Embed Size (px)
Citation preview
21 DAVID SUTTON
DAVID SUTTON PICTURES
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
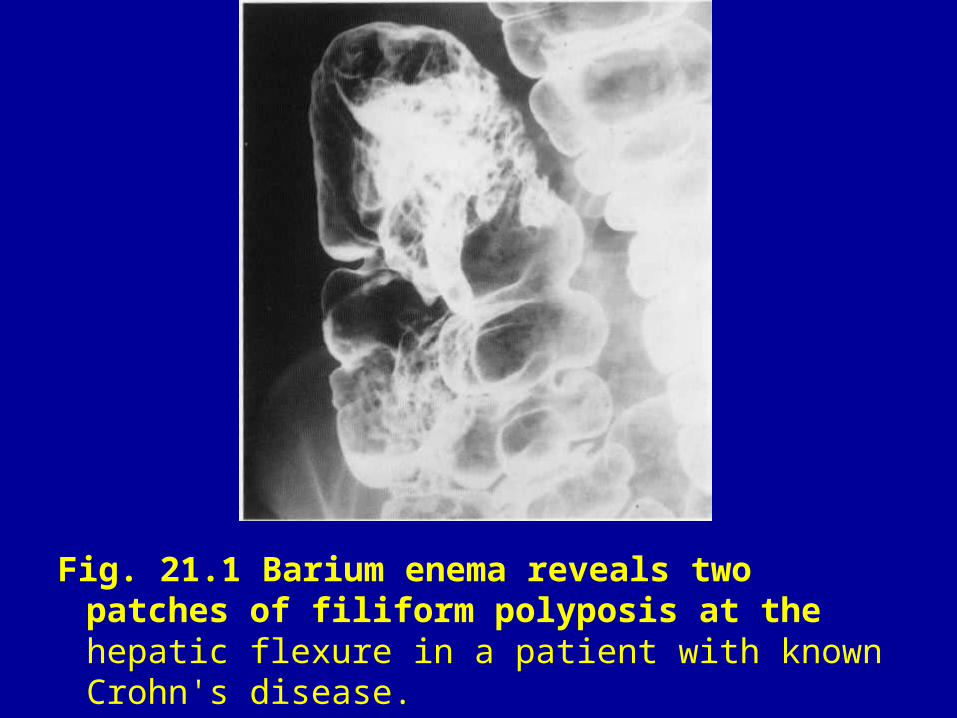
Fig. 21.1 Barium enema reveals two patches of filiform polyposis at the hepatic flexure in a patient with known Crohn's disease.
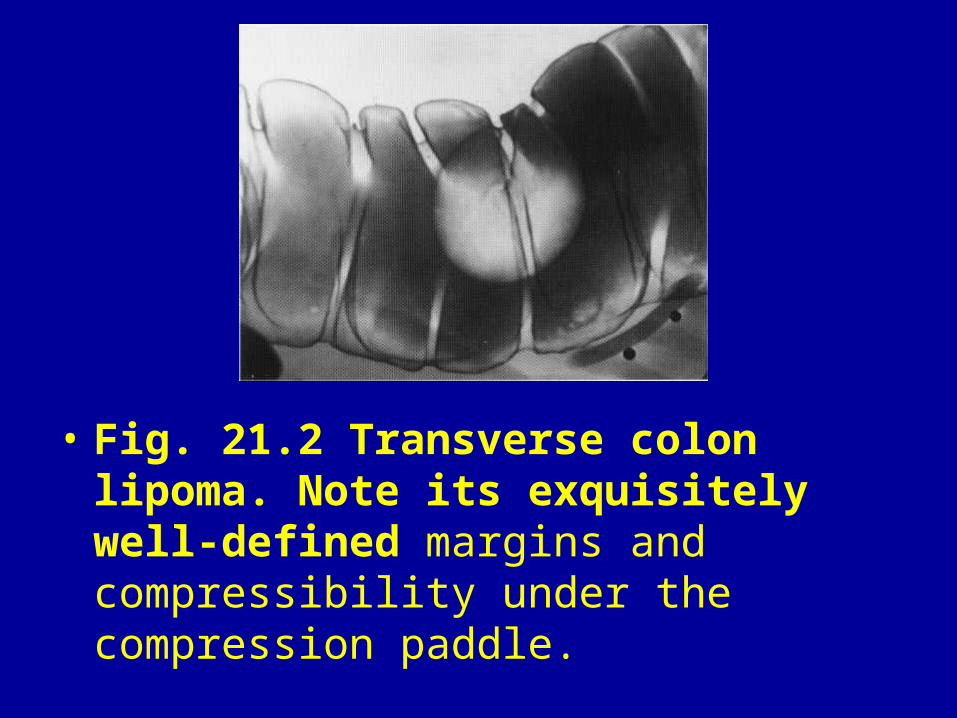
• Fig. 21.2 Transverse colon lipoma. Note its exquisitely well-defined margins and compressibility under the compression paddle.
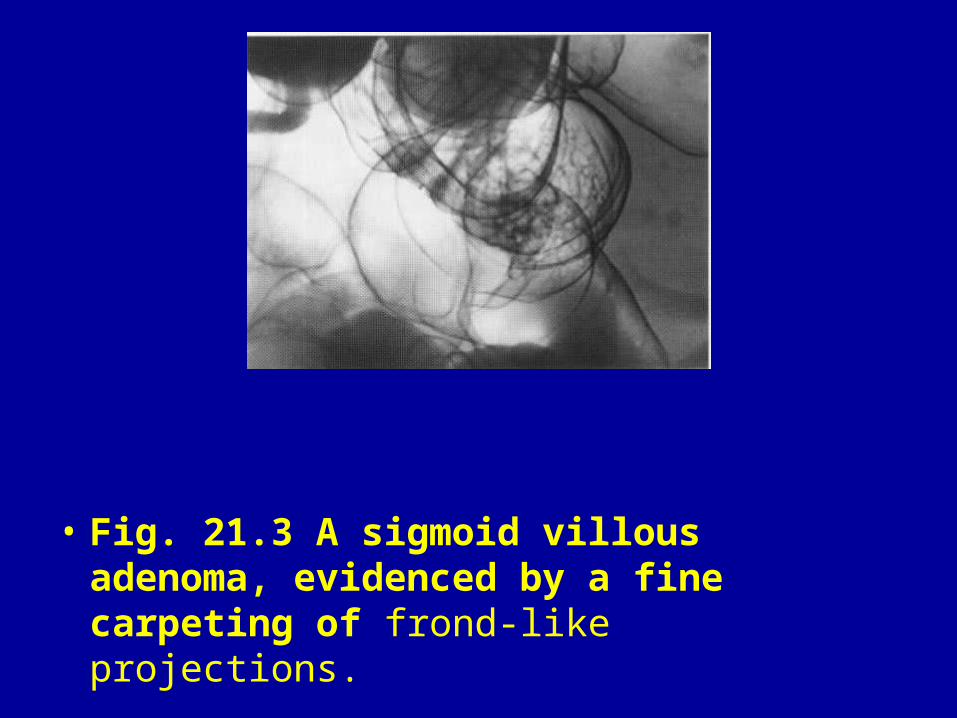
• Fig. 21.3 A sigmoid villous adenoma, evidenced by a fine carpeting of frond-like projections.
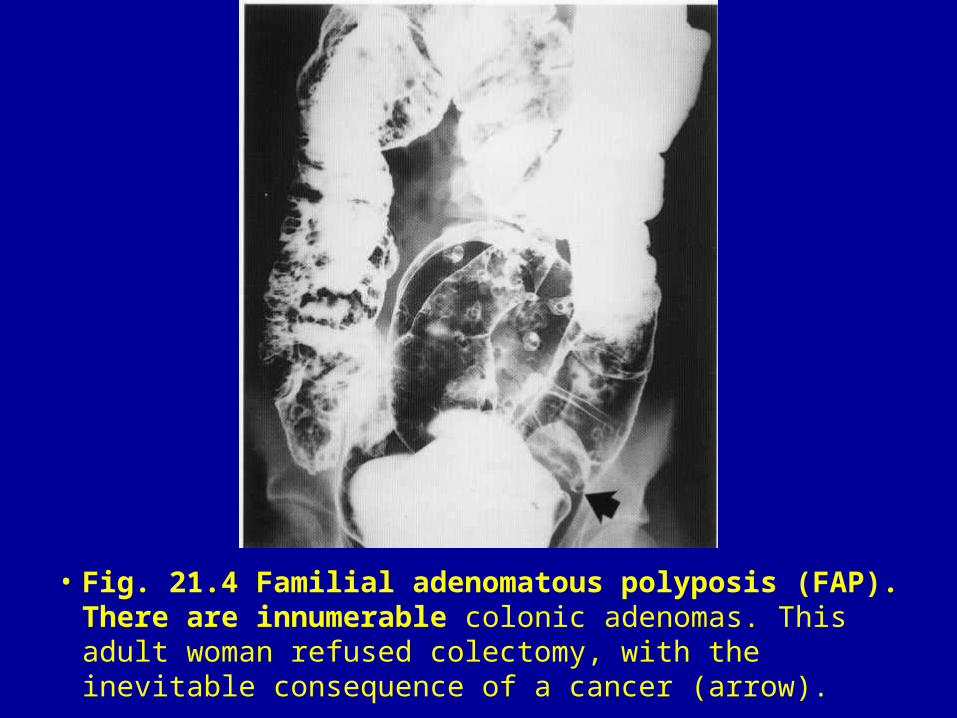
• Fig. 21.4 Familial adenomatous polyposis (FAP). There are innumerable colonic adenomas. This adult woman refused colectomy, with the inevitable consequence of a cancer (arrow).
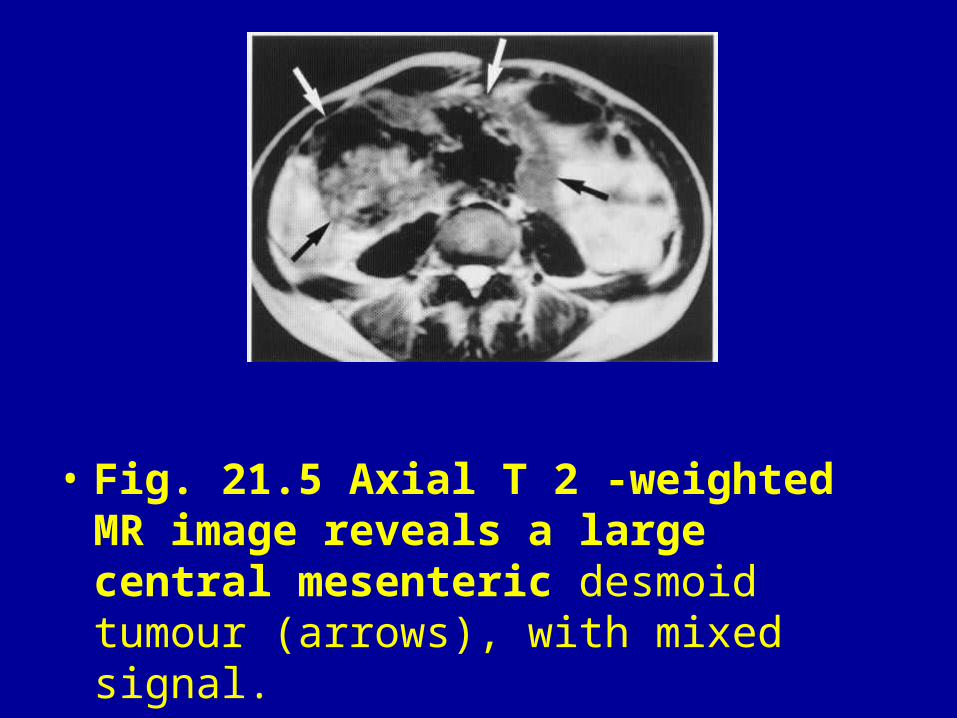
• Fig. 21.5 Axial T 2 -weighted MR image reveals a large central mesenteric desmoid tumour (arrows), with mixed signal.
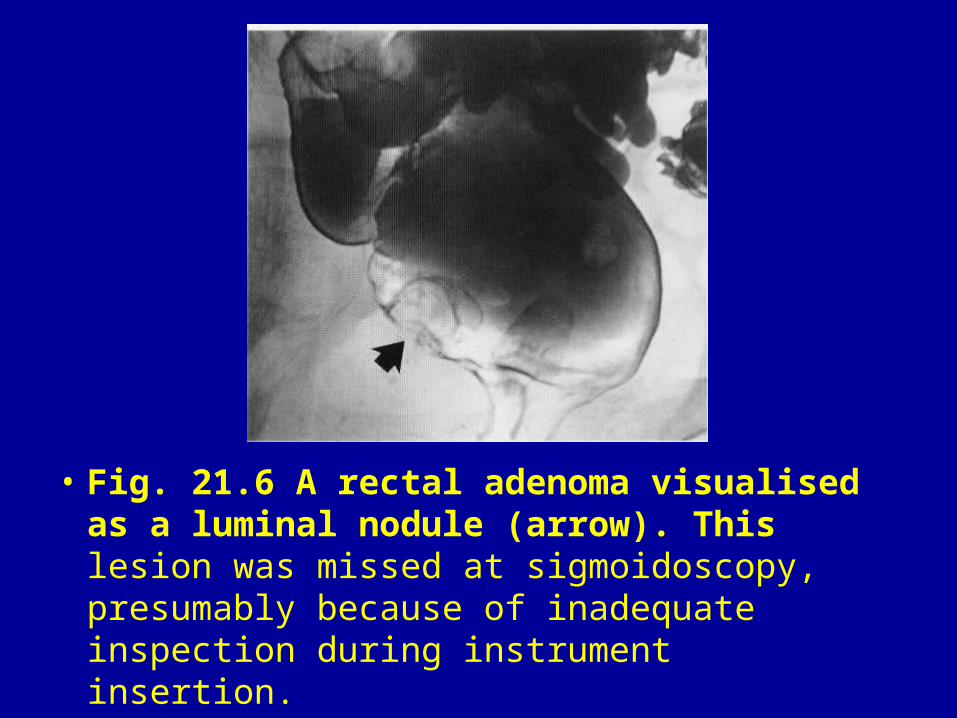
• Fig. 21.6 A rectal adenoma visualised as a luminal nodule (arrow). This lesion was missed at sigmoidoscopy, presumably because of inadequate inspection during instrument insertion.
