A biomechanical assessment of a distally-fixed lateral extra-articular
augmentation procedure in the treatment of anterolateral rotational laxity of the
knee
Devitt BM1*, Lord BR2*, Williams A3, Amis AA2,4, and Feller JA1
1 OrthoSport Victoria, Epworth Healthcare, Melbourne, Australia
2 The Biomechanics Group, Department of Mechanical Engineering, Imperial College
London, London, SW7 2AZ, United Kingdom
3 Fortius Clinic, London, United Kingdom
4 Musculoskeletal Surgery Group, Imperial College London School of Medicine,
London, United Kingdom.
* The following authors are co-first-named authors
Corresponding author: Brian M Devitt
Email: [email protected]
Twitter feed: @OSVResearchUnit
Address: OrthoSport Victoria, 89 Bridge Road, Richmond, VIC 3121, Australia
Telephone: +61390385200
Fax: +61390385200
Primary Affiliation:
This investigation was performed at Department of Mechanical Engineering, Imperial
College London, London, SW7 2AZ, United Kingdom.
Acknowledgements:
1 of 24
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26

Mr BR Lord was supported by a grant from the North Hampshire Hospital
Orthopaedic Research Fund. The robotic testing system was provided by the
Imperial College London Centre of Excellence in Biomedical Engineering in
Osteoarthritis, funded by the Wellcome Trust and the EPSRC. We thank Dr H El-
Daou for writing the robot control software and running the robot, Dr JM Stephen for
help in the laboratory, and Dr KK Athwal for the statistical analysis.
2 of 24
27
28
29
30
31
32
33

A biomechanical assessment of a distally-fixed lateral extra-articular
augmentation procedure in the treatment of anterolateral rotational laxity of the
knee
3 of 24
34
35
36
37

Abstract:
A variety of lateral extra-articular tenodesis (LEAT) procedures have been described
and most rely upon passing a strip of the iliotibial band (ITB) under the Fibular
(lateral) collateral ligament (FLCL) and fixing it proximally to the femur. One of the
concerns is the potential to increase lateral compartment constraint. The Ellison
procedure is a distally-fixed lateral extra-articular augmentation procedure with no
proximal fixation of the ITB. It has the potential advantages of maintaining a dynamic
element of control of knee rotation and avoiding the possibility of over-constraint.
Purpose:
To assess the ability of a distally-fixed lateral extra-articular augmentation procedure
(modified Ellison) to restore native knee kinematics following complete sectioning of
the anterolateral capsule (ALC). A secondary aim was to assess what effect closure
of the ITB defect would have on knee kinematics.
Hypothesis:
The modified Ellison procedure would restore native knee kinematics following
sectioning of the ALC, and closure of the ITB defect would decrease rotational laxity
of the knee.
Study design: Controlled laboratory study
Methods:
Twelve fresh frozen cadaveric knees were tested in a 6 degrees of freedom robotic
system through 0-90 of knee flexion to assess anteroposterior, internal (IR) and
external rotation (ER) laxities. The simulated pivot-shift (SPS) was performed at 0,
15, 30, and 45 of flexion. Kinematic testing was performed in the intact knee, ALC-
injured knee, and following the modified Ellison procedure, with and without closure
4 of 24
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65

of the ITB defect. A novel pulley system was used to load the ITB at 20N for all
testing states. Statistical analysis used repeated-measures analyses of variance and
paired t tests with Bonferroni adjustments.
Results:
Sectioning of the ALC significantly increased anterior drawer and IR during isolated
displacement and with the SPS (P<0.05). Analysis of both isolated and coupled IR, at
0° of knee flexion or greater, revealed that the modified Ellison reduced this
anterolateral rotatory laxity significantly (P<0.05). During isolated IR testing, IR was
reduced close to the intact state with the modified Ellison procedure, except at 30 of
knee flexion when it was slightly below the intact knee (overconstraint).
Measurement of IR during the SPS revealed that IR with the closed modified Ellison
was below that of the intact state at 15° and 30° of flexion. No significant differences
in knee kinematics were seen between the ‘ITB-defect open’ and ‘ITB-defect closed’
states.
Conclusion:
A distally-fixed lateral extra-articular augmentation procedure (modified Ellison) can
reduce anterolateral rotatory laxity of the knee and restore knee kinematics close to
the intact state. Closing the ITB defect did not affect knee kinematics, compared to
leaving it open.
Clinical Relevance:
A distally-fixed lateral extra-articular augmentation procedure (modified Ellison) is
effective in reducing anterolateral laxity of the ALC-injured knee and restores
kinematics close to the intact state. Closure of the ITB defect has no effect on knee
kinematics.
5 of 24
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93

Key terms: Extra-articular tenodesis, Ellison, Anterolateral Rotatory Instability, knee
kinematics
What is known about the subject:
The vast majority of biomechanical studies to date have focused on proximally-fixed
LEAT and no biomechanical studies have analysed the efficacy of a distally-fixed
lateral augmentation procedure to control anterolateral rotatory laxity (ALRL) of the
knee.
What this study adds to existing knowledge:
This study uses a novel loading of the ITB in a robotic testing system, designed to
replicated normal physiological loads in the knee during simulated clinical
manoeuvres. In doing so, the authors have tested a distally-based lateral
augmentation procedure (modified Ellison) and demonstrated that it can reduce
ALRL and restore the knee kinematics close to the intact state. The study has also
shown that closure of the ITB defect has no effect on knee kinematics, which is a
new finding in the literature.
6 of 24
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115

