Embed Size (px)
DESCRIPTION
Guided tissue regenerative techniques in periapical surgery
Citation preview

Review Article
Guided Tissue Regeneration in Periapical SurgeryLouis Lin, BDS, DMD, PhD,* Melody Y.-H. Chen, DDS, MS,† Domenico Ricucci, DDS, MD,‡
and Paul A. Rosenberg, DDS*
Abstract
Tissue regeneration by using membrane barriers andbone grafting materials in periapical surgery is anexample of tissue engineering technology. Membranebarriers and/or bone grafts are often used to enhanceperiapical new bone formation. However, the periapicaltissues also consist of the periodontal ligament (PDL)and cementum. For regeneration of the periapical tissuesafter periapical surgery, one of the important require-ments is recruitment and differentiation of progenitor/stem cells into committed pre-osteoblasts, pre-PDL cells,and pre-cementoblasts. Homing of progenitor/stem cellsinto the wounded periapical tissues is regulated byfactors such as stromal cell–derived factor 1, growthfactors/cytokines, and by microenvironmental cuessuch as adhesion molecules and extracellular matrixand associated noncollagenous molecules. Tissue regen-eration after injury appears to recapitulate the pathwayof normal embryonic tissue development. Multiple tissueregeneration involves a complex interaction betweendifferent cells, extracellular matrix, growth/differentia-tion factors, and microenvironmental cues. Little isknown concerning the biologic mechanisms that regu-late temporal and spatial relationship between alveolarbone, PDL, and cementum regeneration during periapi-cal wound healing. Simply applying a membrane barrierand/or bone graft during periapical surgery might notresult in complete regeneration of the periapical tissues.It has not been clearly demonstrated that these biomate-rials are capable of recruiting progenitor/stem cells andinducing these undifferentiated mesenchymal cells todifferentiate into PDL cells and cementoblasts afterperiapical surgery. (J Endod 2010;36:618–625)Key WordsBone grafting materials, guided tissue regeneration,membrane barriers, periapical surgery
From the *Department of Endodontics, New York Univer-sity College of Dentistry, New York, New York; †Departmentof Endodontics, Chi Mei Medical Center, Yong Kang, Tainan,Taiwan; and ‡Private practice, Rome, Italy.
Address requests for reprints to Dr Louis Lin, Department ofEndodontics, New York University College of Dentistry, 345 E24th St, New York, NY 10010. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2009.12.012
618 Lin et al.
Systematic review of the literature concerning guided tissue regeneration in periap-ical surgery is not possible because of wide variations in research methodology.
Tissue engineering involves the use of biologic and engineering sciences to develop bio-logic substitutes that restore, maintain, or enhance tissue function (1). In general, thereare 3 main approaches to tissue engineering: (1) to use isolated cells or cell substitutesas cellular replacement parts, (2) to use acellular biomaterials (scaffolds) capable ofinducing tissue regeneration, and (3) to use a combination of cells and biomaterials (1,2). These approaches are suitable for single tissue regeneration such as new boneformation. For example, in terms of multiple tissue regeneration, new periodontalor periapical tissue formation, the involvement of tissue engineering technologymight be even more complex (2). The process of introducing biomaterials into thehost to enhance or modify natural wound healing can be considered as tissueengineering (1, 2). Tissue regeneration by using membrane barriers and/orbone grafting materials in periapical surgery is an example of tissue engineeringtechnology.
Guided tissue regeneration is a technique(s) for enhancing and directing cellgrowth to repopulate specific parts of the periodontium that have been damaged byperiodontal diseases, tooth diseases, or trauma (3). Guided tissue regeneration byusing membrane barriers and bone grafting materials has been extensively investigatedin periodontal regenerative therapy to induce new attachment of periodontiumdamaged by periodontal disease (4–8). Guided tissue regeneration, especially byusing bone grafting materials, has also been widely used in implant dentistry toenhance new bone formation for placement of implants (9). Histologic assessmentsof guided tissue regenerative therapy in periodontal disease often show down-growthof junctional epithelial cells between the membrane barrier and root surface (10).Bone grafting materials have little osteoinductive capacity and generally become en-cased in a dense fibrous connective tissue (10). In addition, junctional epithelium stillappears to form between the bone grafts and root surface (10–12). Bone graftingmaterials are not capable of inducing new connective tissue attachment afterguided tissue regenerative therapy in periodontal disease (13). The variability insafety, clinical effectiveness, and stability over time of bone grafting materials usedfor guided tissue regeneration in periodontal therapy has been questioned (10, 14,15). A systematic review of the literature concerning bone replacement grafts inthe treatment of periodontal osseous defects concludes that alloplastic graftssupport periodontal repair rather than regeneration (16). Guided tissue regenerationby using membrane barriers and/or bone grafting materials has also been used inperiapical surgery to enhance new bone formation (17–22). Those studies weremainly focused on new bone formation and did not address formation ofperiodontal ligament (PDL) and cementum, which are also components of theperiapical tissues.
Application of guided tissue regeneration concepts to periapical surgery isprimarily based on extensive studies of periodontal regenerative therapy. However,there are significant differences in the application of guided tissue regeneration in peri-odontal regenerative therapy and in periapical surgery, and these will be discussed inthis review. The purpose of this review is to provide a better understanding of basicmolecular and cellular biologic concepts when using membrane barriers and/orbone grafts in periapical surgery, with specific reference to guided tissue regenerationin periodontal regenerative therapy (8). To avoid repeating the excellent review byBashutski and Wang (8), the types of membrane barriers and bone grafting materialswill not be included in this review.
JOE — Volume 36, Number 4, April 2010

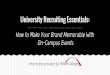
Figure 1. Histology of apical periodontitis of an extracted human tooth.Proliferation of epithelial strands occurs in the chronically inflamed periapicaltissues around the apical foramen, which is surrounded by a band of densefibrous connective tissue. Note destruction of the apical alveolar bone andapical periodontal ligament as well as apical root resorption involvingcementum and dentin (arrows) (Hematoxylin-eosin; original magnification,�16).
