References
Conclusions
1) Investigate the prevalence, types, and severity ofchildhood anemia and iron status by study nation, age,and gender
2) Examine protective and risk factors associated withanemia and ID
3) Study and document the possible associations betweenblood Mn, Zn, Co, Cd, Pb and iron biomarkers,considering relevant co-variables
Results
Study design
Introduction• Canada is among countries with the lowest prevalence ofanemia (3%).• This prevalence is invariably higher among its First Nations,particularly children1.• Childhood anemia is associated with growth, developmental,cognitive, psychomotor and immune system impairments.• In First Nations communities, iron and other micronutrientsdeficiencies, infections and lead exposure are frequent, andpossibly risk factors for iron deficiency (ID) and anemia2.• Higher intake of animal proteins (rich in bioavailable heme-iron), vitamin C (non-heme iron absorption enhancer), fruitsand vegetables (rich in vitamins) are considered protectivefactors against ID and anemia2.• Divalent metals − manganese (Mn), zinc (Zn), cobalt (Co), cadmium (Cd) and lead (Pb) − interact with iron at differentlevels in human body3.• ID may upregulates the absorption and concentration ofthese metals inside human body, possibly increasing theirtoxicities3.
• The study Youth Environment Study (YEH) wasconducted among four First Nation communities inQuebec in Québec, Canada (see Figure 1)• Two Anishinabe communities (Abitibi-Temiscamingue region)• Two Innu communities (North Shore region)
• Transversal study conducted in May-June and Sept-Oct 2015, with 198 participants aged 3 to 19 years
• Data collected relevant for the present project:• Anthropometric measurements• Blood samples: Hemoglobin (Hb) (in situ), inflammatory
biomarker (hs-CRP), and iron, Mn, Cd, Pb, Zn, Co biomarkers• Individual questionnaires:
• Socio-demographic• Food security & lifestyle• Food Frequency Questionnaires (FFQ) (traditional food & market
foods)• Intakes calculated based on FFQ and food composition data
Figure1:StudiedFirstNationsandcommunities
Objective(1)prevalenceofanemiaandID
DescriptivestatisticstypesofanemiaandID
Objective(2)riskfactorsforanemiaandID
StructuralEquationModeling
Objective(3)associations
Mn,Zn,Co,Cd,Pbandiron
MultipleregressionanalysisforIronbiomarkersandMn,Zn,Co,CdandPb
Figure2:Statisticalanalysis
1. GovernmentofCanada.(2016).QuebecIndigenousCommunityprofiles.RetrievedMarch13,20172. Couture,A.,Levesque,B.,Dewailly,É.,Muckle,G.,Déry,S.,&Proulx,J.-F.(2012).LeadexposureinNunavik:fromresearchtoaction.International
JournalofCircumpolarHealth,71,18591.3. Aschner,J.L.,&Aschner,M.(2005).Nutritionalaspectsofmanganesehomeostasis.MolecularAspectsofMedicine,26,353–362.4. Roth,J.A.,&Garrick,M.D.(2003).Ironinteractionsandotherbiologicalreactionsmediatingthephysiologicalandtoxicactionsofmanganese.
BiochemicalPharmacology,66(1),1–13.5. WHO.(2001).IronDeficiencyAnaemia:Assessment,PreventionandControl,Aguideforprogrammanagers.Aguideforprogramme mangers.6. Cooper,M.,Greene-Finestone,L.,Lowell,H.,Levesque,J.,&Robinson,S.(2012).IronsufficiencyofCanadians.HealthReports/StatisticsCanada,
CanadianCentreforHealthInformation
• Thanksextendedtostudyparticipants,theirparentsandprojectpartners
Studyfundedby:
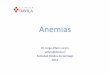
• IDandanemiaareconsiderablyhigherthanCHMSandcomparableinbothstudiednations• IDisparticularlyhighamong12-19yearsoldgirls• AccordingtoOMS:anemiaisamoderatepublichealthproblem
among6-11yearsoldboysand12-19yearsoldgirls• Higherintakeofpowderjuice(fortifiedwithvitamin
C)andrelatedvitaminCintake(anironabsorptionenhancer)isassociatedwithlowerIDandanemia
• HighbloodMn concentrationsissimilarbetweennationsandnoenvironmentalsources wereidentified
• LowbloodPb concentrations• BloodMn andCoconcentrationscorrelatesnegatively
withironstores• Thesepreliminaryfindingssuggestthatincreasing
