Received 11/24/2018 Review began 12/03/2018 Review ended 01/01/2019 Published 02/24/2019
© Copyright 2019Burke et al. This is an open accessarticle distributed under the terms ofthe Creative Commons AttributionLicense CC-BY 3.0., which permitsunrestricted use, distribution, andreproduction in any medium, providedthe original author and source arecredited.
In Situ Cranioplasty for Renal Cell SkullMetastasis: Technical NoteJohn F. Burke , Vivek Sudhakar , Steve Braunstein , Michael McDermott
1. Neurosurgery, University of California - San Francisco, San Francisco, USA 2. Radiation Oncology,University of California - San Francisco, San Francisco, USA 3. Neurological Surgery, University ofCalifornia, San Francisco, USA
Corresponding author: John F. Burke, [email protected]
AbstractTreatment of a large, symptomatic skull metastasis requires surgical excision and in many casespostoperative radiation therapy. Immediate reconstruction of the skull for cerebral protectionusually involves cranioplasty with titanium mesh and/or methyl methacrylate. Preoperativesynthetic cranioplasty technology is yet to evolve sufficiently to allow computer-generatedprostheses to precisely fit a defined craniectomy defect created at the time of tumor removal.We document the techniques used for simultaneous craniectomy and composite cranioplasty inthe setting of a large occipital renal cell skull metastasis. Preoperative computed tomography(CT) and magnetic resonance (MR) imaging identified the pathological anatomy of an occipitalskull metastasis presenting as an exophytic scalp mass. Preoperative angiography andembolization was performed followed by craniectomy in the semi-sitting position andcomposite cranioplasty using titanium mesh and methyl methacrylate. A series of steps in thesurgical procedure are outlined to assist with safely and accurately performing the craniectomyand cranioplasty to guarantee the best surgical and cosmetic outcome. Postoperative CTimaging confirmed excellent contours of the cranioplasty. The method described herein allowsfor a single-step surgical procedure to excise a large skull metastasis and create a structurallysound and cosmetically acceptable composite cranioplasty. This method can also be used forthe excision and repair of other skull tumors or anomalies requiring excision.
Categories: NeurosurgeryKeywords: cranioplasty
IntroductionPatients with early cranioplasties have been reported to demonstrate improvements inneurological function. These improvements are posited to be due to restoration of normalcerebral spinal fluid (CSF) flow dynamics and a resolution of a phenomenon termed the“syndrome of the trephined” [1-3]. Currently, the existing skull defects are routinely repairedwith computer-generated cranioplasty implants. A variety of materials are used to constructthese implants, including methyl methacrylate, polyether ether ketone (PEEK) [4], and otherpolymers.
The excision of large, symptomatic skull lesions, such as primary or secondary skull neoplasms,often requires a simultaneous cranioplasty. However, excising a large, symptomatic skull lesionand creating a simultaneous cranioplasty with an appropriate shape and contour is problematicfor surgeons. It is difficult to repair a large skull defect immediately following the excision of apathological lesion. In particular, repairs are complicated by the need to maintain the tensileand compressive strength of the skull while also ensuring a cosmetic/symmetric result. This is
1 1 2 3
Open Access TechnicalReport DOI: 10.7759/cureus.4128
How to cite this articleBurke J F, Sudhakar V, Braunstein S, et al. (February 24, 2019) In Situ Cranioplasty for Renal Cell SkullMetastasis: Technical Note. Cureus 11(2): e4128. DOI 10.7759/cureus.4128