Review Article
Periodontal Tissue Destruction in PeriodontalDisease and in Apical Periodontitis
The etiology and pathogenesis of periodontal disease (marginal pe-riodontitis) and apical periodontitis are similar. Both diseases arecaused by bacterial biofilm infection and manifest periodontal tissuedestruction; gingival tissue, PDL, cementum, and alveolar bone areaffected in periodontal disease and the last 3 tissues as well as dentinin apical periodontitis (Fig. 1). Periodontal disease is an open wound,which is constantly challenged by direct oral infection even after therapy.Apical periodontitis is a closed wound. Destruction of periodontal tissuesin periodontal disease and in apical periodontitis is caused indirectly byactivation of the host’s innate and adaptive immune cells (23, 24).Microorganisms and their toxins in periodontal pockets are in directcontact with the sulcular epithelium of periodontium in periodontaldisease. In contrast, in the presence of apical periodontitis,microorganisms and their toxins are in the root canal system ratherthan in the periapical tissues. In certain types of periodontal defects,the attachment apparatus destroyed by established periodontal diseasecannot be predictably regenerated after removal of bacterial plaqueand calculus from the affected root surface by open flap debridementor even with guided tissue regenerative therapy (25). In contrast,damaged periapical tissues in established apical periodontitis lesionscan be predictably regenerated after elimination of intraradicularbacteria by proper nonsurgical endodontic therapy without the needof periapical surgery and guided tissue regenerative procedures (26)(Fig. 2). In addition, unlike guided periodontal regenerative therapy,periapical surgery is indicated only because nonsurgical root canaltherapy is not feasible for established apical periodontitis lesions, espe-cially in retreatment cases. The molecular and cellular biology associatedwith complete regeneration of periapical tissues, cementum, PDL, andalveolar bone after nonsurgical and/or surgical endodontic therapiesof apical periodontitis lesions is not fully understood.
Biology of Periapical Wound Healing AfterPeriapical Surgery
It is important to understand the natural wound healing potentialof periapical lesions after elimination of the etiology, before consideringthe application of biomaterials such as membrane barriers and/or bonegrafts during periapical surgery. As described previously, the woundhealing potential of apical periodontitis is different from that of marginalperiodontitis after treatment. The principle of periapical wound healingafter periapical surgery is similar to that of connective tissue woundhealing elsewhere in the body. It is a host’s ‘‘programmed event,’’ whichbegins with (1) hemostasis or coagulation phase, (2) inflammationphase, (3) proliferative phase, (4) regeneration and/or repair phase,and last (5) remodeling or maturation phase (27–30).
Regardless of the size of a wound, granulation tissue in the prolif-erative phase, a necessary element of wound healing, fills the wound andhelps complete the wound healing process (30). Wound healing usuallyinvolves recruitment and differentiation of progenitor/stem cells intotissue committed cells (27, 31–35). Wound healing can result ineither regeneration or repair, depending on the nature of wound,availability of progenitor/stem cells, growth/differentiation factors, andmicroenvironmental cues such as adhesion molecules, extracellularmatrix (ECM), and associated noncollagenous protein molecules (27,35, 36). Regeneration represents the replacement of damaged tissueby the cells of the same tissue. Importantly, it reconstitutes, althoughnot completely, both the architecture and functions of the originaltissue, such as healing of an uninfected simple surgical incision of theskin approximated by surgical sutures, because tissue destruction andgranulation tissue formation are minimum (29, 30). Repair represents
JOE — Volume 36, Number 4, April 2010
the restoration of the destroyed tissue by new tissue different from theoriginal tissue. It does not reconstitute the architecture and functionsof the original tissue as, for instance, healing of a myocardial infarctby fibrosis (29, 30). In periapical surgery, the resected root endcannot be regenerated.
Regeneration of periapical tissues after periapical surgery requires(1) recruitment of progenitor/stem cells to differentiate into committedosteoblasts, PDL cells, and cementoblasts (Fig. 3); (2) growth/differen-tiation factors as necessary signals for attachment, migration, prolifer-ation, and differentiation of progenitor/stem cells; and (3) localmicroenvironmental cues such as adhesion molecules, and ECM andassociated noncollagenous protein molecules (10, 37). Lack of anyone of these elements would result in repair rather than regeneration(37). In addition, all these components must coordinate precisely intheir temporal and spatial relationship to reconstitute the architectureand functions of the damaged periapical tissues. Homing of progenitor/stem cells to wounded periapical tissues is regulated by factors such asstromal cell–derived factor–1, growth factors/cytokines, and by micro-environmental cues (27). Although wound healing appears to recapit-ulate the pathway of normal embryonic tissue development, the tissueregenerated might be similar to but will not exactly replicate thedamaged original tissue in architecture and functions (38). Forexample, mineralized tissue referred to as reparative dentin can beformed in uncontaminated, exposed vital pulps after capping withappropriate biomaterials; however, the regenerated reparative dentinis different from primary dentin (39–42). This is becauseodontoblasts are highly differentiated postmitotic cells and cannotregenerate after lethal injury. Reparative dentin is formed byodontoblast-like cells, which are differentiated from pulp progenitor/stem cells. Similarly, root resorption including cementum and dentinin chronic apical periodontitis lesions can only be repaired by cellularcementum and not by both dentin and cementum after root canaltherapy (43) (Fig. 2D). An analogy might be that Picasso’s paintingscannot be precisely reproduced, even though numerous copies canbe created. It has been proposed that the local environment ofcementum matrix and associated molecules could influence recruit-ment and functions of cementum-forming progenitor/stem cells in
Guided Tissue Regeneration in Periapical Surgery 619

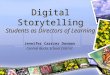
Figure 2. (A) Preoperativer radiograph of tooth #19. A large osteolytic lesion associated with the distal root and a small lesion associated with the mesial root areshown. Histologically, resorption of the root apex is usually present in chronic apical periodontitis such as in (A). (B) Follow-up radiograph of tooth in (A) taken 3years and 7 months after nonsurgical root canal therapy shows healing of periapical lesions. (C) Follow-up radiograph of tooth in (A) taken 6 years postoperativelywhen the patient presented for emerging symptoms. The mesial root had a vertical root fracture, and the tooth was extracted for histologic examination. (D)Histology of the distal root in (C). The resorbed root apex involving cementum and dentin was repaired by deposition of cellular cementum on the externalroot surface (solid arrows) and inside the root canal (open arrow). Incremental lines indicate alternating periods of activity and quiescence of cementum depo-sition (hematoxylin-eosin; original magnification, �50).
Review Article
the PDL during cementum wound healing and regeneration (36).However, the molecular and cellular biology of cementum formationon an exposed root dentin surface after inflammatory resorption andperiapical surgery is not clear.
Although resident cells, cementoblasts, PDL cells, and osteoblastsin the periapical tissues are differentiated cells, they still retain thepotential to undergo cell division and proliferation on stimulation byappropriate signals during physiologic turnover and periapical woundhealing. However, these cells are not progenitor/stem cells and are notcapable of self-renewal and differentiation. Therefore, the regenerativepotential of these committed cells is limited. In addition, it is not knownwhether the regenerative potential of PDL cells, cementoblasts, and
620 Lin et al.
osteoblasts is related to their life span exactly. In small periapicallesions, resident osteoblasts, PDL cells, and cementoblasts might becapable of restoring damaged periapical tissues. However, in largeperiapical lesions, periapical wound healing requires recruitmentand differentiation of progenitor cells/stem cells into osteoblasts,cementoblasts, and PDL cells. It has been well-demonstrated thatPDL harbors adult stem cells in the paravascular spaces, and thesestem cells are capable of differentiating into PDL-like, cementoblast-like, and osteoblast-like cells (37, 44, 45). In addition, bonemarrow mesenchymal stem cells (46) and periosteal osteoprogenitorcells (47, 48) are capable of differentiating into osteoblasts. Celldifferentiation involves a change from one pattern of gene expression
JOE — Volume 36, Number 4, April 2010

Endostealosteoprogenitor cells
Periostealosteoprogenitor cells
Bone marrow mesenchymal stem cells
CementoblastPDL cell
PDL stem cellsPDL stem cells
Osteoblast
Figure 3. Schematic illustration of recruitment and differentiation of progen-itor/stem cells into osteoblasts, PDL cells, and cementoblasts during periapicalwound healing.
