Trabeculectomy, Trabeculotomy, Goniotomy and their
complications
Trabeculectomy, Trabeculotomy, Goniotomy and their
complicationsDR. NAMRATA GUPTA
Incisional Surgery Frequently used for chronic forms of glaucoma
in adults Filtering procedure External filtration:Full
thickness(Scheie) procedures: Thermal sclerostomy, sclerectomy,
Elliotts trephinationGuarded procedures: TrabeculectomyInternal
filtration:CyclodialysisTrabecular meshwork
disruption:Trabeculotomy ab externoGoniotomy
Open angle glaucoma-No internal flow block and IOP remains too
high despite medical therapy, surgery is needed to relieve outflow
block2
Trabeculectomy
IntroductionTrabeculectomy, a guarded filteration procedure
remains the gold standard for long lasting intraocular pressure
reduction in uncontrolled glaucomaPopularized by Cairns (1968)
Mechanism of actionCreation of a fistula at the limbus which
allows a direct communication between anterior chamber and
subconjunctival space bypassing the trabecular meshwork, schlemm
canal and collecting channels
Theories of mechanism
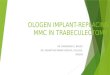
15432
1, Aqueous flow into cut ends of Schlemm canal (rare); 2,
cyclodialysis (if tissue is dissected posterior to scleral spur);
3, filtration through outlet channels in scleral flap; 4,
filtration through connective tissue substance of scleral flap; 5,
filtration around the margins of the scleral flap.6
Pre-operative evaluation
Indications Intraocular pressure too high to prevent future
glaucoma damage and functional visual lossDocumented progression of
glaucoma damage at current level of intraocular pressure with
treatmentPresumed rapid rate of progression of glaucoma damage
without interventionPoor compliance with medical therapy : cost ,
inconvenience, understanding of diseaseIntolerance to medical
therapy due to side effects
Assessment of filtration risk factorsThorough slit lamp
evaluation, gonioscopy, record review of past surgeryBest site for
filtration determined: PAS, IOL and haptic orientation, aberrant
vessels, wound dehiscence, limbal scarring, vitreous prolapseRisk
factors for filtration failure: African race, uveitis, aphakia,
neovascular glaucoma, prior failed filtration, prolonged
anti-glaucoma medicationOcular surface disease: ocular rosacea,
blepheritis
Prolonged anti-glaucoma-proliferation of lymphocytes and
fibroblasts9
Surgical Technique Perioperative preparations:Intravenous
sedation : pediatric, adults unable to co-operateLocal anesthesia:
Retro-bulbar injection, peribulbar injection, subtenon,
subconjunctival or topical anesthesiaPositioning to maximize
exposure to superior globe: protection by lid, no diplopia after
PI
Modified small incision trabeculectomy,
microtrabeculectomy10
Traction sutures
Superior rectus traction (or bridle) suture
Complications: subconjunctival hemorrhage, conjunctival defects,
scleral perforation postoperative ptosis
Globe rotated down and SR grasped with forcep thru conjunctiva
10-15 mm behind limbus11
Traction suturesClear Corneal traction sutures: A 7-0
polyglactin (vicryl) suture is passed through approx. th thickness
of superior peripheral cornea(4-5 mm width) 1mm form limbusMay
distort the cornea and anterior chamber during surgery
Conjunctival flapGeneral principles: Gentle handling-
buttonholing (antifibrotics)Removal of portion of Tenon capsule :
source of fibroblast (controversial)
Conjunctival flapTwo types of conjunctival flap:Limbal based
conjunctiva flap (LBCF) incision deep in fornix with base at
limbus
Fornix based conjunctival flap (FBCF) incision at limbus with
base at fornix
Limbal based versus fornix based flap
Anti-metabolite decisionAdjunctive antimetabolites inhibit the
natural healing response that may preclude successful filtration
surgeryStratified according to patient risk factors
5-FluorouracilPyrimidine analogue antimetaboliteInhibition of
thymidylate synthesis, blocks DNA synthesisInhibit fibroblastic
proliferationConcentration: Cellulose sponge soaked in 50mg/ml for
5 mins
Edges of conjunctival incision free of 5-fu17
Mitomycin CMore potent than 5-FUAntineoplastic antibiotic
isolated from Streptomyces caespitosusSelectively inhibits DNA
replication, mitosis and protein synthesis-inhibits proliferation
of fibroblast, suppresses vascular ingrowthConcentration: 0.2-0.5
mg/ml for 1-5 mins depending on magnitude of risk factors
Delivering the anti-fibrotic agentCellulose sponge 5 3 mm soaked
in antimetabolite is placed under dissected tenons capsule for 5
mins before paracentesis of AC followed by thorough irrigation with
BSS
Ring of steelCover largest area possible for more diffuse
noncystic bleb and prevent posterior limiting scar (ring of
steel)
Moorfields Eye Hospital (More Flow) intra-operative Single Dose
Anti- Scarring Regimen 2006 Low Risk Patients (Nothing or
intra-operative 5-FU 50mg/ml)No risk factorsTopical medications
(beta-blockers/pilocarpine)Afro-CaribeanYouth