Embed Size (px)
Citation preview

PATTERNS OF FAILURE AND TREATMENT RELATED TOXICITY IN ADVANCED
CERVICAL CANCER PATIENTS TREATED USING EXTENDED FIELD RT WITH
CURATIVE INTENT
ABHIJIT DAS 2ND YEAR PGT DEPARTMENT OF RADIATION ONCOLOGYAHRCC
AIMS AND OBJECTIVES:
• Efficacy of CTRT in cervical cancer patients treated with EFRT.
• patterns of failure in these patients
• Treatment related toxicity
Methods & materials:Nature of study: retrospectivePlace of study: PETER MCCULLUM CANCER CENTRE, Melbourne , Australia
TIME PERIOD: JANUARY 1996 TO JUNE 2007
TOTAL NO PATIENTS : 39 PATIENTS
PATIENTS SELECTION CRITERIA:• untreated patients with diagnosis of locally advanced ca cervix planned for
definitive RT.• Histopathology may be squamous cell carcinoma/ adenocarcinoma. ( clear cell ,
endometriod carcinoma and mucinous carcinoma.)• Evidence of metastasis in common iliac / para aortic nodes (imaging e.g PET CT
and by surgical staging- laparotomy.)• FIGO staging IB – IIIB• All are treated with EFRT with curative intent.
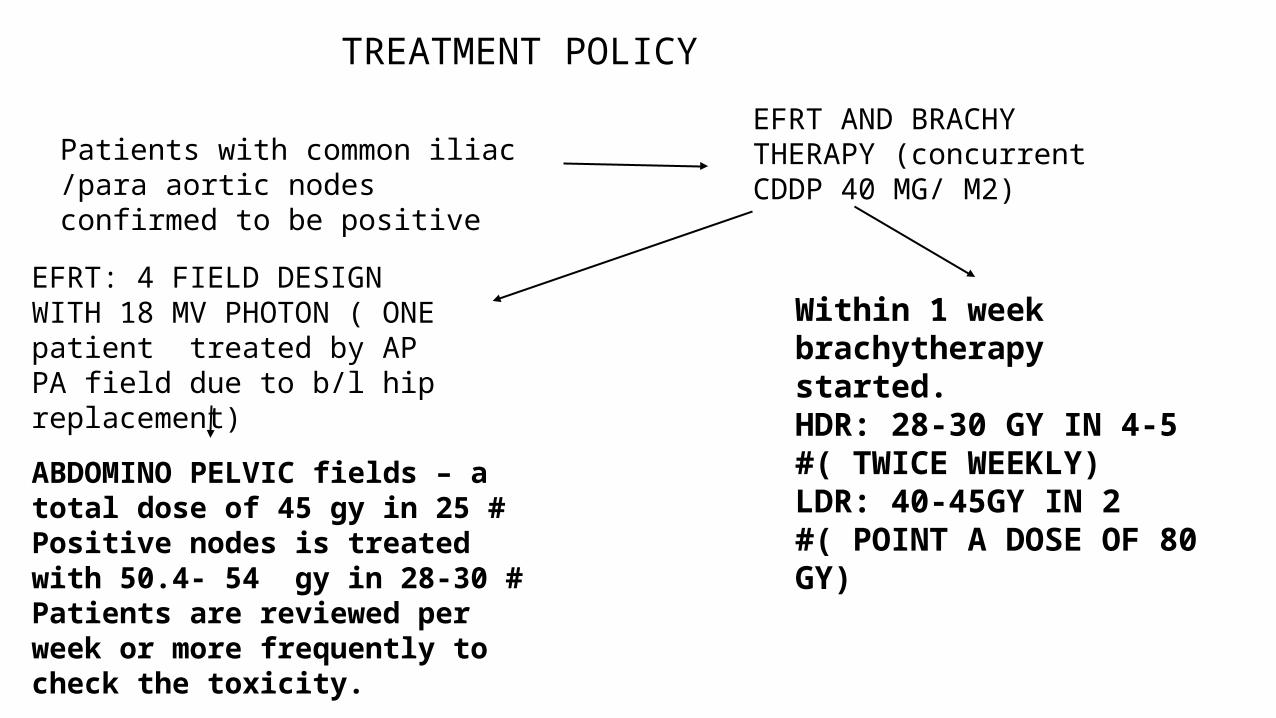
TREATMENT POLICY
Patients with common iliac /para aortic nodes confirmed to be positive
EFRT AND BRACHY THERAPY (concurrent CDDP 40 MG/ M2)
EFRT: 4 FIELD DESIGN WITH 18 MV PHOTON ( ONE patient treated by AP PA field due to b/l hip replacement)
ABDOMINO PELVIC fields – a total dose of 45 gy in 25 #Positive nodes is treated with 50.4- 54 gy in 28-30 # Patients are reviewed per week or more frequently to check the toxicity.
