Nasopharyngeal & Oropharyngeal Cancer Update
Richard E. Braun, MDChief Medical Director and Vice President,SCOR Global Life Americas

Oral & Nasopharyngeal Cancer
2
Review anatomy and tissues of the head & neck Nasopharyngeal & Oropharyngeal Cancer Etiology Epidemiology Diagnosis Natural History Treatment Prognosis

Oral Cancer
3
~ 90-95% Squamous Cell Carcinoma~ 5% Lymphoid origin< 1% Sarcoma

Oral Cancer
4
Estimated 263,000 cases per year, worldwideResulting in 127,000 deaths

Oral Cancer
Risk Factors for Head & Neck Cancers Smoking (cigarettes, cigars, pipe, ??marijuana) Cigarette smokers have 5 to 25 times the risk of
developing oral cancer Appears to be a dose-response relationship Chewing tobacco & “Snuff” also increase risk Other ingredients (betel nut) may increase risk
even more Evidence that second hand smoke in the home
also increases risk, especially in women.
5

Oral Cancer – Risk Factors/Etiology
Alcohol Dose dependent 5-6 fold risk with >50 gms/day (3-4 drinks)
versus <10 gms/day Tobacco smoking and Alcohol appear to have a
synergistic effect to increase the risk May also be a connection to genetic
polymorphisms of alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH)
Betel Nut chewing also implicated alone and in synergy with alcohol and tobacco (India & Asia)
6

Oral Cancer – Risk Factors/Etiology
Viral infections Epstein-Barr virus (EBV) – EBV DNA and gene
expression detected in precursor and tumor cells Human Papilloma virus (HPV) – primarily Type 16,
often occurs at the base of the tongue or tonsils, typically seen in young men who do not use alcohol or tobacco, may be causing “epidemic”
Human Immunodeficiency Virus (HIV) – 2 to 3 fold increase in SCC of the head and neck
Herpes Simplex Virus (HSV) – The association is weaker, but has converted cells to malignant in vitro
7

Oral Cancer – Risk Factors/Etiology
Radiation to the head and neck linked to squamous cell tumors, salivary tumors and sarcomas
Diet – Protective effect of fruits and vegetables. Possible increased risk of preserved meats containing added nitrites
Occupational Exposure – asbestos, pesticides, formaldehyde, polycyclic aromatic hydrocarbons, napthalene, perchloroethylene, ethanol, sulfuric acid mist, and Agent Orange have all been implicated
Genetic Factors – include DNA repair defects and variations in pathways that contribute to carcinogenesis
Others include poor dental hygiene and periodontal disease
8

Nasopharyngeal Cancer - Etiology
Diet may play a larger role in endemic areas Salt cured foods release nitrosamines when cooked, which
can coat the mucosa Tradition of weaning babies on salted fish Fermented foods high in nitrosamines Chinese medicinal herbs may activate or promote EBV Rancid butter and sheep’s fat contain butyric acid (Tunisia,
Algeria & Morocco) EBV Heredity – one study showed an increase of 7 fold when a 1st
degree relative was affected Smoking, Alcohol, and HPV in Western cultures HPV – more often an extension of disease from the oropharynx
9

Oropharyngeal Cancer - Epidemiology 135,000 deaths worldwide, up from 84,000 in 1990
Age Standardized death rate per 100,000 in 2004
10Source: World Health Organization

Nasopharyngeal Cancer - Epidemiology
Males are affected predominately Countries where lip & oral caity cancers are the most common type
11

Lip & Oral Cavity – Incidence rates

US Incidence trends
13https://seer.cancer.gov/statfacts/html/common.html

Incidence Trends Oropharynx Cancer - US
14Evolution of the Oropharynx Cancer Epidemic in the United States: Moderation of Increasing Incidence in Younger Individuals and Shift in the Burden to Older Individuals, J Clin Oncol 37, 2019.