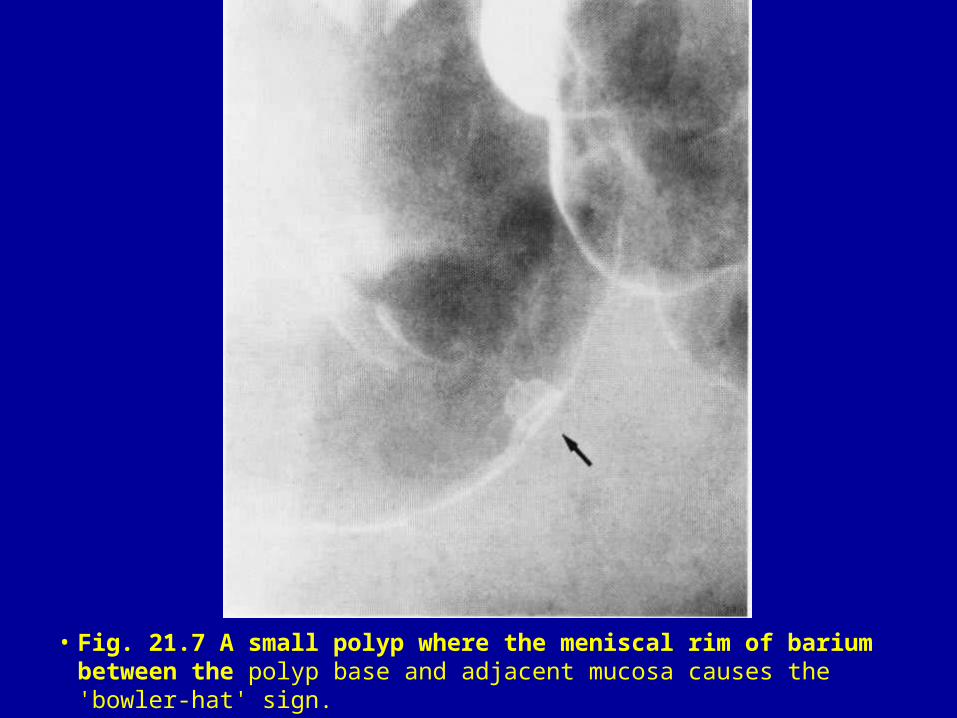
• Fig. 21.7 A small polyp where the meniscal rim of barium between the polyp base and adjacent mucosa causes the 'bowler-hat' sign.
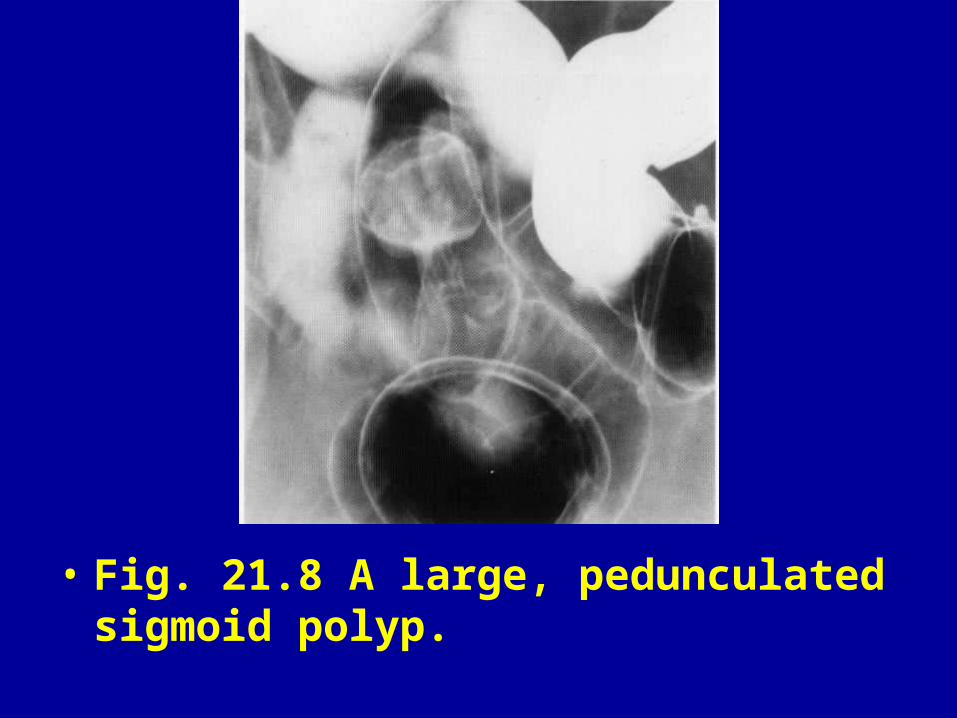
• Fig. 21.8 A large, pedunculated sigmoid polyp.
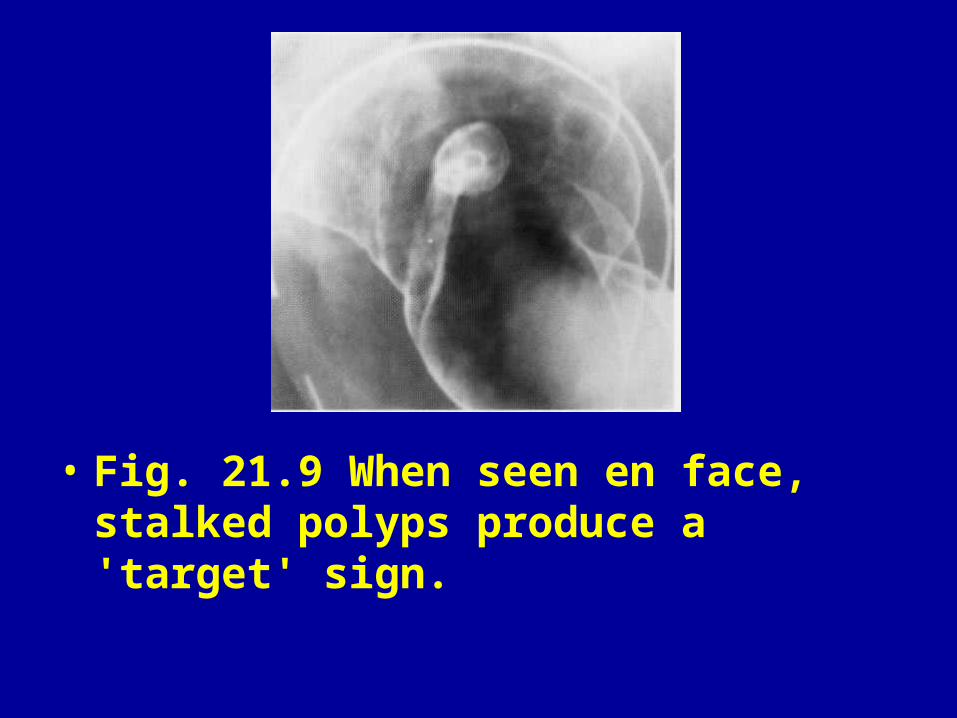
• Fig. 21.9 When seen en face, stalked polyps produce a 'target' sign.
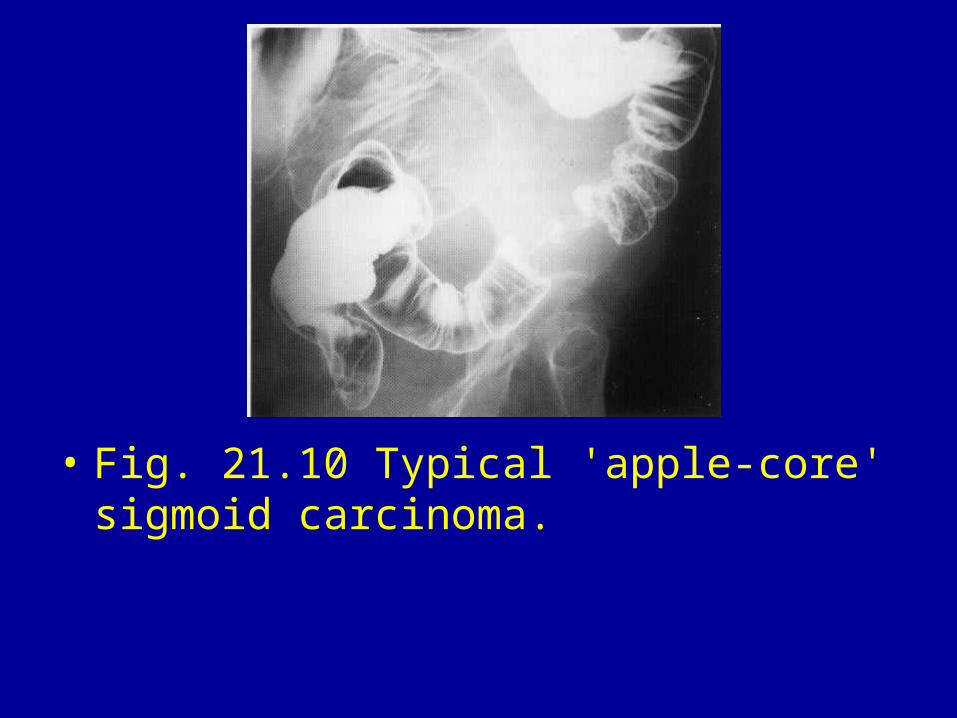
• Fig. 21.10 Typical 'apple-core' sigmoid carcinoma.
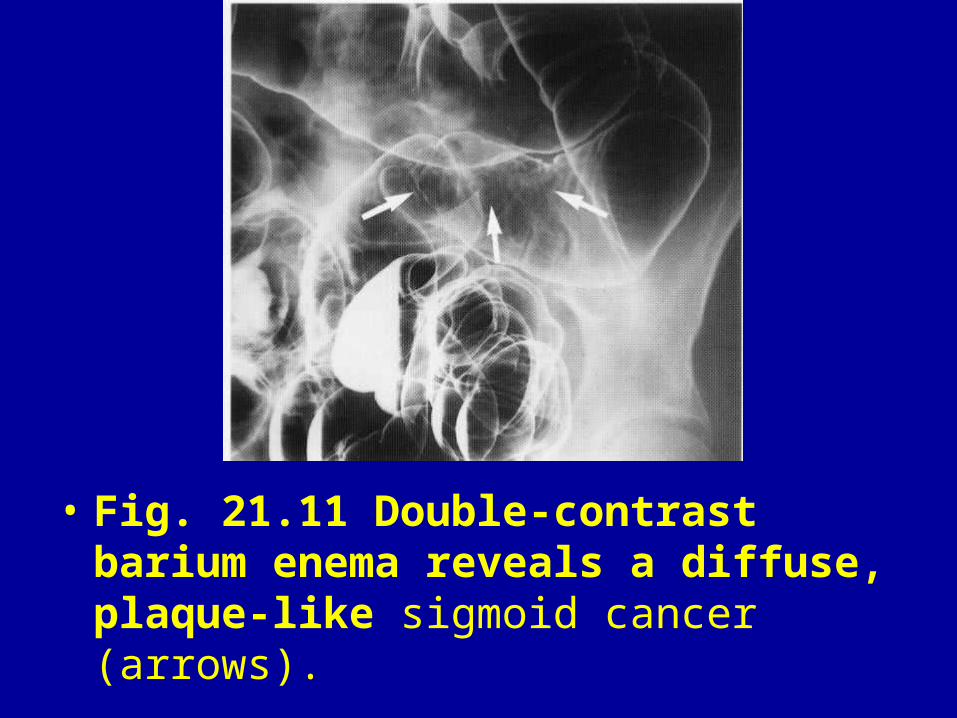
• Fig. 21.11 Double-contrast barium enema reveals a diffuse, plaque-like sigmoid cancer (arrows).
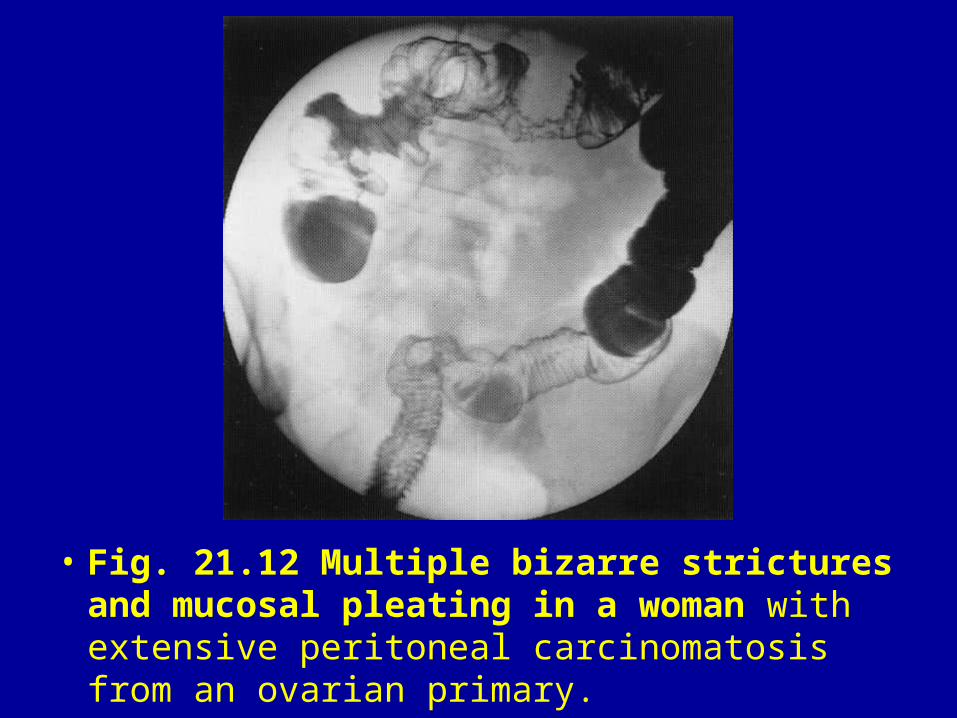
• Fig. 21.12 Multiple bizarre strictures and mucosal pleating in a woman with extensive peritoneal carcinomatosis from an ovarian primary.
