
564
ORIGINAL ARTICLE
Measuring Participation EnfranchisementAllen W. Heinemann, PhD, Jin-Shei Lai, PhD, Susan Magasi, PhD, Joy Hammel, PhD,
John D. Corrigan, PhD, Jennifer A. Bogner, PhD, Gale G. Whiteneck, PhDaUim
H
sHhofinaaa
o
Ca
ABSTRACT. Heinemann AW, Lai J-S, Magasi S, Hammel J,Corrigan JD, Bogner JA, Whiteneck GG. Measuring participationenfranchisement. Arch Phys Med Rehabil 2011;92:564-71.
Objective: To reflect the perspectives of rehabilitationstakeholders in a measure of participation enfranchisement thatcan be used by people with and without disabilities.
Design: Survey.Setting: Community settings.Participants: We pilot-tested a draft instrument with 326
adults who had sustained stroke, spinal cord injury, traumaticbrain injury, or other disabling condition, as well as a generalpopulation sample. We administered a revised version of theinstrument to a statewide sample drawn from the 2006 Colo-rado Behavioral Risk Factors Surveillance System that in-cluded persons with (N�461) and without (N�451) self-iden-tified activity limitations.
Interventions: None.Main Outcome Measure: Participation enfranchisement.Results: We used multidimensional scaling, exploratory factor
analysis (EFA) and confirmatory factor analysis (CFA), followedby rating scale analysis to evaluate the psychometric properties ofthe instrument. EFA identified 3 participation enfranchisementfactors that describe perceived choice and control, contributing toone’s community, and feeling valued; the factors were supportedmarginally by CFA. Rating scale analysis revealed marginal per-son separation and no misfitting items.
Conclusions: Participation enfranchisement constitutes anew, previously unmeasured aspect of participation—one thataddresses subjective perceptions rather than objective perfor-mance—with items that are clearly distinct from more gener-alized satisfaction with participation. The 19 enfranchisementitems describe aspects of participation that may prove useful incharacterizing longer-term rehabilitation outcomes.
Key Words: Patient participation; Psychometrics; Rehabil-itation.
© 2011 by the American Congress of RehabilitationMedicine
From the Departments of Physical Medicine and Rehabilitation (Heinemann) andMedical Social Sciences (Lai, Magasi), Feinberg School of Medicine, NorthwesternUniversity, Chicago, IL; the Rehabilitation Institute of Chicago, Chicago, IL (Hei-nemann); University of Illinois at Chicago, Chicago, IL (Hammel); Ohio StateUniversity, Columbus, OH (Corrigan, Bogner); Craig Hospital, Englewood, CO(Whiteneck).
Presented to the American Psychological Association, August 19, 2007, SanFrancisco, CA; the American Congress of Rehabilitation Medicine, October 6, 2007,Washington, DC; and the American Psychological Association Division 22, April 6,2008, Tucson, AZ.
Supported by the National Institute on Disability and Rehabilitation Researchthrough a grant from the Rehabilitation Research and Training Center on MeasuringRehabilitation Outcomes and Effectiveness (grant no. H133B040032).
No commercial party having a direct financial interest in the results of the researchsupporting this article has or will confer a benefit on the authors or on any organi-zation with which the authors are associated.
Reprint requests to Allen W. Heinemann, PhD, Rehabilitation Institute of Chicago,345 E Superior St, Chicago, IL 60611-2654, e-mail: [email protected].
Published online March 2, 2011 at www.archives-pmr.org
0003-9993/11/9204-00166$36.00/0doi:10.1016/j.apmr.2010.07.220
Arch Phys Med Rehabil Vol 92, April 2011
THE WORLD HEALTH Organization’s ICF1 defines par-ticipation as involvement in life situations and refers to
ctive engagement in real world activities and environments.nfortunately, neither the ICF’s definition of participation nor
ts taxonomy of activities and participation provides a clearechanism to operationalize participation.A review of participation measures indicates that the Craig
andicap Assessment and Reporting Technique2 is perhaps themost widely used measure of participation in disability re-search.3 While both the original 38-item Craig Handicap As-essment and Reporting Technique and the 18-item Craigandicap Assessment and Reporting Technique–short formave demonstrated good reliability and validity, they are basedn an earlier conceptual framework (the International Classi-cation of Impairment, Disability and Handicap4), providearrow consideration of settings in which participation occurs,nd were developed with limited input from people with dis-bilities. Other instruments used to measure participation, suchs the Community Integration Measure5 and the Community
Integration Questionnaire,6 were developed for specific reha-bilitation populations like people with TBIs and may not beapplicable to other populations. In addition, none of theseinstruments accounts for other influences that may affect par-ticipation—personal preferences and environmental, social,and economic factors.