Review Article
to another. It does not involve a change in the DNA sequence itself(49). Cell differentiation is regulated by extrinsic local microenviron-mental cues and intrinsic master regulatory genes (49). Cell differen-tiation is usually a part of the regenerative process (49).
Regardless of the size of periapical lesions, persistence of rootcanal infection is the primary cause of inflamed periapical tissues notto heal after endodontic therapy (50). There are no published studiesdemonstrating that membrane barriers and/or bone grafts contributedto the cause of periapical surgery failure. Complete periapical woundhealing after periapical surgery should include regeneration of alveolarbone, PDL, and cementum.
Membrane Barriers in Periapical SurgeryThe application of a membrane barrier in periodontal regenera-
tive therapy is to prevent apical migration of gingival epithelial andconnective tissue cells onto the denuded root surface and to facilitatethe repopulation of the damaged root surface with PDL progenitor/stem cells to differentiate into PDL cells and cementoblasts (5–7,10). Without a membrane barrier, open flap debridement does notprevent apical migration of junctional epithelium along denuded rootsurfaces (7). Some clinicians place a membrane barrier over a bonydefect beneath a full-thickness mucoperiosteal flap during periapicalsurgery. Most often the cases involve treatment of large periapicallesions or through-and through bony defects, theoretically to preventproliferation of fibroblasts from the periosteum into the bony defect.This could result in scar tissue formation (19, 51–56). However,PDL also contains numerous fibroblasts (42, 57) and bone marrowmesenchymal stem cells, which are capable of differentiating intofibroblasts as well (58, 59). In addition, during the proliferativephase of wound healing, there is proliferation of not only newvasculature but also fibroblasts at the wound site (29, 30). Amembrane barrier might actually prevent osteoprogenitor cells in theperiosteum from proliferating into the bony defect to help new boneformation. The epithelial cells from gingivomucosal epithelium arenot able to proliferate into the apical bony defect after periapicalsurgery if there is no periodontal involvement. A membrane barrierwill not selectively allow specific cell types, such as PDL progenitor/stem cells, bone marrow mesenchymal stem cells, or endostealosteoprogenitor cells, to repopulate a root surface damaged by apicalperiodontitis or by surgical root resections during periapical surgery.
Scar tissue formation is a pathologic process occurring duringtissue repair and is sometimes observed in through-and-through
JOE — Volume 36, Number 4, April 2010
human inflammatory periapical lesions after endodontic surgery (60,61). In animal studies at 3- to 5-month observation periods, ifmembrane barriers were not used to cover the bony defects bothbuccally and palatally/lingually, when through-and-through osseousdefects were created in jawbones, the defects were filled with fibrousconnective tissue (51, 52). This is most likely due to the lack ofavailable osteogenic progenitor/stem cells rather than to fastmovement of fibroblasts. Cell migration does not simply depend oncell mobility. Cells migrate directionally in response to a variety ofcues, including gradients of chemokines, growth factors, and ECMmolecules. These factors engage cell surface receptors and direct cellmigration (27, 62). During wound healing, activated fibroblastsinitially lay down excess new collagen of subtypes I and III. Thesecollagen fibers, especially type III, become remolded or degraded bymatrix metalloproteinase and collagenase released by activatedmacrophages and fibroblasts and are ultimately replaced by type Icollagen at a later stage of wound healing. Fibroblasts differentiateinto myofibroblasts at the remodeling phase (27, 28). Sometimes theuncontrolled matrix accumulation of collagen types I and III bymyofibroblasts, often involving aberrant cytokine pathways, mightoccur and leads to excess scarring and fibrotic sequelae (27).Nevertheless, the cellular and molecular biology of fibrosis or scartissue formation is not fully understood. It has been suggested thatimmune regulation, up-regulation of collagen production by myofibro-blasts, down-regulation of matrix metalloproteinases, and up-regulationof transforming growth factor (TGF)–b, as well as dysregulation ofapoptosis of myofibroblasts might play an important role in fibrosisor scar tissue formation (27, 63, 64).
It seems that if both buccal and palatal/lingual cortical plates arelost as a result of apical periodontitis lesions or periapical surgery,periapical wounds will most probably heal by scar tissue formation(51, 52, 60). Studies have shown no difference in bone tissuehealing if only the buccal cortical plate was destroyed, whether ornot a membrane barrier was used in periapical surgery (65, 66). Onthe basis of limited controlled clinical trials, there is no conclusiveevidence to demonstrate that the application of membrane barriersin large or through-and through bony lesions/defects has a betterlong-term outcome than a control in periapical surgery. By definition(3), application of membrane barriers in periapical surgery does notappear to meet the concept of guided tissue regeneration. In contrast,in periodontal regenerative therapy membrane barriers serve toguide progenitor/stem cells to repopulate their specific parts of theperiodontium.
Clinically, the best application of membrane barriers in periapicalsurgery appears to be in combined endodontic-periodontal orperiodontal-endodontic lesions (67) or large periapical lesionscommunicating with the alveolar crest (68, 69). In this kind ofapicomarginal bony defect, the PDL and cementum are destroyed.Accordingly, application of a membrane barrier is indicated duringperiapical surgery to prevent apical migration of junctional epitheliumalong the denuded root surface into the periapical wound and toinduce selective repopulation of cells of the connective tissueattachment (67–69). In combined endodontic-periodontal orperiodontal-endodontic lesions, the use of a membrane to manage thelesions is directed at the periodontal tissue rather than periapical tissueregeneration. Oh et al (70) have presented an excellent review of theapplication of guided tissue regeneration in combined endodontic-periodontal lesions with apicomarginal bony defects. It should be notedthat a true new connective tissue attachment can only be demonstratedby means of histologic rather than clinical examination (14).