Within 1 week brachytherapy started.HDR: 28-30 GY IN 4-5 #( TWICE WEEKLY)LDR: 40-45GY IN 2 #( POINT A DOSE OF 80 GY)
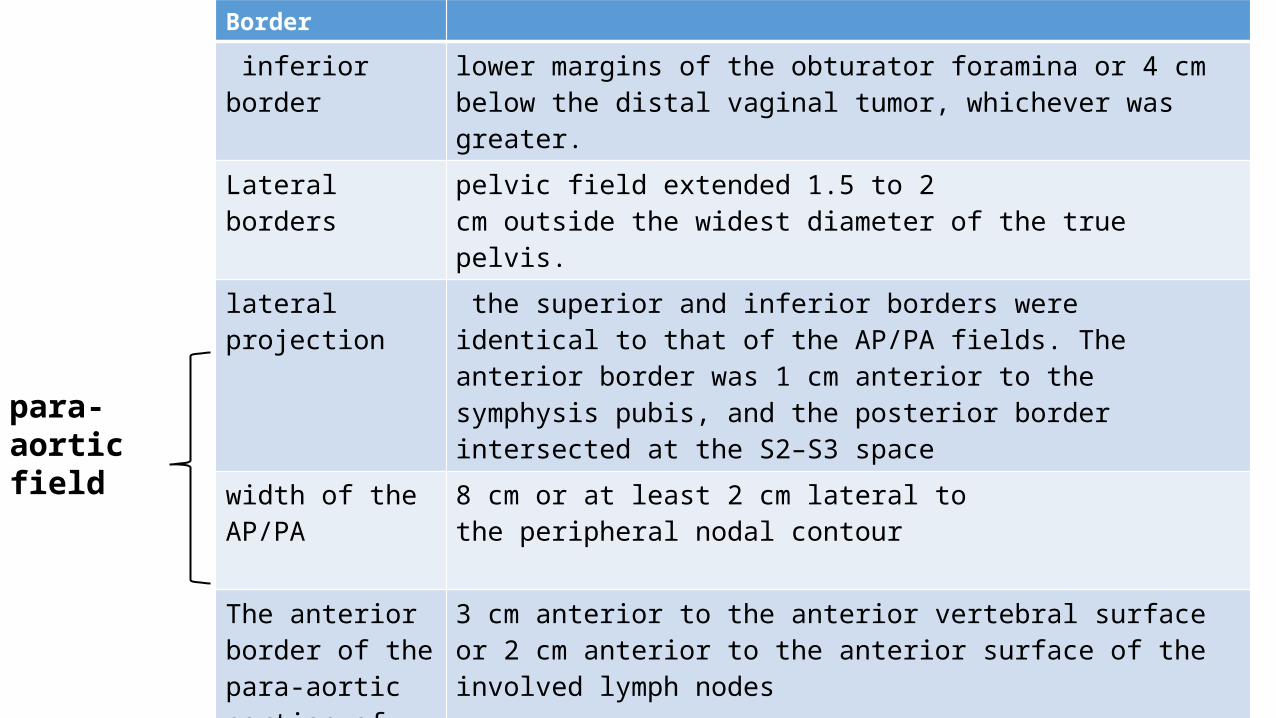
Border
inferior border lower margins of the obturator foramina or 4 cm below the distal vaginal tumor, whichever was greater.
Lateral borders pelvic field extended 1.5 to 2cm outside the widest diameter of the true pelvis.
lateral projection the superior and inferior borders wereidentical to that of the AP/PA fields. The anterior border was 1 cm anterior to the symphysis pubis, and the posterior border intersected at the S2–S3 space
width of the AP/PA 8 cm or at least 2 cm lateral tothe peripheral nodal contour
The anterior border of the para-aortic portion of the field
3 cm anterior to the anterior vertebral surface or 2 cm anterior to the anterior surface of the involved lymph nodes
Thirty-three (85%) patients were treated up to the vertebral junction between T12 and L1. Three patients were treated up to the L2– L3 vertebral intersection and 3 patients up to the L3–L4 vertebral intersection
para-aortic field

FOLLOW UP TIME PERIOD INVESTIGATIONS
1ST 4-6 Wks after RT Every 6 months post RT PET repeated.Patients having suspected of recurrence is examined using PET as appropriate.
During 1st year Every 3 months
During 2nd & 3rd year Every 4 months
4th & 5th years Every 6 months
After 5 yrs. Yearly visit
At each follow up a form is filled up using disease status & late complications.( using RTOG toxicity criteria: ACUTE TOXICITY is defined as toxicity within 3 months of start of RT. LATE TOXICITY is defined as toxicity after 3 months of start of RT.)