Introduction
Anterior cruciate ligament (ACL) rupture typically occurs due to sudden axial loading
of the knee in conjunction with a coupled valgus and rotational moment about the
tibia27, 28, 36. The ACL is not the only structure damaged during this mechanism of
injury and studies have shown that the anterolateral complex of the knee is also
commonly involved5, 15, 34, 45. The anterolateral complex has been reported to consist
of the iliotibial band (ITB) with its superficial, middle, deep, and capsulo-osseous
layers as well as the anterolateral joint capsule (ALC)17. Among these structures,
some authors have identified a capsulo-osseous band: the anterolateral ligament
(ALL)6,9. Biomechanical studies have established that the anterolateral complex plays
a role as a secondary stabilizer to control anterolateral rotational laxity 13, 19, 24, 38.
Indeed, it has been suggested that failure to address the anterolateral injury at the
time of ACL reconstruction may increase the risk of graft failure due to persistent
anterolateral rotational laxity 1, 4, 19, 24, 37 38, 42.
Surgeons have long recognised that lateral extra-articular augmentation procedures
are an effective method to control rotation of the knee 10, 29, 33. The concept of
combining a lateral extra-articular augmentation with an intra-articular reconstruction
for the treatment of ACL injury emerged with a view to decrease the failure rate of
either technique carried out in isolation. The approach became popular in the 1980s
and was adopted by a number of surgeons using a variety of extra-articular
augmentation procedures, all non-anatomical in nature.10, 22, 29-31 However, following
recent reports describing the anterolateral ligament of the knee, anatomic
anterolateral reconstructions have also been reported41, 42.
The majority of these lateral extra-articular augmentation procedures are based on a
proximally-fixed construct, typically using a strip of ITB, which remains attached to its
7 of 24
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143

insertion at or near to Gerdy’s tubercle40. The free proximal end passes either deep
or superficial to the lateral collateral ligament (LCL)FCL, and is fixed to the femur
proximal to the lateral epicondyle. However, a distally-fixed ITB transfer, originally
described by Ellison, has also been used10. This technique uses a strip of ITB, which
is elevated from Gerdy’s tubercle with a sliver of bone and reflected proximally, then
passed deep to the FLCL, and reattached to the region of Gerdy’s tubercle. Prior to
passage of the strip of ITB deep to the FLCL, the ALC is plicated. The defect in the
ITB is subsequently closed. The proposed advantage of this technique was that it
maintained an element of dynamic control of rotation by not fixing the strip of ITB
proximally, but keeping it in continuity with the rest of the ITB. As a result the
construct will tend to tighten in extension, as it deviates from its natrural alignment
around the FLCL, and slacken as the knee flexes25 . As a result it will be effective at
the lower flexion angles when the pivoit shift phenomenon occurs and not have an
effect with more flexed knee positions so not interfering with natural rotatory laxities
and avoiding excess tightness.
One of the major concerns regarding proximally fixed lateral extra-articular tenodesis
(LEAT) procedures is that they can potentially increase the ‘constraint’ of the lateral
compartment and that this may have a long term impact on the knee35. To date,
biomechanical studies comparing LEAT procedures have focused on both
proximally-fixed techniques and anatomical ALL reconstructions. There have been no
studies examining the knee kinematics with a distally-fixed lateral extra-articular
augmentation procedure, which may potentially cause less constraint of the lateral
compartment due to the absence of proximal fixation to the femur.
The primary aim of this study was to investigate the effect of a modified Ellison
procedure in restoring native kinematics of the knee following complete sectioning of
the ALC. The secondary aim was to assess the effect of closure of the ITB graft
8 of 24
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171

harvest site on knee kinematics. The authors hypothesised that a distally-fixed lateral
extra-articular augmentation procedure would restore native knee kinematics
following sectioning of the ALC and that closure of the ITB defect would decrease
rotational laxity of the knee compared to leaving it open.
Materials and Methods
Specimen Preparation
Twelve fresh-frozen (6 female and 6 male; 4 left and 8 right) human cadaveric knees
(mean age 55 years (SD, ±7.5 years; range, 42-64 years) without evidence of prior
injury, abnormalities or surgery, were used in this study. A power calculation based
on a previous studiesy determined that a sample size of 8 would allow the
identification of changes in translation and rotation of 2 mm and 1.2, respectively,
with 80% power and 95% confidence24, 26, 32. Based on the greatest SD of laxity being
±1.1 mm at 60, 12 knees were used to identify potentially small differences.
The specimens were procured from a tissue bank after approval from the local
research ethics committee. Each specimen was thawed for 24 hours before use. The
femur was sectioned 190 mm from the joint line and the soft tissues resected from
the proximal 80 mm, leaving 110 mm of ITB and soft tissue remaining. The tibia was
sectioned 160 mm from the joint line and the soft tissue resected from the distal 60
mm. The fibula was transfixed to the tibia with a tri-cortical screw.
A longitudinal lateral incision was made from Gerdy’s tubercle to the proximal skin
edge and the superficial fat was reflected to expose the ITB. The ITB was identified
and the proximal 20 mm was reinforced with a cotton patch to avoid suture pull out.
Two strands of 2-0 suture (wasn't it #2?) (Ultrabraid, Smith & Nephew Endoscopy,
Andover, Massachusetts) were whip-stitched to the anterior and posterior borders of
9 of 24
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199