In an animal study, Nyman and Karring (71) surgically elevatedbuccal mucoperiosteal flaps. A strip of buccal alveolar bone between
Guided Tissue Regeneration in Periapical Surgery 621

Review Article
the mesial and distal line angles was removed corono-apically from theroots to a notch prepared in the root surface as a landmark. This wasdone without significantly injuring the PDL and cementum. The flapswere then repositioned and sutured. Fibrous connective tissue reattach-ment and varying degrees of alveolar bone regeneration were histolog-ically observed on the root surfaces 8 months postoperatively.Lindhe et al (72) experimentally extracted the teeth in an animalstudy. Immediately after tooth extraction, the buccal root surfaces of theteeth were planed with curettes to a level corresponding to half the rootlength. Before reimplantation of the teeth, the buccal alveolar bonebetween mesial and distal line angles was removed to a level corre-sponding to half the depth of the sockets. Histologically, a fibrousconnective tissue reattachment failed to form on that part of the reim-planted teeth, which had been deprived of their PDL 6 months postop-eratively. In addition, dentogingival epithelium had migrated apicallyalong the denuded root surface.
In another animal study, Gottlow et al (73) surgically raised buccalmucoperiosteal flaps. The buccal alveolar bone between the mesial anddistal line angles of each root was removed to a level corresponding toapproximately 50%–75% of the length of the root. The coronal portionof the root surfaces was left open to bacterial plaque accumulation for 6months. Subsequently, the coronal root surfaces were thoroughlyscaled and planed, and the cementum was removed. Immediatelybefore suturing of the coronally positioned flap, a membrane wasplaced over the denuded root surfaces to prevent granulation tissuefrom the soft tissue flaps from reaching contact with the denudedroot surfaces during wound healing. New cementum with insertingcollagen fibers was histologically observed on the previously exposedroot surfaces 30 days postoperatively. However, the newly formedcementum is primarily cellular and not acellular cementum.
Therefore, the nature of a dehiscence (naturally occurring orpathologic) is an important factor in determining whether applicationof a membrane barrier is necessary. If dehiscence is naturally occur-ring, a fibrous connective attachment is present between the rootsurfaces and the mucosa. A membrane barrier is not required duringperiapical surgery because fibrous connective tissue reattachmentwill occur onto the root surface after reposition and suturing of asurgical flap (71). However, if the cause of dehiscence is pathologicas a result of marginal periodontitis, a membrane barrier is suggestedto prevent apical migration of junctional epithelium along the rootsurfaces during periapical surgery (70).
Bone Grafts in Periapical SurgeryA systematic review of the literature concerning regeneration of
periodontal tissues in periodontal regenerative therapy indicates thatcombination of barrier membranes and grafting materials mightproduce histologic evidence of periodontal regeneration, which ispredominantly bone repair (74). Bone grafting materials include auto-grafts, allografts, xenografts, and alloplasts. They have been used inperiodontal regenerative therapy as space maintainers for selectivecell repopulation onto the denuded root surfaces or to act as osteoin-ductive or osteoconductive biomaterials for regeneration of bone lossas a result of periodontal disease (8, 75, 76). Bone grafts have alsobeen successfully used to regenerate new bone formation in implantdentistry (9). The same bone grafting materials, especially alloplastssuch as calcium sulfate, have been widely used in periapical surgeryto enhance new bone formation as well (17, 18, 20, 77–80).Calcium sulfate must dissolve in tissue fluid or integrate into bonebefore or during new bone formation. Similar to periodontalregenerative therapy, evaluation of wound healing after periapicalsurgery by using bone grafts should also include regeneration of PDL
622 Lin et al.
and cementum. Histologically, very few studies of bone grafts inperiapical surgery have investigated whether grafting materials arecapable of inducing PDL and cementum regeneration (17, 18, 22,78, 79). Therefore, the nature of regenerated periapical tissues afterthe use of bone grafts in periapical surgery remains unknown,despite radiographs showing some evidence of PDL space (56). Thepossibility of ankylosis after bone grafts in periapical surgery shouldbe investigated in long-term studies because grafting materials mightencourage osteoprogenitor cells and prevent PDL progenitor/stem cellsfrom repopulating damaged root surfaces caused by apical periodonti-tis or the resected root surfaces after periapical surgery. In 2 studies,calcium sulfate was placed in the osteotomy sites during periradicularsurgery, and it did not appear to affect cementum deposition onto theresected root surfaces (20, 22).
Bone grafting materials, except autogenous bone grafts, areforeign to the host’s tissue and can interfere with the normal woundhealing process, resulting in delayed healing or a foreign body reaction(29, 30). Some studies with bone grafts in periapical surgerydemonstrated favorable hard tissue healing compared with a control(17, 18, 22, 78, 79, 81, 82), whereas other studies showed nodifference (20, 21, 80, 83). All reported outcome studies ofperiapical wound healing by using bone grafts in periapical surgeryare short term, lasting no more than 12 months. Bone is a dynamictissue and, throughout life, constantly undergoes remodeling(resorption and deposition). During the healing of bone, osteoblastsinitially produce immature trabecular woven bone, and thenosteoclasts slowly remove this provisional woven bone. Later,osteoblasts replace it with lamellar bone (84, 85). Remodeling or thematuration phase of wound healing can take months to years to becomplete (29, 30). The long-term biologic nature of new bone formedafter using bone grafts after periapical surgery is unknown. It might besimilar to reparative dentin after capping of exposed vital pulps withappropriate biomaterials. Reparative dentin is different from primarydentin in structure and/or function. Nevertheless, it is a biologicproduct of dentin-pulpal complex after pulpal wound healing.
Most bone grafts, especially calcium sulfate used in periapicalsurgery, are neither osteogenic nor osteoinductive (86). Therefore,calcium sulfate is not capable of recruiting mesenchymal stem cellsin the bone marrow or endosteum and osteoprogenitor cells in the peri-osteum to differentiate into committed pre-osteoblasts. Calcium sulfateis osteoconductive (8, 87, 88), which refers to the ability of someforeign materials to serve as a scaffold on which cells can attach,migrate, and grow and divide (86). Even though bone grafts are osteo-conductive, they are not ideal materials for promoting periodontaltissue regeneration such as PDL and cementum in periodontal regener-ative therapy because they are not able to stimulate the formation ofa new connective tissue attachment (8, 13, 14). Many studies haveclearly demonstrated that calcium sulfate can serve as scaffold fornew bone formation in periapical surgery (17, 18, 78–80). However,a question remains: can bone grafts induce regeneration of apicalPDL and cementum damaged by large apical periodontitis lesionsafter periapical surgery? In one human histologic study, as many as81% of the teeth with apical periodontitis revealed apicalinflammatory root resorption including cementum and/or dentin (89).