In response to these limitations, a new generation of partic-ipation measures is being developed that corresponds to con-temporary definitions of participation, evaluates the subjectiveexperiences of people with disabilities, and seeks to capitalizeon contemporary measurement theories such as item responsetheory (eg, Participation Measure for Post-Acute Care,7 Impactn Participation and Autonomy Questionnaire,8 Participation
Survey/Mobility9). The Participation Measure for Post-Acuteare is a 65-item fixed-length measure, and a computerizeddaptive testing platform has been developed as well.10 The
Participation Measure for Post-Acute Care focuses on partici-pation limitations, represents items inconsistently across do-mains, and is somewhat cumbersome to administer with 65items. The computer adaptive testing version offers more effi-cient administration with only modest reductions in sensitivity
List of Abbreviations
BRFSS Behavioral Risk Factor Surveillance SystemCFA confirmatory factor analysisCFI comparative fit indexCPI Community Participation IndicatorsDIF differential item functioningEFA exploratory factor analysisICF International Classification of Functioning,
Disability and HealthMDS multidimensional scalingRMSE root mean square errorRSQ squared correlation fit indexTBI traumatic brain injury
TLI Tucker-Lewis index
o
Cmf
ocrviccgtpgbspiaasttp
mbtvrpigbt
fsetvmpduspwo
I
smr
565MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
and responsiveness.10 The Impact on Participation and Auton-my Questionnaire8 integrates principles of decisional auton-
omy within the ICF framework using 32 items across 5 sub-domains. Although this questionnaire emphasizes subjectiveappraisals of participation across 6 of the ICF’s activity andparticipation domains, it does not document objective perfor-mance, nor does it explore how contextual factors influenceparticipation. The Participation Survey/Mobility assesses ob-jective performance, subjective evaluation, participation sup-ports (people, devices, etc.), and health-related impairments in20 activity categories. However, it is lengthy and complex, andit focuses on mobility impairments. A limitation of many ofthese participation measures is that they were developed withlimited stakeholder input (Participation Measure for Post-Acute Care) or focused on a limited range of disabling condi-tions (Participation Survey/Mobility). Furthermore, while theICF framework describes participation outcomes as an inter-action between a person’s body structure and function, personfactors, and environmental contexts, most measures assessparticipation or environmental factors; no measure describesthe dynamic interplay with the environment that frames peo-ple’s experiences of participation.
Other recent approaches to participation measurement em-phasize perceived involvement in society, fulfilling one’s po-tential, and self-direction. van de Ven et al11 attempt to reflectpeople’s perception of environmental and societal barriers andopportunities and how they influence participation choice andcontrol. Their instruments link participation and context inter-action and ground ratings in the experience of persons withdisabilities. Townley and Kloos12 developed the Brief Sense of
ommunity Index that reflects themes of social connections,utual concerns, community values, and disability acceptance
or persons with mental illness residing in community settings.We reported in 2 previous publications our methods to
btain input in defining the construct of participation as con-eptualized by rehabilitation stakeholders, and to use theseesults to assess participation that is grounded in and sociallyalidated by these stakeholders.13,14 Eighteen focus groupsncluding 148 participants representing diverse consumers,aregivers, providers, payers, and policy-makers were held toapture the meaning of participation. We transcribed eachroup’s discussion, then coded, analyzed, and reviewed theranscripts. We compared the perspectives of insiders—that is,eople with disabilities (n�63)—with the perspectives of care-ivers and important others, rehabilitation professionals, reha-ilitation funders, and national policy-makers (n�75). Con-umers conceptualized participation as a cluster of valuesertaining to enfranchisement that included active and mean-ngful engagement/being a part of; choice and control; accessnd opportunity; personal and societal responsibilities; havingn impact and supporting others; and social connection, inclu-ion, and membership. Although various stakeholders sharedhemes related to the importance and values of full participa-ion, each group emphasized different priorities about the out-ut required from participation assessment.A valid participation measure should not only be psycho-etrically sound and easy to administer, score and interpret,
ut also reflect a variety of stakeholder perspectives, considerhe settings in which people live, and not expect all people toalue all forms of participation. It is the ultimate goal of thisesearch team to develop such a comprehensive measure ofarticipation from the perspective of multiple stakeholders thatncludes both objective and subjective assessments. While thislobal objective has not been achieved, major progress haseen made in advancing the measurement of 1 aspect of par-
icipation that directly reflects the way people with disabilitiesrame participation in their own lives. Thus, the purpose of thistudy is to report the development of a measure of participationnfranchisement that assesses the extent to which people feelhey participate in the community in a manner that is personallyaluable, as opposed to assessing actual performance of com-unity-based activities. This study evaluated the psychometric
roperties of participation enfranchisement items with diverseisability and general population samples, reflecting the pop-lation for which the instrument is intended. Development of aeparate measure derived from engagement items (measuringerformance of community-based activities) is reported else-here given our collaboration with TBI Model System collab-rators that proceeded in parallel.15
METHODS
nstrument DevelopmentMixed method approaches that integrate qualitatively derived
takeholder perspectives with the state-of-the-art in psycho-etrics and measurement theory are emerging as the standard for
igorous instrument development.16 Qualitative methodologies areused to develop conceptual frameworks on which instruments arebased and to write items that incorporate language that reflects thefirst-hand experiences of the target population. After a processof cognitive testing to ensure item comprehension, measuresare field-tested with the target population. Data from the fieldtest are evaluated using methods such as item response theory,factor analysis, and multidimensional scaling to select itemsand determine the instrument’s measurement properties.
We used this process to create a new measure that seeks toaddress the limitations in participation measurement described.We completed a thorough literature review of participation mea-sures and reported the findings of the qualitative focus group workpreviously.14 Three aspects of participation emerged from thiscross-group analysis: (1) engagement, (2) evaluation, and (3)participation enfranchisement. Engagement refers to how muchone participates in activities within 3 domains (productivity,social participation, being out and about in the community),and evaluation refers to subjective ratings of satisfaction withina participation domain. We defined participation enfranchise-ment as a set of perceptions and values that give meaning toparticipation and that apply across domains. Therefore, unlikeengagement and evaluation, enfranchisement is not tied to aparticular activity or form of participation.
While participation enfranchisement is clearly a complexconstruct, we believe at its core is the assessment of whetherthe community in which a person participates actually valuestheir participation. Enfranchisement is the antithesis of disen-franchisement. Examples of disenfranchisement might includebeing a member of a racial or ethnic group that a community orsociety explicitly or implicitly discriminates against, beingfrom a different cultural background that is misunderstood anddisrespected by the community, or being labeled (eg, sexoffender, illegal alien) in a way that is abhorred by the com-munity. In contrast, positive enfranchisement reflects belong-ingness to one’s community or society.