Projected Trends Oropharynx Cancer – US Men
15

Incidence Trends Oropharynx Cancer - US
16

Oral cavity and Pharynx Cancer
17https://seer.cancer.gov/statfacts/html/oralcav.html

Oral Cancer
18
Median age at diagnosis – 62Rate of new cases 11 per 100,000
http://seer.cancer.gov/statfacts/html/oralcav.html

Lip Cancer
19https://seer.cancer.gov/statfacts/html/lip.html

Tongue Cancer
20https://seer.cancer.gov/statfacts/html/tongue.html

Oral Cancer - Diagnosis Leukoplakia presents as white patches or plaques on the lining of the
mouth (mucosa) It can be a benign, reactive process It is hyperplasia of the epithelial cells which can lead to dysplasia and
eventually carcinoma Progresses in 1 to 20% of lesions within 10 years More prone to progress in “thin” skin areas Common in smokeless tobacco users Indurated areas should be biopsied
Oral proliferative verrucous leukoplakia Rare & aggressive, more frequent in older women Multifocal, develop wart-like exophytic lesions 60% progress to SCC within 7 years Recurrence rate of 90% 10 year mortality rate 30%
Erythroplakia – red patches, associated with Ca in situ or invasive up to 40%
21

Oral Cancer
22http://seer.cancer.gov/statfacts/html/oralcav.html
While recognized that examination of the mouth is important, less than 1/5 of physicians surveyed routinely did such exams.
Almost 4/5ths of physicians did not correctly diagnoses a picture of early Squamous Cell Carcinoma (SCC) of the mouth
SCC of the mouth can present as ulcers or masses Persistent papules, ulcers, erosions, or plaques should be biopsied Nasopharyngeal (90%) and tongue (up to 66%) cancers often present as
enlarged nodes in the neck. Oral cancers can present with pain. If it is growing, enlarging, changing - Biopsy

Oral Cancer
23
Benign oral lesions Apthous Ulcers (heal in 10-14
days without scarring)Variety of viral infections
Herpes Simplex
Coxsackie
Varicella

Oral Cancer
24
More Benign lesions
Mucoceles
Amalgam Tattoo
Torus palatinus

Oral Cancer Squamous cell cancer of the lip (~ 35% of oral cavity cancer)
Lower lip - Squamous Cell is more common than basal cell Tumor invasion correlates with metastatic spread to regional lymph
nodes Upper lip – exhibits a worse prognosis, they grow more quickly and
metastasize sooner Floor of the Mouth (~20%)
Tend to invade locally Occult node metastasis in 21% (Stage I) and 26% (Stage II)
Oral tongue (~ 20%) Risk of lymph node involvement is proportional to depth of invasion
Retromolar Trigone and lower alveolar ridge (~ 4%) High risk of bony extension and/or occult lymph node metastasis
Upper alveolar ridge and hard palate (4%) Usually have to resect bone to get adequate margins
Buccal Mucosa (1%) & Soft palate (15%) High local recurrence rates, often require surgery and radiotherapy (RT)
25

Head and Neck carcinoma Nasopharyngeal Most frequent complaint is a neck mass due to
regional lymph node involvement (90%) May involve surrounding structures leading to hearing
loss, tinnitus, nasal obstruction or pain – could also impair Cranial nerves II to VI
Sinus tumors present with bleeding and nasal obstruction Oropharyngeal Tumors can present with
snoring/obstructive sleep apnea, dysphagia or pain with swallowing, and/or a neck mass
Hypopharyngeal tumors can present with referred pain to the ear, weight loss, hemoptysis, difficulty swallowing and neck mass as they tend to present later in the course of the disease
26

