Outcome of Embolized Outcome of Embolized Vascular Metastatic Spinal Vascular Metastatic Spinal
Tumours causing Cord Tumours causing Cord CompressionCompression
N A Quraishi, FRCS (Tr & Orth), LLMS Purushothamdas, FRCS (Tr & Orth)
R Lenthall , FRCRM P Grevitt , FRCS (Tr & Orth)
Eurospine, Milan Eurospine, Milan 20112011
Centre for Spinal Studies & Surgery Department of RadiologyQueens Medical Centre, Nottingham

BackgroundBackground Vascular metastatic spinal tumours with cord compression have a high Vascular metastatic spinal tumours with cord compression have a high
risk of morbidity & mortalityrisk of morbidity & mortality
Role of pre-operative embolisation is well recognisedRole of pre-operative embolisation is well recognised
Multiple factors (size of tumour, extent of surgical intervention, degree of Multiple factors (size of tumour, extent of surgical intervention, degree of vascularity and extent of embolisation) influence the blood loss and vascularity and extent of embolisation) influence the blood loss and clinical outcomeclinical outcome
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk
Study the effect of embolisation of vascular Study the effect of embolisation of vascular metastatic tumours causing spinal cord metastatic tumours causing spinal cord compression and their outcomecompression and their outcome
AimAim

Patient and MethodsPatient and Methods
Retrospective cohort studyRetrospective cohort study Period: January 2004 to September Period: January 2004 to September
20102010 23 patients (14 males : 19 females)23 patients (14 males : 19 females) Average Age 59.2 years (24-78)Average Age 59.2 years (24-78) Follow-up: 7.3 months (3-23.3)Follow-up: 7.3 months (3-23.3) Primary diagnosis: Primary diagnosis:
Renal cell carcinomaRenal cell carcinoma : 21: 21 ParagangliomaParaganglioma : 1: 1 CarcinoidCarcinoid : 1: 1
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk

Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk
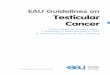
15%
15%
66%
4%
PainNeurologyBothAsymptomatic
Clinical presentationClinical presentation
Most patients presented with both Most patients presented with both pain and deteriorating neurologypain and deteriorating neurology

Operative DetailsOperative Details Ave. blood lossAve. blood loss : 2211 (400-10,000) mls: 2211 (400-10,000) mls Ave. operating timeAve. operating time : 291 (90-840)mins: 291 (90-840)mins Ave. blood transfusionAve. blood transfusion : 3.5 (max.19)units: 3.5 (max.19)units Ave. pre-operative Hb Ave. pre-operative Hb : 12.6 (9.5-16 ) g/dl: 12.6 (9.5-16 ) g/dl Ave. post-operative Hb Ave. post-operative Hb : 9.6 (6.9-14.6) g/dl: 9.6 (6.9-14.6) g/dl
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk
Type of surgery
0
2
4
6
8
10
12
14
16
Corpectomy Decom/stabil Debulking
No
. of
pat
ien
ts

Embolisation details Embolisation details (performed by senior interventional (performed by senior interventional
radiologist)radiologist) Endovascular, transarterial; combination of liquid & particulate Endovascular, transarterial; combination of liquid & particulate
agentsagents
Angiography grade: Angiography grade: Grade 0Grade 0 : Normal vascularisation: Normal vascularisation Grade IGrade I : Homogenous blush (normal feeding arteries): Homogenous blush (normal feeding arteries) Grade IIGrade II : Hypervascularisation (dilated feeding : Hypervascularisation (dilated feeding
arteries)arteries) Grade IIIGrade III : Arterio-venous fistula: Arterio-venous fistula
Embolisation grade: Embolisation grade: Not embolisedNot embolised <50% embolisation<50% embolisation 51-90% embolisation51-90% embolisation 90-100% embolisation90-100% embolisation
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk

EmbolisationEmbolisation
Grade 0 (Normal vascularisation) 0 (0%)
Grade I (Homogenous blush) 1 (4.4%)
Grade II (Hypervascular) 11 (47.8%)
Grade III (AV fistula) 10 (43.5%)
Angiography grade
0
2
4
6
8
10
12
Grade 0 (Normalvascularisation)
Grade I (Homogenousblush)
Grade II (Hypervascular) Grade III (AV fistula)
No
. o
f p
atie
nts
Embolisation Grade
0
2
4
6
8
10
12
14
16
None <50% 51-90% 91-100%
No
. o
f p
atie
nts
None 4 (17.4%)
<50% 3 (13.1%)
51-90% 4 (17.4%)
91-100% 14(60.9%)
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk

Neurological change by Neurological change by Frankel gradesFrankel grades
Change of Frankel Grade
0
2
4
6
8
10
12
No change 1 + 2 + 1 - 2 -
No
. o
f p
atie
nts
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk
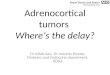
Neurological status
0
2
4
6
8
10
12
14
A B C D E
Frankel Grade
No
. of
pa
tie
nts
Pre-op
Post-op

Neurological change by Neurological change by Frankel GridFrankel Grid
AAAA00 ABAB00 ACAC00 ADAD00 AEAE00
BABA00 BBBB00 BCBC00 BDBD00 BEBE00
CACA00 CBCB00 CCCC55 CDCD11 CECE11
DADA00 DBDB00 DCDC22 DDDD55 DEDE55
EAEA00 EBEB00 ECEC11 EDED22 EEEE11
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk

Timing of embolisation to surgery
Immediate
(n = 10)24 hours
(n=10) p value
Blood loss (mls) 1537.5 2058.3 p = 0.49
Op time (minutes) 261 301 p =0.44
Transfusion (units) 2.6 2.9 p = 0.77
Survival (months) 16.1 16.5 p = 0.97
Extent of embolisation
>90%(n = 14)
<90%(n=9) p value
Blood loss (mls) 1902.5 2588.9 p = 0.54
Op time (minutes) 236 370 p =0.12
Transfusion (units) 2.6 4.6 p = 0.86
Survival (months) 17.1 14.5 p = 0.71

Complications 9/23, 39.1%Complications 9/23, 39.1%((major: 2/23,8.7%major: 2/23,8.7% ; minor: 7/23, ; minor: 7/23,
30.4%)30.4%)No. of No. of
PatientPatientss
Wound infectionWound infection 11
Urinary retentionUrinary retention 22
Chest infectionChest infection 22
Metal ware failureMetal ware failure 22
SepticaemiaSepticaemia 11
PneumothoraxPneumothorax 11
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk

ConclusionsConclusions Blood loss remains a major concern in vascular Blood loss remains a major concern in vascular
metastatic spinal tumours with cord metastatic spinal tumours with cord compressioncompression
No statistical significance is observed in amount No statistical significance is observed in amount of blood loss, operation time, blood transfusion of blood loss, operation time, blood transfusion and survival in terms of time of surgery since and survival in terms of time of surgery since embolisation and also extent of embolisationembolisation and also extent of embolisation
Higher complication rate is observed in such Higher complication rate is observed in such tumourstumours
Centre for Spinal Studies & Surgery, Nottingham www.nottinghamspine.co.uk
Financial Disclosure:Financial Disclosure:None of the authors have None of the authors have received from any commercial entity any payments or any pecuniary, in kind, or other professional or personal benefits including stock, honoraria, or royalties (collectively, “Benefits”) or any commitment or agreement to provide such Benefits
Recommended