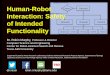
the ITB to facilitate tensioning during robotic testing (Figure 1). This was necessary
due to the fact that in the Ellison technique10 there is no proximal fixation of the ITB,
as it relies upon the dynamic effect of the tensor fasciae latae on the ITB.
Figure 1: A clinical photograph of a right knee. The ITB (black arrow) was identified
and the proximal 20 mm was reinforced with a cotton patch (white arrow) to avoid
suture pull out. Two strands of 2-0 (?) suture (ULTRABRAID (ltrabraid, Smith &
Nephew Endoscopy, Andover, Massachusetts) were whip-stitched on the anterior (A)
and posterior (B) borders of the ITB to facilitate tensioning during robotic testing.
The tibia was cemented into a 60 mm diameter stainless steel pot using
polymethylmethacrylate (Simplex Rapid, Kemdent, UK). The long axis of the cylinder
was perpendicular to the joint surface in the coronal plane and parallel to the long
axis of the bone in the sagittal plane. Having fixed the tibia into the end-effector of the
robot, zero degrees flexion was defined when 3.2 mm guide wires drilled postero-
anteriorly through the tibia and femur at 70 mm and 100 mm from the joint line,
respectively, were parallel. A 60 mm pot was mounted on the base plate with anterior
10 of 24
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217

and posterior polyethylene tubes passed through it, aligned with the respective
borders of the ITB; these were lubricated with food grade silicone lubricant (CRC,
Horsham, PA) to minimise the friction during dynamic testing. Having cemented the
femur and the tubes with the knee in extension, the ITBT loading sutures were tied in
loops, passed through the appropriate tube and a 30 N tensile load was applied
parallel to the femoral axis 43 (Figure 2A and B).
Figure 2A and B: A clinical photograph of a right cadaveric knee with the femur (F)
mounted on the base plate with the tibia (T) connected to the robotic arm. A: A lateral
view of the specimen demonstrating the iliotibibial band (ITB) under tension with the
sutures running through anterior and posterior polyethylene tubes aligned with the
respective borders of the ITB; B: The sutures fixed to the ITB pass throught the
polyethylene tubes (Red arrow,) which areis lubricated with silicone to reduce friction,
are passed over a pulley (White arrrow) and a fixed to weights applying a 30 N
tensile load (Dashed arrow).
Robotic System
11 of 24
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234

The robotic biomechanical testing system comprised a 6 degrees-of-freedom (DOF)
robotic manipulator (TX90, Stäubli Ltd, Switzerland) and a 6-axis universal force-
moment sensor (Omega 85, ATI Industrial Automation), with custom-designed tibial
and femoral fixtures (Figure 2 B). The force sensor had a resolution of 0.3 N, 0.3 N
and 0.4 N for X, Y and Z axis forces, respectively, and 0.01 Nm for X, Y and Z axis
torques. The robotic system had a load capacity of 200N and a test-retest SD of ±
0.10 mm and ± 0.12 in translation and rotation between the bone mountings.
Biomechanical Testing
Maintaining 0° knee flexion, the system minimized the forces and torques in the
remaining 5 DOF and recorded a known starting point for the intact knee. From this
point, the force sensor guided the passive path of knee flexion from 0°-90° while
minimizing the five remaining forces and torques. Three cycles of flexion-extension
were performed to minimize error from the inherent stress-relaxation properties of
soft tissue17. As in previous work using this platform32, knee laxity was quantified by
holding a fixed degree of flexion along the passive path whilst imposing a
rotatory/translational displacement and neutralising the remaining four DOF: 90 N for
anterior tibial translation, 5 Nm for internal/external rotation (IR/ER) and coupled
moments of 4 Nm IR with 8 Nm valgus to simulate the pivot-shift laxity21. The
anterior, IR and ER laxities were evaluated at 0, 30, 60 and 90 of flexion3, 13, 26,
47.The simulated pivot shift (SPS) was performed at 0, 15, 30 and 45 of flexion3, 12, 46
and the coupled tibial displacement divided into IR and anterior translation
components.
Transection of Anterolateral Capsule
12 of 24
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262