Nasopharyngeal Cancer (NPC) - Diagnosis
In endemic areas screening is being investigated, often with a family history of NPC Rise in antibodies to viral capsid antigen (VCA) of the Epstein-
Barr virus (EBV) and to early antigen (EA) IgA typical of NPC May also see elevated levels of circulating EBV DNA (no
consensus on cutoff, 1500 and 4000 have been used) Another strategy is screening with VCA/IgA and confirming
elevations with EBV DNA by polymerase chain reaction (PCR), shown to be 99% sensitive in one study.
Once the diagnosis is made, the work-up should include MRI of the head and neck, Chest x-ray, CBC & SMA, and complete nasopharyngoscopy. If at risk for metastasis should add CT of the chest and upper abdomen and bone or PET scan.
27

Oral & Nasopharyngeal Cancer
28
Dysplasia
Oncology Letters, July 2014, Volume 8:Issue 1;PP 7-11.
Well differentiated SCC >75% keratinization
Moderately differentiated SCC Poorly differentiated SCC
25-75%keratin
<25%keratin

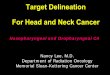
Axial T1-weighted MR image postcontrast of the nasopharynx of a patient with proved NPC (group 1) undergoing staging with a small cancer confined to the left side of the nasopharynx
(arrows) (stage T1).
King A et al. AJNR Am J Neuroradiol 2006;27:1288-1291

HPV Testing
Prevalence of oral HPV in the population age 14-69 was 6.9%, HPV 16, 18, 6, or 11 was 1.6% (those reporting HPV vaccination, it was .11%)
Oropharyngeal (OP) squamous cell carcinomas should be tested for HPV
1990s ~50% of OP cancers related to HPV, recently 70-80% have HPV
Base of the tongue and tonsils are the most common sites Immunohistochemical surrogate marker is p16
Threshold of > 70% staining of at least moderate to strong intensity Polymerase Chain Reaction (PCR) for HPV when discordant or
borderline Positive p16 expression has a better prognosis
30

Oral Cancer Staging
Stage Local (T) Nodes Distant Mets
0 Insitu 0 0I < 2 cm with DOI < 5 mm 0 0II < 2 cm and DOI 5.1-10 mm or
2.1 -4 cm with DOI up to 10 mm0 0
III 2.1 -4 cm with DOI > 10 mm or> 4 cm with DOI < 10 mm
0 0
III T 1, 2,or 3 above N1(ipsilat small) 0IVA Locally advanced (> 10 mm) or
Invades adjacent structuresN0, N1, or N2 0
IVB Any local N3(ENE+, mult) 0IVC Any local Any N M1
31
DOI – Depth of Invasion ENE – Extranodal extension
AJCC UICC 8th edition

Primary Tumor StagingNasopharyngeal Cancer
32AJCC Cancer Staging Manual, Seventh Edition (2010)
Stage Local Nodes MetsTis In situ 0 0I Confined or minimal extension 0 0II Extension to parapharyngeal or
soft tissues0 or N1 (small, local nodes)
0
II Confined or minimal extension N2 (small, bilat, local)
0
III Infiltrating Bone or sinuses or localized with nodes +
N0, N1, N2 0
IVA Intracranial extension or extensive soft tissue
N0, N1-3, 3 (cervical nodes, large)
0
IVB any any M1

Oropharyngeal clinical cancer staging
Stage Local (T) Nodes (N) Distant Mets
0 In situ 0 0I < 2 cm 0 0II 2.1-4 cm 0 0III 4 cm or extends to epiglottis or smaller
With N10 or 1 0
IVA Moderately advanced local disease 0, 1, or 2 0IVB Any with N3 or Very advanced local 0-3 0IVC Any Any M1
33AJCC Cancer Staging Manual, Seventh Edition (2010)
HPV Negative
HPV + very similar, no T for locally very advanced and Stage IV is single category with distal Mets

Head & Neck Cancer – Lymph node regions of the neck
34
Submental
SubmandibularUpper Jugular
Middle Jugular
Lower Jugular
Anterior compartmentPosteriortriangle VII
Superior Mediastinal
AJCC Staging Manual 7th & 8th (2017) edition