Biologically, a blood clot is a better space filler or ECM than allbone grafting materials. A blood clot is the host’s own biologic productand is essential to tissue wound healing. Without a blood clot, tissuewound healing would be impaired (29, 30), as in a dry socket aftertooth extraction. A blood clot is composed of insoluble fibrin (90)and many growth factors/cytokines such as platelet-derived growthfactor (PDGF), TGF-b, vascular endothelial growth factor (VEGF),endothelial growth factor, insulin-like growth factor (IGF), and basic
JOE — Volume 36, Number 4, April 2010

Review Article
fibroblast growth factor (FGF) (91, 92). During wound healing, fibrinfilaments cross-linked to fibronectin provide a provisional matrix forattachment and migration of immune cells, fibroblasts, endothelialcells, and tissue cells (27, 30). The degraded products of fibrin, byplasmin, are chemotactic to the host’s immune cells (30). In addition,FGF, TGF-b, VEGF, and endothelial growth factor in blood clot promoteangiogenesis to enhance tissue wound healing (93). Bone grafts alonewithout a blood clot or angiogenic factors are unlikely to be capable ofpromoting periapical wound healing (25).Growth/Differentiation Factors in PeriapicalSurgery
Growth factors/cytokines play a crucial role in tissue wound heal-ing because they regulate immune function and proliferation and differ-entiation of cells participating in wound healing (27, 93, 94). Growthfactors are multifunctional and often have more than 1 target cell(27, 93). Many of the host’s natural growth factors have beensynthesized in vitro and used alone or incorporated into bone graftsin periapical surgery to enhance new bone formation. In a clinicalstudy, combination of platelet-rich plasma and tricalcium phosphateplaced in a bony defect after periapical surgery was shown to enhancebone regeneration (82). However, when exogenous recombinanthuman bone morphogenetic protein-1 (rhOP-1) (95), rhBMP-2(96), IGF combined with PDGF, or FGF alone (97) was delivered tothe bony defect during periapical surgery, the growth/differentiationfactors did not demonstrate any obvious benefit to the process ofbone healing. The concentration and stability of exogenous growthfactor/factors and their presence in relation to the temporal and spatialexpression of other growth/differentiation factors as well as their exacttarget cells are important in tissue wound healing (27, 93, 94).
It is challenging to study the biologic functions of growth factorsduring wound healing because many growth factors are involved atthe same or different stages of the wound healing process (93, 94).The biologic functions of most growth factors are redundant, andthey crosstalk to each other. In addition, most growth factors affectmore than a single cellular activity, and most cellular activities area response to the summation of several growth factors (93, 94). Thebiologic functions of growth factors might be synergistic orantagonistic (93, 94). More investigations are needed in this areabecause growth factors are the host’s own biologic products andimportant in tissue wound healing.
Factors Influencing Periapical Wound HealingNumerous factors such as infection, foreign bodies, systemic
disease, and an impaired host’s immune system can influence woundhealing (29, 30). Infection and foreign bodies are the mostimportant factors that can affect periapical wound healing. Implantedbiomaterials such as bone grafts, despite being inert and nontoxic,often trigger adverse foreign body reactions such as inflammation,fibrosis, infection, and thrombosis (98, 99). The foreign bodyreaction composed of activated macrophages and foreign body giantcells is the end-stage response of inflammation and wound healing afterimplantation of biomaterials (98). Foreign bodies favor infection due tobiofilm formation (30). In addition, any foreign materials such as bonegrafts have to dissolve in tissue fluid or be phagocytosed by activatedmacrophages before wound healing can be completed. If that doesnot occur, bone grafts will be surrounded by fibrous connective tissueor embedded in newly formed bone, as in some instances of periodontalregenerative therapy (10).
JOE — Volume 36, Number 4, April 2010
ConclusionExcept in apicomarginal bony defects caused by combined
periodontal-endodontic or endodontic-periodontal lesions (67, 70)or in large periapical lesions communicating with the alveolar crest(68, 69), the use of membrane barriers in periapical surgery has notbeen shown to have a clear benefit in regenerating periapical tissues.The ability of bone grafts to induce new bone formation has beenwell-documented (17, 18, 20–22, 78–83). However, new PDL andcementum regeneration in periapical surgery has not been shown tobenefit from the use of bone grafts.
Similar to the outcome assessment of nonsurgical (100) andsurgical endodontic therapy (61) as well as periodontal regenerativetherapy, long-term outcome studies are required to provide a betterunderstanding of the use of membrane barriers and/or bone grafts inperiapical surgery. Further assessment is also needed concerning histo-logic evaluation of periapical wound healing: complete regeneration ofalveolar bone, PDL, and cementum. It must be reemphasized that regen-eration of periapical tissues after severe injury or periapical surgeryrequires recruitment and differentiation of progenitor/stem cells intoperiapical tissue committed cells, growth/differentiation factors, andmicroenvironmental cues. All these factors have to work together atthe right time, space, and concentration to reconstitute the architectureand functions of the damaged periapical tissues. Little is known of thebiologic mechanisms that regulate temporal and spatial relationship ofalveolar bone, PDL, and cementum regeneration during periapicalwound healing. Simply applying a membrane barrier and/or bone graft-ing material during periapical surgery might not result in complete peri-apical tissue regeneration, because these biomaterials are not capableof recruiting progenitor/stem cells and signaling these undifferentiatedmesenchymal cells to differentiate into pre-osteoblasts, pre-PDL cells,and pre-cementoblasts. In particular, very little is known about cemen-togenesis after cementum injury or resorption and the mechanismsnecessary for attachment between dentin and newly formed cementum(10, 101). There are several types of cementum (57), which are formedby cementoblasts of different origins (101, 102). In addition, it is notknown whether new cementum formed on the root surfaces denudedof PDL and cementum is by interdigitation of collagen fibrils fromnew cementum and dentin matrix embedded in hydroxyapatitecrystals or by interlocking of hydroxyapatite crystals from dentin andcementum after periapical surgery (13). The exact origin ofcementoblast-like cells in periapical wound healing is not clear becauseHertwig’s epithelial root sheath (HERS) cells play pivotal roles incementum formation through their interplay with PDL stem cells(101–104). In mature teeth, HERS cells become disintegrated andremain as epithelial cell rests of Malassez in the PDL (103). Histologi-cally, cellular cementum can be very similar to bone (102). There areno appropriate cell markers for cementoblasts (101). Andreasen(105) has described different types of cementum repair and ankylosisafter apicoectomy in humans.
Without using membrane barriers and/or bone grafts in periapicalsurgery for large apical peridontitis lesions, complete periapical tissueregeneration has been observed histologically in many animal andhuman studies (60, 106–111). This is different from severeperiodontal tissue destruction caused by marginal periodontitis afteropen flap debridement without using membrane barriers and/orbone grafts, because gingival tissues, especially epithelial cells, willimmediately occupy denuded root surfaces before progenitor/stemcells from the PDL.
To fully understand the rational basis of regenerative procedures,we need to have more information concerning the variety of molecularand cellular biologic processes associated with the formation of each
Guided Tissue Regeneration in Periapical Surgery 623

Review Article
component of the periapical tissues (10). The clinician is advised not tothink that because there is a hole (surgical wound), it must be filled withsomething such as a bone graft (10). We must be concerned not onlyabout regeneration of alveolar bone but also the PDL and cementumafter periapical surgery. Although periapical tissue repair such asfibrosis or ankylosis is not considered a failure, periapical tissue regen-eration is the ideal outcome of periapical surgery. As stated previously,the host’s blood clot provides an excellent natural scaffold for woundhealing.More conclusive animal studies are needed to determine whichtypes of periapical lesions could benefit from using membrane barriersand/or bone grafts to regenerate new tissues, including PDL andcementum in periapical surgery. However, the results of animal studiesshould be extrapolated with caution to human clinical application(112), even though animal studies are a necessary step before clinicaltrials (113). It appears that we still lack controlled clinical trials witha high level of evidence concerning membrane barriers and/or bonegrafts in periapical surgery.