Following assessment of the intact state, the knee was held in 90 of flexion. The
lateral fibular collateral ligament (FLCL) was identified deep to the ITB. The ITB was
retracted with a Langenbeck retractor and, using a Beaver blade (Smith & Nephew
Endoscopy, Andover, Massachusetts), the ALC was incised by making an incision
directly anterior to the anterior border of the FLCL; the incision was approximately 20
mm in length and extended from the femoral attachment of the FLCL to the joint line
as previously described6, 9, 23, 25. The release was confirmed using a haemostat
forceps to ensure all fibres had been transected (Figure 3).
Figure 3: A clinical photograph of a left knee specimen with the femur(F) and tibia(T)
marked. The iliotibial band was undermined distal to the fibular collateral ligament
(FCL) (outlined with white dashed-lines) (we need to be consistent re LCL or FCL as
the text uses both – for AJSM I think FCL preferred) and is being elevated with a
scissors(S). A blade was used to transect the anterolateral capsule of the knee distal
to the FCL without violating the ITB a as depicted by the red dashed-line.
Surgical Technique
A modified Ellison procedure was performed in line with current clinical practise
among the authors. The modifications of the technique were that the ALC was
neither repaired or plicated, and the distal end of the strip of ITB was reduced
anatomically and fixed, rather than shifted anteriorly and proximally as advocated in
the original description10. In order to focus purely on the effect that the ALC pathology
13 of 24
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284

and Ellison procedure had on knee kinematics, the ACL was left intact, to represent a
‘perfect’ ACL reconstruction.
The knee was held in 60 of flexion and neutral tibial rotation. The bony landmarks of
the lateral femoral epicondyle and Gerdy’s tubercle were identified and the posterior
border of the ITB was clearly exposed. An incision was made 10 mm anterior and
parallel to the posterior border of the ITB starting distally at Gerdy’s tubercle and
extending proximally to a point proximal to the origin femoral attachment of the FLCL.
A second parallel incision was made 10 mm anterior to the first to develop a strip of
ITB. At Gerdy’s tubercle a10 mm osteotome was used to remove a sliver of bone
along with the distal insertion of the ITB strip. The ITB strip was mobilised and
reflected in a proximal direction. The FLCL was identified and isolated by making
incisions anterior and posterior to the ligament. The distal end of the ITB strip was
then passed deep to the FLCL from proximal to distal, and secured anatomically to
the bone attachment site using a 5 mm TwinFix titanium anchor with Ultrabraid
(Smith & Nephew Endoscopy Co, Andover, Massachusetts) sutures. When
performed, primary closure of the ITB graft donor site was with a continuous stitch
using a 1-vicryl (Ethicon, Somerville, NJ, USA) suture.
With regard to the secondary aim of the study to assess the effect to closure of the
ITB on knee kinematics, the order of testing of the ‘open’ versus ‘closed’ ITB defect
was randomly selected for each knee.
Statistical Analysis
If Kiron was involved in stats does he need to be an author?
The kinematic data of the intact and deficient states were analysed using a 1-way
paired sample t-test to evaluate the effect of ALC transection. All kinematic data were
14 of 24
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312

subsequently analysed using a two-factor repeated measures analysis of variance
(RM-ANOVA) with Bonferroni corrections. The two factors assessed were the state of
the anterolateral side of the knee and the flexion angle of the knee. Pairwise
comparisons using a paired t test were performed where appropriate. The level of
significance was set at P < 0.05 for a single comparison. Statistical analysis was
performed in SPSS v 21, IBM Corp.
Results
The data for the intact state, ALC-sectioned state, and ITB-open and ITB-closed
modified Ellison procedures are displayed in Table 1.
Compared to the intact state, transection of the ALC resulted in very small but
statistically significant increases in both internal tibial rotation (IR) (mean increase
approximately 2o) and anterior tibial translation (ATT) (mean change approximately
0.2 mm) when measured as isolated displacements or as part of the simulated pivot
shift (SPS)(P<0.05, apart from coupled ATT in the SPS testing mode).
The modified Ellison procedures gave rise to a significant reduction in the laxity
increases seen with transection of the ALC (Figures 4 and 5). Specifically, there was
a reduction in IR in isolation and during the SPS compared to the ALC-sectioned
state (P<0.05). In some instances the IR was reduced to less than the intact state;
this overconstraint occurred at 30° of knee flexion for both the closed and open
modified Ellision procedures (Figure 4), but only for the closed procedure during the
SPS (Figure 5). Although the closure of the ITB resulted in a statistically significant
reduction in coupled IR during SPS at 15° and 30° compared to the intact state, there
was no significant difference between the open or closed modified Ellision procedure
at any flexion angle.
15 of 24
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340