Oropharyngeal Cancer - US
35http://seer.cancer.gov/statfacts/html/oralcav.html

Head and Neck Cancer - Treatment Stage I or II Generally either primary surgery or radiation therapy
(RT) 5-year survival generally 70-90%
Stage III & IV (Locoregionally advanced disease) Surgery, RT, and/or chemotherapy Cervical lymph node involvement – definitive RT or
chemoradiotherapy Nasopharyngeal
Surgery less common, RT is the mainstay, with chemotherapy for stage II up
Squamous cell of nodes with unknown Primary Base of the tongue primary in 50-72% Definitive RT can be pursued
36

Head & Neck Squamous Cell Carcinoma Post treatment Follow-up and Surveillance (Uncertain if it alters outcome)
Imaging at 12 weeks to document regression Every 1- 3 months the 1st year; every 2-4 months the second year; every
4-6 months in 3-5 years; yearly thereafter Imaging is case specific. Positron Emission Tomography (PET),
Computed Tomography (CT) , and Magnetic Resonance Imaging (MRI) are all options.
80-90% of recurrences occur in the first 4 years Risk of a second primary is higher than recurrence risk after 3 years and
remains elevated for at least 10 years Continued smoking and alcohol use increase the risk Lung Cancer is not uncommon as a second Cancer with a cumulative
incidence or ~13% at 20 years Other complications
Post radiation accelerated carotid atherosclerosis Obstructive sleep apnea may develop after treatment
37

US Mortality Trends
38https://seer.cancer.gov/statfacts/html/common.html

Oral Cavity and Pharynx Cancer
39http://seer.cancer.gov/statfacts/html/oralcav.html

Survival based on HPV (p16)
40
HPV status Stage I II III IVA IVBHPV + 88 82 84 81 60HPV - 76 68 53 45 34
5 year survival oropharyngeal cancer
Lancet Oncol. 2016;17(4):440.
Treatment for HPV + or – remains the same at presentTrials are underway to test deintensification of treatment

Nasopharyngeal Carcinoma Survival
41

ORAL CANCER – Disease Specific Survival (UK)
42
By extra capsular spread By Lymph Node Involvement
Oral Oncology (2009) 45, 201– 211

ORAL CANCER - Survival
43Oral Oncology (2009) 45, 201– 211
DSS – Disease specific survival; OS – Overall survival

ORAL CANCER
44
Oral Oncology (2009) 45, 201– 211
“Smoking cessation in particular improves prognostic outcomes reducing the risk of secondary disease by ∼2–3-fold.” Oral Onc 46, Issue 6, June 2010, Pages 407–410

Oral and Pharyngeal Cancer
45https://seer.cancer/explorer
Oral Cavity and Pharynx Cancer

Oral and pharyngeal cancer
46https://seer.cancer/explorer

US Survival Oral and Pharynx Cancer
47https://seer.cancer.gov/statfacts/html/oralcav.html

Oral Cancer
48AJCC Staging Manual 8th (2017) edition

Oral Cancer
49AJCC Staging Manual 8th (2017) edition

Lip Cancer
50

Tongue Cancer
51https://seer.cancer.gov/statfacts/html/tongue.html
Overall 5-year survival 66.4%

Nasopharyngeal Cancer
52
Stage Percent of patients Five-year OS, percent I 7 90II 41 84III 25 75
IVA-B 28 58
OS: overall survival.Data from: Lee, AW, Sze, WM, Au, JS, et al. Treatment results for nasopharyngeal carcinoma in the modern era: The Hong Kong experience. Int J Radiat Oncol BiolPhys 2005; 61:1107

Nasopharyngeal Cancer
53Journal of the National Cancer Institute, Vol. 97, No. 7, April 6, 2005
Survival all patients Survival Stage 3 & 4

Comparison of overall survival curves in the two treatment arms. Nasopharyngeal carcinoma
Daniel T.T. Chua et al. JCO 2005;23:1118-1124
©2005 by American Society of Clinical Oncology

Questions??
If you think of some later:
Richard Braun, MD
Or call (913) 901-4749
55
Recommended