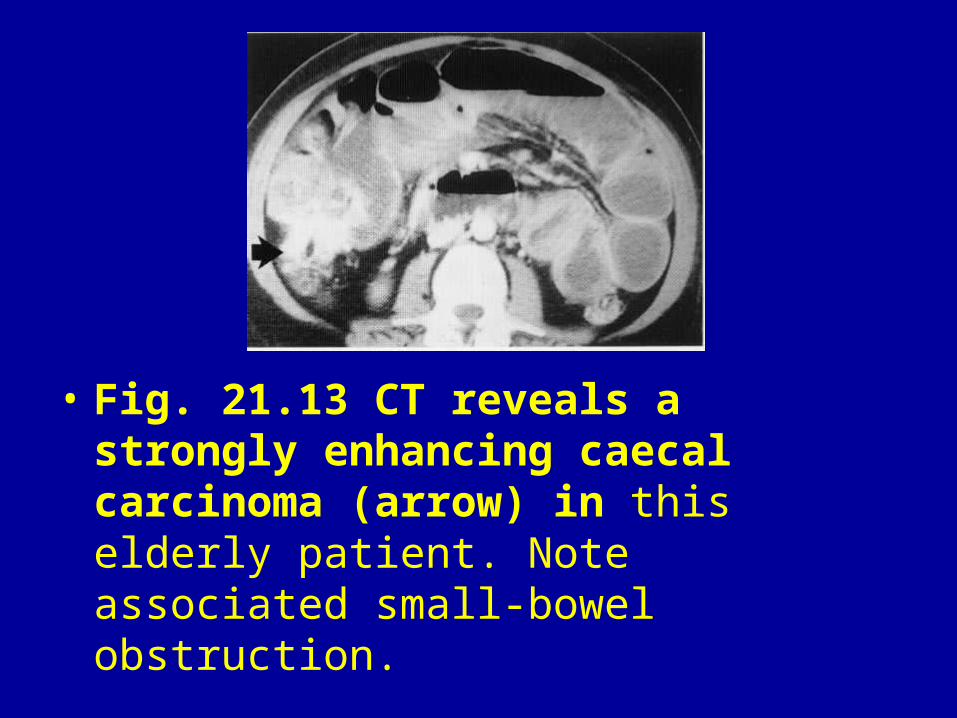
• Fig. 21.13 CT reveals a strongly enhancing caecal carcinoma (arrow) in this elderly patient. Note associated small-bowel obstruction.
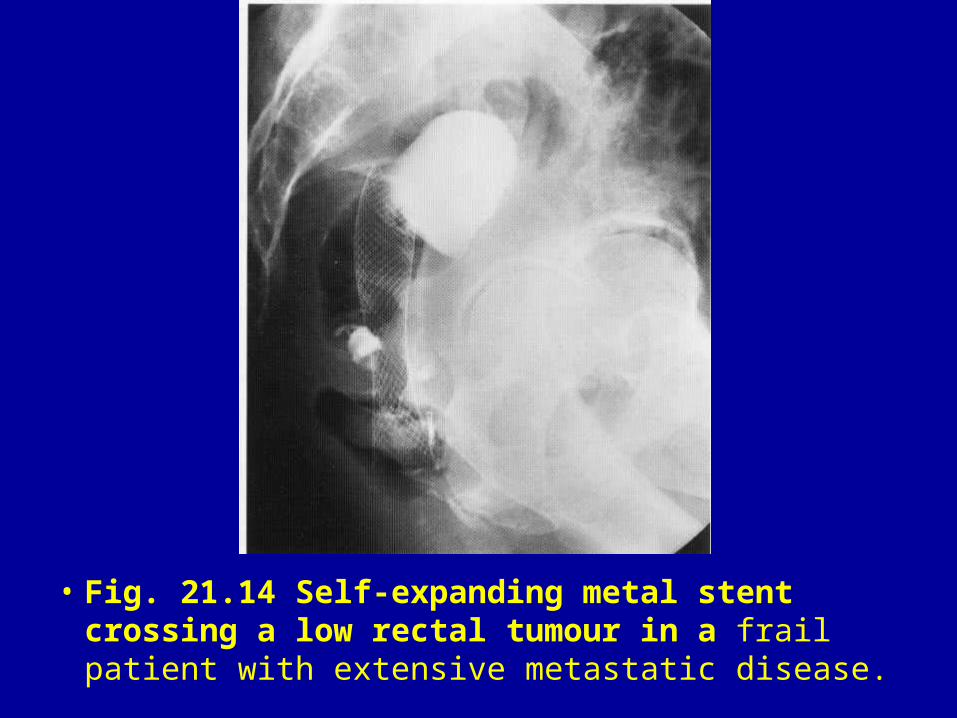
• Fig. 21.14 Self-expanding metal stent crossing a low rectal tumour in a frail patient with extensive metastatic disease.
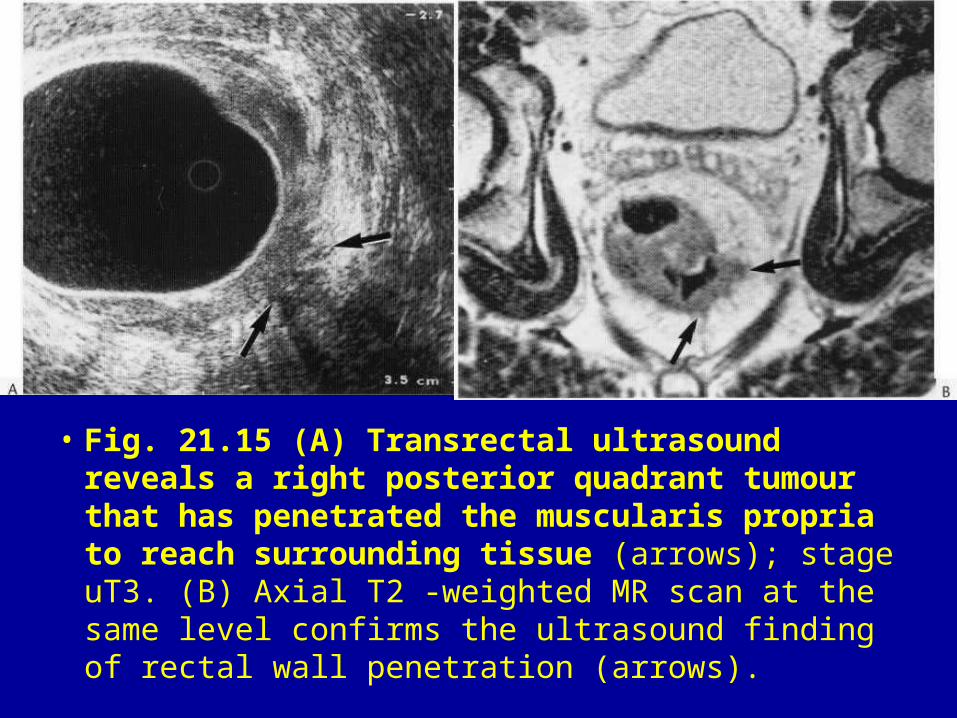
• Fig. 21.15 (A) Transrectal ultrasound reveals a right posterior quadrant tumour that has penetrated the muscularis propria to reach surrounding tissue (arrows); stage uT3. (B) Axial T2 -weighted MR scan at the same level confirms the ultrasound finding of rectal wall penetration (arrows).
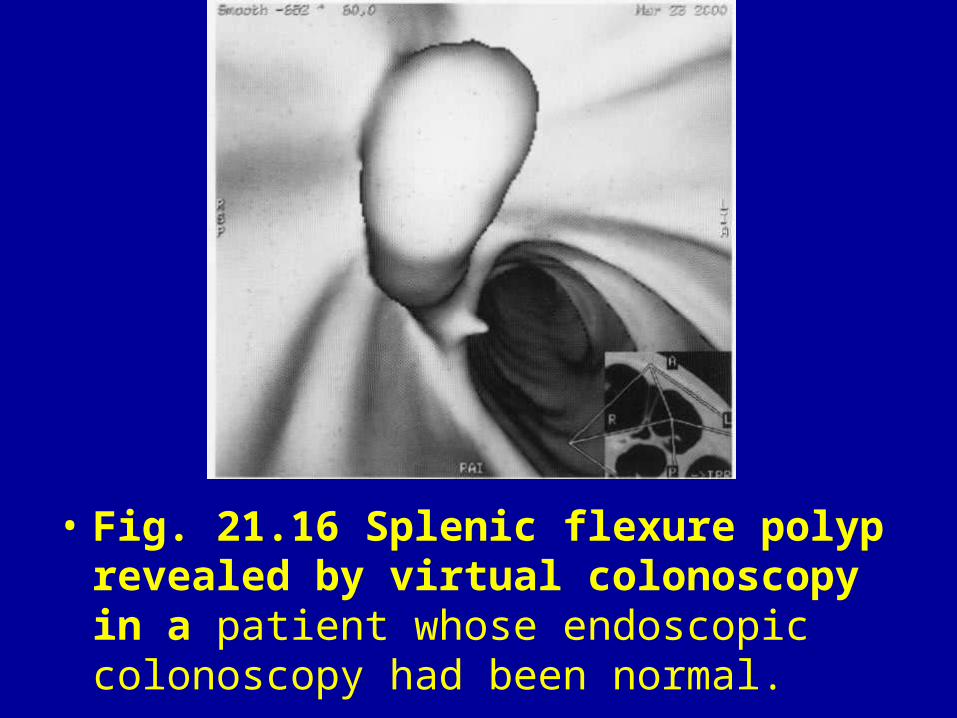
• Fig. 21.16 Splenic flexure polyp revealed by virtual colonoscopy in a patient whose endoscopic colonoscopy had been normal.
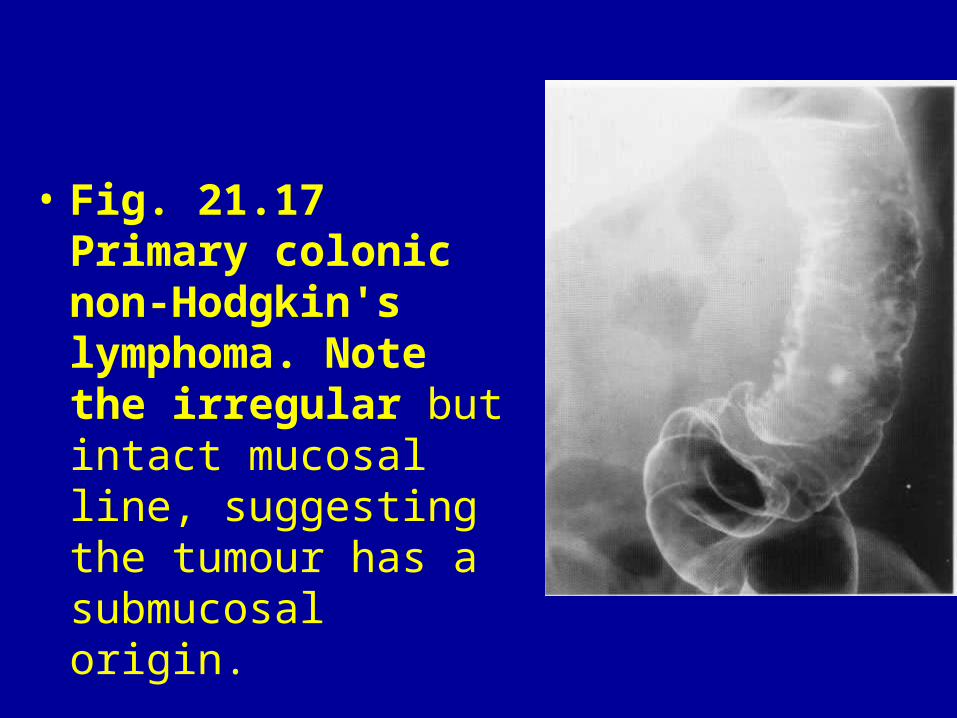
• Fig. 21.17 Primary colonic non-Hodgkin's lymphoma. Note the irregular but intact mucosal line, suggesting the tumour has a submucosal origin.
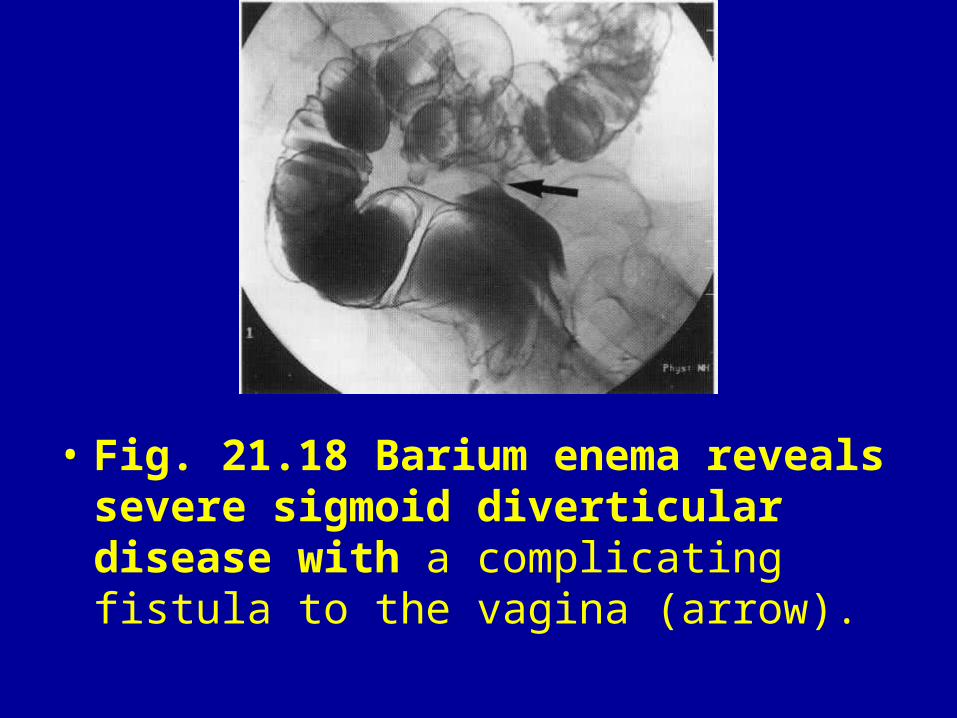
• Fig. 21.18 Barium enema reveals severe sigmoid diverticular disease with a complicating fistula to the vagina (arrow).