We drafted participation enfranchisement items using assource material a comprehensive literature review and the focusgroup transcripts and value themes. We used a 4-category rating scalefor the enfranchisement items to reflect how true each statementwas for respondents—that is, to what extent the item reflectedtheir life experiences and participation opportunities. We con-ducted cognitive interviews with 16 adults with spinal cordinjury or TBI in Colorado, Illinois, and Ohio to ascertain thatitems were understood and responded to in the manner in-
tended. Using the guide by Willis,17 we asked respondents toArch Phys Med Rehabil Vol 92, April 2011

pdwabma
ym
ftsiw
i
wa
rmtsosgvtsscveW
566 MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
A
repeat the question in their own words, explain the meaning ofeach item, and offer alternate phrasing when comprehensionwas limited. Interviewers kept detailed notes that the researchteam reviewed.
Institutional review boards at Craig Hospital, NorthwesternUniversity, and Ohio State University approved the proceduresused in this study.
Data SourcesPsychometric evaluation of the participation enfranchise-
ment items occurred along with other types of participationitems included in the larger CPI instrument and involved 2phases of data collection: (1) pilot data collection and (2)telephone interviews with a randomly selected, statewide sam-ple as part of an addendum to the BRFSS administered inColorado.
Pilot sample. We recruited a pilot sample of 258 consum-ers, 108 at the Rehabilitation Institute of Chicago, 100 at CraigHospital, and 50 at Ohio State University. By selection, im-pairments included spinal cord injury (103), TBI (80), stroke(72), and other impairments (3). We also recruited 68 generalpopulation respondents using random digit telephone dialing.Women made up 33% of the disability sample and 71% of thegeneral population sample. White respondents were the largestracial group for the disability (77%) and for the general pop-ulation sample (90%). Mean age � SD was 47�16 years forthe disability sample and 54�17 years for the general popula-tion sample.
BRFSS sample. After analysis of pilot data and instrumentrevision, we recruited a sample with diverse disabilities drawnfrom the general population as well as a sample from thenondisabled general population using random digit dialing. TheColorado Department of Public Health administered the instru-ment as an addendum to the 2006 BRFSS. The BRFSS wasdeveloped by the Centers for Disease Control and Prevention;it is designed to track health risks in the United States. We used2 standard BRFSS questions to determine whether respondentshad a disability (“Are you limited in any activities because ofphysical, mental, or emotional problems?” and “Do you haveany health problem that requires you to use special equip-ment?”). Approximately 20% of the general population re-sponded positively to 1 or both of these screener questions,18
which is nearly identical to the 21% found in Colorado.By oversampling people with disabilities, about half of the
BRFSS sample (n�461) had a self-identified disability, andhalf (n�451) did not. The statewide sample was 94% white (vs84% in the 2006–2008 American Community Survey19); edu-cational attainment included less than high school (6%), highschool (21%), and more than high school education (73% vs12%, 24%, and 64%, respectively, in the survey). The meanand median ages were 55 years (SD�16 vs 35.6y in thesurvey). Women made up 63% of the sample (vs 50% in thesurvey). White subjects, women, persons with more years ofeducation, and older adults were overrepresented comparedwith Colorado’s population.
Statistical ApproachMultidimensional scaling. MDS20 is an exploratory ap-
roach that is suited to the diverse content of the CPI. Itescribes the proximity of items and assesses the extent tohich a conceptual framework is reflected in the data. MDS,
lso known as perceptual mapping, calculates relative distancesetween all items based on responses and positions them on aap. MDS involves several steps: (1) selecting an initial item
t a desired initial dimensionality; (2) computing the distances
rch Phys Med Rehabil Vol 92, April 2011
between the items and comparing the relationships with ameasure of fit; (3) continuing iterations until the best improve-ment of fit is obtained and the proportion of the variance notaccounted for by the model is minimized; then (4) reducing thedimensionality by 1, and repeating the process iteratively untilthe lowest dimensionality with acceptable fit is reached. Weconducted MDS with SPSS, Version 17.0a using the program’sdefault parameters with half of the sample (n�459). The num-ber of dimensions among items is determined by examining thechange in unexplained variance (ie, stress measures) whendecreasing the number of dimensions, which is conceptuallysimilar to the scree plot used in EFA. The location of the elbowof the MDS scree plot indicates substantial improvement in thegoodness of fit, and therefore, the most appropriate number ofdimensions. The squared correlation fit index, RSQ, is definedas the proportion of variance accounted for by the MDS pro-cedure, which is similar to the R2 in multiple regression anal-sis. RSQ values of .60 and greater are considered acceptableodel fit.20
EFA and CFA. After identifying the 19 participation en-ranchisement items as a distinct group, we used EFA with halfhe sample, selected the most parsimonious solution, and thenought to replicate the factor structure with CFA. EFA wasmplemented with SPSS software using Promax rotation; CFAas implemented with Mplus softwareb using the weighted
least squares estimation procedure on the second half of thesample. We defined adequate fit as CFI and TLI values greaterthan .90 and RMSE less than .08.21 Weakly loading items weredentified by squared item loadings less than .30.22 We examined
residual correlations to identify occurrences of local depen-dence; the criterion was a residual correlation between itempairs greater than .20.