References1. Langer R, Vacanti JP. Tissue engineering. Science 1993;260:920–6.2. Griffth LG, Naughton G. Tissue engineering: current challenges and expanding
opportunities. Science 2002;295:1009–14.3. Guided tissue regeneration, periodontal. Available at: http://www.symptomstoday.
com/medical/guided_tissue_regeneration_periodontal.htm. Accessed March2010.
4. Melcher AH. On the repair potential of periodontal tissues. J Periodontol 1976;47:256–60.
5. Nyman S, Lindhe J, Karring T, Rylander H. New attachment following surgical treat-ment of human periodontal disease. J Clin Periodontol 1982;9:290–6.
6. Caton JG, DeFuria EL, Polson AM, Nyman S. Periodontal regeneration via selectivecell repopulation. J Periodontol 1987;58:546–52.
7. Nyman S, Gottlow J, Lindhe J, Karring T, Wennstrom J. New attachment formationby guided tissue regeneration. J Periodontal Res 1987;22:252–4.
8. Bashutski JD, Wang H-L. Periodontal and endodontic regeneration. J Endod 2009;35:321–8.
9. Misch CE, Dietsh F. Bone-grafting materials in implant dentistry. Implant Dent1993;2:158–67.
10. Bartold PM, McCulloch CAG, Narayanan AS, Pitaru S. Tissue engineering: a newparadigm for periodontal regeneration based on molecular and cell biology.Periodontol 2000 2000;24:253–69.
11. Dragoo MR, Sullivan HC. A clinical and histological evaluation of autogenous iliacbone grafts in humans. J Periodontol 1973;44:599–613.
12. Moskow BS, Karsh E, Stein SD. Histological assessment of autogenous bone graft:a case report and critical evaluation. J Periodontol 1979;50:291–300.
13. Egelberg J. Regeneration and repair of periodontal tissue. J Periodont Res 1987;22:233–42.
14. Karring T, Nyman S, Gottlow J, Laurell L. Development of the biological concept ofguided tissue regeneration: animal and human studies. Periodontol 2000;1993(1):26–35.
15. Becker W, Becker BE. Periodontal regeneration: a contemporary evaluation. Pe-riodontol 2000;1999(19):104–14.
16. Reynolds MA, Aichelmann-Reidy ME, Branch-Mays GL, Gunsolley JC. The efficacyof bone replacement grafts in the treatment of periodontal osseous defects:a systematic review. Ann Periodontol 2003;8:227–65.
17. Saad AY, Abdellatief EM. Healing assessment of osseous defects of periapicallesions associated with failed endodontically treated teeth with use of freeze-dried bone allograft. Oral Surg Oral Med Oral Pathol 1991;71:612–7.
18. Pinto VS, Zuolo ML, Mellonig JT. Guided bone regeneration in the treatment ofa large periapical lesion: a case report. Pract Periodontic Aesthe Dent 1995;7:76–82.
19. Taschieri S, Del Fabbro M, Testori T, Saita M, Weinstein R. Efficacy of guided tissueregeneration in the management of through-and through lesions following surgicalendodontics: a preliminary study. Int J Periodontics Restorative Dentistry 2008;28:265–71.
20. Apaydin ES, Torabinejad M. The effect of calcium sulfate on hard-tissue healingafter periapical surgery. J Endod 2004;30:17–20.
21. Beck-Coon RJ, Newton CW, Kafrawy AH. An in vivo study of the use of a nonresorb-able ceramic hydroxyapatite as an alloplastic graft material in periapical surgery.Oral Surg Oral Med Oral Pathol 1991;71:483–8.
624 Lin et al.
22. Yoshikawa G, Murashima Y, Wadachi R, Sawada N, Suda H. Guided bone regen-eration (GBR) using membrane and calcium sulfate after apicectomy: a compara-tive histomorphometrical study. Int Endod J 2002;35:255–63.
23. Page RC. The role of inflammatory mediators in the pathogenesis of periodontaldisease. J Periodontol Res 1991;26:230–42.
24. Stashenko P, Teles R. Periapical inflammatory responses and their modulation.Crit Rev Oral Biol Med 1998;9:498–521.
25. Laurell L, Gottlow J. Guided tissue regeneration update. Int Dent J 1998;48:386–98.
26. Bystrom A, Happonen RP, Sjgren U, Sundqvist G. Healing of periapical lesion ofpulpless teeth after endodontic treatment with controlled asepsis. Endod DentTraumatol 1987;3:58–63.
27. Clark RAF. The molecular and cellular biology of wound repair. 2nd ed. New York:Plenum Press; 1996.
28. Witte Mb, Barbul A. General principle of wound healing. Surg Clin North Am 1997;77:509–28.
29. Cotran RS, Kumar V, Collins T. Robbin’s pathologic basis of disease. 6th ed. Phil-adelphia: WB Saunders; 1999.
30. Majno G, Joris I. Cell, tissue, and disease. 2nd ed. Oxford: Oxford University Press;2004.
31. Kruse FE, Volcker HE. Stem cells, wound healing, growth factors, and angiogenesisin the cornea. Curr Opin Ophthalmol 1997;8:46–54.
32. Roth C, Lyle S. Cutaneous stem cells and wound healing. Pediatric Res 2006;59:100R–3.
33. Wu Y, Chen PG, Tredget EE. Mesenchymal stem cells enhance wound healingthrough differentiation and angiogenesis. Stem Cell 2007;25:2648–59.
34. Wu Y, Wang J, Scott PG, Tredget EE. Bone marrow-derived stem cells in woundhealing: a review. Wound Repair Regen 2007;15:S18–26.
35. Gurtner GC, Werner S, Barrandon Y, et al. Wound repair and regeneration. Nature2008;453:314–21.
36. Grzesik WJ, Narayanan AS. Cementum and periodontal wound healing and regen-eration. Crit Rev Oral Biol Med 2002;13:474–84.
37. Ivanovski S, Gronthos S, Shi S, Bartold PM. Stem cells in the periodontal ligament.Oral Disease 2006;12:358–63.
38. Slauson DO, Cooper BJ. Mechanisms of disease. 3rd ed. St Louis: Mosby; 2002.39. Goldberg M, Six N, Decup F, et al. Application of bioactive molecules in pulp-
capping situations. Adv Dent Res 2001;15:91–5.40. Aeinehchi M, Eslami B, Ghanbariha M, et al. Mineral trioxide aggregate (MTA) and
calcium hydroxide as pulp-capping agent in human teeth: a preliminary report. IntEndod J 2003;36:225–35.