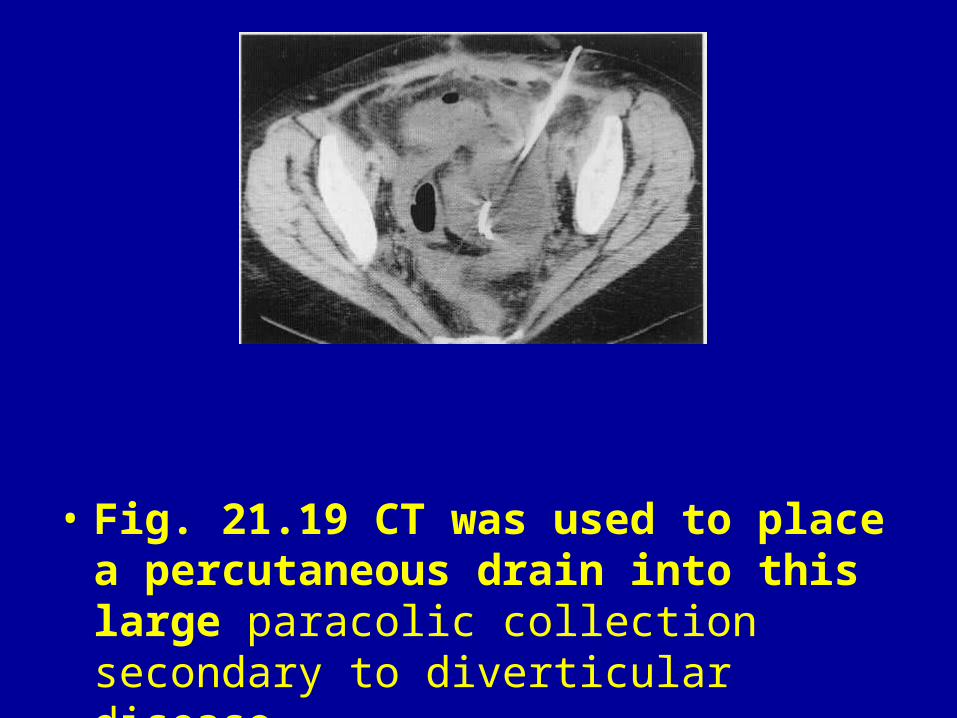
• Fig. 21.19 CT was used to place a percutaneous drain into this large paracolic collection secondary to diverticular disease.

• Fig. 21.20 CT reveals intravesical gas and the site of sigmoid fistulation on delayed scans.

• Fig. 21.21 Toxic megacolon. Luminal dilatation, abnormal haustration, mural thickening and mucosal islands.
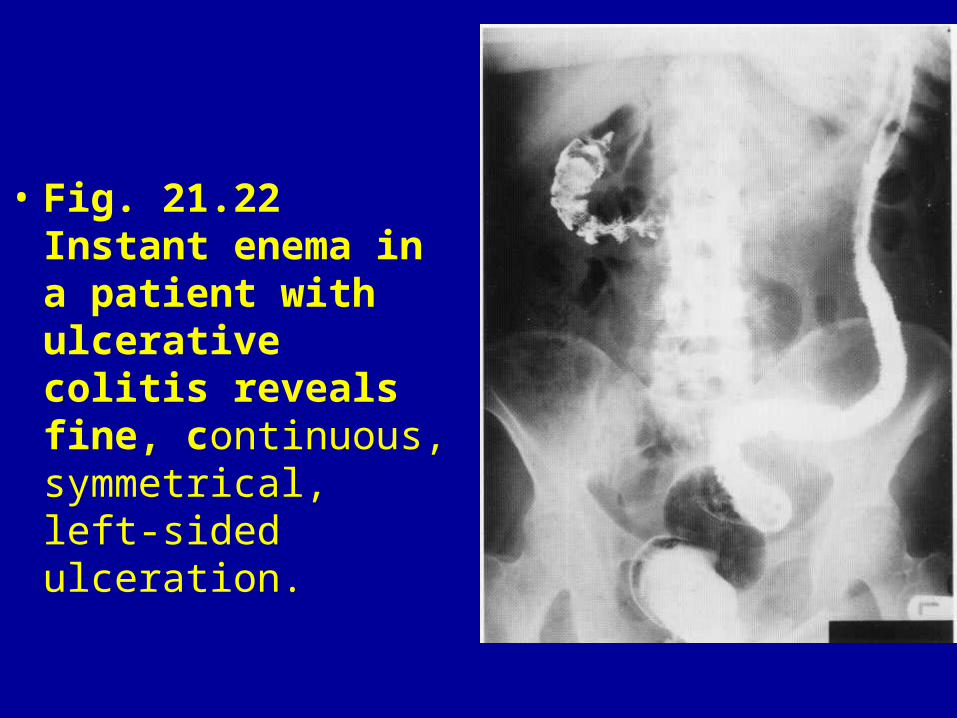
• Fig. 21.22 Instant enema in a patient with ulcerative colitis reveals fine, continuous, symmetrical, left-sided ulceration.
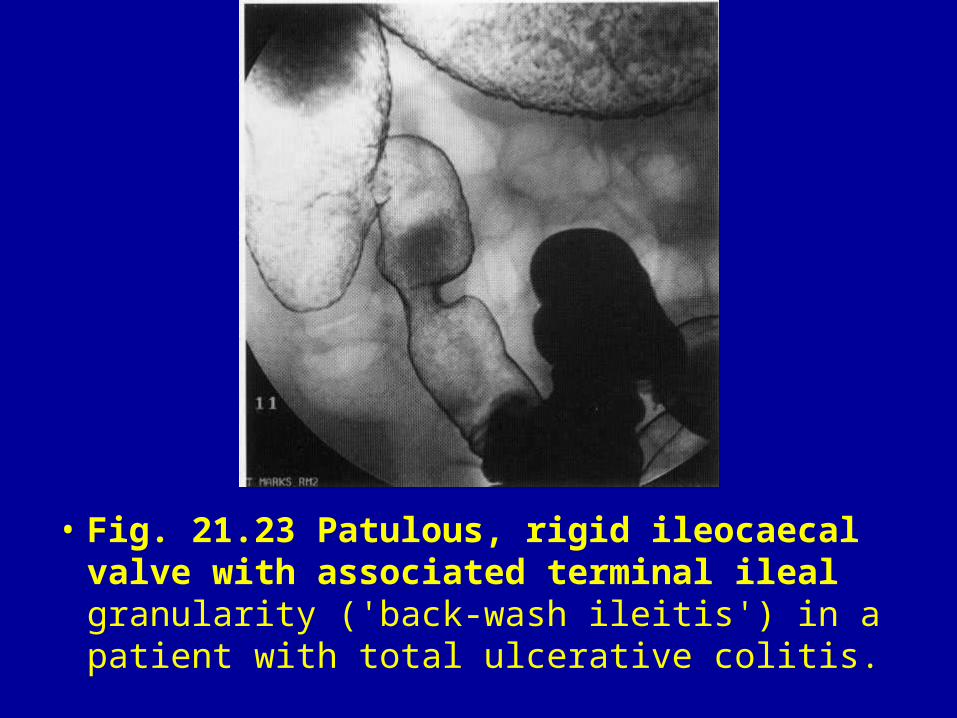
• Fig. 21.23 Patulous, rigid ileocaecal valve with associated terminal ileal granularity ('back-wash ileitis') in a patient with total ulcerative colitis.
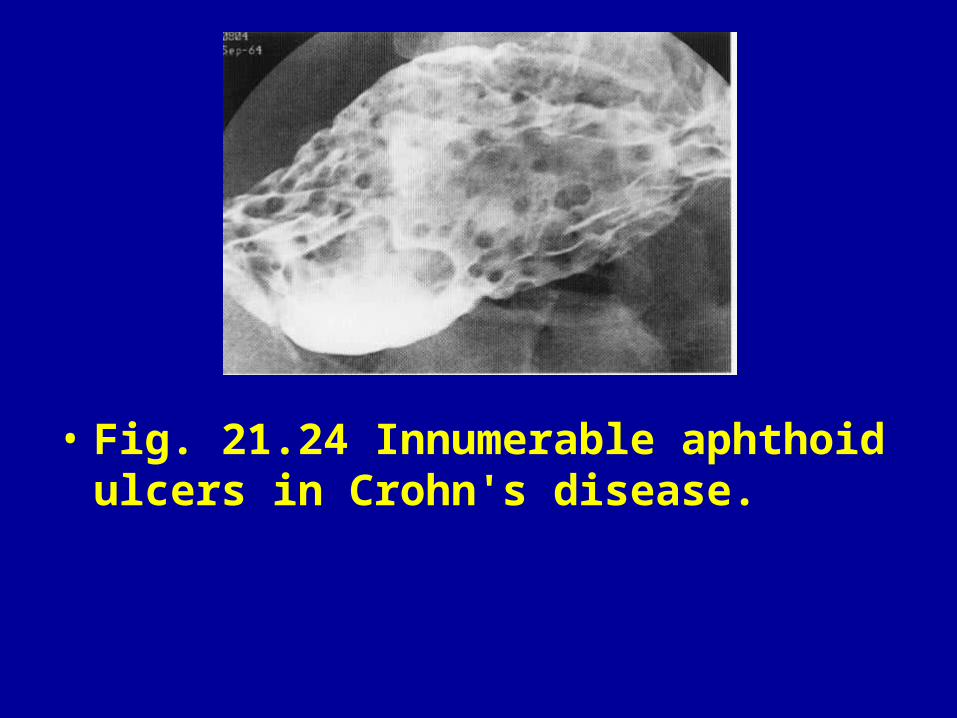
• Fig. 21.24 Innumerable aphthoid ulcers in Crohn's disease.
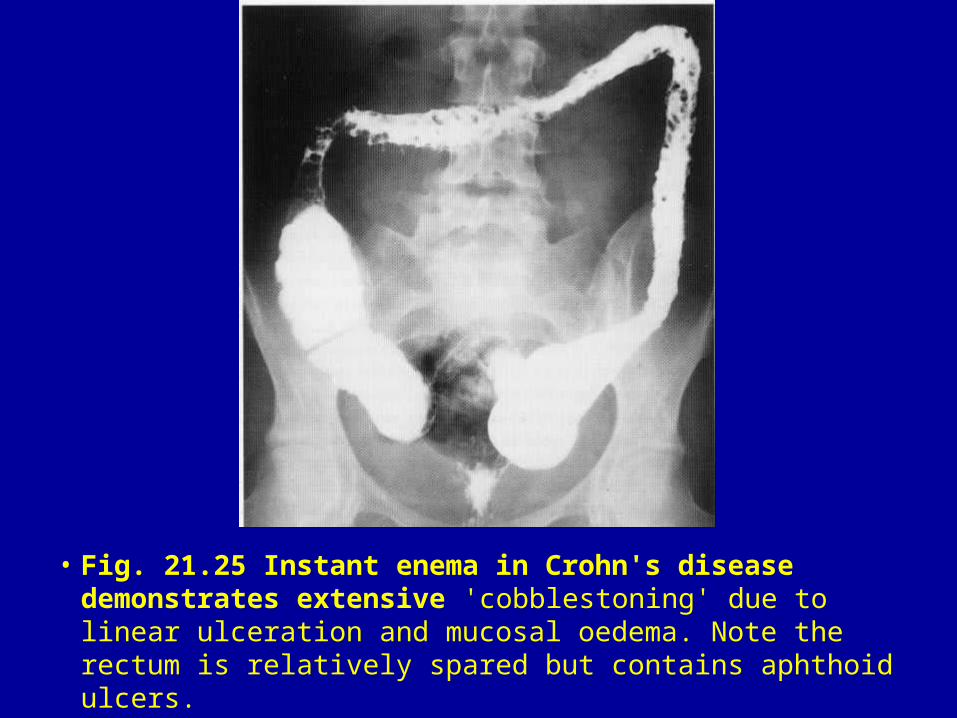
• Fig. 21.25 Instant enema in Crohn's disease demonstrates extensive 'cobblestoning' due to linear ulceration and mucosal oedema. Note the rectum is relatively spared but contains aphthoid ulcers.
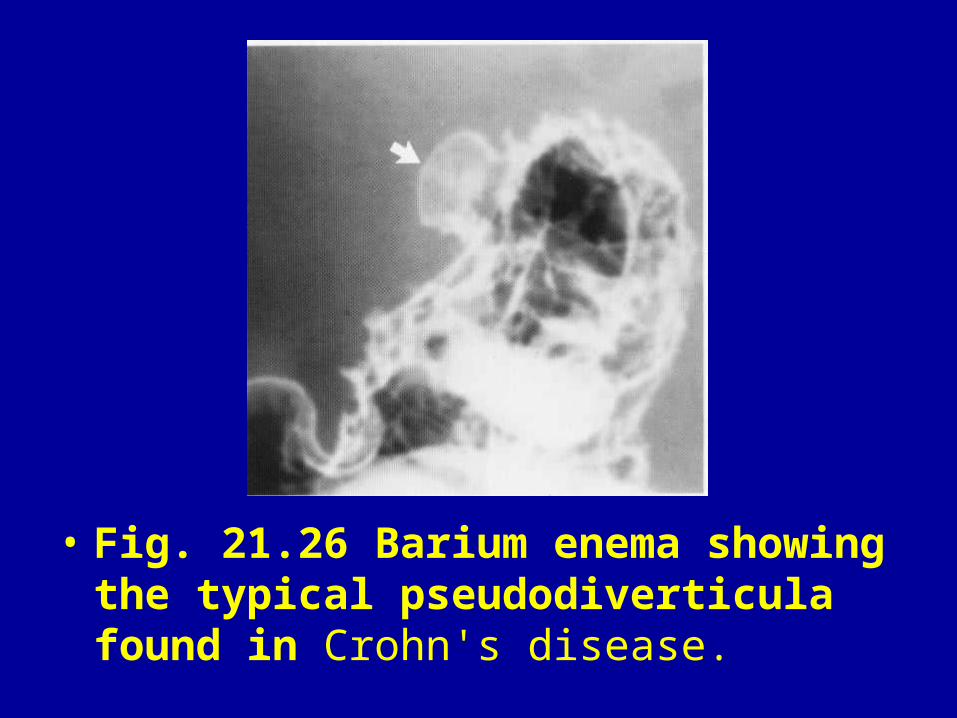
• Fig. 21.26 Barium enema showing the typical pseudodiverticula found in Crohn's disease.