16 of 24
341
342
343
344
345

Table 1 : Translational and rotational differences relative to the intact state
Flexion Angle
Translation/rotation at intact state (mm/deg)
Differences from intact (mm)
ALC-Sectioned “Closed” Modified Ellison
“Open” Modified Ellison
Anterior Tibial Translation (mm) 0° 2.5 ± 0.6 0.2 ± 0.1* 0.0 ± 0.1 -0.1 ± 0.1‡
30° 4.4 ± 0.6 0.2 ± 0.2* 0.1 ± 0.3 -0.1 ± 0.260° 4.6 ± 1.1 0.2 ± 0.2* 0.2 ± 0.3 0.0 ± 0.290° 3.4 ± 1.0 0.1 ± 0.2* 0.2 ± 0.4 0.1 ± 0.3
Simulated pivot shift: anterior tibial translation (mm) 0° 0.7 ± 0.5 0.1 ± 0.1* -0.3 ± 0.2*‡ -0.4 ± 0.3*‡
15° 1.3 ± 1.8 0.2 ± 0.3* -0.6 ± 0.4*‡ -0.7 ± 0.4*‡
30° 2.1 ± 2.4 0.3 ± 0.5 -0.5 ± 0.4*‡ -0.5 ± 0.4*‡
45° 2.5 ± 2.5 0.3 ± 0.6 -0.4 ± 0.4‡ -0.3 ± 0.4‡
Simulated pivot shift: internal tibial rotation (o) 0° 7.3 ± 4.7 1.1 ± 1.7* 0.1 ± 1.8‡ -0.1 ± 1.8‡
15° 11.3 ± 16.5 1.4 ± 2.0* -1.5 ± 1.8*‡ -1.9 ± 1.4‡
30° 14.6 ± 21.7 2.0 ± 2.3* -1.7 ± 1.8‡ -2.2 ± 1.9‡
17 of 24
346

45° 15 ± 24.3 2.4 ± 2.1* 1.2 ± 1.7‡ -1.8 ± 2.4‡
Internal Tibial Rotation (o) 0° 7.1 ± 3.8 1.2 ± 0.5* -0.5 ± 0.9‡ -0.9 ± 0.8*‡
30° 15.6 ± 18.8 1.7 ± 0.7* -1.5 ± 1.3*‡ -1.6 ± 1.4*‡
60° 15.9 ± 21.4 1.9 ± 0.8* -0.6 ± 1.6‡ -0.4 ± 1.5‡
90° 14.4 ± 20.0 1.9 ± 0.7* 0.6 ± 1.4‡ 1.3 ± 0.9*‡
Key: Anterolateral Capsule (ALC), * – statistically significant difference from the intact state (P<0.05), ‡ - statistically significant difference from the ALC-sectioned state
18 of 24

Figure 4: The difference from the laxity of the intact knee in degrees of tibial internal
rotation at 0°-90 of flexion following ALC-sectioning and a modified Ellison lateral
augmentation procedure (with and without closure of the ITB) during isolated internal
rotation testing. (ALC – anterolateral capsule, * significant difference from the intact
knee - P<0.05, ‡ significant difference from the ALC-sectioned state – P<0.05).
19 of 24
347
348
349
350
351
352
353

Figure 5: The difference in degrees of tibial internal rotation between 0°-45 of flexion
following ALC-sectioning and a modified Ellison lateral augmentation procedure (with
and without closure of the ITB) compared to the intact knee during simulated pivot
shift. (ALC – anterolateral capsule, * significant difference from the intact knee -
P<0.05, ‡ significant difference from the ALC-sectioned state – P<0.05).
20 of 24
354
355
356
357
358
359

Discussion
The main finding of this study was that the modified Ellison procedure was effective
in controlling anterolateral rotatory laxity of the knee. Specifically, the modified Ellison
procedure significantly reduced tibiofemoral motion from the anterolateral complex-
sectioned state and restored kinematics close to the intact state. This study also
found no statistically significant difference in knee kinematics at any flexion angle
whether the ITB defect was closed or left open following a modified Ellison
procedure. To the authors’ knowledge, this is the first biomechanical study to analyse
a distally-fixed lateral extra-articular augmentation procedure using a 6-DOF robotic
system with loading of the ITB.
A number of in vitro biomechanical studies have been performed to assess knee
kinematics following lateral augmentation or reconstructive procedures41. These
studies have focused mostly on proximally-fixed LEAT procedures or ALL
reconstruction and have reported varying results19, 39. A recent controlled laboratory
study by Geeslin et al14, using a 6-DOF robotic system, determined that both a
modified-Lemaire and an ALL reconstruction combined with an ACL reconstruction
resulted in significant reductions in tibiofemoral motion at most knee flexion angles,
although overconstraint was also identified. The current study found a reduction in
isolated internal rotation with the modified Ellison procedure across 0o to 90o flexion.
Similarly, during a simulated pivot shift, the coupled internal rotation was significantly
reduced at 15 and 30 of knee flexion compared to the native knee with a modified
Ellison procedure when the ITB was closed. These findings are similar to the results
of Geeslin et al14 during SPS when the modified Lemaire or ALL reconstruction had a
fixation angle of 30, albeit with less overconstraint at 30 of knee flexion. It is
important to note that there were methodological differences between the two studies
despite using a similar robotic testing model: in the study by Geeslin et al, the distal
21 of 24
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387