41. Itota T, Tashiro Y, Tagaki R, et al. Dentin regeneration by direct pulp capping usinga bioabsorbable material. J Oral Tissue Engin 2006;4:17–24.
42. Nair PNR, Ducan HF, Pitt Ford TR, Luder HU. Histological, ultrastructural andquantitative investigations on the response of healthy human pulps to experimentalcapping with mineral trioxide aggregate: a randomized controlled trial. Int Endo J2008;41:128–50.
43. Lindskog S, Blomlof L, Hammarstrom L. Cellular colonization of denuded rootsurfaces in vivo: cell morphology in dentin resorption and cementum repair. JClin Periodontol 1987;14:390–5.
44. Seo BM, Miura M, Gronthos S, et al. Investigation of multipotent postnatal stemcells from human periodontal ligament. Lancet 2004;364:149–55.
45. Bartold PM, Shi S, Gronthos S. Stem cells and periodontal regeneration. Periodon-tol 2000 2006;40:164–72.
46. Pittenger MF, Mackay AM, Beck SC, et al. Multilineage potential of adult humanmesenchymal stem cells. Science 1999;284:143–7.
47. De Bari C, Dell’Accio F, Vanlauwe J, et al. Mesenchymal multipotency of adult peri-osteal cells demonstrated by single-cell lineage analysis. Arthritis Rheum 2006;54:1209–21.
48. Alexander D, Kalkreuter P, Munz A, et al. Jaw periosteal cells: a suitable source formesenxchymal stem cells? Eur Cell Materials 2007;14(Suppl 1):48.
49. Albert B, Johnson A, Lewis J, et al. Molecular biology of the cell. 5th ed. New York:Garland Science; 2008.
50. Nair PNR. Pathogenesis of apical periodontitis and the causes of endodontic fail-ures. Crit Rev Oral Biol Med 2004;15:348–81.
51. Dahlin C, Linde A, Gottlow J, Nyman S. Healing of bone defects by guided tissueregeneration. Plast Reconstr Surg 1988;81:672–6.
52. Dahlin C, Gottlow J, Linde A, Nyman S. Healing of maxillary and mandibular bonedefects using a membrane technique: an experimental study in monkeys. Scand JPlast Reconstr Hand Surg 1990;24:13–9.
53. Baek SH, Broome C, Zechner W, Kim S. Healing of through-and-throughosseous defects by membrane barrier technique in ferrets. J Endod 1995;21:228, RS 52.
54. Baek S-H, Kim S. Bone repair of experimentally induced through-and throughdefects by Gore-Tex, Guidor, and Vicryl in ferrets: a pilot study. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2001;91:710–4.
JOE — Volume 36, Number 4, April 2010

Review Article
55. Pecora G, Kim S, Celletti R, Davarpanah M. The guided tissue regeneration prin-ciple in endodontic surgery: one-year postoperative results of large periapicallesions. Int Endod J 1995;28:41–6.
56. Pecora G, Baek S-H, Rethnam S, Kim S. Barrier membrane techniques inendodontic surgery. Dent Clin North Am 1997;41:1–16.
57. Ten Cate R. Oral histology. 5th ed. St Louis: Mosby; 1998.58. Direkze NC, Forbes SJ, Brittan M, et al. Mutiple organ engraftment by bone-
marrow-derived myofibroblasts and fibroblasts in bone-marrow-transplantedmice. Stem Cell 2003;21:514–20.
59. Ebihara Y, Masuya M, Larue AC, et al. Hematopoietic origins of fibroblasts: II—in vitro studies of fibroblasts, CFU-F, and fibrocytes. Exp Haematol 2006;34:219–29.
60. Andreasen JO, Rud J. Modes of healing histologically after endodontic surgery in70 cases. Int Oral Surg 1972;1:148–60.
61. Rud J, Andreasen JO, Moller-Jensen JE. A multivariate analysis of the influence ofvarious factors upon healing after endodontic surgery. Int J Oral Surg 1972;1:258–71.
62. Ridley AJ, Schwartz MA, Burridge K, et al. Cell migration: integrating signals fromfront to back. Science 2003;302:1704–9.
63. Mutsaers SE, Bishop JE, McGrouther G, Laurent GJ. Mechanisms of tissue repair:from wound healing to fibrosis. Int J Biochem Cell Biol 1997;29:5–17.
64. Wynn TA. Cellular and molecular mechanisms of fibrosis. J Pathol 2008;214:199–210.
65. Bohning BP, Davenport WD, Jeansonne BJ. The effect of guided tissue regenerationon the healing of osseous defects in rat calvaria. J Endod 1999;25:81–4.
66. Garrett K, Kerr M, Hartwell G, O’Sullivan S, Mayer P. The effect of a bioresorbablematrix barrier in endodontic surgery on the rate of periapical healing: an in vivostudy. J Endod 2002;28:503–6.
67. Britain SK, von Arx T, Schenk RK, et al. The use of guided tissue regeneration prin-ciples in endodontic surgery for induced chronic periodontic-endodontic lesions:a clinical, radiographic and histological evaluation. J Periodontol 2005;76:450–60.
68. Rankow HJ, Krasner PR. Endodontic applications of guided tissue regeneration inendodontic surgery. J Endod 1996;22:34–43.
69. Pompa DG. Guided tissue repair of complete buccal dehiscences associated withperiapical defects: a clinical retrospective study. J Am Dent Assoc 1997;128:989–97.
70. Oh S-L, Fouad AF, Park S-H. Treatment strategy for guided tissue regeneration incombined endodontic-periodontic lesions: case report and review. J Endod 2009;35:1331–6.
71. Nyman S, Karring T. Regeneration of surgically removed buccal alveolar bone indogs. J Periodontal Res 1979;14:86–92.
72. Lindhe J, Nyman S, Karring T. Connective tissue reattachment as related to pres-ence or absence of alveolar bone. J Clin Periodontol 1984;11:33–40.
73. Gottlow J, Nyman S, Karring T, Lindhe J. New attachment formation as the result ofcontrolled tissue regeneration. J Clin Periodontol 1984;11:494–503.
74. Sculean A, Nikolidakis D, Schwarz F. Regeneration of periodontal tissues:combination of barrier membranes and grafting materials—biological founda-tion and preclinical evidence: a systematic review. J Clin Periodontol 2008;35:106–16.
75. Mellonig JT, Nevins M, Sanchez R. Evaluation of a bioabsorbable physical barrierfor guided bone regeneration: part II—material and bone replacement graft. Int JPeriodontics Restorative Dent 1998;18:129–37.
76. Schwartz Z, Mellonig JT, Carnes DL Jr, et al. Ability of commercial demineralizedfreeze-dried bone allograft to induce new bone formation. J Periodontol 1995;67:918–26.