Rating scale analysis. Once conceptually linked itemsere identified with MDS, we used rating scale (or Rasch)
nalysis23 to evaluate the psychometric properties of item sets.Rasch analysis provides a method of (1) describing the hierar-chy of item endorsement, (2) describing a person’s positionalong an equal-interval continuum, (3) evaluating the extent towhich items cohere in defining a unidimensional construct, and(4) evaluating the extent to which a person’s responses fit ageneral pattern of item responses. We chose the Rasch modelrather than a 2-parameter or 3-parameter IRT model becauseour purpose was not to fit a model to a unique data set, butrather to assess how well person and item performance corre-sponded to the theoretic ideal of objective, reproducible, andadditive measures. Psychometric criteria used to describe thequality of an instrument include (1) person separation—theratio of person variation to measurement error (�2.0, corre-sponding to a Cronbach � of .80, is desirable), (2) item sepa-ation (the potential range of participation covered by theeasure; values �2.0 are desirable), (3) item misfit—the ex-
ent to which the sample as a whole responds unexpectedly topecific items, (4) person misfit—the extent to which personsr subgroups respond idiosyncratically to the item set, and (5)cale structure—the extent to which respondents use the cate-ories of rating scales consistently (ie, higher ratings on indi-idual items correspond to a higher total degree of participa-ion). Similar to a chi-square statistic, item and person fittatistics summarize the residuals between expected and ob-erved responses. Large mean square infit values (�1.4) indi-ate excessive noise caused by unexpected responses; smallalues (�.6) indicate observed values that are too similar to thexpected values. We used a rating scale model implemented ininsteps.c
We evaluated DIF related to disability status by comparing
item locations on the measurement continuum (ie, item hierar-
False 1.20%
567MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
chy) defined by the sample with and without disabilities. DIFinvolves calibrating the total sample, anchoring the rating scalesteps, and then calibrating the samples with and without disabil-ities separately. Further evaluation of items that demonstrate DIFis warranted because it suggests that these items may not share thesame underlying construct between these subgroups.
Information function and reliability function curves de-scribe an instrument’s precision across its measurementcontinuum. To identify areas requiring improvement, weexamined item and scale information function curves, whichwere produced via the Rasch model. The information func-tion indicates the degree of accuracy with which a person’slevel of the characteristic of interest is estimated along thecontinuum. The item information functions for all itemswere summed to produce a scale information function. Weconverted standard error into reliability and set 0.7 as theminimum acceptable reliability.
RESULTS
Pilot Sample DataAnalysis of the 326 pilot sample cases identified items with
skewed response distributions. We dropped an enfranchise-ment item that was endorsed by nearly the entire sample (“I amnot overly protected or isolated by my family and friends”) andreworded 2 other enfranchisement items. Because of a highlevel of endorsement of most items designed to capture enfran-chisement, we wrote 4 new items (items 16–19) that weexpected would be endorsed less unanimously. Table 1 lists the19 participation enfranchisement items.
Multidimensional Scaling of the BRFSS Sample’s DataWe used MDS with data from the 912 adults who completed
the CPI as part of the BRFSS addendum to identify meaningfulgroups of items that might form reliable subscales. Two di-mensions were identified, and an RSQ value of .610 suggestsgood model fit.
We compared the relative distances between items as well asitem content and then determined the association among items.The participation enfranchisement items and 2 evaluation itemsformed a distinct cluster. Item-scale correlations ranged from.26 to .65. The 2 evaluation items correlated least well with theother items in this group. Excluding these 2 evaluation items,“Do you talk or spend time with your family as often as youwould like?” and “Do you talk or spend time with your friendsas often as you would like?” correlations ranged from .45 to.65. The engagement items made up the second group. TheMDS results clearly indicated that the participation enfran-chisement items represented a coherent item pool differentfrom that measured by the engagement items, and for thisreason, our focus turned to elucidating the nature of this itempool. Additional study of the engagement items was conductedin collaboration with our TBI Model Systems collaborators andreported elsewhere.15