especially important in nonhair bearing scalp locations.
Bloch and McDermott previously described a so-called “in situ” cranioplasty for the excisionand reconstruction of cranial vault hyperostosing meningiomas [5]. The same technique isapplicable to other lesions of the skull such as metastatic tumors and fibrous dysplasias.Performing a simultaneous repair avoids the need for a second surgical procedure to implant acomputer-generated prosthesis after a period of risk exposure from a large skull defect.
We describe the technique of in situ cranioplasty used for the excision of a large occipital renalcell skull metastasis and point out the sequence of steps that may be used to ensure a safeexcision and structurally sound and cosmetically acceptable cranioplasty performed at the timeof tumor removal.
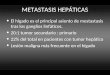
Technical ReportA 43-year-old man presented with a large occipital scalp mass that had been growing quicklyover the prior three months. His local oncologist had performed a body positron emissiontomography (PET) CT revealing a hypermetabolic kidney mass consistent with renal cellcarcinoma, as well as a large occipital skull mass. Figure 1 shows the preoperative MRI of theskull lesion in panels A and B. The patient was referred for surgical excision and cranioplastypreceded by angiography and embolization; preoperative angiogram is shown in Figure 1C.Image guided volumetric MRI images were obtained with fiducials for intra-operative imageguidance.
FIGURE 1: Preoperative imaging.A: Postcontrast T1 weighted coronal magnetic resonance (MR) image showing a calvarial-basedmetastatic lesion invading the calvarium over the left parietal-occipital region. B: Postcontrast T1weighted sagittal MR image showing the same lesion. C: Preoperative angiogram showed that thetumor had arterial supply from multiple branches of the bilateral superficial temporal, middlemeningeal, and occipital arteries as well as intracranially from the left anterior falcine artery.
The patient was positioned semi-sitting with the skull clamp positioned anteriorly andconnected to a table attachment over the body of the patient (Figure 2). Preoperative bubbleechocardiography had been done to confirm there was no open atrial septal defect. Precordialultrasound monitoring and central venous access was included to detect and treat anysignificant intraoperative venous air embolism.
2019 Burke et al. Cureus 11(2): e4128. DOI 10.7759/cureus.4128 2 of 6

FIGURE 2: Intraoperative photographs.Photographs show the tumor both before (A) and after (B) resection and in situ cranioplasty. Thetitanium mesh is seen attached to the 1.5 cm strip of native bone around the original bony tumorsite. The tumor was resected and the resulting bony defect was replaced with compositecranioplasty material.
Following registration of imaging to physical space, the margin of tumor-involved bone underthe scalp was outlined to assist with scalp incision planning. A bicoronal-parietal-occipitalincision was marked extending from the vertex down to behind both ears. The scalp wasopened, and the subgaleal plane was dissected using electrocautery for hemostasis. As thepericranium was removed from over the tumor-involved skull, bleeding was controlled withboth absorbable and nonabsorbable bone wax. The margin of the tumor in bone was thenoutlined on the skull and a separate margin of 1.5 cm of additional bone in a ring around this.The protruding skull with tumor was then drilled down using a 6 mm cutting burr. Enough bonewas removed to blend in with the contours of the surrounding skull and to recreate the occipitalcurvature when viewed in profile from either side. A large piece of titanium mesh was thenmolded and cut to the shape of the drilled down tumor-involved skull. The molded mesh wasthen placed on the back table.
Next the 6 mm cutting burr was used to drill a trough in the bone around the skull metastasisdown to a thin shell over the dura. Hemostasis was maintained using malleable absorbable bonewax. Once the circumference of the tumor had been drilled the remaining thin layer of bone atthe depth of the trough was removed with a 3 mm Kerrison after dissecting the dura away fromthe bone. The isolated central portion of the skull invaded by tumor, which was very adherentto the underlying dura, was removed in pieces using the footplate attachment of the drill andLeksell rongeurs. The surrounding 1.5 cm rim of normal skull was then removed in a singlecircular piece and the dura tacked up at the edge of the craniectomy in standard fashion.
As the tumor did not penetrate the dura, soft tissue in the epidural space was scraped off usingthe Penfield #1 and the dura was coagulated throughout. The previously molded mesh was thentaken from the side table and was screwed into the surrounding circular bone flap using 4 mmscrews. The inner circumference of the circular craniectomy was traced with a surgical markingpen on a paper template. We then used this template to estimate the size of themethyl methacrylate piece for the composite construct. The plastic was mixed and, after aperiod of time to allow for setting of the polymer, it was then cut to the approximate shape ofthe paper template. Then, the cut polymer was placed into the inner table defect and securedonto the interstices of the outer table mesh. Excess plastic was scrapped off the outer table sideand the material was allowed to harden off the field where the exothermic event would causeno tissue damage.
2019 Burke et al. Cureus 11(2): e4128. DOI 10.7759/cureus.4128 3 of 6

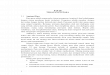
The composite cranioplasty was then secured to the surrounding skull with titanium plates andscrews, irrigated with 3% betadine solution, then saline, followed by the application ofVancomycin powder. A 1/8” hemovac drain was placed in the subgaleal space and the scalpclosed in the standard fashion. The entire procedure is summarized in Figure 3.
FIGURE 3: Illustrations of the in situ cranioplasty method.Top panel: the bone is divided into three sections: (1) tumor-involved bone; (2) native bone in a rim1-2 cm around the tumor-involved bone (1.5 cm was used in the case report). This bone will beremoved for the cranioplasty; (3) native bone not involved with the cranioplasty. Bottom panel: thetitanium mesh is fit to the tumor-involved bone, which is subsequently resected.
Illustrations by Ken Probst
The patient’s postoperative course was uncomplicated. Postoperative MR and CT imagingrevealed an appropriate contour of the cranioplasty and gross total tumor excision (Figure 4).The patient was recommended for external beam radiotherapy. Upon discharge he has beendoing well and has had no complaints regarding his excision site, no wound infection, and no
2019 Burke et al. Cureus 11(2): e4128. DOI 10.7759/cureus.4128 4 of 6