Criteria for assessing outcomes:
Failure Either persistent disease/ recurrence of disease following RT
Date of failure Date of sign of any of these failure either clinical or imaging
Site of failure Nodal relapse: Either in field /outside the treatment field
Distant failure: Any failure outside the treated failure including supraclav / mediastinal nodes.
Local: Residual/ recurrent disease at cervic /uterus
Overall survival
Time of beginning of treatment to death due to any cause
Disease free survival
Time of beginning of treatment to failure or death as aresult of of disease progression
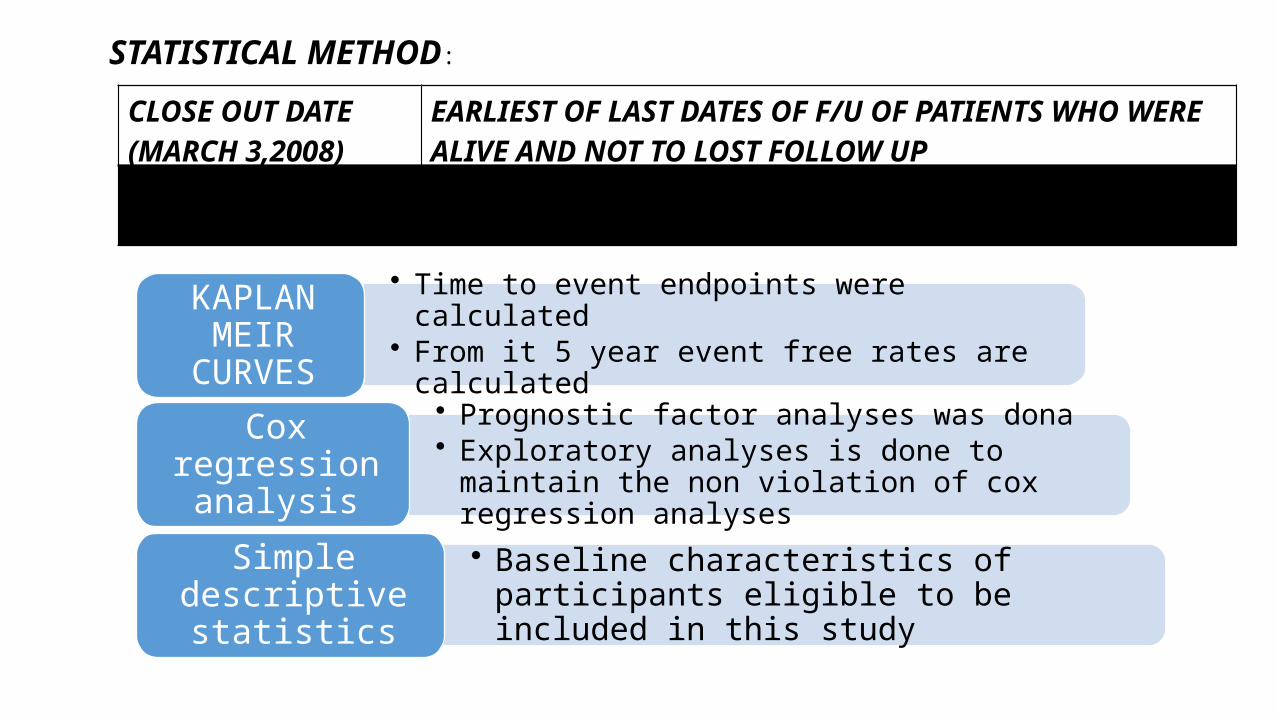
STATISTICAL METHOD:
• Time to event endpoints were calculated• From it 5 year event free rates are calculated