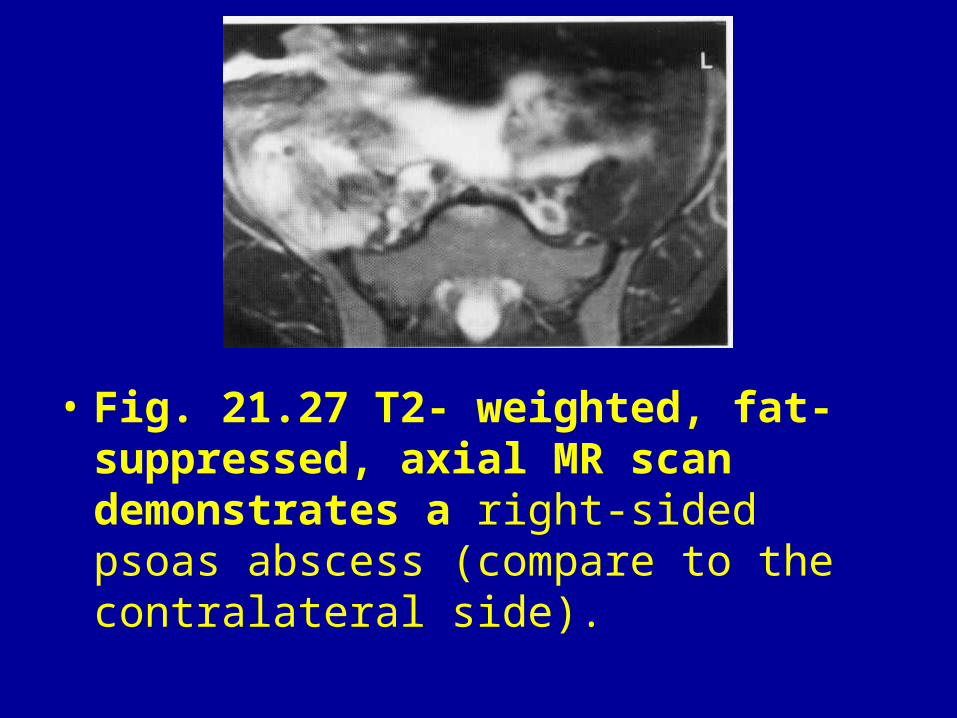
• Fig. 21.27 T2- weighted, fat-suppressed, axial MR scan demonstrates a right-sided psoas abscess (compare to the contralateral side).
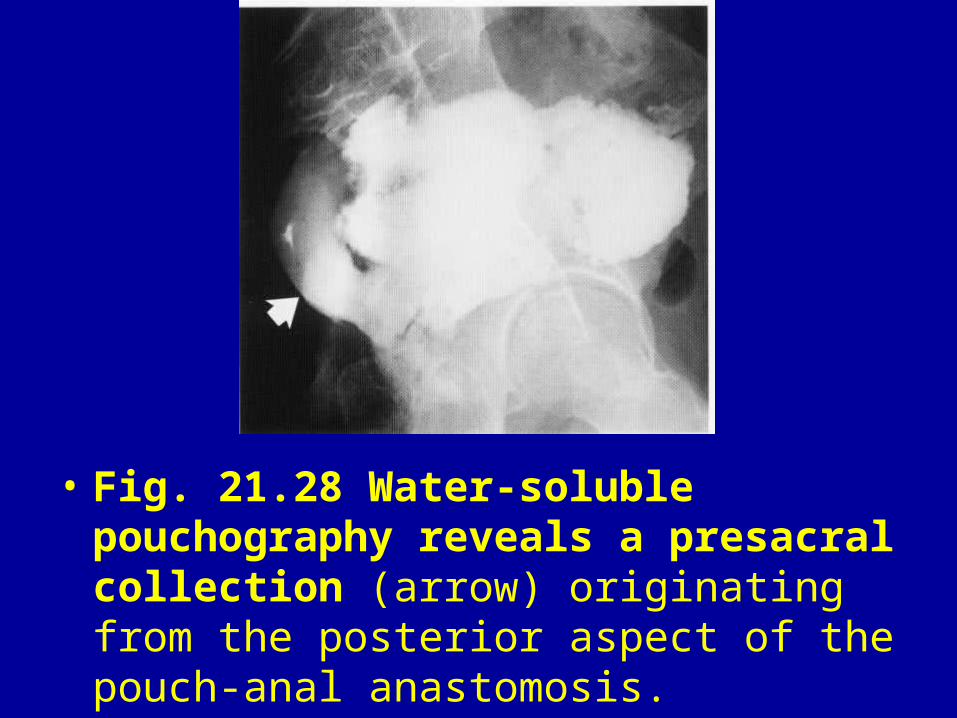
• Fig. 21.28 Water-soluble pouchography reveals a presacral collection (arrow) originating from the posterior aspect of the pouch-anal anastomosis.
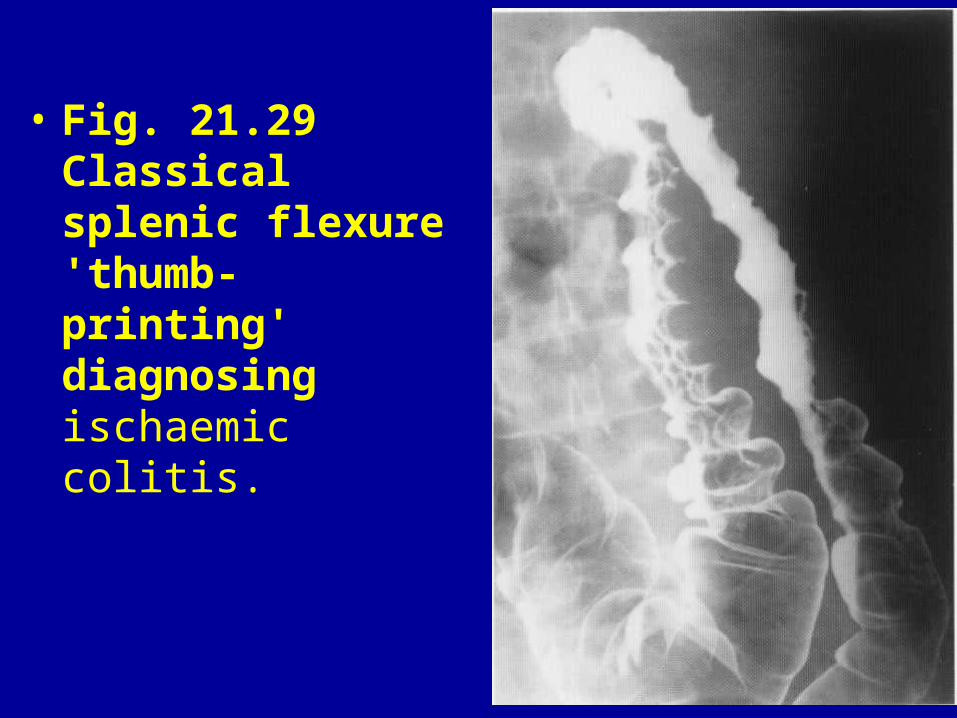
• Fig. 21.29 Classical splenic flexure 'thumb-printing' diagnosing ischaemic colitis.
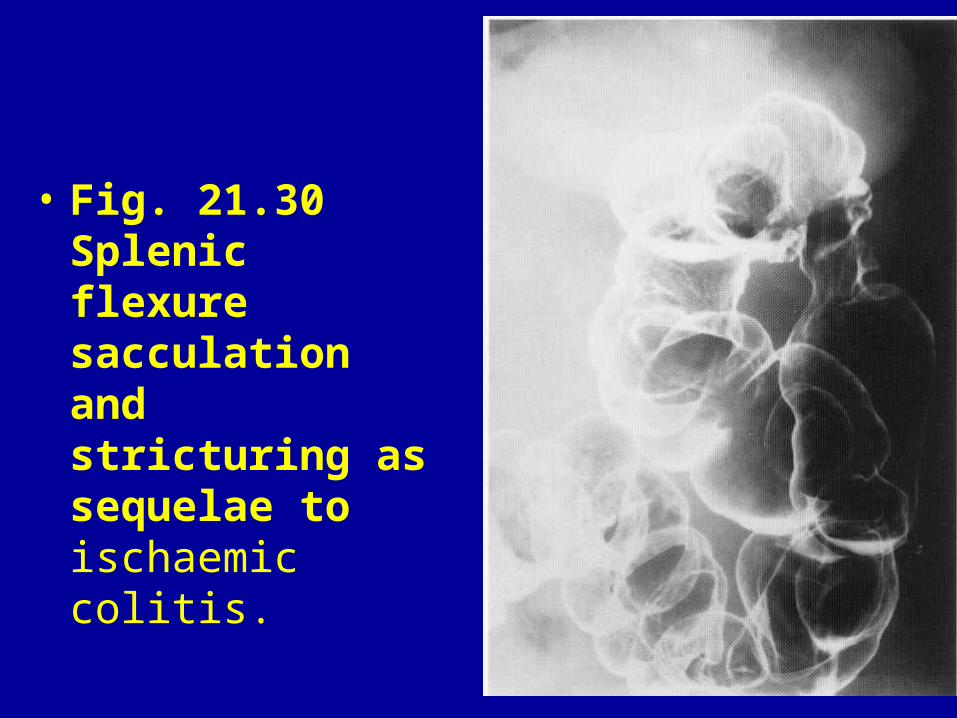
• Fig. 21.30 Splenic flexure sacculation and stricturing as sequelae to ischaemic colitis.
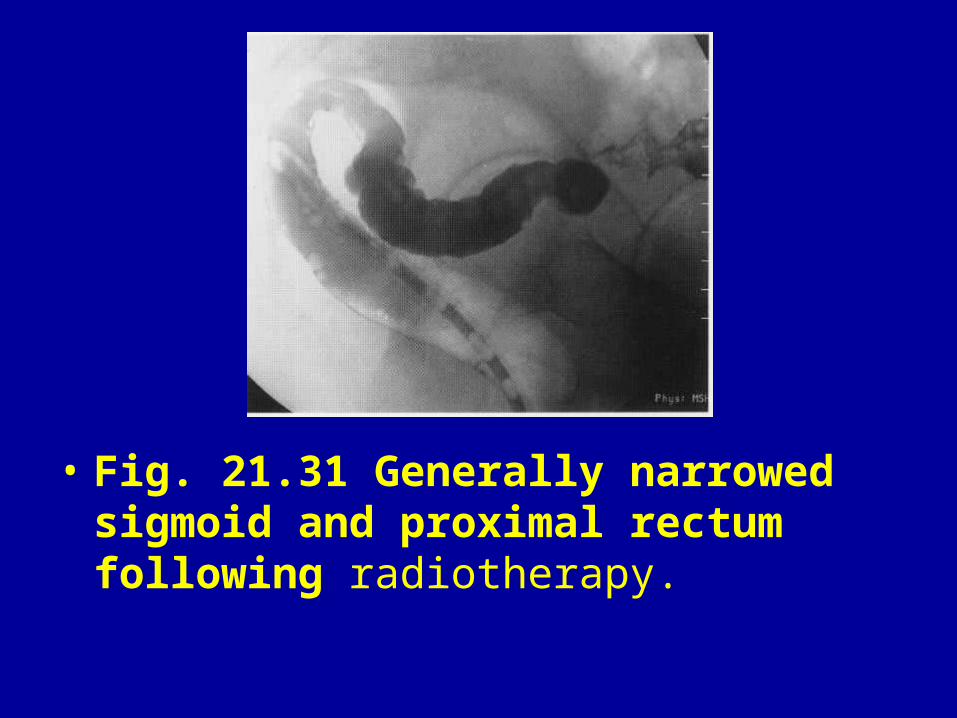
• Fig. 21.31 Generally narrowed sigmoid and proximal rectum following radiotherapy.
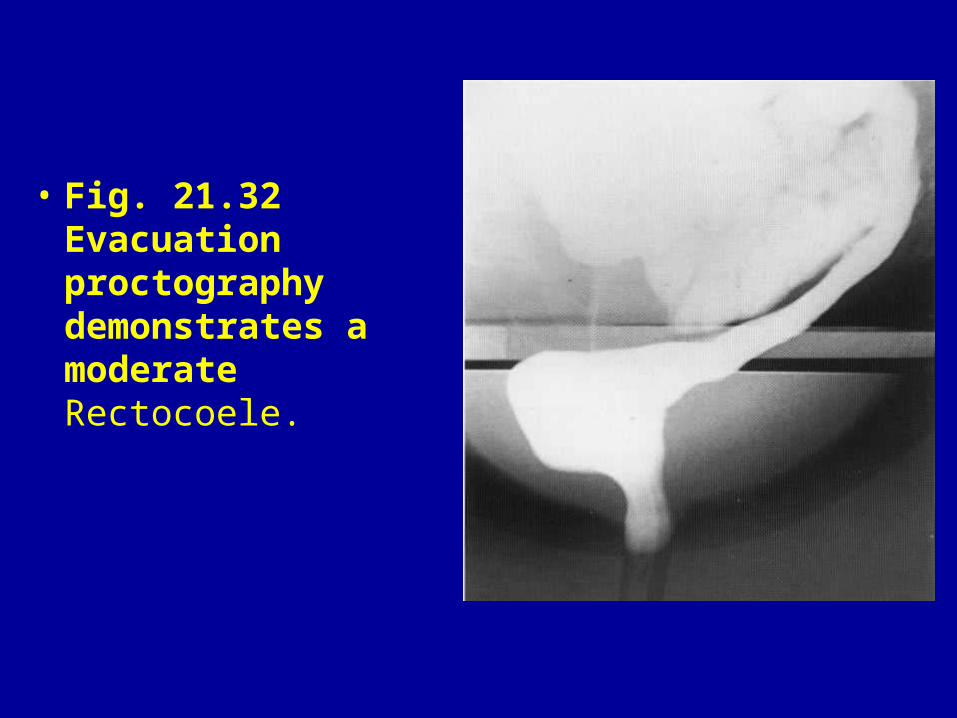
• Fig. 21.32 Evacuation proctography demonstrates a moderate Rectocoele.
