeseverityofthefracture.• Traumaticfracturesarecodedusinganappropriateseventhcharactercode.
Initial Encounters for Fracture CareThe initial encounter for active treatment of the fracture (eg, surgical treatment, emergency department encounter, evaluation and treatment by a new physician) is reported using seventh character code A, B, or C. Seventh character codes A, B, and C are also used to identify the initial encounter for the patient who delayed seeking treatment for an open or closed fracture.
A: Initial encounter for closed fractureB: Initial encounter for open fracture type I or II Initial encounter for open fracture not otherwise specifiedC: Initial encounter for open fracture type IIIA, IIIB, or IIIC
(continued on page 274)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

274
Subsequent Encounters for Fracture CareSeventh character codes D, E, and F are used to report routine follow-up fracture care (eg, cast change or removal, removal of external or internal fixation device, medication adjust-ment, postoperative visits) during the healing or recovery phase of open or closed fractures.
D: Subsequent encounter for closed fracture with routine healingE: Subsequent encounter for open fracture type I or II with routine healingF: Subsequent encounter for open fracture type IIIA, IIIB, or IIIC with routine healing
Seventh character codes G, H, J, K, M, N, p, Q, and R are used to report care of complica-tions of open or closed fracture healing, such as delayed healing, malunion, or nonunion.
G: Subsequent encounter for closed fracture with delayed healingH: Subsequent encounter for open fracture type I or II with delayed healingJ: Subsequent encounter for open fracture type IIIA, IIIB, or IIIC with delayed healingK: Subsequent encounter for closed fracture with nonunionM: Subsequent encounter for open fracture type I or II with nonunionN: Subsequent encounter for open fracture type IIIA, IIIB, or IIIC with nonunionp: Subsequent encounter for closed fracture with malunionQ: Subsequent encounter for open fracture type I or II with malunionR: Subsequent encounter for open fracture type IIIA, IIIB, or IIIC with malunion
Seventh character code S is assigned to report complications or conditions that arise as a direct result of a condition. It identifies the injury responsible for the sequela. When reporting the sequela, report the injury code that caused the sequela and the code for the sequela itself. The specific type of sequela is sequenced first, followed by the injury code.
S: Sequela
Care for complications of surgical treatment for fracture repairs during the healing or recovery phase should be coded with the appropriate complication codes. For example, a subsequent encounter for infection due to internal fixation device of the right humerus is reported with ICD-10-CM code T84.610D. (The seventh character code D reflects a subsequent encounter.)
Codes Z48–Z51 (encounter for aftercare) are not used to report follow-up encounters for traumatic fractures because seventh character codes designate aftercare.
Each fracture code category includes a list of appropriate seventh character codes. For example, when reporting an unspecified right clavicular fracture (S42.001), the seventh digit will be reported with codes A, B, D, G, K, p, or S.
Let’s code the vignette from “Coding Fracture Care: And the Answer Is?” (see Electronic Pages on http://coding.aap.org) using ICD-10-CM codes. To summarize, a 9-year-old established patient with a non-displaced buckle fracture of the distal right radius is seen and treated. The patient is seen again in follow-up several weeks later and is healing well.
The initial visit will be reported with ICD-10-CM code S52.521A (torus fracture of lower end of right radius, initial encounter). The subsequent encounter will be reported with ICD-10-CM code S52.521D (torus fracture of lower end of right radius, subsequent encounter with routine healing).
Appendix B-21Transitioning to 10: Coding for Traumatic Fractures (continued from page 273)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