KAPLAN MEIR CURVES
• Prognostic factor analyses was dona• Exploratory analyses is done to maintain the non
violation of cox regression analyses
Cox regression analysis
• Baseline characteristics of participants eligible to be included in this study
Simple descriptive statistics
CLOSE OUT DATE(MARCH 3,2008)
EARLIEST OF LAST DATES OF F/U OF PATIENTS WHO WERE ALIVE AND NOT TO LOST FOLLOW UP
FOLLOW UP TIME TIME OF STUDY ENTRY TO ( COMMENCEMENT OF EFRT) TO THE LAST DATE OF KNOWN F/U OR THE DATE OF CLOSE OUT
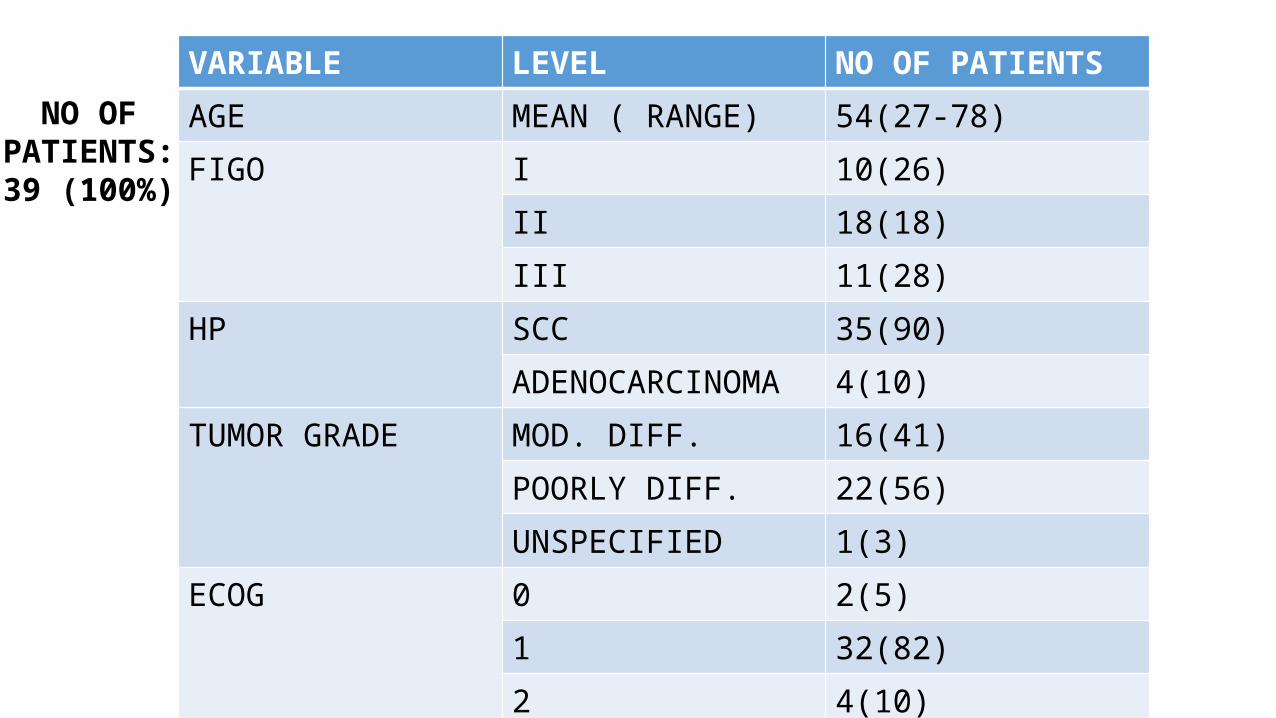
VARIABLE LEVEL NO OF PATIENTSAGE MEAN ( RANGE) 54(27-78)FIGO I 10(26)
II 18(18)III 11(28)
HP SCC 35(90)ADENOCARCINOMA 4(10)
TUMOR GRADE MOD. DIFF. 16(41)POORLY DIFF. 22(56)UNSPECIFIED 1(3)
