EUROTIMES | Volume 17 | Issue 9
Ab interno trabeculectomy performed with the Trabectome (NeoMedix Corp) appears to offer a safe and straightforward
method of lowering intraocular pressure (IOP) in primary open-angle glaucoma (POAG) compared to conventional trabeculectomy, Douglas J Rhee MD told delegates attending the World Ophthalmology Congress.
“Our own clinical experience and the available studies suggest that the Trabectome is an elegant and safe anterior segment procedure for POAG. However, it does have limited effectiveness as an individual procedure, so the ideal clinical scenario might be to use it combined with cataract surgery,” he added.
Dr Rhee, associate professor, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, US, said that the basic concept of the Trabectome is to ablate and remove a strip of trabecular meshwork in order to re-establish access to the eye’s natural drainage pathway. He noted that targeting the trabecular meshwork makes perfect sense bearing in mind the pathophysiology of POAG.
“It has been known since the time of Chandler and Grant in 1958 that the cause of the elevated IOP that we see in POAG is at the level of the trabecular meshwork and it is not a problem of aqueous, hypersecretion or altered uveoscleral outflow. Traditional procedures such as trabeculectomy and tube shunt surgery both rely on creating a transscleral pathway by making a full thickness hole through the sclera, resulting in a direct communication between the anterior chamber and subconjunctival space to create a filtration bleb,” he said.
While targeting the trabecular meshwork is not a new concept, the difference with the Trabectome lies in its minimally invasive approach and reduced complication rate, said Dr Rhee. “We have some very good data from randomised controlled clinical trials concerning the complication rates with conventional trabeculectomy. The Collaborative Initial Glaucoma Treatment Study (CIGTS) and Tube Versus Trabeculectomy (TVT) Study reported intraoperative complications at a rate of about 10 per cent. During the perioperative period complications such as hypotony,
wound leak, flat anterior chamber, haemorrhage, hyphaema, and infection occur at a rate of between 50 per cent to 57 per cent in these two studies. In all, visually significant complications occurred at a rate of between 15 and 27 per cent,” he said.
Focusing on the Trabectome, Dr Rhee explained that it was developed by George Baerveldt MD at the University of California and received FDA approval in 2004. The handpiece of the device incorporates a variable power bipolar microsurgical pulse with simultaneous irrigation and aspiration, which allows for ablation and removal of the trabecular meshwork, unroofing Schlemm’s canal and exposing the natural drainage pathway of the eye to aqueous humour.
“What we are doing is ablating the tissue to create a direct communication between the anterior chamber and collecting channels. It is performed through a temporal clear corneal incision, and we ablate between 60 and 150 degrees of nasal trabecular meshwork,” he said.
Lowering IOP In terms of clinical performance, Dr Rhee said that the device has limited effectiveness at lowering IOP. “Don Minckler MD published his first series of 37 patients in 2005 and he reported a reduction in mean pressure from approximately 28 mmHg preoperatively down to about 16 mmHg at six months' follow-up,” he said.
A further study by Minckler et al. which looked at 738 patients treated with Trabectome only and 366 patients with combined Trabectome-phacoemulsification surgeries reported a decrease in IOP among Trabectome-only cases with or without medications of 40 per cent at 24 months and 32 per cent at 60 months. Failure, defined as additional glaucoma surgery, was reported in 100 of 738 Trabectome-only cases (14 per cent), which is a relatively low failure rate, noted Dr Rhee.
While the success rates reported in the study are impressive at first glance, Dr Rhee said that closer inspection of the data raises some important concerns. “In general when you are doing a clinical study you do not want to lose more than 10 per cent to 15 per cent of the sample per year. In this study, we see the Trabectome group of 738 patients reduced to 260 at six months, 102 at 12 months and just 46 at 24 months, so
the sample attrition is well beyond what we would expect from a usual study,” he said.
Another study published in January 2012 by Jea et al. comparing ab interno trabeculectomy with conventional trabeculectomy found a much lower success rate for Trabectome compared to conventional trabeculectomy. The trabeculectomy success rate was 85 per cent at one year and 76 per cent at two years, compared to 46 per cent at one year and 22 per cent at two years for the Trabectome.
Dr Rhee said that the findings did not invalidate the hypothesis of Chandler and Grant, that the trabecular meshwork is directly implicated in POAG.
“If we look at the initial one-month,
three-month, six-month data, the Trabectome success rate is excellent, so there is every reason to believe that the trabecular meshwork is the site of resistance. However, the reason the procedure is failing is probably due to wound healing issues,” he said.
Dr Rhee added that initial data from a study presented at ARVO in 2010 indicated that phacoemulsification in combination with Trabectome offered a similar IOP-lowering effect and decrease in anti-glaucoma medication use as phacoemulsification combined with trabeculectomy. The failure rate of both groups was also similar.
Douglas J Rhee – [email protected]
cont
act
LoWERING IoPTrabectome may work best in combined phacoemulsification proceduresby Dermot McGrath in Abu Dhabi
53
LASER…INNOVATION
MADE IN GERMANY
A.R.C. Laser GmbHBessemerstraße 14D-90411 NürnbergGermany
+49 (0) 911 217 79-0 +49 (0) 911 217 79 [email protected]
Your local distributor:
A.R
.C. L
aser
cer
tifie
s th
at th
e pr
oduc
t com
plie
s to
21
CFR
104
0.10
and
104
0.11
EN
134
85/ 2
003
- 93/
42 E
WG
A.R.C. Laser GmbHBessemerstraße 14D-90411 NürnbergGermany
+49 (0) 911 217 79-0 +49 (0) 911 217 79 [email protected]
Your local distributor:
A.R
.C. L
aser
cer
tifie
s th
at th
e pr
oduc
t com
plie
s to
21
CFR
104
0.10
and
104
0.11
EN
134
85/ 2
003
- 93/
42 E
WG
www.arclaser.de
This year you can expect a brand new range of lasers and ophthalmic products from A.R.C. Laser. Watch out for the stars.
PHACO
SLT
YAG
KTP
•5 magnification levels
•brilliant view
•single hand operation
•wide range of accessories
Its a PCL5 yearIts a PCL5 year
SLIT
LAMPS
2012-03_EUROTIMES_120x120.indd 2 04.06.2012 14:31:40
Update
GLAUCOMA
Our own clinical experience and the available studies suggest that the Trabectome is an elegant and safe anterior segment procedure for POAG
“
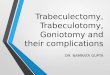
Douglas J Rhee MD Intraoperative and intraocular image of the Trabectome device after ablation of the trabecular meshwork
Cour
tesy
of D
ougl
as J
Rhe
e M
D
Recommended