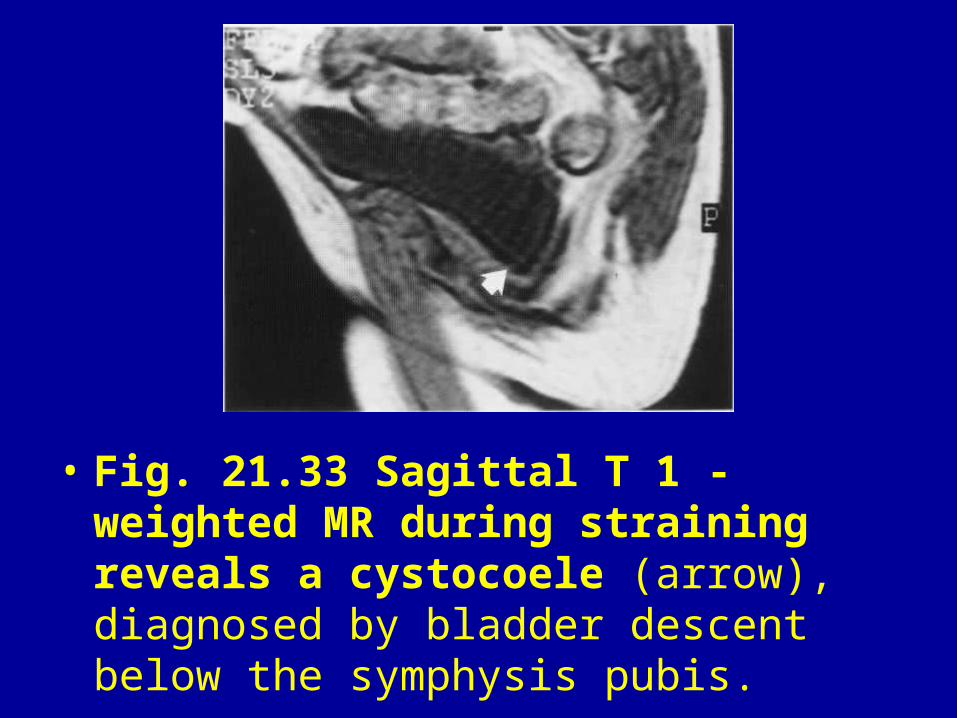
• Fig. 21.33 Sagittal T 1 -weighted MR during straining reveals a cystocoele (arrow), diagnosed by bladder descent below the symphysis pubis.
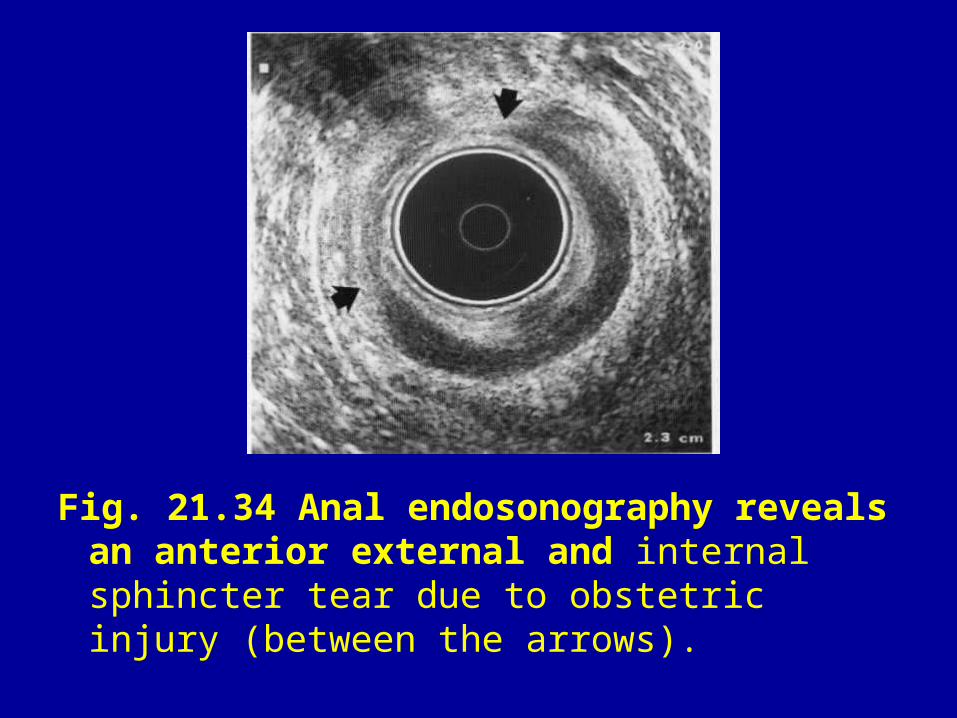
Fig. 21.34 Anal endosonography reveals an anterior external and internal sphincter tear due to obstetric injury (between the arrows).
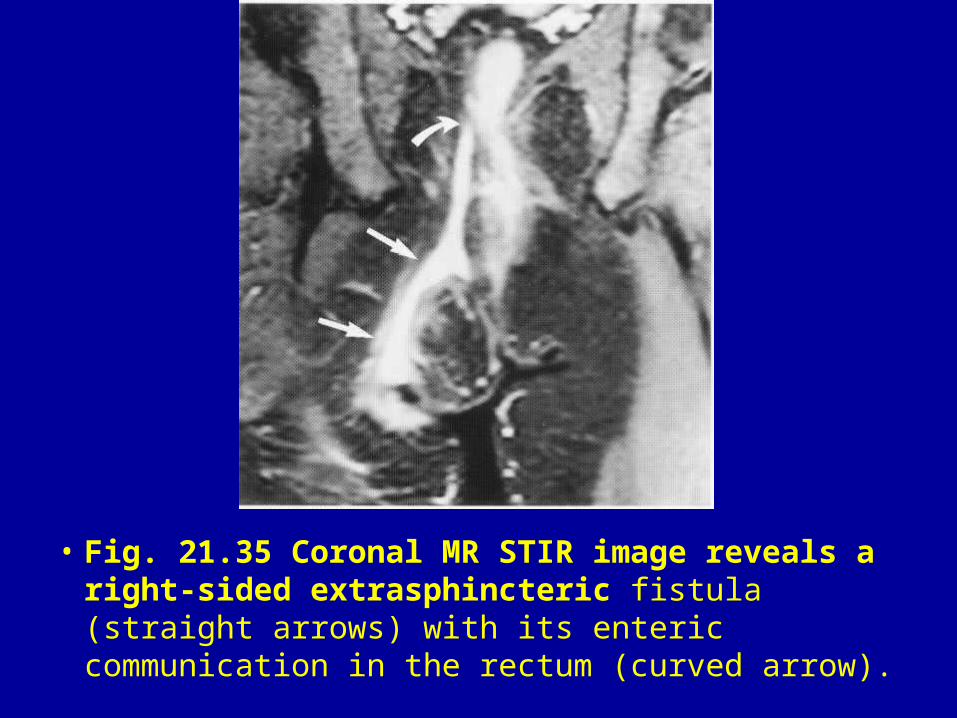
• Fig. 21.35 Coronal MR STIR image reveals a right-sided extrasphincteric fistula (straight arrows) with its enteric communication in the rectum (curved arrow).
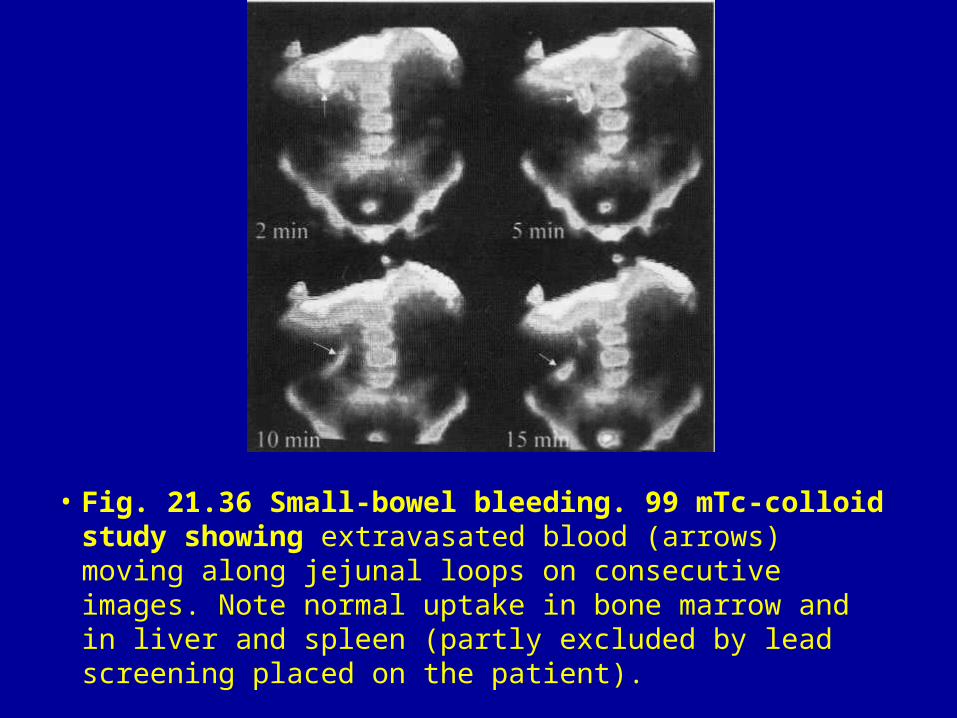
• Fig. 21.36 Small-bowel bleeding. 99 mTc-colloid study showing extravasated blood (arrows) moving along jejunal loops on consecutive images. Note normal uptake in bone marrow and in liver and spleen (partly excluded by lead screening placed on the patient).
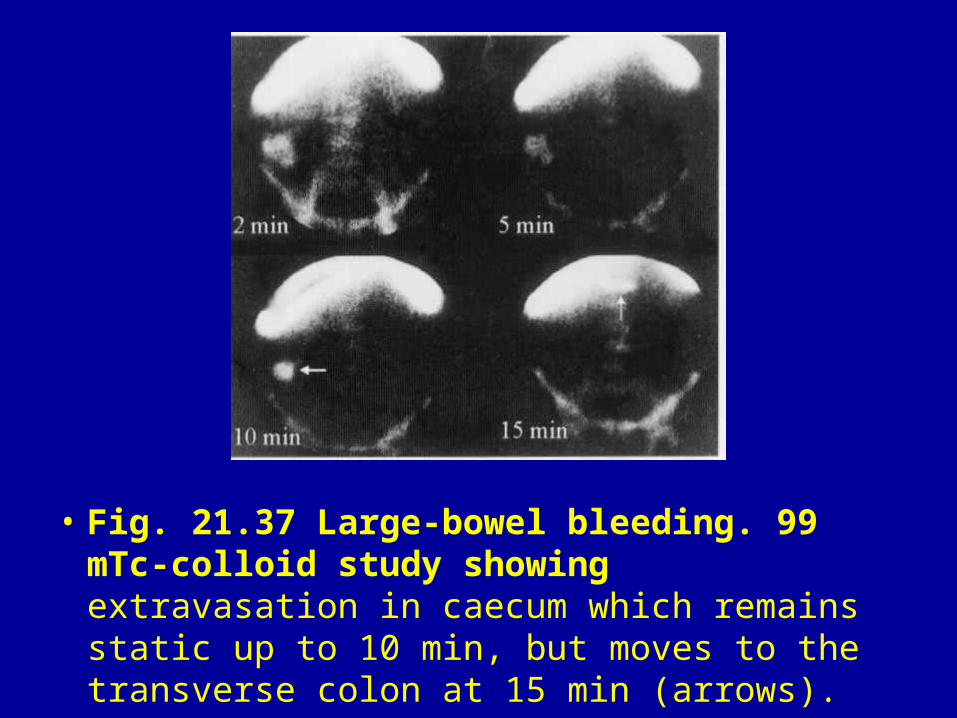
• Fig. 21.37 Large-bowel bleeding. 99 mTc-colloid study showing extravasation in caecum which remains static up to 10 min, but moves to the transverse colon at 15 min (arrows).
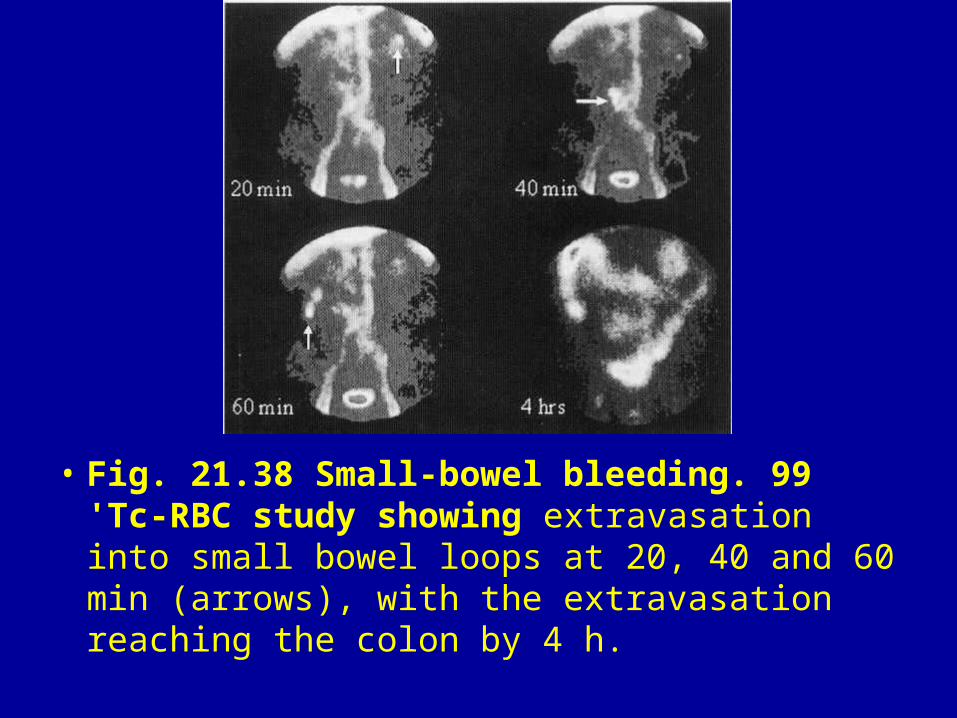
• Fig. 21.38 Small-bowel bleeding. 99 'Tc-RBC study showing extravasation into small bowel loops at 20, 40 and 60 min (arrows), with the extravasation reaching the colon by 4 h.