ECOG 0 2(5)1 32(82)2 4(10)3 1(3)
NO OF PATIENTS: 39
(100%)
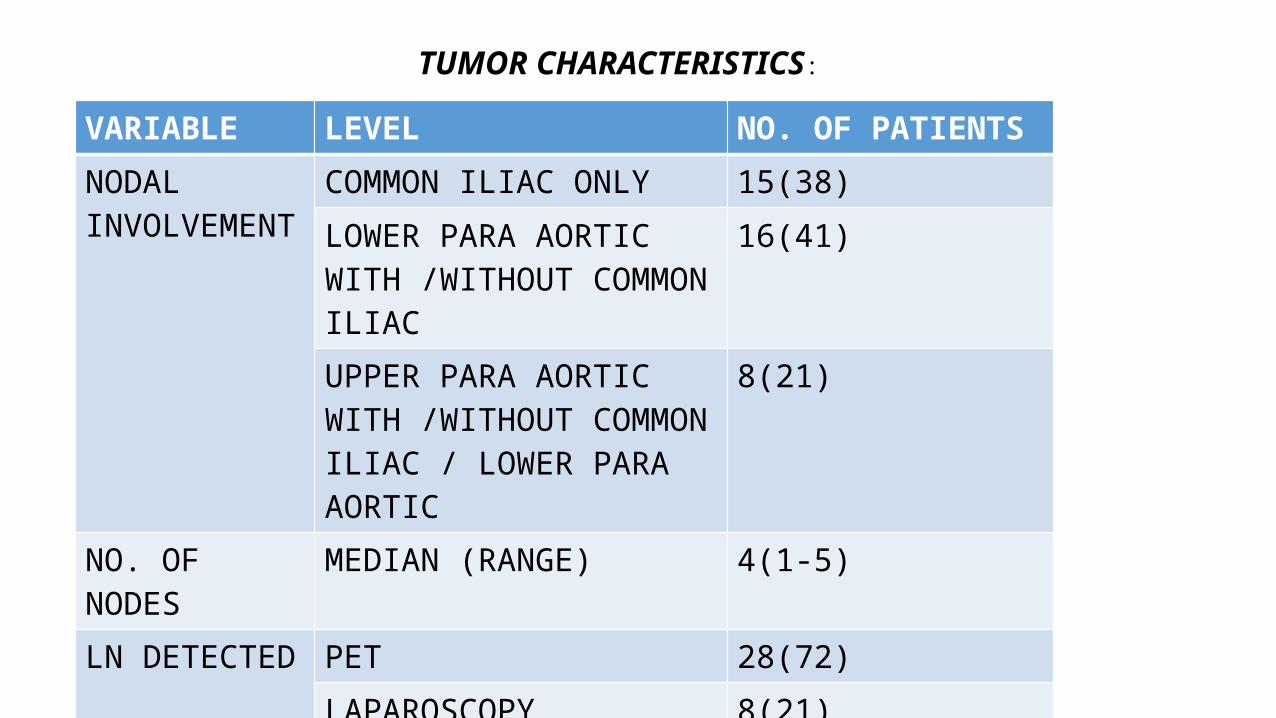
VARIABLE LEVEL NO. OF PATIENTS
NODAL INVOLVEMENT
COMMON ILIAC ONLY 15(38)
LOWER PARA AORTIC WITH /WITHOUT COMMON ILIAC
16(41)
UPPER PARA AORTIC WITH /WITHOUT COMMON ILIAC / LOWER PARA AORTIC
8(21)
NO. OF NODES MEDIAN (RANGE) 4(1-5)
LN DETECTED PET 28(72)
LAPAROSCOPY 8(21)
PET/ LAPAROSCOPY 3(7)
TUMOR CHARACTERISTICS:
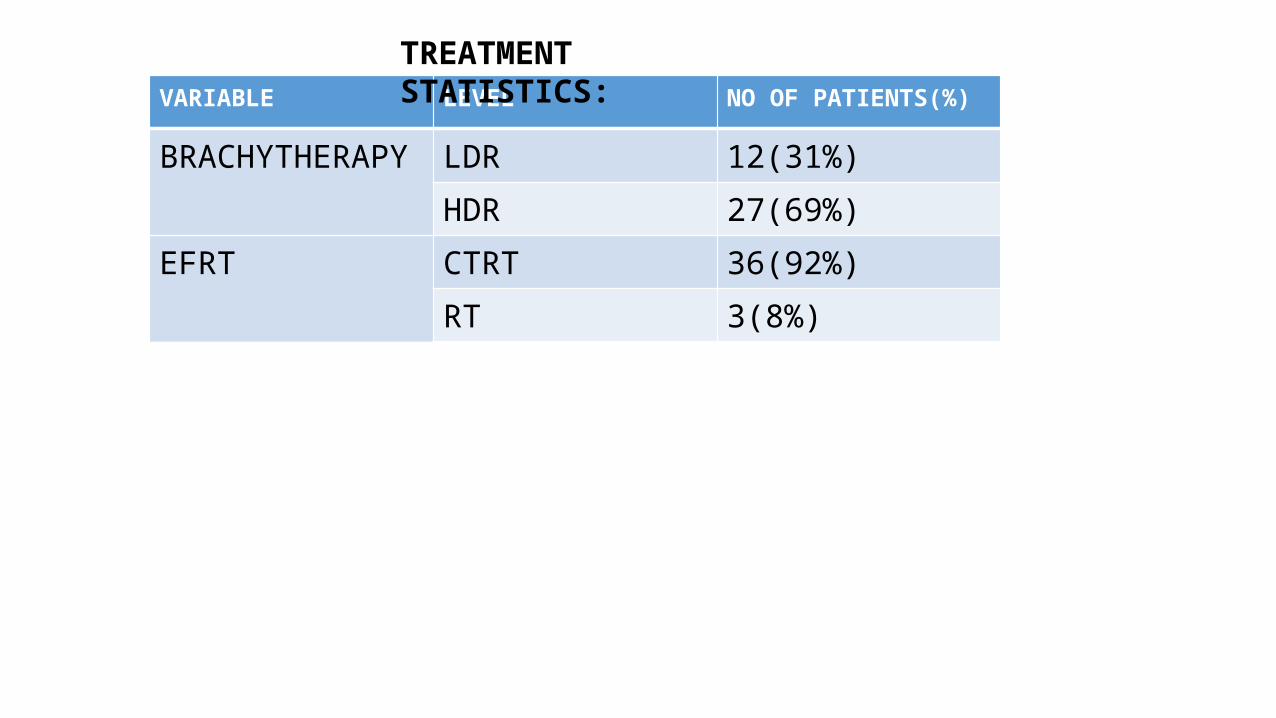
VARIABLE LEVEL NO OF PATIENTS(%)
BRACHYTHERAPY LDR 12(31%)
HDR 27(69%)
EFRT CTRT 36(92%)
RT 3(8%)
TREATMENT STATISTICS:

result analysis

NO OF PATIENTS FAILURE SITE20 INSIDE AND
OUTSIDE THE TREATMENT FIELD
Among these 16 patients had failure in nodal sites outside the treated field.