EFA and CFAWe estimated reliability for the 19 enfranchisement items
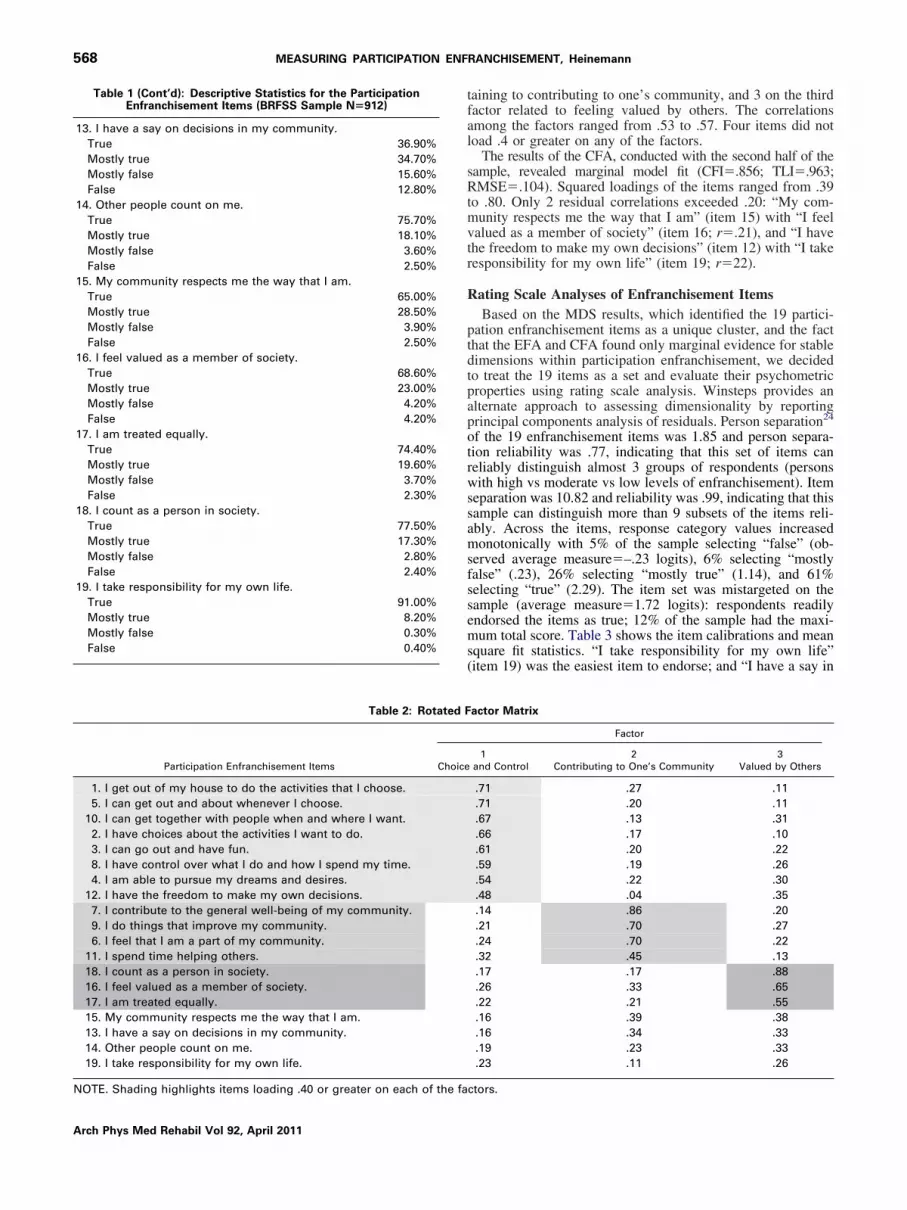
and observed a Cronbach alpha of .91. The item-total correla-tions ranged from .13 to .69. The EFA yielded 4 factors withinitial eigenvalues greater than 1.0; they accounted for 59.6%of the variance. The scree plot and item loadings suggested that3 factors were an optimal solution; they accounted for 54.2% ofthe variance. Table 2 shows the rotated factor matrix. Factor 1contains 8 items that loaded .40 or greater on the first factor
pertaining to choice and control, 4 on the second factor per-Table 1: Descriptive Statistics for the ParticipationEnfranchisement Items (BRFSS Sample N�912)
1. I get out of my house to do the activities that I choose. [Wouldyou say that statement is:]
True 70.60%Mostly true 23.20%Mostly false 3.10%False 3.10%
2. I have choices about the activities I want to do.True 68.90%Mostly true 25.80%Mostly false 3.00%False 2.30%
3. I can go out and have fun.True 75.70%Mostly true 16.60%Mostly false 3.60%False 4.10%
4. I am able to pursue my dreams and desires.True 49.00%Mostly true 34.40%Mostly false 8.50%False 8.10%
5. I can get out and about whenever I choose.True 72.00%Mostly true 19.50%Mostly false 3.70%False 4.70%
6. I feel that I am a part of my community.True 57.00%Mostly true 25.40%Mostly false 9.70%False 7.90%
7. I contribute to the general well-being of my community.True 49.70%Mostly true 30.50%Mostly false 10.80%False 8.90%
8. I have control over what I do and how I spend my time.True 71.60%Mostly true 22.40%Mostly false 3.10%False 2.90%
9. I do things that improve my community.True 45.50%Mostly true 32.40%Mostly false 11.70%False 10.50%
10. I can get together with people when and where I want.True 62.70%Mostly true 25.40%Mostly false 6.30%False 5.70%
11. I spend time helping others.True 60.50%Mostly true 28.20%Mostly false 5.80%False 5.40%
12. I have the freedom to make my own decisions.True 83.40%Mostly true 14.60%Mostly false 0.80%
Arch Phys Med Rehabil Vol 92, April 2011
False 0.40%
NOTE. Shading highlights items loading .40 or greater on each of the fa
568 MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
Arch Phys Med Rehabil Vol 92, April 2011
taining to contributing to one’s community, and 3 on the thirdfactor related to feeling valued by others. The correlationsamong the factors ranged from .53 to .57. Four items did notload .4 or greater on any of the factors.
The results of the CFA, conducted with the second half of thesample, revealed marginal model fit (CFI�.856; TLI�.963;RMSE�.104). Squared loadings of the items ranged from .39to .80. Only 2 residual correlations exceeded .20: “My com-munity respects me the way that I am” (item 15) with “I feelvalued as a member of society” (item 16; r�.21), and “I havethe freedom to make my own decisions” (item 12) with “I takeresponsibility for my own life” (item 19; r�22).
Rating Scale Analyses of Enfranchisement ItemsBased on the MDS results, which identified the 19 partici-
pation enfranchisement items as a unique cluster, and the factthat the EFA and CFA found only marginal evidence for stabledimensions within participation enfranchisement, we decidedto treat the 19 items as a set and evaluate their psychometricproperties using rating scale analysis. Winsteps provides analternate approach to assessing dimensionality by reportingprincipal components analysis of residuals. Person separation24
of the 19 enfranchisement items was 1.85 and person separa-tion reliability was .77, indicating that this set of items canreliably distinguish almost 3 groups of respondents (personswith high vs moderate vs low levels of enfranchisement). Itemseparation was 10.82 and reliability was .99, indicating that thissample can distinguish more than 9 subsets of the items reli-ably. Across the items, response category values increasedmonotonically with 5% of the sample selecting “false” (ob-served average measure�–.23 logits), 6% selecting “mostlyfalse” (.23), 26% selecting “mostly true” (1.14), and 61%selecting “true” (2.29). The item set was mistargeted on thesample (average measure�1.72 logits): respondents readilyendorsed the items as true; 12% of the sample had the maxi-mum total score. Table 3 shows the item calibrations and meansquare fit statistics. “I take responsibility for my own life”(item 19) was the easiest item to endorse; and “I have a say in
actor Matrix
Factor
1and Control
2Contributing to One’s Community
3Valued by Others
.71 .27 .11
.71 .20 .11
.67 .13 .31
.66 .17 .10
.61 .20 .22
.59 .19 .26
.54 .22 .30
.48 .04 .35
.14 .86 .20
.21 .70 .27
.24 .70 .22
.32 .45 .13
.17 .17 .88
.26 .33 .65
.22 .21 .55
.16 .39 .38
.16 .34 .33
.19 .23 .33
.23 .11 .26
Table 1 (Cont’d): Descriptive Statistics for the ParticipationEnfranchisement Items (BRFSS Sample N�912)
