FluidBalanceinanEnhancedRecoveryPathway
EdwinItenberg,DO,FACS,FASCRSSt.JosephMercyOaklandMSQC/ASPIREMeetingApril28,2017
2
NoDisclosures
Introduction
3
• Theoptimalintravenousfluidregimenforpatientsundergoingmajorabdominalsurgeryisunclear.
• Perioperativefluidmanagementiscontroversial,withalargevariabilityindailypractice
• Maingoalofintraoperativefluidtherapyistomaintaintissueperfusionbyoptimizingintravascularvolumestatusandstrokevolume
©2015
1.ChappellD,JacobM,Hofmann-KieferK,etal.Arationalapproachtoperioperativefluidmanagement.Anesthesiology2008;109:723.2.LowellJA,Schifferdecker C,DriscollDF,etal.Postoperativefluidoverload:notabenignproblem.Crit CareMed1990;18:728.
EnhancedRecoveryAfterSurgery
4©2015
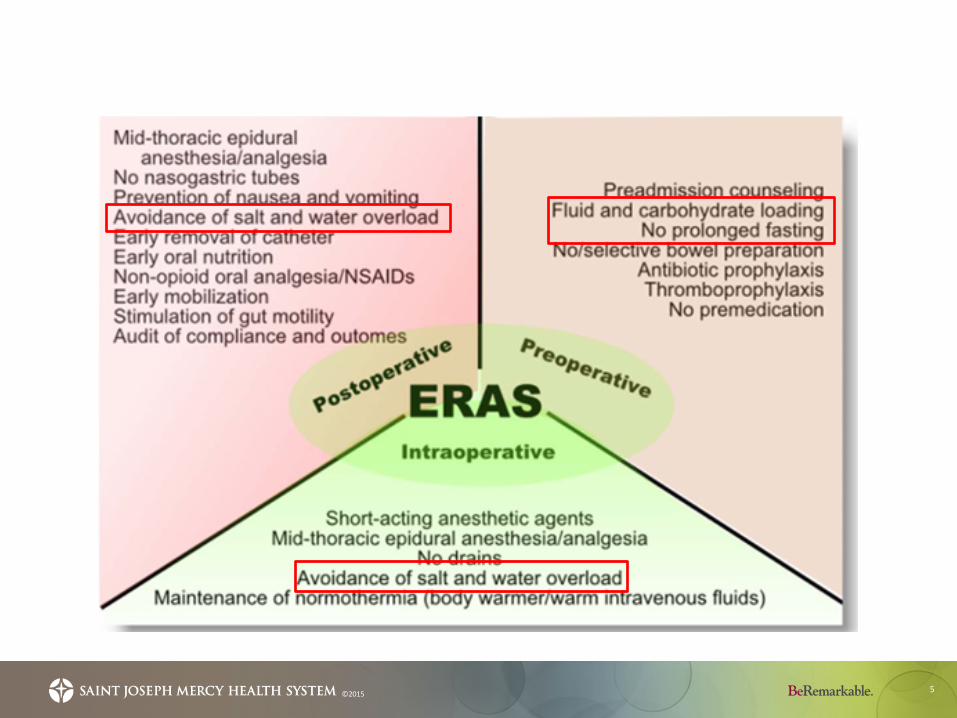
• ERAS,alsoknownas“fasttrack”programs,areevidence-basedprotocolsdesignedto:– reducesurgicaltraumaandpostoperativestress– minimizingpain– reducingcomplications– standardizemedicalcare– improveoutcomes– lowerhealthcarecostsandLOS
5©2015
EnhancedRecoveryAfterSurgery
6©2015
• WhatisthemostimportantcomponentoftheERASpathway?– Noprolongedfasting– Carbohydrateloading– Paincontrol– Fluidadministration– Earlyfeeding
FluidAdministration
7©2015
• Standardor“liberal”• Restrictive• Goaldirectedtherapy
• FluidmanagementwithinERASshouldbeviewedasacontinuumthroughthepreoperative,intraoperative,andpostoperativephases
FluidAdministration
8©2015
• Hypovolemialeadstolowcardiacoutputanddecreasedtissueperfusion
• Hypervolemiaassociatedwithincreasesinmorbidity,lengthofintensivecareunitstay,andpostoperativemortality
EffectonGITract
9©2015
• Incardiacsurgerypatients,plasmavolumeexpansiontoachievemaximalventricularstrokevolume,assessedbyoesophageal Doppler,ledtosignificantlybetterperfusionofthegastrointestinalmucosaandasignificantdecreaseinmajorpostoperativecomplications
• Incontrast,in57patientsundergoingbowelsurgery,nodifferencesinpostoperativeileusandhospitalstaywerefoundintheinterventiongroupreceivinggoal-directedfluidtherapycomparedwithstandardfluidinfusions
1. MythenMG,WebbAR.Perioperativeplasmavolumeexpansionreducestheincidenceofgutmucosalhypoperfusion duringcardiacsurgery.ArchSurg 1995;130:423–9.
2. ConwayDH,Mayall R,Abdul-LatifMS,GilliganS,Tackaberry C.Randomised controlledtrialinvestigatingtheinfluenceofintravenousfluidtitrationusingoesophageal Dopplermonitoringduringbowelsurgery.Anaesthesia 2002;57:845–9
Hypovolemia
10©2015
• Leadstodecreaseintissueperfusionà1. Acutekidneyinjury2. Splanchnicvasoconstriction
Chieveley-WilliamsS,Hamilton-DaviesC.Theroleofthegutinmajorsurgicalpostoperativemorbidity.Int Anesthesiol Clin 1999;37:81.