7 EXCLUSIVELY OUTSIDE THE FIELD
3 EXCLUSIVELY WITHIN THE TREATED FIELD
PATTERNS OF FAILURE: 30 (77%)13 patients has treatment upto T12-L1 junction.
2 patients upto L3-L4 junction.1 patients upto L2-L3 junction.These 3 patients belongs to 1st group.
90% of total patients
• Distant failure is noticed in 49 % of patients as site of first failure.
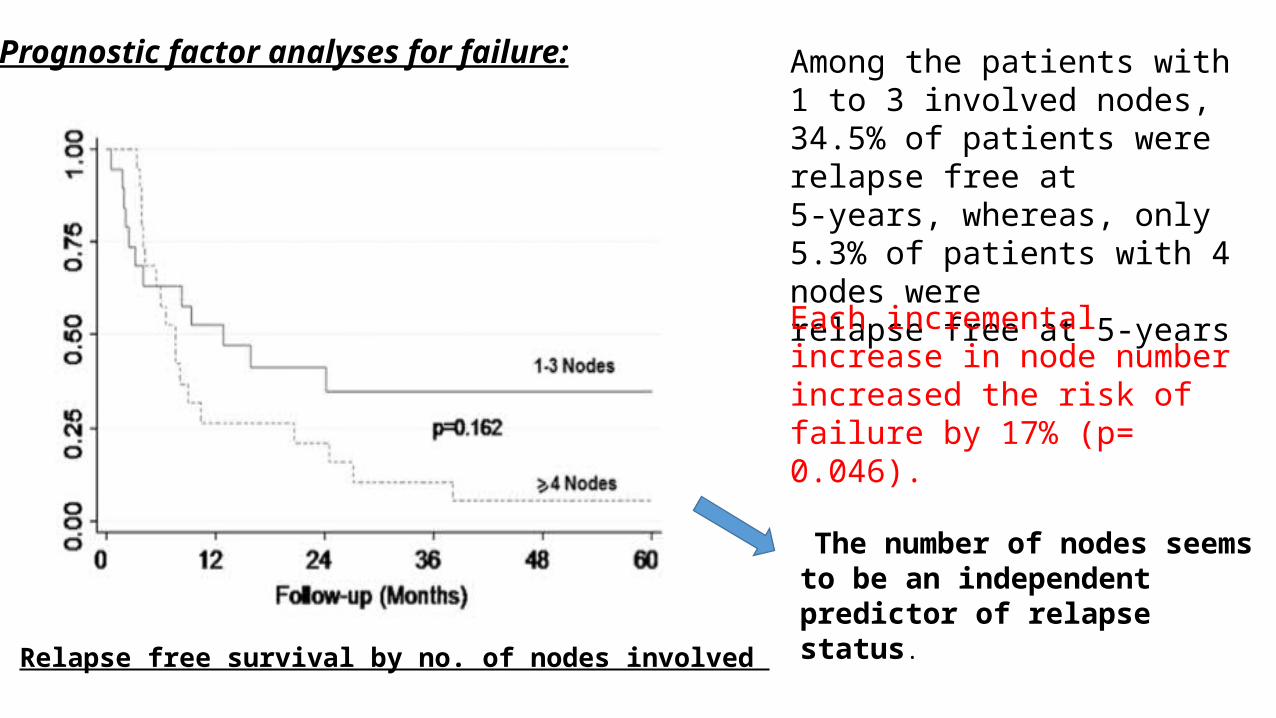
Prognostic factor analyses for failure: Among the patients with1 to 3 involved nodes, 34.5% of patients were relapse free at5-years, whereas, only 5.3% of patients with 4 nodes wererelapse free at 5-years
Each incremental increase in node number increased the risk of failure by 17% (p= 0.046).
Relapse free survival by no. of nodes involved
The number of nodes seems to be an independent predictor of relapse status.

Treatment-related acute side effects Treatment breaks during EFRT
• only 3 patients (8%) experienced treatment breaks due to radiation toxicity, with a mean delay of 6.5 days
• Fifteen patients (38%) had overall grade 3 to 4 acute toxicity

Treatment-related late side effects
only 2 patients (5%) had significant late toxicity. One of these patients had urinary incontinence related to a large tumor involving the external surface of the bladder base, and the other patient had a rectovaginal fistula which resulted from recurrent tumor.
No deaths occurred due to toxicity.