issues with the healing process. At one-year follow up, he was doing well and surveillanceMR imaging revealed no tumor recurrence.
FIGURE 4: Postoperative imaging.A: Sagittal and B: coronal postcontrast T1 weighted postoperative MR image showing gross totalresection of the metastatic lesion. C: bone weighted postoperative CT scan showing thecranioplasty site. D: The different areas of bone involved in the cranioplasty are shown color codedbased on the image in C.
DiscussionMetastatic lesions to the central nervous system can either be resected, irradiated, or treatedwith both surgery and radiation. Increasing data have shown that, for larger lesions, surgeryand radiation offer the best source control for metastatic lesions. When lesions are completelyintra-axial, surgical options can be more straightforward and usually involve a typicalcraniotomy for tumor excision, much like a primary glioma. However, lesions that primarilyinvolve the calvarium also need to be resected, but doing so is complicated by the fact that thebony defect has to be reconstructed. Indeed, the alternative to reconstructing the bony defect isto leave the patient with a craniectomy which places the patient at risk for trauma to the region,as well as wound breakdown over exposed parenchyma given that these regions will beirradiated in the near future. Thus, whenever possible, it is preferable to perform cranioplastyfor calvarial-based lesions as soon as possible after surgery. Here, we argue for in situcranioplasty.
Given that an in situ cranioplasty is done at the time of tumor resection, it is generally notpossible to perform a computer-aided regeneration of the synthetic bone flap. Thus, it isnecessary to use techniques to reconstruct the bone flap at the time of surgery, which we
2019 Burke et al. Cureus 11(2): e4128. DOI 10.7759/cureus.4128 5 of 6

describe above. In addition to being a fast method to place the bone flap, the insitu cranioplasty is inexpensive and very durable: the mesh and methyl methacrylate act assteel rebar and cement, providing both compressive and tensile strength to the bone flap.These methods were initially described by Bloch et al. for hyperostosing meningiomas, but areextended in this case to metastatic lesions of the calvarium [5].
ConclusionsThe above in situ cranioplasty technique provides a durable and lasting repair of calvarialmetastatic lesions, and offers better cosmesis than a free-handed technique.
Additional InformationDisclosuresHuman subjects: Consent was obtained by all participants in this study. Animal subjects: Allauthors have confirmed that this study did not involve animal subjects or tissue. Conflicts ofinterest: In compliance with the ICMJE uniform disclosure form, all authors declare thefollowing: Payment/services info: All authors have declared that no financial support wasreceived from any organization for the submitted work. Financial relationships: All authorshave declared that they have no financial relationships at present or within the previous threeyears with any organizations that might have an interest in the submitted work. Otherrelationships: All authors have declared that there are no other relationships or activities thatcould appear to have influenced the submitted work.
References1. Waziri A, Fusco D, Mayer SA, et al.: Postoperative hydrocephalus in patients undergoing
decompressive hemicraniectomy for ischemic or hemorrhagic stroke. Neurosurgery. 2007,61:489-494. 10.1227/01.NEU.0000290894.85072.37
2. Winkler PA, Stummer W, Linke R, et al.: Influence of cranioplasty on postural blood flowregulation, cerebrovascular reserve capacity, and cerebral glucose metabolism. J Neurosurg.2000, 93:53-61. 10.3171/jns.2000.93.1.0053
3. Joseph V, Reilly P: Syndrome of the trephined. J Neurosurg. 2009, 111:650-652.10.3171/2009.3.JNS0984
4. Punchak M, Chung LK, Lagman C, et al.: Outcomes following polyetheretherketone (PEEK)cranioplasty: systematic review and meta-analysis. J Clin Neurosci. 2017, 41:30-35.10.1016/j.jocn.2017.03.028
5. Bloch O, McDermott MW: In situ cranioplasty for hyperostosing meningiomas of the cranialvault. Can J Neurol Sci. 2011, 38:59-64.
2019 Burke et al. Cureus 11(2): e4128. DOI 10.7759/cureus.4128 6 of 6
Recommended