13. I have a say on decisions in my community.True 36.90%Mostly true 34.70%Mostly false 15.60%False 12.80%
14. Other people count on me.True 75.70%Mostly true 18.10%Mostly false 3.60%False 2.50%
15. My community respects me the way that I am.True 65.00%Mostly true 28.50%Mostly false 3.90%False 2.50%
16. I feel valued as a member of society.True 68.60%Mostly true 23.00%Mostly false 4.20%False 4.20%
17. I am treated equally.True 74.40%Mostly true 19.60%Mostly false 3.70%False 2.30%
18. I count as a person in society.True 77.50%Mostly true 17.30%Mostly false 2.80%False 2.40%
19. I take responsibility for my own life.True 91.00%Mostly true 8.20%Mostly false 0.30%
Table 2: Rotated F
Participation Enfranchisement Items Choice
1. I get out of my house to do the activities that I choose.5. I can get out and about whenever I choose.
10. I can get together with people when and where I want.2. I have choices about the activities I want to do.3. I can go out and have fun.8. I have control over what I do and how I spend my time.4. I am able to pursue my dreams and desires.
12. I have the freedom to make my own decisions.7. I contribute to the general well-being of my community.9. I do things that improve my community.6. I feel that I am a part of my community.
11. I spend time helping others.18. I count as a person in society.16. I feel valued as a member of society.17. I am treated equally.15. My community respects me the way that I am.13. I have a say on decisions in my community.14. Other people count on me.19. I take responsibility for my own life.
ctors.

P
irTvcwcgttng––t
csf–s7
D
id
lslp
Nm h is s“ ent
569MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
community decisions” (item 13) was the hardest item to en-dorse. All items fit within acceptable limits (mean square infitswere between 0.6 and 1.4) and correlated adequately with theunderlying latent trait. Construct validity is supported by theobservation that persons without self-identified disabilities re-ported a higher level of enfranchisement (x�2.3�1.5 logits)than did persons with disabilities (1.9�1.6 logits; t910�3.88;
�.001).We evaluated the dimensionality of the enfranchisement
tems by completing a principal component analysis of theesidual information after the Rasch measure was extracted.he first residual factor accounted for 64.9% of the totalariance; the second factor explained 4.6%. The first factorontained 3 positively loaded and 3 negatively loaded itemsith loadings that exceeded .40. Positively loading items fo-
used on giving to one’s community (“I contribute to theeneral well-being of my community” [item 7, .60], “I dohings that improve my community” [item 9, .56] and “I feelhat I am a part of my community” [item 6, .55]), whileegatively loading items focused on perceived freedom (“I canet together with people when and where I want [item 10,.57], “I can get out and about whenever I choose” [item 4,.55], and “I have control over what I do and how I spend myime” [item 8, –.50]).
We examined the information function curve for the enfran-hisement items to evaluate the range of scores which areufficiently reliable. The enfranchisement items producedairly precise measures for persons with scale scores between2.5 and 2.5 logits with reliability greater than 0.7. For thisample, whose scaled scores ranged from –2.58 to 3.99 logits,0% of them were measured in a precise manner.
isability Status and DIFWe evaluated disability-related DIF by contrasting the
tem calibrations for the respondents with a self-identified
Table 3: Enfranchisement Item Cali
Measure SEE Infit Mean Square r
1.29 .04 1.20 .60.98 .05 .96 .64.82 .05 .96 .63.76 .05 .94 .60.61 .05 1.05 .60.32 .05 1.10 .54.29 .05 .93 .58.02 .06 1.02 .52
–.01 .06 .95 .56–.10 .06 1.18 .50–.18 .06 .96 .52–.18 .06 .97 .50–.24 .06 .91 .52–.27 .06 1.11 .51–.36 .06 1.11 .48–.39 .07 1.33 .42–.50 .07 1.05 .50
–1.04 .08 .96 .44–1.82 .11 1.18 .32
.00 .06 1.05 Mean
.71 .02 .11 SD
OTE. “Measure” indicates the item location (difficulty) in log-odd uean square” is the inlier-sensitive or information-weighted fit, whic
r” indicates the correlation between the item and the enfranchisem
isability separately from the respondents without a disabil- o
ity using the Winsteps DIF procedure. Two of the itemsdemonstrated disability-related DIF: “I am able to pursuemy dreams and desires” (item 4) and “I can get out andabout whenever I choose” (item 5). The items were signif-icantly more difficult for the sample with disabilities toendorse (Mantel-Haenszel P�.0001, difference�.33 logits;and P�.0002, difference�.41 logits, respectively). Wecomputed the person measures with and without these items.The measures were correlated .99, and the average differ-ence in the measures with and without this item was .10logits, small enough not to create bias in measurement.
DISCUSSION
Participation is a complex construct that can be characterizedin myriad ways in the lives of people from various backgroundsand with varied experiences and preferences who are operatingin diverse social worlds and within the context of societaleconomies, policies, systems, beliefs, and attitudes. This proj-ect developed an item bank that describes an important aspectof participation using the input of stakeholders from diversebackgrounds and perspectives. This report describes the devel-opment of a participation enfranchisement measure that reflectsconsumer perspectives and is applicable to persons with orwithout disabilities.