275
When it comes to reporting injuries, International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) provides specificity that International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) lacked.
ICD-10-CM codes for most injuries will be reported with the S codes found in Chapter 19 of the tabular list. Unlike ICD-9-CM, which classified injuries by category of injury, S codes are divided into blocks based on single body regions.
Appendix B-22
Sprains and Strains
(continued on page 276)
S00–S09 Injuries to the headS10–S19 Injuries to the neckS20–S29 Injuries to the thoraxS30–S39 Injuries to the abdomen,
lower back, lumbar spine, pelvis, and external genitals
S40–S49 Injuries to the shoulder and upper arm
S50–S59 Injuries to the elbow and forearm
S60–S69 Injuries to the wrist, hand, and fingers
S70–S79 Injuries to the hip and thighS80–S89 Injuries to the knee and
lower legS90–S99 Injuries to the ankle and foot
Chapter 19 also includes T codes that cover injuries to unspecified body regions as well as poisoning, burns, corrosions, and certain other consequences of external causes.
A key change in ICD-10-CM is the differentiation of a sprain of a ligament from a strain of a muscle or tendon. These conditions were reported with a single code by site in ICD-9-CM.
ExamplesFor a follow-up visit for a sprain of the calcaneofibular ligament of the right ankle, code as follows:
ICD-9-CM845.02 Sprains and strains of ankle and foot; ankle; calcaneofibular (ligament)
ICD-10-CMS93.411D Sprain of calcaneofibular ligament of right ankle, subsequent encounter
For the initial encounter for a strain of extensor digitorum longus of the right foot, code as follows:
ICD-9-CM845.19 Sprains and strains of ankle and foot; foot; other
ICD-10-CMS96.011A Strain of muscle and tendon of long flexor muscle of toe at ankle and
foot level, right foot, initial encounter
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

276
Appendix B-22Transitioning to 10: Sprains and Strains (continued from page 275)
The seventh character represents the type of encounter—A is initial, D is subsequent, and S is sequela. The addition of the seventh character S to ICD-10-CM codes for injuries allows for a simpler and more specific mechanism than ICD-9-CM, which classified sequela (late effects) to a different category, Late Effects of Injuries, Poisonings, Toxic Effects, and Other External Causes (905–909).
ExampleA patient is seen for a sequela of strained extensor digitorum longus of the right foot.
ICD-9-CM905.7 Late effects of musculoskeletal and connective tissue injuries; late effect of
sprain and strain without mention of tendon injury
ICD-10-CMS96.011S Strain of muscle and tendon of long flexor muscle of toe at ankle and foot
level, right foot, encounter for sequela
From the initial injury until healing is complete, these codes allow for more specific reporting. Here’s hoping that the sequela codes are seldom necessary. (As with ICD-9-CM, there are also codes to report the external cause of injury, but those are the stuff of another article.)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

277
Concerned parents often seek reassurance from pediatricians when their children experience the bumps and bruises of childhood. Finding diagnoses for these injuries will change a bit with the transition to International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) classifies injuries first by type of injury and then body part; for example, all superficial injuries such as abrasions, blisters, and bug bites are found in categories 910–919 with subcategories for body areas.
In ICD-10-CM, injuries are classified according to body part and then type of injury; for example, injuries to the head are reported with codes in categories S00–S09 with subcategories for types of injuries.
These categories begin with codes for superficial injuries. Types of superficial injuries included here are abrasions, nonthermal blisters, contusions, external constriction, superficial foreign body, insect bites, and other superficial bites.
ICD-10-CM guidelines provide a few instructions that are helpful when selecting a code.
• Whencodinginjuries,assignseparatecodesforeachinjuryunlessacombinationcode is provided, in which case the combination code is assigned.
• Thecodeforthemostseriousinjury,asdeterminedbytheproviderandthefocusoftreatment, is sequenced first.
• Superficialinjuriessuchasabrasionsorcontusionsarenotcodedwhenassociatedwith more severe injuries of the same site.
• AftercareZ codes should not be used for aftercare for conditions such as injuries or poisonings, where seventh characters are provided to identify subsequent care. For example, for aftercare of an injury, assign the acute injury code with the seventh character D (subsequent encounter).
• TheseventhcharacterS identifies the injury responsible for the sequela. The specific type of sequela (eg, scar) is sequenced first, followed by the injury code with seventh character S.
• UseanadditionalcodefromcategoryZ18 to identify any retained foreign body when applicable.
• Externalcause-of-morbiditycodesfromChapter20shouldbeassignedinadditionto injury codes to identify the cause, intent, place, activity, and status of the patient at the time of the accident.
Appendix B-23
Bites, Bruises, and Other Superficial Injuries
(continued on page 278)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