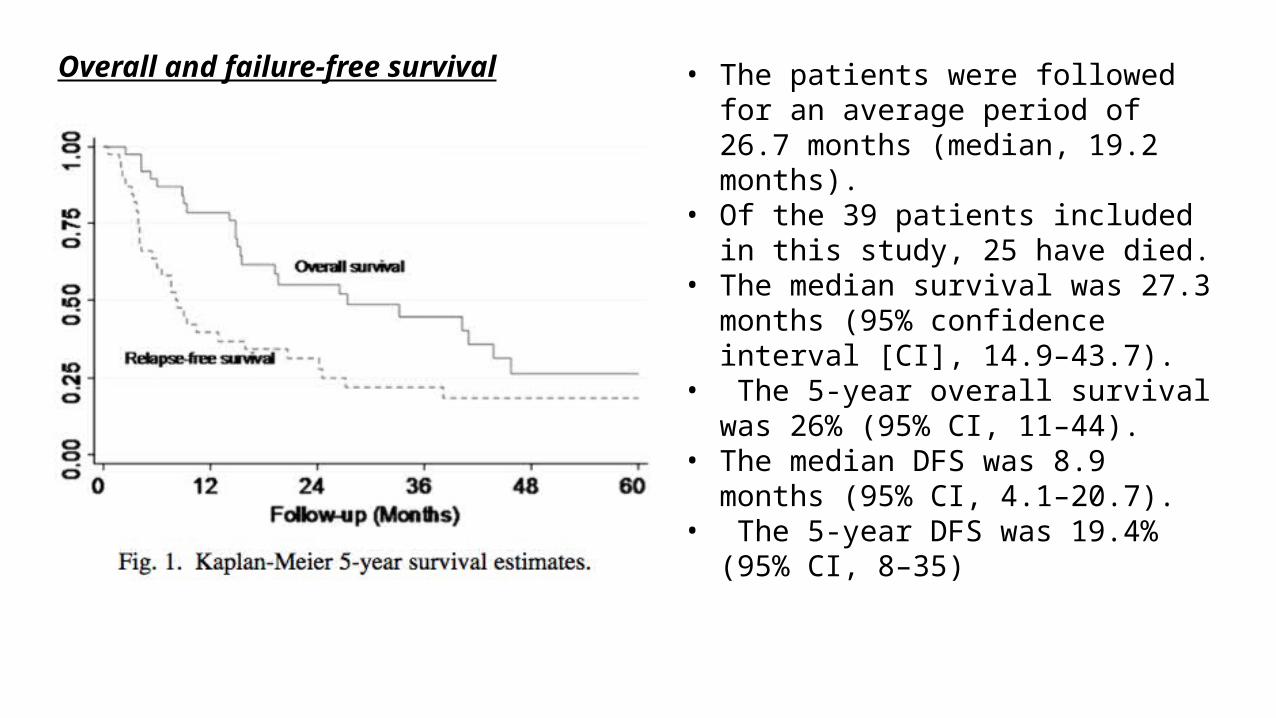
• The patients were followed for an average period of 26.7 months (median, 19.2 months).
• Of the 39 patients included in this study, 25 have died.
• The median survival was 27.3 months (95% confidence interval [CI], 14.9–43.7).
• The 5-year overall survival was 26% (95% CI, 11–44).
• The median DFS was 8.9 months (95% CI, 4.1–20.7).
• The 5-year DFS was 19.4% (95% CI, 8–35)
Overall and failure-free survival

DISCUSSION
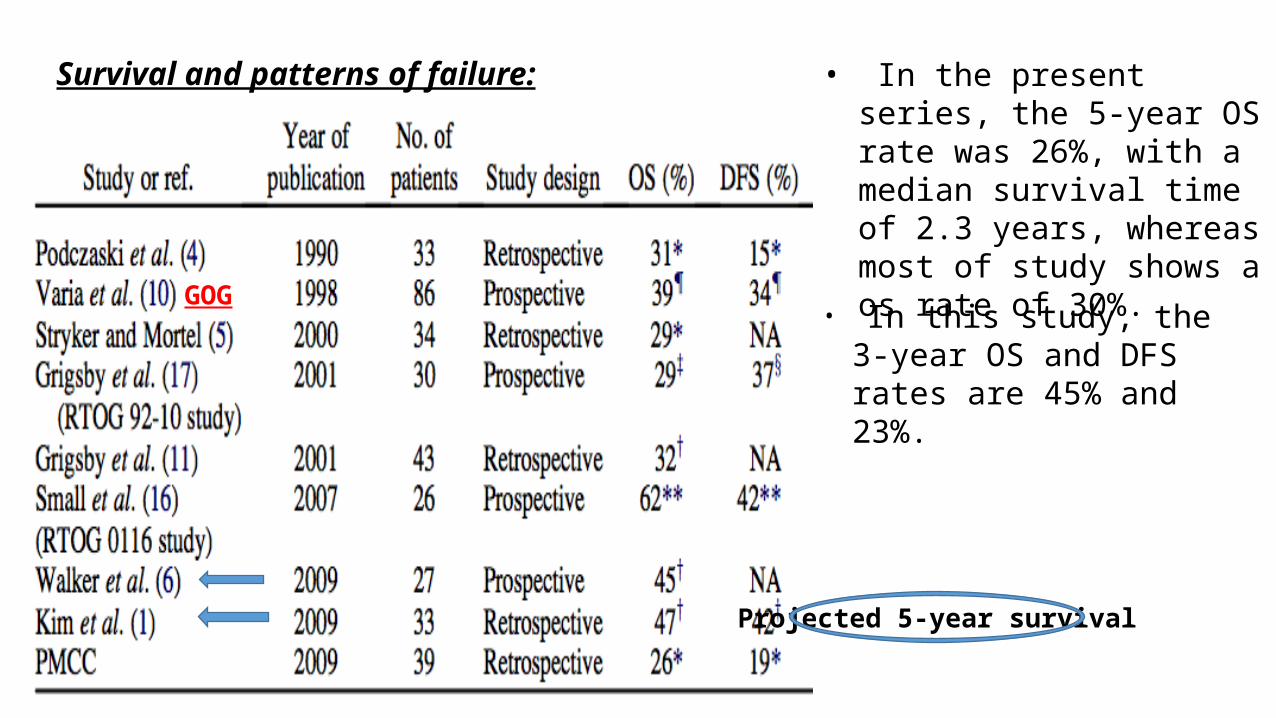
Survival and patterns of failure: • In the present series, the 5-year OS rate was 26%, with a median survival time of 2.3 years, whereas most of study shows a os rate of 30%.
• In this study, the 3-year OS and DFS rates are 45% and 23%.
GOG
Projected 5-year survival

• Patterns of failure in cervix cancer patients treated with EFRT have changed over the last 4 decades. • Pelvic failure was the predominant site of failure in patients treated with radiotherapy, without the use of
concurrent chemotherapy. An observation was made by Podczaskiet al, who reported a pelvic failure rate of 48% and a distant failure rate of 18% as the initial site of failure. That rate is in contrast to the 49% incidence of distant failure as the initial site of failure reported in the present study
• The higher incidence of distant metastases as the initial site of failure can be explained by the use of PET scanning at the time of first relapse.
• Use of concurrent CTRT reduces the tumor size, after which conformal brachytherapy gives a satisfactory dose distribution.
The gross nodal disease was treated to 50.4 to 54 Gy, with only 1 patient experiencing isolated in-field nodal failure.
These results suggest that the doses used in the present study were adequate to control curable disease. Some investigators have attempted dose escalation to para-aortic nodes using intensity-modulated RT in order to improve outcome. However, because the poor survival is related to high failure rates outside the treatment field, increasing dose within the treatment field is unlikely to improve survival.