intakeofvitaminC(fromothersourcesthanpowerjuicewhichareexcessivelyelevatedinaddedsugar)wouldpreventID,anemiaandbloodmanganeseexcessAcknowledgements
Characteristics of anemia and iron status and their associations with blood manganese and lead among children aged 3 to 19 years old from four First Nation communities in Québec
EmadTahir1,2,PierreAyotte1,2,3,MatthewLittle1,2,RichardE.Bélanger1,4,MichelLucas1,2,DonnaMergler5,ElhadjiA.LaouanSidi2,CommunityofWinneway– LongPointFirstNation,CommunityofLacSimon,CSSSTshukuminuKananiofNutashkuan,CommunityofUnamenShipu,NancyGros-LouisMcHugh6,MélanieLemire1,2
1NasivvikResearchChairinEcosystemApproachestoNorthernHealth,Axesantédespopulationsetpratiquesoptimalesensanté,CentrederechercheduCHUdeQuébec– UniversitéLaval;2Départementdemédecinesocialeetpréventive,UniversitéLaval,Québec,QC,Canada;3InstitutnationaldesantépubliqueduQuébec,Québec,QC,Canada;4Départementdepédiatrie,UniversitéLaval,Québec,QC,Canada;5CINBIOSE,UniversitéduQuébecàMontréal,Montréal,QC,Canada;6FirstNationofQuébecand
LabradorHealthandSocialServicesCommission,Wendake,QC,Canada
Study objectives
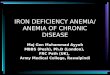
Figure4:ProportionsofIDbyagegroups:YEHvsCanadianHealthMeasuresSurvey(CHMS)
Figure5:Proportionsofanemiabyagegroups:YEHvsCHMS
RedlinesrefertoWHOreferencevaluesforpublichealthsignificanceofanemia 5,6
PleasenotethatCHMScodingforIDandanemiaisslightlydifferentthanintheYEHproject
Figure3:Prevalenceofanemia,anemiasubtypesandIDbynation
Table2:Resultsofthestructuralequationmodeling/factorialanalysisforprotective
andriskfactorsforHbandferritin
Modelsareadjustedforage,sex,nation,education,household,interviewer,inflammatorybiomarker,manganese ,iron,zincandvitamincintake,BMI,andsourcesofdrinkingwater.
Figure6:SignificantassociationsbetweenbloodMn,Coandserumferritinconcentrations(ironstores)
Resultsarepresentedfor193participants,5participantswereexcludeddueofmissingdata
• Higherintakeofpowderjuice(fortifiedwithvitaminC)andrelatedvitaminCintake(anironabsorptionenhancer)isassociatedwithlowerIDandanemia
• Modelsarecontrolledforhousehold,age,sex,nation,interviewerandbodymassindex(BMI)andsocioeconomicstatus
FactorStandardizedestimatesfor
Hb(95%CI)Standardizedestimatesfor
ferritin(95%CI)
Vegetablesandfruits 0.13(-0.38,0.52) 0.13(-0.16,0.44)
Powderjuice→vitaminC 0.15(0.004,0.16)* 0.15(0.02,0.27)*
Inflammatorymarkers - 0.1(-0.23,0.04) 0.12(0.04,0.18)*
Traditionalmeat 0.07(-0.17,0.32) 0.03(-0.29,0.36)
Marketmeat 0.02(- 0.34,0.37) - 0.02(-0.62,0.59)
Table3:DivalentmetalsinYEHbynationandcomparedtoCHMS
• Exclusionof3participantsbasedonliverdiseasesordysfunctions• BloodMnishigherandbloodPbislowerthaninCHMS(Cycle2or3)(3-19yrs old)
Manganese(Mn) Zinc(Zn) Cobalt(Co) Cadmium(Cd) Lead(Pb)
Essentialtraceelementandcofactorformanyenzymes
Essentialtraceelement,cofactorformanyenzymes
EssentialtraceelemententreinvitaminB12synthesis
Xenobiotic Xenobiotic
Food,airborne,water,miningactivities
Food,miningactivities,steelsmelting
Food,airborneduetometalsmelting
Smoking,wateringestion,batterydisposal
Oldresidentialpaints,huntingactivities
Neurobehavioral,memoryandmovementproblem
Hematological,gastrointestinaleffects,immunotoxic
Possiblycarcinogenictohuman
Chronicexposurecarcinogenic
Attention,IQ,hematological&neurobehavioral
Table1:Divalentmetalsprofile
Contact:[email protected]
>20%Moderatepublichealthproblem
>5%Mildpublichealthproblem
Anishinabe N=112
Role
Sourceof
expo
sure
Health
effects
MetalAnishinabe(n=106)Geo mean (range)
Innu(n=84)Geo mean (range)
BloodMn(µg/L ) 15.33(11.83,18.83) 16.17(12.71,19.63)
PlasmaZn(µg/L ) 1134.34(980.38,1288.30) 1081.87(935.09,1228.66)
BloodCo(µg/L ) 0.26(0.19,0.33)* 0.18(0.12,0.25)
BloodCd(µg/L ) 0.51(0.43,0.58) 0.48(0.40,0.56)
BloodPb(µg/L ) 5.35(3.51,7.65) 7.21(5.07,9.87)*
Figure7:InsignificantassociationsbetweenbloodCd,Zn,Pbandserumferritinconcentrations(ironstores)
*:significantassociationforcombineddirectandindirecteffects(p<0.05)
*:significantdifferencebetweennation(T-test,p<0.05)
Recommended