Kaplan fibres were cut as part of their sectioning to of the anterolateral complex, an
ACL reconstruction was performed in conjunction with the LEAT, and there was no
loading of the iliotibial bandITB. In the current study, the ITB was loaded for all
testing states to facilitate testing of a distally-fixed LEAT, which relies upon the
dynamic effect of the ITB. Furthermore, the ACL was left intact in the current study to
represent a ‘perfect’ ACL reconstruction.
It is evident from the literature that a distally-fixed LEAT is less widely used than a
proximally-fixed procedure8, 40. The operative technique of a distal ITB transfer was
described by Ellison in 1979 and used in isolation for the treatment of ACL-deficient
knees with anterolateral rotatory instability10. The technique described was more
extensive than the modified version detailed in the current study. The theory behind
this technique was that the broad-based shape of the strip of ITB preserves the blood
supply to the fascia and the dynamic pull of the tensor fasciae latae and part of the
gluteus maximus10. This theory was disputed by Kennedy et al in an earlier
publication in 1978, who reported relatively poor results using this technique in
isolation or combined with other reconstructive procedures22. The authors claimed
that they could not prove the dynamic function clinically and the subjective results did
not suggest such a function existed. Lipscomb et al, reporting on a series of 75 knees
with chronic ACL deficiency which were treated with a semitendinosus and gracilis
intra-articular ACL reconstruction, posteromedial and lateral capsular ligament
reefing, and an Ellison LEAT, contended that the distally-fixed LEAT did not
adequately prevent anterolateral instability 10, 30, 31, 33. However, no objective evidence
to support this assertion was presented in their studies. They subsequently went on
to use a proximally-fixed Losee procedure, which the authors claimed was static, and
therefore more effective33.
In the context of LEAT, it is important to consider what is the appropriate amount of
22 of 24
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415

constraint and what represents ‘over-constraint’. The term ‘over-constraint’ is usually
used to imply there will be longterm consequences of osteoarthritis from a procedure.
However authors rarely explain what they men by the term. It could mean loss of
normal flexion range, loss of normal rotational laxity, or increased articular contact
pressure. Biomechanical studies are limited by the fact that they assess the laxity of
a joint at time zero, i.e. immediately after surgery, but fail to account for laxity that
may occur as a result of elongation of tissues over time. In their systematic review,
Slette et al suggested that after a period of initial stability, LEAT procedures have
often shown a tendency to elongate, with return of anterolateral rotatory instability in
the ACL-deficient knee40. However, the studies used to support this claim focused on
LEAT procedures performed in isolation for the treatment of chronic ACL-deficiency2,
7, 22, 40. It is notable that two of these studies included distally-fixed Ellison LEAT
procedures, which is perhaps why this procedure fell out of favour. On the other
hand, Engebretsen et al have shown that when an LEAT is performed in conjuction
with an ACLR, the ACL graft is subjected to less load11.
Kittl et al have demonstrated that the superficial ITB, as well as deep layers, plays an
integral role in controlling anterolateral rotatory laxity25. Based on this finding, the
hypothesis that closure of the ITB defect would result in further restriction of IR due to
anteriorisation of the iliotibial tract was postulated. This study rejected this
hypothesis: closure of the ITB defect was not found to have a significant effect on
rotational laxity. Interestingly, in the original description of the Ellison procedure,
complete closure of the ITB defect was considered an essential step10. On a practical
level, closure of the defect may prevent muscle herniation of vastus lateralis and
makes for a more cosmetically acceptable appearance. Although it would seem
logicalis possible that closure of an ITB defect may also increase the contact
pressure placed on the lateral facet of the patella, this has only been found with a
proximally-fixed ITB graft excessively tensed to 80 N20 thereby causing fixed external
23 of 24
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442

rotation of the tibia (it did not occur with lower levels of tension and a neutral position
of fixation of the tibia) 20 . It, so would clearly not occur with the minimally-tensed
distally-fixed procedure.
Limitations
The authors acknowledge that there are some limitations of the present study. The
specimens were 55 ± 7.5 years old, higher than the patient group that typically suffer
an ACL rupture, but comparable to previous similar cadaveric studies19, 32. The results
presented are only representative of a ‘time zero’ state and do not take into account
subsequent healing, cyclic loading and rehabilitation. The clinical pivot shift is a
dynamic examination through a range of motion. Using a single robotic manipulator,
this and other studies have not replicated in vivo kinematics but only the coupled
laxities16, 24, 32. On the other hand, the advantages of this study design included
loading of the ITB to simulate any dynamic effect it might have in a lateral
augmentation. Because the optimal ACL reconstruction technique continues to be
debated, leaving the native ACL intact avoided any variations in technique or
prejudice against a particular technique of ACL reconstruction44. It is also important to
note that the differences in tibial anterior translation were less than 1 mm in all cases,
reflecting the dominant role of the ACL, and raising the question of the clinical
relevance of using a lateral procedure to control anterior translation despite the
statistical differences found.
Conclusion
A distally-fixed lateral augmentation procedure can closely restore knee laxities to
native values in an anterolateral capsule-sectioned knee. No significant difference
24 of 24
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468

was found between closing or leaving the ITB defect open in the modified Ellison
procedure.
References:
1. Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F. Anterior cruciate ligament
reconstruction: bone-patellar tendon-bone compared with double
semitendinosus and gracilis tendon grafts. J Bone Joint Surg Am.
2004;86(10):2143-2155.
2. Amirault JD, Cameron JC, MacIntosh DL, Marks P. Chronic anterior cruciate
ligament deficiency. Long-term results of MacIntosh's lateral substitution
reconstruction. Journal of Bone and Joint Surgery Series B. 1988;70(4):622-
624.
3. Anderson CJ, Westerhaus BD, Pietrini SD, et al. Kinematic impact of
anteromedial and posterolateral bundle graft fixation angles on double-bundle
anterior cruciate ligament reconstructions. Am J Sports Med.
2010;38(8):1575-1583.
4. Branch T, Lavoie F, Guier C, et al. Single-bundle ACL reconstruction with and
without extra-articular reconstruction: evaluation with robotic lower leg rotation
testing and patient satisfaction scores. Knee Surgery, Sports Traumatology,
Arthroscopy. 2015;23(10):2882-2891.
5. Claes S, Luyckx T, Vereecke E, Bellemans J. The Segond fracture: a bony
injury of the anterolateral ligament of the knee. Arthroscopy.
2014;30(11):1475-1482.
6. Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J. Anatomy of
the anterolateral ligament of the knee. J Anat. 2013;223(4):321-328.
25 of 24
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494