The participation enfranchisement items form a distinct sub-set of items with an internal consistency estimate of .91. Thecontent reflects perceived freedom to participate in one’s com-munity and having influence in and contributing to the wellbeing of one’s community. The items are closest to constructsof community integration by van de Ven,11 McColl5 and col-eagues, and Townley and Kloos,12 including taking part inociety, trying to fulfill one’s potential, and directing one’s ownife. Participation enfranchisement items may also reflect peo-le’s perception of environmental and societal barriers and
ns for the BRFSS Sample (N�912)
Item
13. I have a say in community decisions.9. I do things to improve my community.7. I contribute to the general well-being of my community.4. I am able to pursue my dreams and desires.6. I feel that I am part of my community.
11. I spend time helping others.10. I can get together with people when and where I want.15. My community respects me the way that I am.16. I feel valued as a member of society.5. I can get out and about whenever I choose.1. I get out of my house to do the activities that I choose.2. I have choices about the activities I want to do.8. I have control over what I do and how I spend my time.3. I can go out and have fun.
17. I am treated equally.14. Other people count on me.18. I count as a person in society.12. I have the freedom to make my own decisions.19. I take responsibility for my own life.
SEE” indicates the standard error of the estimate for the item. “Infitensitive to the pattern of responses to items targeted on the person.measure.
bratio
nits. “
pportunities and how they influence participation choice and
Arch Phys Med Rehabil Vol 92, April 2011

rptaohwwpp
smpecitcctpa
S
sUpsattl
aaps
uptPA
570 MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
A
control; thus, the items tie participation and context interactiontogether and ground ratings in the experience of persons. Theparticipation enfranchisement items are unique and, to ourknowledge, no other participation measure directly evaluatesthe extent to which persons feel enfranchised in their commu-nities and in the broader society. Not all of the focus group–derived categories of enfranchisement values13 were repre-sented adequately in the enfranchisement item pool, and the3-factor solution suggested by EFA was supported marginallywith CFA. Thus, future development should focus on expand-ing the pool of participation enfranchisement items to evaluatemore fully the impact that stakeholder-defined values have onparticipation choice and control.
A more fully developed measure of participation enfran-chisement has the potential to reflect the effects of disabilityand societal influences on community participation for severalapplications, including clinical, program monitoring, and re-search purposes. Clinicians may find that the enfranchisementconstruct provides a point of entry into discussions regardinginvolvement in life situations and the extent to which clientneeds are met. Programs that have as a goal enhancing com-munity participation may find that the construct reflects theeffect of interventions. Researchers may find the constructuseful to monitor population differences and trends. Furtherresearch is required to develop an item pool of sufficient sizethat allows development of measures of participation enfran-chisement that are unidimensional, hierarchic, and internallyconsistent.
The concept of participation has emerged as a central con-cern in rehabilitation theory, clinical practice, and outcomesresearch. Since 2001 when the World Health Organization’sICF1 identified participation as a major component of health,esearchers and clinicians have sought conceptually sound andsychometrically valid participation measures. Unfortunately,he measurement of participation is complicated by conceptualmbiguity and measurement challenges. The ICF’s definitionf participation as involvement in life situations is vague andas proven difficult to operationalize. Debate persists aroundhether performance in normative life roles such as family,ork, and community or satisfaction with one’s ability toarticipate is the most appropriate criteria for characterizingarticipation.25 There is no consensus on optimal ways in
which participation definitions could be operationalized.26 Re-ults from this study inform the World Health Organizationodel of function, disability, and health. The ICF assumes that
articipation occurs in a community context. The participationnfranchisement items reflect the extent to which persons per-eive their community as valuing, respecting, and fully includ-ng them. Thus, one could be highly engaged and yet feel thathe community is hostile or unaccepting. Participation enfran-hisement may tap the extent to which a person experiences theommunity as restricting or enabling participation. Participa-ion enfranchisement issues may also arise from economic,olitical, or attitudinal sources independent of disability, suchs racism and poverty.
tudy LimitationsSeveral study features limit the generalizability of the re-
ults. The pilot sample was obtained from only 3 areas of thenited States and may not reflect all constituent stakeholders’erspective on participation. The BRFSS general populationample obtained by random digit dialing reflects people whore available during the day and early evening and are willingo answer anonymous surveys. The BRFSS sample has rela-ively few persons from minority backgrounds and a higher
evel of education than the general population. Collection ofrch Phys Med Rehabil Vol 92, April 2011
dditional data from larger and disability-specific samples willllow us to evaluate an item pool tapping distinct aspects ofarticipation enfranchisement that are suitable for clinical, re-earch, and policy applications.
CONCLUSIONSParticipation enfranchisement constitutes a new, previously
nmeasured aspect of participation that addresses subjectiveerceptions rather than objective performance and is concep-ually distinct from generalized satisfaction with participation.articipation enfranchisement may be the concept closest to themericans with Disabilities Act27 goal of full participation in
society. This study developed participation enfranchisementitems using the perspectives of rehabilitation stakeholders thatmay be useful to monitor longer-term rehabilitation outcomes.Additional items are needed to evaluate the factor structure ofthe construct. With additional items, we may be able to definedistinct aspects of participation enfranchisement that are uni-dimensional and hierarchic and that may be useful in describ-ing perceived involvement in one’s community.
Acknowledgments: Project team members include ElizabethMorgan, MS, OTR/L, Evelyn Rodriguez, and Robin Jones, MPA,COTA/L, ROH, at the University of Illinois at Chicago; C. A. Brooks,MSHA, and Melissa Sendroy-Terrill, MA at Craig Hospital; and RitaBode, PhD, Holly DeMark Neumann, MPA, Trudy Mallinson, PhD,OTR/L, NZROT, Patrick Semik, BA, and Kendall Stagg, MA, JD atthe Rehabilitation Institute of Chicago. We appreciate the suggestionsprovided by John M. Linacre, PhD, and Jack Stenner, PhD, afterearlier presentations of this work and the editorial review by MarcelDijkers, PhD.