77. Gouldin AG, Fayad S, Mellonig JT. Evaluation of guided tissue regeneration in inter-proximal defects: II—membrane and bone versus membrane alone. J Clin Perio-dontol 1996;23:485–91.
78. Pecora G, Andreana S, Margarone JE, Covani U, Sottosanti JS. Bone regenerationwith a calcium sulfate barrier. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1997;84:424–9.
79. Pecora G, Leonardis De, Ibrahim N, Bovi M, Cormelini R. The use of calciumsulfate in the surgical treatment of a ‘‘through and through’’ periradicular lesion.Int Endod J 2001;34:189–97.
80. Taschieri S, Del Fabbro M, Testori T, Weinstein R. Efficacy of xenogenic bone graft-ing with guided tissue regeneration in the management of bone defects aftersurgical endodontics. J Oral Maxillofac Surg 2007;65:1121–7.
81. Tobon SI, Arismendi JA, Marin ML, Mesa AL, Valencia JA. Comparison betweena conventional technique and two bone regeneration techniques in periradicularsurgery. Int Endod J 2002;35:635–41.
82. Demiralp B, Kecali HG, Muhtarogullari M, Serperr A, Demiralp B, Eratalay K.Treatment of periapical inflammatory lesion with the combination of platelet-rich plasma and tricalcium phosphate: a case report. J Endod 2004;30:796–800.
JOE — Volume 36, Number 4, April 2010
83. Stassen LFA, Hislop WS, Still DM, Moos KF. Use of anorganic bone in periapicaldefcts following apical surgery: a prospective trial. Br J Oral Maxillofacial Surg1994;32:83–5.
84. Kierszenbaum AL. Histology and cell biology. St Louis: Mosby; 2002.85. Al-Aql ZS, Alagl AS, Graves DT, Gerstenfeld LC, Einhorn TA. Molecular mechanisms
controlling bone formation during fracture healing and distraction osteogenesis. JDent Res 2008;87:107–18.
86. Albrektsson T, Johansson C. Osteinductiion, osteoconduction and osteointegra-tion. Eur Spine J 2001;10:S96–101.
87. Bauer TW, Muschler GF. Bone graft materials: an overview of the basic science.Clin Orthopaed Related Res 2000;371:10–27.
88. Bucholz RW. Non allografts osteoconductive bone graft substitutes. Clin OrthopaedRelated Res 2002;395:44–52.
89. Laux M, Abbott PV, Pajarola G, Nair PNR. Apical inflammatory root resorption:a correlative radiographic and histological assessment. Int Endod J 2000;33:483–93.
90. Mosesson MW. Fibrinogen and fibrin structure and functions. J Thrombosis Hae-mostasis 2005;3:1894–904.
91. Martin P. Aiming for perfect skin regeneration. Science 1997;276:75–81.92. Eppley BL, Woodell JE, Higgins J. Platelet quantification and growth factor analysis
from platelet-rich plasma: implications for wound healing. Plast Reconstr Surg2004;114:1502–8.
93. Werner S, Grose R. Regulation of wound healing by growth factors and cytokines.Physiol Rev 2003;83:835–70.
94. Barrientos S, Stojadinovic O, Golinko MS, et al. Growth factors and cytokines inwound healing. Wound Rep Reg 2008;16:585–601.
95. Maguire H, Torabinejad M, McKendry D, McMillan P, Simon JH. Effects of resorb-able membrane placement and human osteogenic protein-1 on hard tissue healingafter periradicular surgery in cats. J Endod 1998;24:720–5.
96. Bergenholtz G, Wikesjo UME, Sorensen RG, Xiropaidis AV, Wozney JM. Observa-tions on healing following endodontic surgery in nonhuman primates (Macaca fas-cicularis): effects of rhBMP-2. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2006;101:116–25.
97. Regan JD, Gutmann JL, Lacopino AM, Diekwisch T. Response of periradiculartissues to growth factors introduced into the surgical site in the root-end fillingmaterial. Int Endod J 1999;32:171–82.
98. Hu W-J, Eaton JW, Ugarova TP, Tang L. Molecular basis of biomaterial-mediatedforeign body reactions. Blood 2001;98:1231–8.
99. Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials.Semin Immunol 2008;20:86–100.
100. Strindberg LZ. The dependence of the results of pulp therapy on certain factors.Acta Odontol Scand 1956;14(Suppl):21.
101. Zeichner-David M. Regeneration of periodontal tissues: cementogenesis revisted.Periodontol 2000;2006(41):106–17.
102. Bosshardt DD. Are cementoblasts a subpopulation of osteoblasts or a uniquephenotype? J Dent Res 2005;84:390–406.
103. Zeichner-Davis M, Oishi K, Su Z, et al. Role of Hertwig’s epithelial root sheath cellsin tooth root development. Dev Dynamics 2003;228:651–63.
104. Sonoyama W, Seo B-M, Yamaza T, Shi S. Human Hertwig’s epithelial root sheathcells play crucial roles in cementum formation. J Dent Res 2007;86:594–9.
105. Andreasen JO. Cementum repair after apicoectomy in humans. Acat Odont Scand1973;31:211–21.
106. Andreasen JO, Rud J, Munksgaard EC. Retrograde filling with resin and a dentinbonding agent: preliminary histologic study of tissue reactions in monkeys. DanishDent J 1989;93:195–7.
107. Andreasen JO, Munksgaard EC, Fredebo L, Rud J. Periodontal tissue regenerationincluding cemtogenesis adjacent to dentin-bonded retrograde composit fillings inhumans. J Endod 1993;19:151–3.
108. Apaydin ES, Shabahang S, Torabinejad M. Hard-tissue healing after application offresh or set MTA as root-end-filling material. J Endod 2004;30:21–4.
109. Baek S-H, Plenk H, Kim S. Periapical tissue responses and cementum regenerationwith amalgam, Super EBA, and MTA as root-end filling materials. J Endod 2005;31:444–9.
110. Tanomaru-Filho M, Luis MR, Leonardo MR, Tanomaru JMG, Silva LAB. Evaluationof periapical repair following retrograde filling with different root-end filling mate-rials in dog teeth with periapical lesions. Oral Surg Oral Med Oral Pathol Oral Ra-diol Endod 2006;102:127–32.
111. Tsesis I, Faivishevsky V, Kfir A, Rosen E. Outcome of surgical endodontic treatmentperformed by a modern technique: a mets-analysis of literature. J Endod 2009;35:1505–11.
112. Palmer RM, Cortellini P. Periodontal tissue engineering and regeneration:Consensus Report of the Sixth European Workshop on Periodontology. J ClinPeriodontol 2008;35(Suppl 8):83–6.
113. ISO. ISO standards: TC 194—biological evaluation of medical devices. Available at:http://www.iso.org/iso/home.htm. Accessed.
Guided Tissue Regeneration in Periapical Surgery 625