7. Dahlstedt LJ, Dalen N, Jonsson U. Extraarticular repair of the unstable knee.
Disappointing 6-year results of the Slocum and Ellison operations. Acta
Orthop Scand. 1988;59(6):687-691.
8. DePhillipo NN, Cinque ME, Chahla J, Geeslin AG, LaPrade RF. Anterolateral
Ligament Reconstruction Techniques, Biomechanics, and Clinical Outcomes:
A Systematic Review. Arthroscopy. 2017.
9. Dodds AL, Halewood C, Gupte CM, Williams A, Amis AA. The anterolateral
ligament: Anatomy, length changes and association with the Segond fracture.
Bone Joint J. 2014;96-B(3):325-331.
10. Ellison AE. Distal iliotibial-band transfer for anterolateral rotatory instability of
the knee. Journal of Bone and Joint Surgery Series A. 1979;61(A3):330-337.
11. Engebretsen L, Lew WD, Lewis JL, Hunter RE. The effect of an iliotibial
tenodesis on intraarticular graft forces and knee joint motion. Am J Sports
Med. 1990;18(2):169-176.
12. Engebretsen L, Wijdicks CA, Anderson CJ, Westerhaus B, LaPrade RF.
Evaluation of a simulated pivot shift test: a biomechanical study. Knee Surg
Sports Traumatol Arthrosc. 2012;20(4):698-702.
13. Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE. Distribution of in situ
forces in the anterior cruciate ligament in response to rotatory loads. J Orthop
Res. 2004;22(1):85-89.
14. Geeslin AG, Chahla J, Moatshe G, et al. Anterolateral knee extra-articular
stabilizers: a robotic sectioning study of the anterolateral ligament and distal
iliotibial band Kaplan fibers. Am J Sports Med 2018; 46: 1352-1361.
15. Goldman AB, Pavlov H, Rubenstein D. The Segond fracture of the proximal
tibia: a small avulsion that reflects major ligamentous damage. AJR Am J
Roentgenol. 1988;151(6):1163-1167.
16. Goldsmith MT, Jansson KS, Smith SD, Engebretsen L, LaPrade RF, Wijdicks
CA. Biomechanical comparison of anatomic single- and double-bundle
26 of 24
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522

anterior cruciate ligament reconstructions: an in vitro study. Am J Sports Med.
2013;41(7):1595-1604.
17. Herbst E, Albers M, Burnham JM, et al. The anterolateral complex of the
knee: a pictorial essay. Knee Surg Sports Traumatol Arthrosc.
2017;25(4):1009-1014.
18. Howard ME, Cawley PW, Losse GM, Johnston RB, 3rd. Bone-patellar
tendon-bone grafts for anterior cruciate ligament reconstruction: the effects of
graft pretensioning. Arthroscopy. 1996;12(3):287-292.
19. Inderhaug E, Stephen JM, Williams A, Amis AA. Biomechanical Comparison
of Anterolateral Procedures Combined With Anterior Cruciate Ligament
Reconstruction. The American Journal of Sports Medicine.
2016:0363546516681555.
20. Inderhaug E, Stephen JM, Williams A, Amis AA. Effect of anterolateral
complex sectioning and tenodesis on patellar kinematics and
patellofemoral joint contact pressures. American Journal of Sports
Medicine in press 20 08 2018 doi 10.1177/0363546518790248.
21. Kanamori A, Zeminski J, Rudy TW, Li G, Fu FH, Woo SL. The effect of axial
tibial torque on the function of the anterior cruciate ligament: a biomechanical
study of a simulated pivot shift test. Arthroscopy. 2002;18(4):394-398.
22. Kennedy JC, Stewart R, Walker DM. Anterolateral rotatory instability of the
knee joint. An early analysis of the Ellison procedure. J Bone Joint Surg Am.
1978;60(8):1031-1039.
23. Kennedy MI, Claes S, Fuso FA, et al. The Anterolateral Ligament: An
Anatomic, Radiographic, and Biomechanical Analysis. Am J Sports Med.
2015;43(7):1606-1615.
27 of 24
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547