References1. World Health Organization. International classification of func-
tioning, disability and health (ICF). Geneva: WHO; 2001.2. Whiteneck GG, Charlifue SW, Gerhart KA, Overhosler JD, Rich-
ardson GN. Quantifying handicap: a new measure of long-termrehabilitation outcomes. Arch Phys Med Rehabil 1992;73:519-26.
3. Magasi S, Heinemann AW, Whiteneck G. Measurement of par-ticipation following traumatic spinal cord injury: an evidence-based review for research. J Spinal Cord Med 2008;31:34-45.
4. Assessment Classification and Epidemiology Group. Internationalclassification of functioning and disability (ICIDH-2). Beta-2 draftfull version. Geneva: World Health Organization; 1999.
5. McColl MA, Davies D, Carlson P, Johnston J, Minnes P. Thecommunity integration measure: development and preliminaryvalidation. Arch Phys Med Rehabil 2001;82:429-34.
6. Willer B, Rosentha lM, Kreutzer JS, Gordon WA, Remple R.Assessment of community integration following rehabilitation fortraumatic brain injury. J Head Trauma Rehabil 1993;8:75-87.
7. Gandek B, Sinclair SJ, Jette AM, Ware JE. Development andinitial psychometric evaluation of the Participation Measure forPost-Acute Care (PM-PAC). Amer J Phys Med Rehabil 2007;86:57-71.
8. Cardol M, de Haan RJ, van den Bos GA, de Jong BA, de Groot IJ.The development of a handicap assessment questionnaire: theImpact on Participation and Autonomy (IPA). Clin Rehabil 1999;13:411-9.
9. Gray DB, Hollingsworth HH, Stark SL, Morgan KA. ParticipationSurvey/Mobility: psychometric properties of a measure of partic-ipation for people with mobility impairments and limitations.Arch Phys Med Rehabil 2006;87:189-97.
10. Haley SM, Gandek B, Siebens H, et al. Computerized adaptivetesting for follow-up after discharge from in-patient rehabilitation:II. Participation outcomes. Arch Phys Med Rehabil 2008;89:275-
83.
2
2
2
2
2
2
2
2
571MEASURING PARTICIPATION ENFRANCHISEMENT, Heinemann
11. van de Ven L, Post M, de Witte L, van den Heuvel W. It takes twoto tango: the integration of people with disabilities into society.Disabil Soc 2005;20:311-29.
12. Townley G, Kloos B. Development of a measure of sense ofcommunity for individuals with serious mental illness residing incommunity settings. J Community Psychol 2009;37:362-80.
13. Magasi S, Hammel J, Heinemann A, Whiteneck G, Bogner J.Participation: a comparative analysis of multiple rehabilitationstakeholders’ perspectives. J Rehabil Med 2009;41:936-44.
14. Hammel J, Magasi S, Heinemann AW, Whiteneck G, Bogner J,Rodriguez E. What does participation mean? An insider perspectivefrom people with disabilities. Disabil Rehabil 2008;30:1445-60.
15. Bogner JA, Whiteneck GG, Corrigan JD, Lai J-S, Dijkers MP,Heinemann AW. Comparison of scoring methods for the Partici-pation Assessment With Recombined Tools-Objective. Arch PhysMed Rehabil 2011;92:552-63.
16. Ader D. Developing the Patient-Reported Outcomes MeasurementInformation System (PROMIS). Med Care 2007;45:S1-2.
17. Willis GB. Cognitive interviewing and questionnaire design: atraining manual. Working Paper #7, National Center for HealthStatistics. Atlanta: Centers for Disease Control and Prevention;1994.
18. State-specific prevalence of disability among adults—11 statesand the District of Columbia, 1998. Morb Mortal Wkly Rep2000;49:711-4.
19. U.S. Census Bureau. 2006-2008 American community survey. Avail-able at: http://factfinder.census.gov/servlet/ADPTable?_bm�y&-geo_id�04000US08&-qr_name�ACS_2008_3YR_G00_DP3YR2&-ds_name�&-_lang�en&-redoLog�false. Accessed No-
vember 9, 2010.0. Cox MF, Cox MA. Multidimensional scaling. London: Chapmanand Hall; 2001.
1. Hu L, Bentler P. Cutoff criteria for fit indexes in covariancestructure analysis: conventional criteria versus new alternatives.Struct Equ Modeling 1999;6:1-55.
2. Muthen B, du Toit S, Spisic D. Robust inference using weightedleast squares and quadratic estimating equations in latent variablemodeling with categorical and continuous outcomes. 1987. Avail-able at: http://www.gseis.ucla.edu/faculty/muthen/articles/Article_075.pdf. Accessed June 12, 2010.
3. Rasch G. Probabilistic models for some intelligence and attain-ment tests. Copenhagen: Danish Institute for Educational Re-search; 1960.
4. Wright BD, Stone MH. Measurement essentials. 2nd ed. Wilming-ton: Wide Range, Inc; 1999.
5. Whiteneck G, Dijkers MP. Difficult to measure constructs: con-ceptual and methodological issues concerning participation andenvironmental factors. Arch Phys Med Rehabil 2009;90(Suppl11):S22-35.
6. Field MJ, Jette AM, Institute of Medicine (U.S.). Committee onDisability in America: a new look. The future of disability inAmerica. Washington (DC): National Academies Pr; 2007.
7. Americans with Disabilities Act of 1990. In: Congress US, ed.Public Law No: 101-3361990. Available at: http://www.ada.gov/pubs/ada.htm. Accessed February 17, 2011.
Suppliersa. SPSS Inc, 233 S Wacker Dr, 11th Fl, Chicago, IL 60606.b. Muthén & Muthén, 3463 Stoner Ave, Los Angeles, CA 90066.
b. Winsteps. Available at http://www.winsteps.com.Arch Phys Med Rehabil Vol 92, April 2011
Recommended

