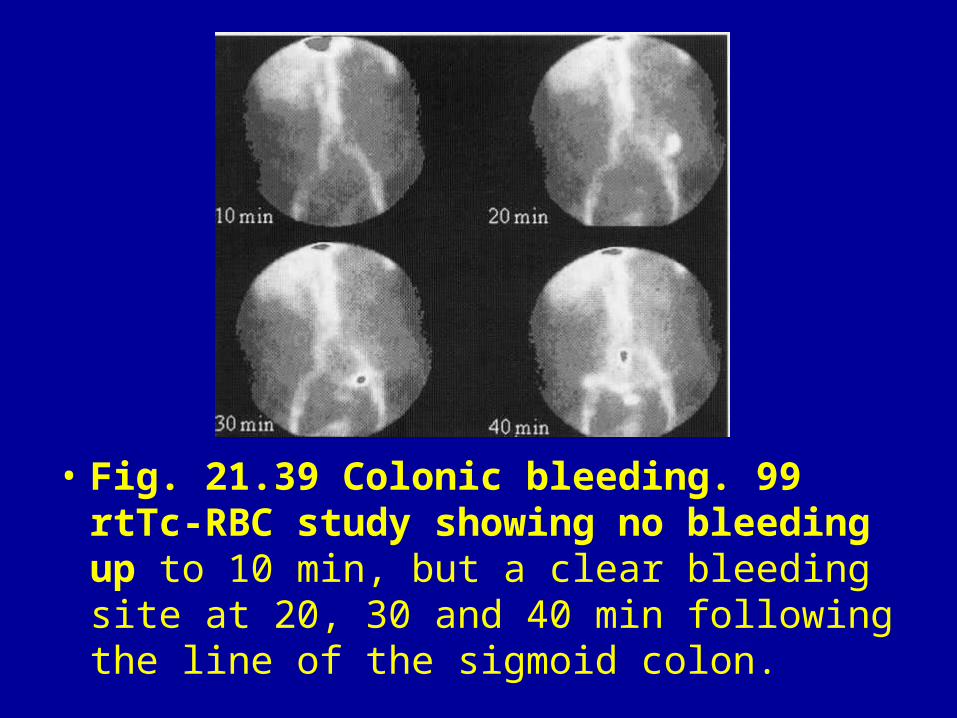
• Fig. 21.39 Colonic bleeding. 99 rtTc-RBC study showing no bleeding up to 10 min, but a clear bleeding site at 20, 30 and 40 min following the line of the sigmoid colon.
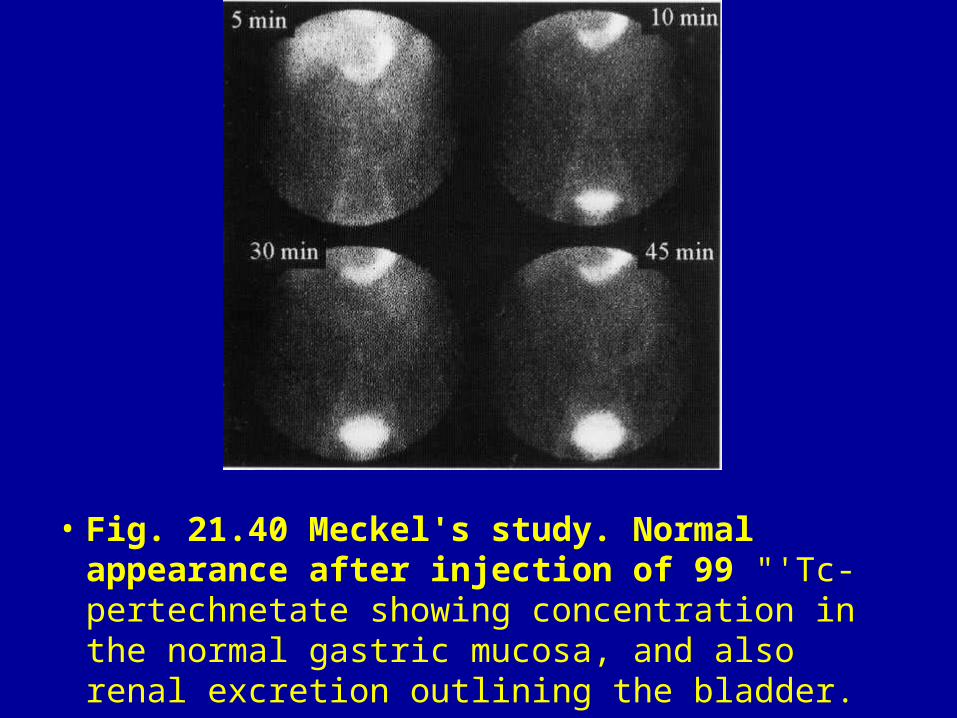
• Fig. 21.40 Meckel's study. Normal appearance after injection of 99 "'Tc-pertechnetate showing concentration in the normal gastric mucosa, and also renal excretion outlining the bladder.
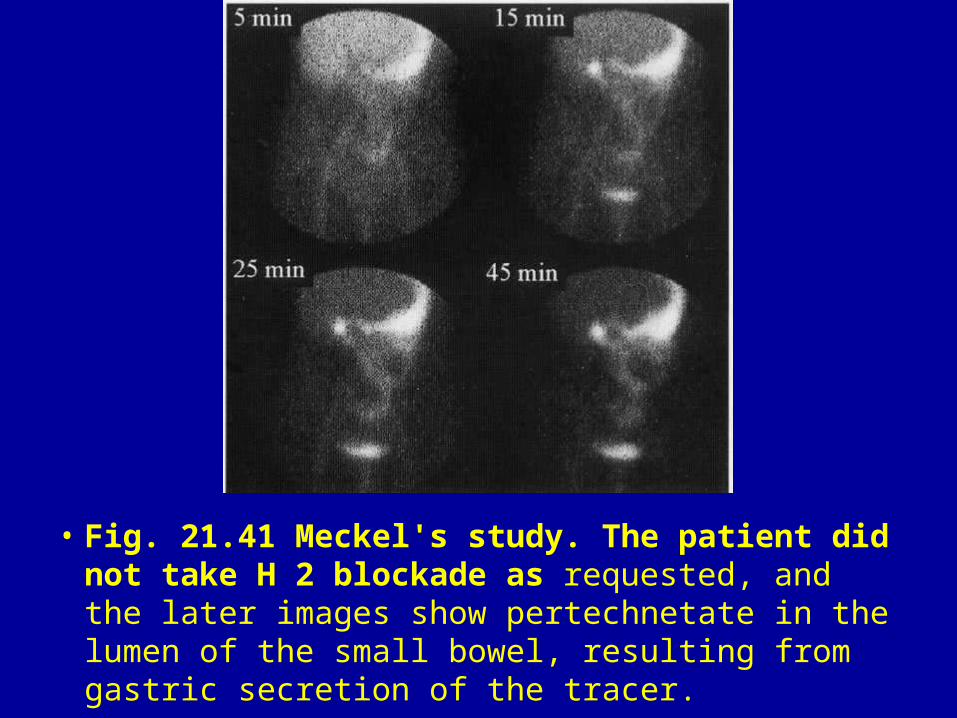
• Fig. 21.41 Meckel's study. The patient did not take H 2 blockade as requested, and the later images show pertechnetate in the lumen of the small bowel, resulting from gastric secretion of the tracer.
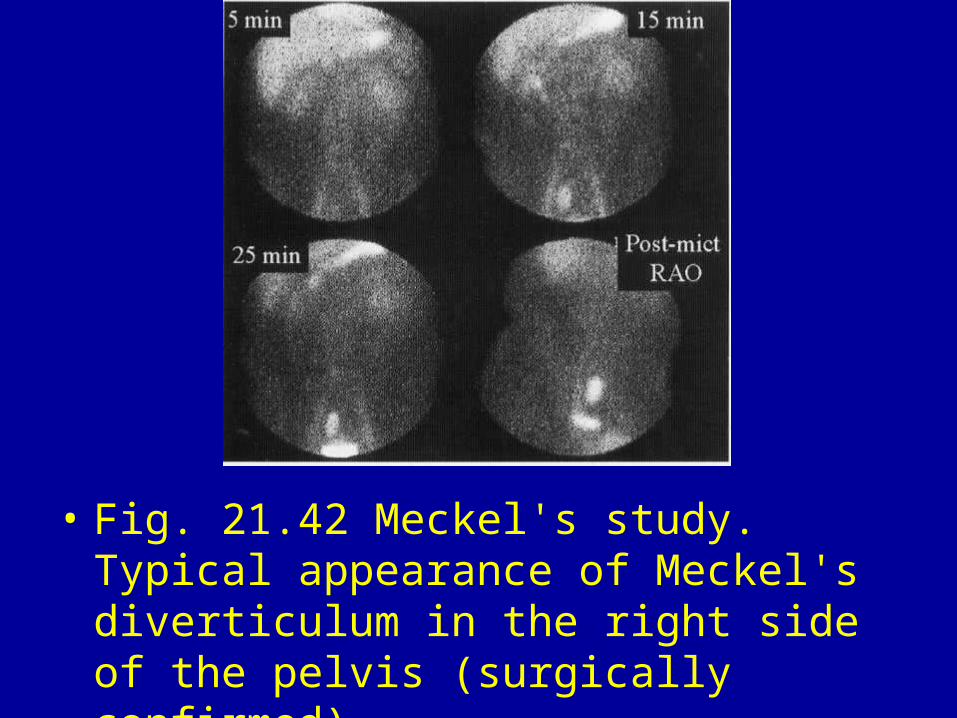
• Fig. 21.42 Meckel's study. Typical appearance of Meckel's diverticulum in the right side of the pelvis (surgically confirmed).
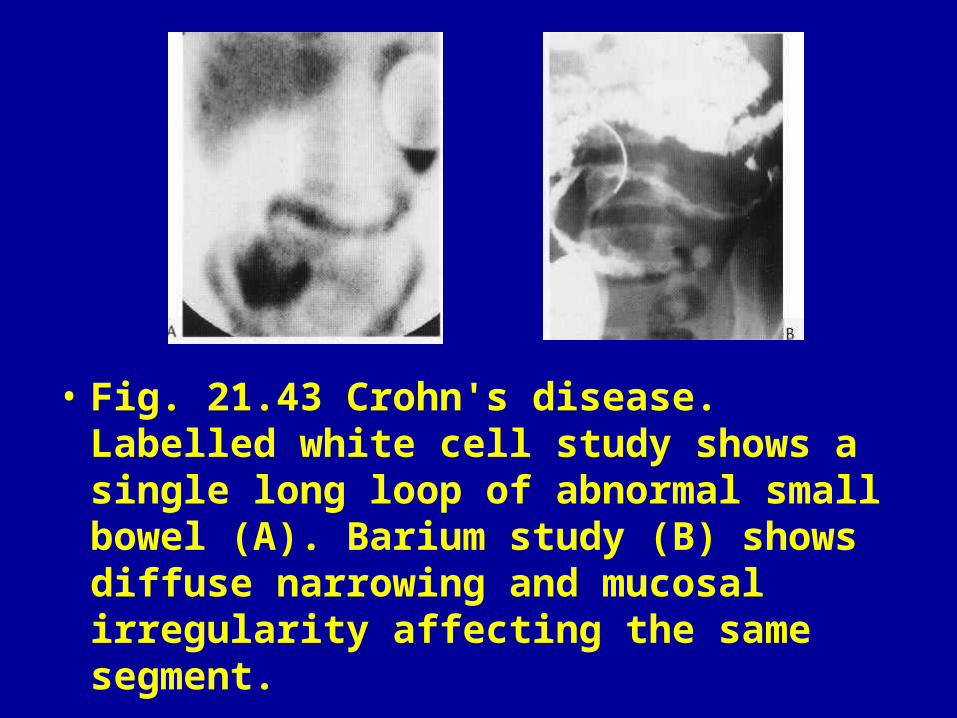
• Fig. 21.43 Crohn's disease. Labelled white cell study shows a single long loop of abnormal small bowel (A). Barium study (B) shows diffuse narrowing and mucosal irregularity affecting the same segment.
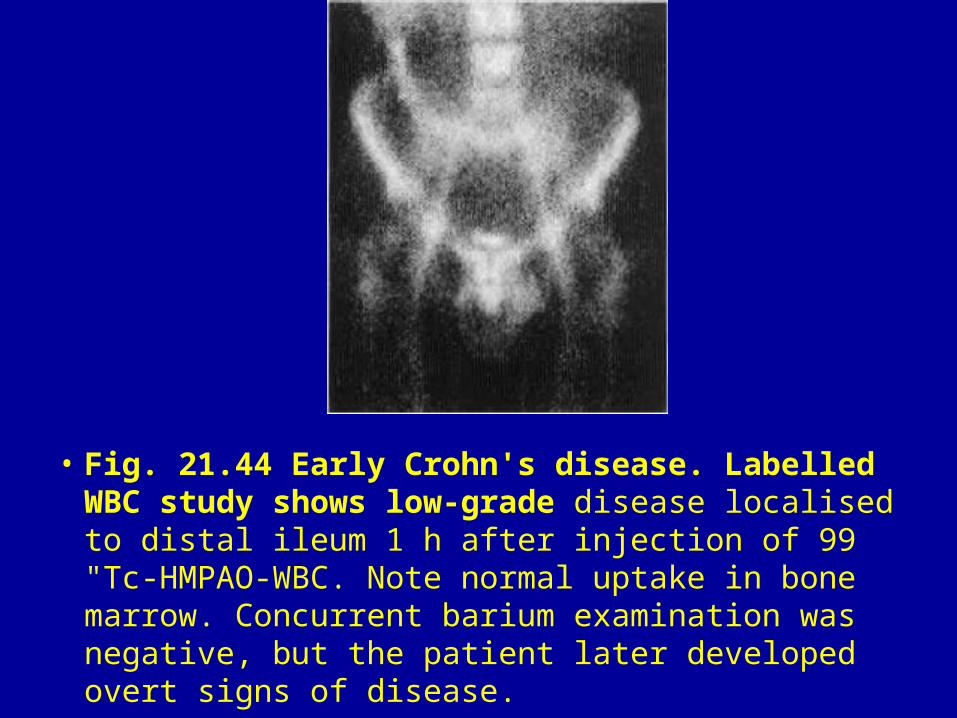
• Fig. 21.44 Early Crohn's disease. Labelled WBC study shows low-grade disease localised to distal ileum 1 h after injection of 99 "Tc-HMPAO-WBC. Note normal uptake in bone marrow. Concurrent barium examination was negative, but the patient later developed overt signs of disease.