24. Kittl C, El-Daou H, Athwal KK, et al. The Role of the Anterolateral Structures
and the ACL in Controlling Laxity of the Intact and ACL-Deficient Knee. The
American journal of sports medicine. 2015:0363546515614312.
25. Kittl C, Halewood C, Stephen JM, et al. Length change patterns in the lateral
extra-articular structures of the knee and related reconstructions. Am J Sports
Med. 2015;43(2):354-362.
26. Kondo E, Merican AM, Yasuda K, Amis AA. Biomechanical comparison of
anatomic double-bundle, anatomic single-bundle, and nonanatomic single-
bundle anterior cruciate ligament reconstructions. Am J Sports Med.
2011;39(2):279-288.
27. Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate
ligament injury in basketball: video analysis of 39 cases. Am J Sports Med.
2007;35(3):359-367.
28. Krosshaug T, Slauterbeck JR, Engebretsen L, Bahr R. Biomechanical
analysis of anterior cruciate ligament injury mechanisms: three-dimensional
motion reconstruction from video sequences. Scand J Med Sci Sports.
2007;17(5):508-519.
29. Lemaire M. [Chronic knee instability. Technics and results of ligament plasty
in sports injuries]. J Chir (Paris). 1975;110(4):281-294.
30. Lipscomb AB, Anderson AF. Tears of the anterior cruciate ligament in
adolescents. J Bone Joint Surg Am. 1986;68(1):19-28.
31. Lipscomb AB, Johnston RK, Snyder RB. The technique of cruciate ligament
reconstruction. American Journal of Sports Medicine. 1981;9(2):77-81.
32. Lord BR, El-Daou H, Sabnis BM, Gupte CM, Wilson AM, Amis AA.
Biomechanical comparison of graft structures in anterior cruciate ligament
reconstruction. Knee Surg Sports Traumatol Arthrosc. 2017;25(2):559-568.
28 of 24
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573

33. Losee RE, Johnson TR, Southwick WO. Anterior subluxation of the lateral
tibial plateau. A diagnostic test and operative repair. J Bone Joint Surg Am.
1978;60(8):1015-1030.
34. Mansour R, Yoong P, McKean D, Teh JL. The iliotibial band in acute knee
trauma: patterns of injury on MR imaging. Skeletal Radiol. 2014;43(10):1369-
1375.
35. Noyes FR. Editorial Commentary: Lateral Extra-articular Reconstructions With
Anterior Cruciate Ligament Surgery: Are These Operative Procedures
Supported by In Vitro Biomechanical Studies? Arthroscopy.
2016;32(12):2612-2615.
36. Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for
anterior cruciate ligament injuries in team handball: a systematic video
analysis. Am J Sports Med. 2004;32(4):1002-1012.
37. Persson A, Fjeldsgaard K, Gjertsen J-E, et al. Increased risk of revision with
hamstring tendon grafts compared with patellar tendon grafts after anterior
cruciate ligament reconstruction: a study of 12,643 patients from the
Norwegian Cruciate Ligament Registry, 2004-2012. The American journal of
sports medicine. 2014;42(2):285-291.
38. Samuelson M, Draganich LF, Zhou X, Krumins P, Reider B. The effects of
knee reconstruction on combined anterior cruciate ligament and anterolateral
capsular deficiencies. The American journal of sports medicine.
1996;24(4):492-497.
39. Schon JM, Moatshe G, Brady AW, et al. Anatomic Anterolateral Ligament
Reconstruction Leads to Overconstraint at Any Fixation Angle: Response.
Am J Sports Med. 2016;44(10):NP58-NP59.
40. Slette EL, Mikula JD, Schon JM, et al. Biomechanical Results of Lateral
Extra-articular Tenodesis Procedures of the Knee: A Systematic Review.
Arthroscopy. 2016;32(12):2592-2611.
29 of 24
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
599
600
601

41. Smith JO, Yasen SK, Lord B, Wilson AJ. Combined anterolateral ligament
and anatomic anterior cruciate ligament reconstruction of the knee. Knee
Surg Sports Traumatol Arthrosc. 2015;23(11):3151-3156.
42. Sonnery-Cottet B, Thaunat M, Freychet B, Pupim BH, Murphy CG, Claes S.
Outcome of a Combined Anterior Cruciate Ligament and Anterolateral
Ligament Reconstruction Technique With a Minimum 2-Year Follow-up. Am J
Sports Med. 2015.
43. Stephen JM, Kittl C, Williams A, et al. Effect of Medial Patellofemoral
Ligament Reconstruction Method on Patellofemoral Contact Pressures and
Kinematics. Am J Sports Med. 2016;44(5):1186-1194.
44. Suomalainen P, Jarvela T, Paakkala A, Kannus P, Jarvinen M. Double-bundle
versus single-bundle anterior cruciate ligament reconstruction: a prospective
randomized study with 5-year results. Am J Sports Med. 2012;40(7):1511-
1518.
45. Terry GC, Norwood LA, Hughston JC, Caldwell KM. How iliotibial tract injuries
of the knee combine with acute anterior cruciate ligament tears to influence
abnormal anterior tibial displacement. Am J Sports Med. 1993;21(1):55-60.
46. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanical
analysis of an anatomic anterior cruciate ligament reconstruction. Am J
Sports Med. 2002;30(5):660-666.
47. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanical
analysis of an anatomic anterior cruciate ligament reconstruction. American
Journal of Sports Medicine. 2002;30(5):660-666.
30 of 24
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
Recommended