278
ExampleA child is seen for evaluation after falling from her bike while riding on her home drive-way. The parents are concerned that the child may have a serious injury to her wrist because she tried to catch herself when falling. After examination and obtaining x-ray film, no fracture or dislocation is found. The child has abrasions on her right hand and right knee. Diagnoses are abrasions to right hand and right knee.
S60.511A Abrasion of right hand
S80.211A Abrasion, right knee
V18.0XXA Pedal cycle driver injured in non-collision transport accident in non-traffic accident
Y92.014 Private driveway to single-family (private) house as the place of occurrence of the external cause
Y99.8 Other external cause status (leisure activity)
Note that seventh character A for initial encounter is used to complete the injury and external-cause codes. The seventh character is not required for the place of occurrence or status code. No activity code was reported because ICD-10-CM guidelines instruct that “[a] code from category Y93 is appropriate for use with external cause and intent codes if identifying the activity provides additional information about the event.” In this example, cause-of-injury code V18.0XXA already identifies that the patient was the driver of a pedal cycle (bicycle) at the time of the injury. Place of occurrence, activity, and status codes are necessary only on the initial claims related to an accident.
The extent of coding for these superficial injuries may appear complex, but there is reason for this. The 5 codes included in this example tell us that this was the initial encounter with this physician for a child who incurred abrasions to her right hand and right knee in a non-collision, non-traffic accident while riding her bike as a leisure activity on the driveway of her residence, which is a single-family house. A claim with this information should be ready for adjudication without delay to obtain accident information and determine liability.
Appendix B-23Transitioning to 10: Bites, Bruises, and Other Superficial Injuries (continued from page 277)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

279
Diagnosis in International Classification of Diseases, Ninth Revision, Clinical Modification: Initial encounters related to an injury should include codes for type of injury, external cause, activity, place of occurrence, and status of patient.
Diagnosis in International Classification of Diseases, 10th Revision, Clinical Modification: All encounters for injuries should include codes for the type of injury and external cause. Initial encounters should also include codes for activity, place of occurrence, and status of patient.
692.71 Sunburn L55.0 Sunburn of first degree
692.76 Sunburn of second degree L55.1 Sunburn of second degree
Add seventh character: A, initialecounter; S, subsequent encounter; D, sequela.
944.24 Blisters, epidermal loss (second degree), two or more digits including thumb
T23.041 Burn of unspecified degree of multiple right fingers (nail), including thumb
T23.042 Burn of unspecified degree of multiple left fingers (nail),
including thumb
078.12 Plantar wart B07.0 Plantar wart
380.12 Acute swimmers’ ear H60.331 Swimmer’s ear, right ear
H60.332 Swimmer’s ear, left ear
H60.333 Swimmer’s ear, bilateral
133.8 Other acariasis (eg, chiggers) B88.0 Other acariasis (eg, chiggers)
Add seventh character: A, initialencounter; S, subsequent encounter;D, sequela.
992.1 Heat syncope T67.1XX Heat syncope
992.3 Heat exhaustion, anhydrotic T67.3XX Heat exhaustion, anhydrotic
992.5 Heat exhaustion, unspecified T67.5XX Heat exhaustion, unspecified
Add seventh character: A, initialencounter; S, subsequent encounter;D, sequela.
993.2 Other and unspecified effects of high altitude (mountain sickness)
T70.29X Other effects of high altitude
Add seventh character: A, initialencounter; S, subsequent encounter;D, sequela.
Appendix B-24
Summertime Diagnoses
(continued on page 280)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