11©2015
AcuteKidneyInjury
• Majorconcernisthatoliguriaisasignofdevelopingrenalfailure
• Asaresult,surgeonsandanesthesiologistsstrivetomaintainUOPmostcommonlywithbolusesofintravenousfluid.
• IntraoperativeUOPmaynotreflectfluidstatusorpredictrenalfailure
• WithinanERASprotocol,postoperativehypotensionandlowUOParecommonwithinthefirst24hr,whereasrenaldysfunctionisextremelyrare
1. Kheterpal S,Tremper KK,Englesbe MJ,etal.Predictorsofpostoperativeacuterenalfailureafternoncardiac surgeryinpatientswithpreviouslynormalrenalfunction.Anesthesiology2007;107:892-902.
2. Hubner M,LovelyJK,HuebnerM,Slettedahl SW,JacobAK,LarsonDW.Intrathecalanalgesiaandrestrictiveperioperativefluidmanagementwithinenhancedrecoverypathway:hemodynamicimplications.JAmColl Surg 2013;216:1124-34.
Hypervolemia
12©2015
• Increasedextracellularfluidinthebowelcanleadsequentiallytogastrointestinaledema,decreasedgastrointestinalmotility,andileus
• Inaddition,forpatientsundergoingbowelsurgery,intestinaledemacanincreasetensionatbowelanastomosesandmaycontributetoanastomoticdehiscence
1. Nisanevich V,Felsenstein I,Almogy G,etal.Effectofintraoperativefluidmanagementonoutcomeafterintraabdominalsurgery.Anesthesiology2005;103:25.2. Holte K,SharrockNE,Kehlet H.Pathophysiologyandclinicalimplicationsofperioperativefluidexcess.BrJAnaesth 2002;89:622.
Hypervolemia
13
Colon&RectalSurgery• Increaseddurationofileus,postoperativecomplications,andhospitalstayaftermajorabdominalsurgery
• Delayedgastricemptyingandileus• Difficultyofadequatelyassessingnormovolemia
©2015
1. Nisanevich V,Felsenstein I,Almogy G,etal.Effectofintraoperativefluidmanagementonoutcomeafterintraabdominalsurgery.Anesthesiology2005;103:25–32.2. LoboDN,BostockKA,NealKR,etal.Effectofsaltandwaterbalanceonrecoveryofgastrointestinalfunctionafterelectivecolonicresection:arandomised
controlledtrial.Lancet2002;359:1812–8
14©2015
So,whatshouldwedo?
15©2015
• Manystudiesexaminedfluidadministration,butfewinthecontextofanERASpathway
• 100patientstotal• GDTmeanof2,115mL• Restrictivearm1500mL
16©2015
• RetrospectivereviewofPremierdatabase• 84,722colon,22,178rectal,and548,526primaryhiporknee
replacementsurgicalpatients• Highfluidvolumesignificantlyassociatedwithincreasedlengthof
stayandtotalcosts• Highfluidutilizationassociatedwithincreasedpresenceofpost-op
ileus• Worseoutcomesareseenintheextremesoffluidadministration• Protocoledapproachtowardoptimalfluidmanagementmay
improveoutcomes
17
• Clearanceoffluidsduringgeneralanesthesiaisonlyasmallfractionofthatobservedwhenawake
• Positivefluidbalancehasbeenshowntobeassociatedwithinincreasedincidenceofacutekidneyinjury(AKI)aftermajorsurgery
• Laparoscopicsurgery
©2015
1. Ewaldsson CA,HahnRG.Kineticsandextravascularretentionoflacetated Ringer’ssolutionduringisofluraneorpropofol anesthesiaforthyroidsurgery.Anesthesiology2005;103:460-9.
2. AlpertRA,RoizenMF,HamiltonWK,etal.Intraoperativeurinaryoutputdoesnotpredictpostoperativerenalfunctioninpatientsundergoingabdominalaorticrevascularization.Surgery1984;95:707-11.
18©2015
• Noliteraturecomparinggoal-directedtherapyorrestrictivetostandardtherapyinanenhancedrecoveryprotocol
• Whenboththeperioperativesurgeon-drivenelementsandtheintraoperativepainandfluidmanagementanesthesia-drivenelementsarecombined,thebenefitsofenhancedrecoveryaremaximized
Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg. 2009;144:961–969.
Outcomes
19
• Amulticenterrandomizedtrialincluding156patientsfoundthatpatientsinthefast-trackprogramhadsignificantlydecreasedmedianLOSandfewerpostoperativecomplications(5versus9days,and21versus49percent,respectively).
• Inoneretrospectivestudy,541consecutiveproceduresreviewed.MedianLOSwas3days,>25%dischargedwithin48hrs.
• Factorsassociatedwithdischargein48hrs:• FullcompliancewithERASpathway• Loworalopiateintake• Highsurgeonvolume
©2015
1. MullerS,Zalunardo MP,Hubner M,etal.Afast-trackprogramreducescomplicationsandlengthofhospitalstayafteropencolonicsurgery.Gastroenterology2009;136:842.
2. LarsonDW,etal.Outcomesafterimplementationofamultimodalstandardcarepathwayforlaparoscopiccolorectalsurgery.BJS2014;101:1023-30.
ThankYou!
20©2015
Questions?
21©2015
Recommended