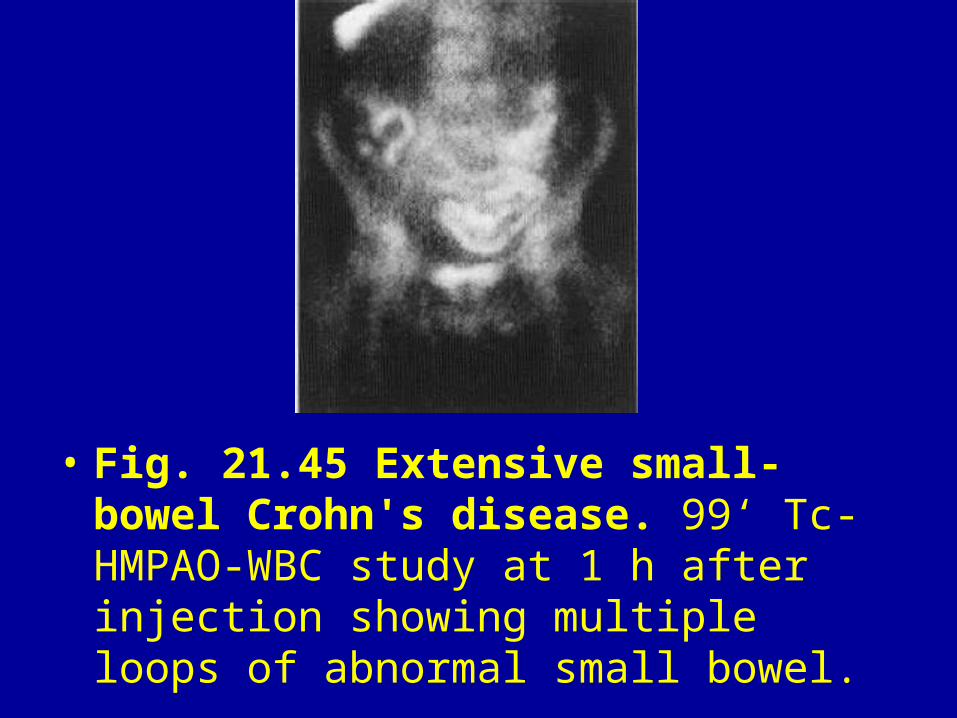
• Fig. 21.45 Extensive small-bowel Crohn's disease. 99‘ Tc-HMPAO-WBC study at 1 h after injection showing multiple loops of abnormal small bowel.
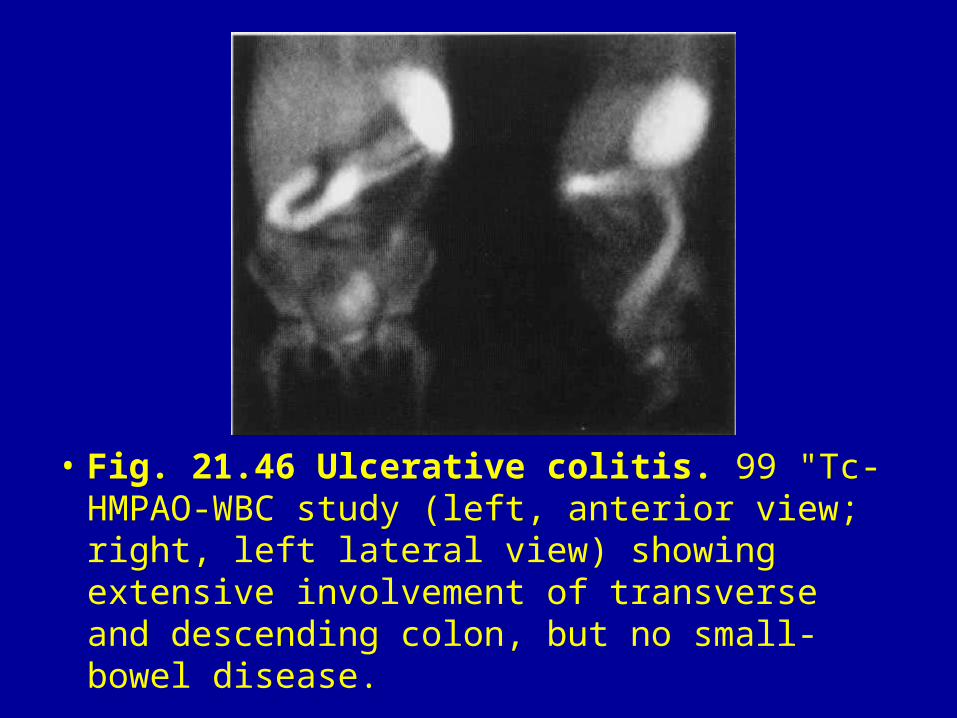
• Fig. 21.46 Ulcerative colitis. 99 "Tc-HMPAO-WBC study (left, anterior view; right, left lateral view) showing extensive involvement of transverse and descending colon, but no small-bowel disease.
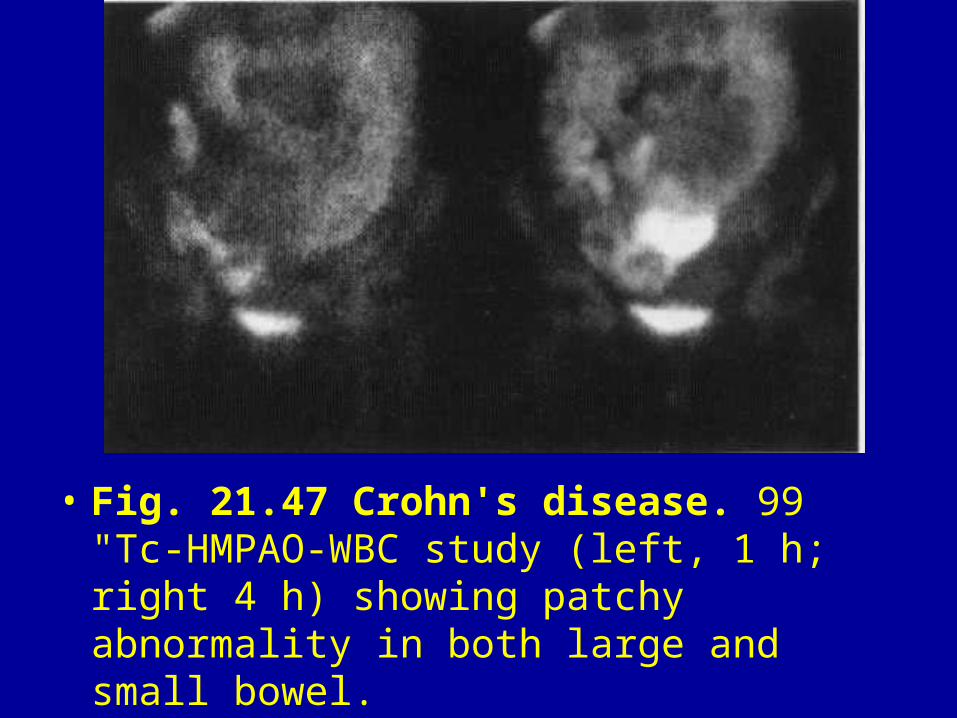
• Fig. 21.47 Crohn's disease. 99 "Tc-HMPAO-WBC study (left, 1 h; right 4 h) showing patchy abnormality in both large and small bowel.
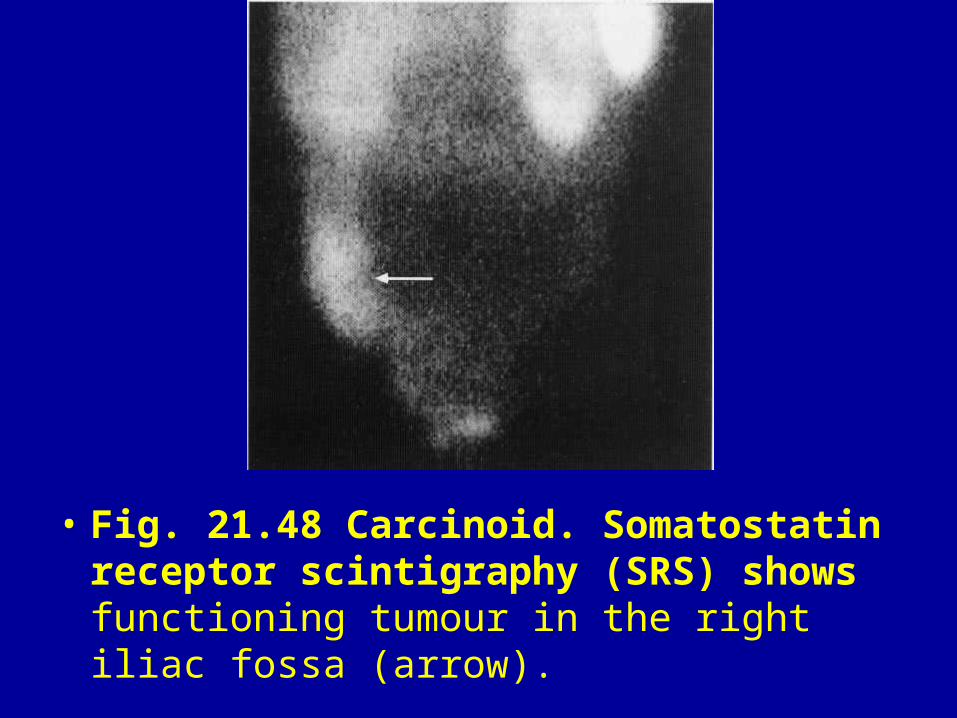
• Fig. 21.48 Carcinoid. Somatostatin receptor scintigraphy (SRS) shows functioning tumour in the right iliac fossa (arrow).
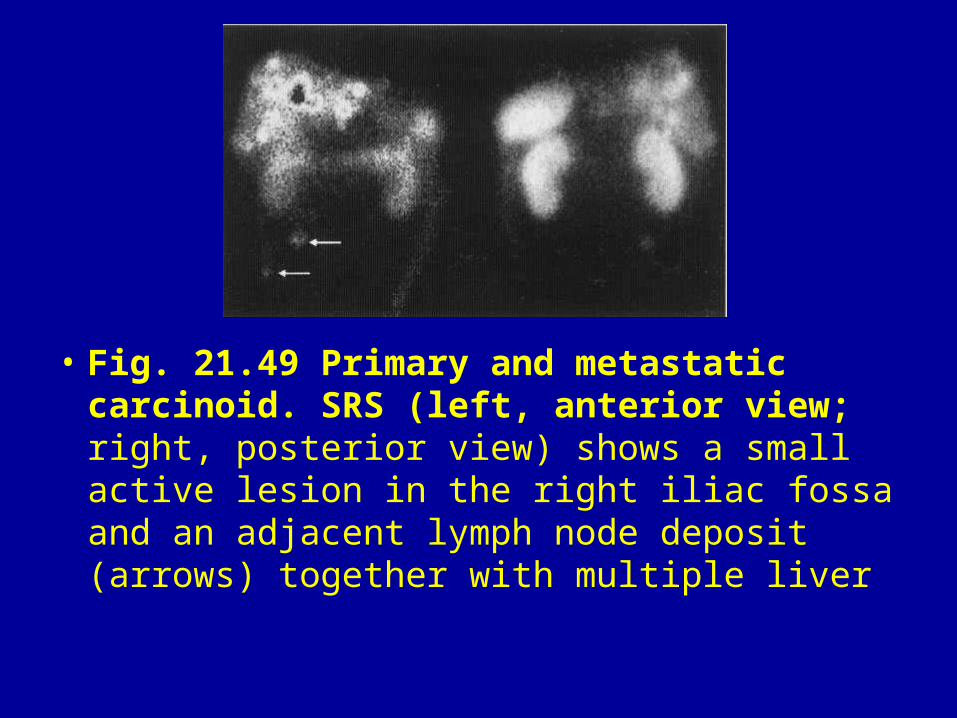
• Fig. 21.49 Primary and metastatic carcinoid. SRS (left, anterior view; right, posterior view) shows a small active lesion in the right iliac fossa and an adjacent lymph node deposit (arrows) together with multiple liver
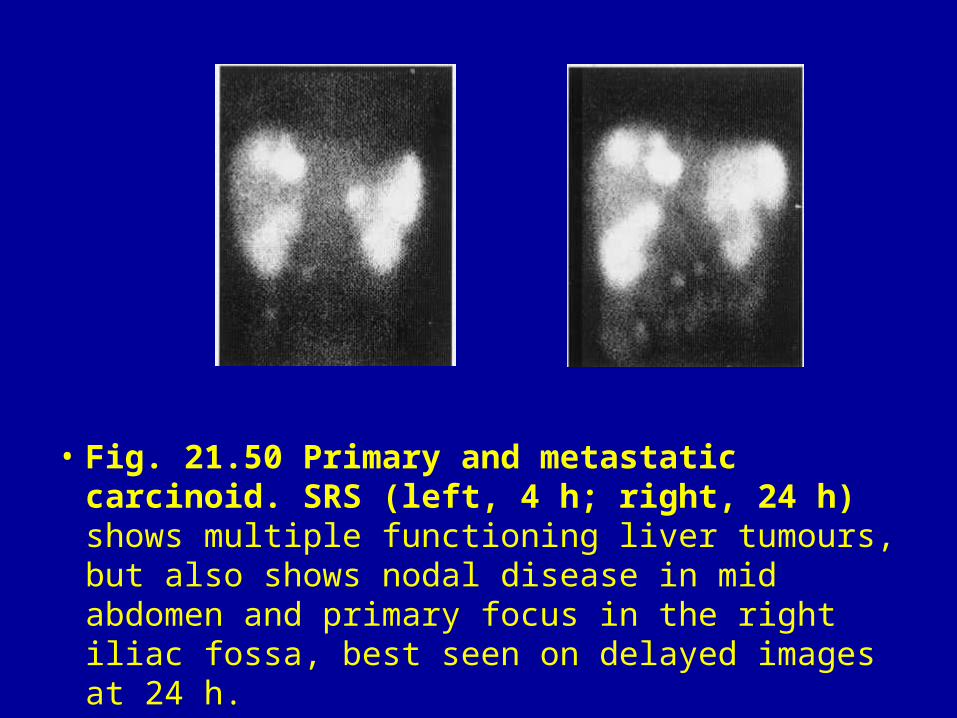
• Fig. 21.50 Primary and metastatic carcinoid. SRS (left, 4 h; right, 24 h) shows multiple functioning liver tumours, but also shows nodal disease in mid abdomen and primary focus in the right iliac fossa, best seen on delayed images at 24 h.