280
994.6 Motion sickness (sea, travel) T75.3XX Motion sickness (Use additional external cause code to identify vehicle or type of motion [Y92.81-, Y93.5-])
005.9 Food poisoning, unspecified A05.9 Bacterial foodborne intoxication, unspecified
309.89 Other specified adjustment reactions (homesickness)
F43.20 Adjustment disorder, unspecified
Add seventh character: A, initialencounter; S, subsequent encounter;D, sequela.
No specific code for insect bites to multiple sites is included in ICD-10-CM;code bite(s), by site, superficial, insect.
Examples
919.4 Insect bite, nonvenomous, multiple sites without
mention of infection
S80.861 Insect bite (nonvenomous), right lower leg
919.5 Insect bite, nonvenomous, multiple sites, infected
S80.862 Insect bite (nonvenomous), left lower leg
Add seventh character: A, initialencounter; S, subsequent encounter; D, sequela.
Code by specific venom found in ICD-10-CM table of drugs andchemicals. Examples
989.5 Toxic effect, venom (snake, jellyfish)
T63.011 Toxic effect of rattlesnake venom, accidental (unintentional)
T63.331 Toxic effect of venom of brown recluse spider, accidental (unintentional)
T63.461 Toxic effect of venom of wasps, accidental (uninten-tional) (includes yellow jacket)
T63.621 Toxic effect of contact with other jellyfish, accidental (unintentional)
Appendix B-24Transitioning to 10: Summertime Diagnoses (continued from page 279)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

281
External Cause of Injury
(Assign for initial encounter only.)
External Cause of Injury
(Add seventh character: A, initialencounter; S, subsequent encounter;D, sequela.)
E923 Accident caused by explosive material, fireworks
W39.XXX Discharge of firework
E884.0 Fall from playground equipment
W09.0XX Fall on or from playground slide
W09.1XX Fall from playground swing
W09.2XX Fall on or from jungle gym
W09.8XX Fall on or from other playground equipment
E885.1 Fall from roller skates (heelies, wheelies)
V00.111 Fall from in-line roller-skates
V00.121 Fall from non-in-line roller-skates
V00.151 Fall from heelies
E885.2 Fall from skateboard V00.131 Fall from skateboard
E900.0 Excessive heat due to weather conditions (sunstroke)
X30.XXX Exposure to excessive natural heat
E902.0 Residence or prolonged visit at high altitude
W94.11X Exposure to residence or prolonged visit at high altitude
E903 Travel and motion T75.3XX Motion sickness
E905.6 Venomous marine animals and plants (jellyfish)
X58.XXX Exposure to other specified factors (venomous animal)
E906.4 Bite of nonvenomous arthropod
W57.XXX Bitten or stung by nonvenomous insect and other nonvenomous arthropods
E826.1 Pedal cycle accident, pedal cyclist
V18.0XX Pedal cycle driver injured in noncollision transport accident in nontraffic accident
E828.2 Accident involving animal being ridden, rider of animal
V80.010 Animal-rider injured by fall from or being thrown from horse in noncollision accident
(continued on page 282)From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

282
Activities associated with injuries
(Assign for initial encounter only; not applicable to poisonings, adverse effects, misadventures, or late effects.)
Activities associated with injuries
(Assign for initial encounter only;not applicable to poisonings, adverseeffects, misadventures, or sequela.)(no seventh character required)
E007.8 Physical games generally associated with school recess, summer camp and children
Y93.6A Activity, physical games generally associated with school recess, summer camp and children
E001.0 Walking, marching and hiking Y93.01 Activity, walking, marching and hiking
E001.1 Running Y93.02 Activity, running
E002.0 Swimming Y93.11 Activity, swimming
E002.1 Springboard and platform diving
Y93.12 Activity, springboard and platform diving
E002.4 Underwater diving and snorkeling (SCUBA diving)
Y93.15 Activity, underwater diving and snorkeling
E002.5 Rowing, canoeing, kayaking, rafting and tubing
Y93.16 Activity, rowing, canoeing, kayaking, rafting and tubing
E002.6 Water skiing and wake boarding
Y93.17 Activity, water skiing and wake boarding
E002.7 Surfing, windsurfing and boogie boarding
E002.8 Water sliding
Y93.18 Activity, surfing, windsurfing and boogie boarding (includes water sliding)
E005.3 Trampoline Y93.44 Activity, trampolining
E006.0 Roller skating (inline) and skateboarding
Y93.51 Activity, roller skating (inline) and skateboarding
E006.1 Horseback riding Y93.52 Activity, horseback riding
E006.4 Bike riding Y93.55 Activity, bike riding
E008.3 Frisbee Y93.74 Activity, Frisbee
E029.2 Rough housing and horseplay Y93.83 Activity, rough housing and horseplay
Appendix B-24Transitioning to 10: Summertime Diagnoses (continued from page 281)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