in view of a small number (6/39) of patients who were treated with limited EFRT (at L2–L4 junction), it is not clear whether there is a benefit in treating patients with common iliac or lower para-aorticnodal disease with large fields extending up to T12–L1.

• Prognostic factors:Lymph node metastasis is the most important prognostic factor in cervical cancer.In the present study, the univariate estimates show that any para-aortic nodal involvement increased the risk of any relapse by 11% and death by 49%.This study was not sufficiently powered to show statistical significance determining the prognostic value of the level of lymph node involvement. But this study showsshowed a trend toward poorer survival with a higher level of nodal involvement.• Treatment-related acute toxicities:
Higher rates of acute gastrointestinal and bone marrow toxicity are expected in patients treated with concurrent chemotherapy and EFRT due to the large field sizes. In this series, 15 patients (38%) had overall grade 3 to 4 toxicity. This level is much lower than the 85% incidence of acute toxicity reported in the RTOG 0116 study.This may be due to 1. parametrial boost used in RTOG trial.(60GY) & Nonpelvic nodes upto 54-59.6gy 2. upper border of T12 used in the portal.late toxicity: Both the 0116 and the 92-10 RTOG studies reported late toxicity rates of 40% and 21%, respectively whereas only 2 patients (5%) had significant late toxicity.

CONCLUSIONS
It is proposed by the author, that • The involvement of common iliac and para-aortic lymph nodes in cervix cancer patients should
be regarded as systemic disease.• The standard radiotherapy doses that are currently used are adequate to successfully control
the primary tumor and the involved nodes in curable patients.
• Toxicity has been a limiting factor in the use of EFRT. Advent of conformal EFRT with concurrent chemotherapy, followed by conformal brachytherapy using moderate doses may optimize tolerable treatment with acceptable toxicity.

Thank you





