283
place of Occurrence
(Assign for initial encounter only.)
place of Occurrence
(Assign for initial encounter only.) (no seventh character required)
E849.0 HomeE849.4 Place for recreation
and sportE849.6 Public building
(hotel, shop)E849.8 Other specified places
(beach, river, woods)
Y92.016 Swimming-pool in single-family (private) house or garden as the place of occurrence of the external cause
Y92.017 Garden or yard in single-family (private) house as the place of occurrence of the external cause
Y92.025 Garage of mobile home as the place of occurrence of the external cause
Y92.026 Swimming-pool of mobile home as the place of occurrence of the external cause
Y92.34 Swimming pool (public) as the place of occurrence of the external cause
Y92.480 Sidewalk as the place of occurrence of the external cause
Y92.481 Parking lot as the place of occurrence of the external cause
Y92.482 Bike path as the place of occurrence of the external cause
Y92.830 Public park as the place of occurrence of the external cause
Y92.831 Amusement park as the place of occurrence of the external cause
Y92.832 Beach as the place of occurrence of the external cause
Y92.833 Campsite as the place of occurrence of the external cause
Y92.828 Other wilderness area as the place of occurrence of the external cause (swamp, mountain, prairie, wilderness)
Y92.834 Zoological garden (Zoo) as the place of occurrence of the external cause
Y92.838 Other recreation area as the place of occurrence of the external cause
Y92.810 Car as the place of occurrence of the external cause
Y92.811 Bus as the place of occurrence of the external cause
Y92.812 Truck as the place of occurrence of the external cause
Y92.813 Airplane as the place of occurrence of the external cause
Y92.814 Boat as the place of occurrence of the external cause
(continued on page 284)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

284
patient Status
(Assign for initial encounter only.)
patient Status
(Assign for initial encounter only.) (no seventh characters required)
E000.2 Volunteer activity Y99.2 Volunteer activity
E000.8 Other external cause status (leisure activity)
Y99.8 Other external cause status (leisure activity)
Appendix B-24Transitioning to 10: Summertime Diagnoses (continued from page 283)
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.

New 2nd edition!You’ll use this handy quick-reference again and again as you integrate the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) nomenclature and code set into your practice. It eases the transition process by listing International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for the most common pediatric diagnoses right alongside their ICD-10-CM counterparts.
This updated second edition provides time-saving coding tips, tables, and tools specific to the crosswalked codes. An expansive index features ICD-10-CM–related articles on various implementation strategies, key transi-tion issues and considerations, and other current coding best practices.
Additional Pediatric Coding Resources From the American Academy of Pediatrics
y New editioN! Coding for Pediatrics 2016Written by pediatric coders for pediatric coders, this year’s completelyupdated edition includes all changes in Current Procedural Terminology (CPT®) codes for 2016—complete with guidelines for their application.You’ll also find expert guidance on ICD-10-CM transition anddocumentation.
y New! Pediatric ICD-10-CM: A Manual for Provider-Based CodingFor the pediatric provider, coder, and biller, here’s the most helpfuland easy-to-use manual on ICD-10-CM yet. This convenient resourcecondenses the vast ICD-10-CM code set into 400 pages of pediatrics-
related codes and guidelines.
y AAP Pediatric Coding Newsletter™This unique monthly service brings you timely updates and expert advice to help you maximize payment, save time, and implement businesspractices that help support quality care delivery. Features include a“Transitioning to 10” column with coding tips and guidelines forsuccessful ICD-10-CM migration.
Streamline the transition to “10”!
Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM
To order these and other pediatric resources, visit
2ndEdition
From Pediatric Code Crosswalk: ICD-9-CM to ICD-10-CM, 2nd edition: ,Linzer Sr, Jeffrey F.;, ;Hughes, Cindy;Dolan, BeckyDownloaded on Nov 1, 2020, 5:37 AM at 54.39.106.173Published by AAP, 2015. All rights reserved.
Recommended