Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=iode20
Download by: [The State University of New York] Date: 11 September 2015, At: 07:58
Acta Odontologica Scandinavica
ISSN: 0001-6357 (Print) 1502-3850 (Online) Journal homepage: http://www.tandfonline.com/loi/iode20
Retention of Titanium Tetrafluoride (TIF4), used asFissure Sealant on Human Deciduous Molars
Tamer Büyükyilmaz, Bilge Hakan Sen & Bjørn Øgaard
To cite this article: Tamer Büyükyilmaz, Bilge Hakan Sen & Bjørn Øgaard (1997) Retentionof Titanium Tetrafluoride (TIF4), used as Fissure Sealant on Human Deciduous Molars, ActaOdontologica Scandinavica, 55:2, 73-78
To link to this article: http://dx.doi.org/10.3109/00016359709115395
Published online: 02 Jul 2009.
Submit your article to this journal
Article views: 27
View related articles
Citing articles: 1 View citing articles

Retention of titanium tetrafluoride (TiF*), used as fissure sealant on human deciduous molars
Tamer Buyukyilmaz, Bilge Hakan Sen and Bj0rn 0gaard Department of Orthodontics, Faculty of Dentistry, University of Oslo, Oslo, Norway, and Department of Operative Dentistry, Faculty of Dentistry, Ege University, Izmir, Turkey
Biiyukyilmaz T, Sen BH, Bgaard B. Retention of titanium tetrafluoride (Ti,), used as ffisure sealant on human deciduous molars. Acta Odontol Scand 1997;55:73-78. Oslo. ISSN 00014357. When dental hard tissues are exposed to aqueous solutions of TiF4, an acid-resistant glaze forms on tooth surfaces. The aim of the present study was to examine the long-term retention of the glaze on TiF4-treated deciduous molars. The occlusal surfaces of four deciduous molars in each of Seven children were treated with 4% TiF, for 1 min. The sealed teeth were extracted after 1, 3, 6, or 12 months and examined with scanning electron microscopy. An extensive surface layer was present on all deciduous molars after I month. After 3 months the glaze appeared to be worn out on the cusp tips and in some a rea on the cusp inclines. At 6 months the glaze was observed as small areas distributed over the cusp inclines with total coverage of the pits and fwures. After 1 year the presence of the glaze was limited to pits and fissures. Clinically, all fmures were caries-free by visual inspection at the end of the experimental period. The results indicate that the glaze formed after topical TiF4 application may be an effective way of sealing pits and fwures under d i c a l conditions. 0 Dmkd mmnCl;jlm&s, topical; scmUting ehbvn microsco~?~
Timer B-, Departmmt of(hlllodonh, Facully of Dentis& U;nsily of Oslo, P. 0. Box I I09 Blindem, 031 7 Oslo, N m q
The fusure sealants were developed in the early 1970s to prevent caries in occlusal surfaces of recently erupted teeth. Today, most widely used BIS-GMA-type resin sealant applications are considered an effective measure for pit and fusure caries prevention. The cariostatic properties of resin sealants were associated with the long-term retention of these materials (1, 2). In the literature a wide range (36-100%) of sigdkant caries reductions, depending totally on sealant retention, was reported (1, 3,4). Glass ionomer cements have also been investigated in comparison with conventional resin- based sealants, and the results have been promising (5, 6). For glass ionomer sealants the retention rate appears to be lower, although similar or even better cariostasis was reported by several investigators (6-8). Simple application, the capability of adhering to unetched enamel surfaces, the continuous release of fluoride and the fact that they can be recharged by application of fluoride gel to increase the fluoride release, and their microbial effect (9) have been considered the main advantages of glass ionomer cements. Nevertheless, for both resin-based and glass ionomer fusure sealants, properties such as physicochemid bonding to tooth structure, resistance to oral acids, surface integrity, chemical compatibility with oral tissues, and cariostatic action (10) still remain to be improved.
An alternative approach for fmure sealing with GIC or resins may be the topical application of TiF4. Previous in vim (1 1, 12) and in vivo studies (13, 14) have already shown the cariostatic effect of TiF4. The aqueous solution of TiF4, when applied topically on dental hard tissues, results in formation of a surface
coating. This surface layer was first detected with the naked eye and identified as 'glaze-like' (1 5). Subsequent scanning electron microscopy (SEW examinations clearly demonstrated a massive coating containing numerous spherical particles (16-19) that were not removed by 24-h synthetic saliva wash (1 8) or after acid etching (1 2). Recently, a similar in vitro study has shown that the glaze formed after TiF4 application was resistant to severe acid and alkali changes and to mechanical forces exerted by scaling (19). The present in vivo study therefore was undertaken to provide more information about the long-term retention of the glaze formed after a topical application of 4% TiF4 solution for 1 min on deciduous enamel.
Materials and methods Seven patients (mean age, 8.9 years) participated in the present study. The children were referred to the orthodontic department for the correction of their malocclusions. The selection criteria included the presence of at least four caries-free deciduous molars, expected to exfoliate or to be extracted in 1 year, while waiting for the start of orthodontic treatment. The teeth were cleaned with pumice and a brush attached to a handpiece, rinsed thoroughly with water spray, and air- dried. Cotton rolls were used to isolate the teeth, and TiF4 was applied for 1 min by means of a cotton pellet soaked in 4% aqueous solution of TiF4. After a water rinse the patients were dismissed. No restrictions in their diet were required. The TiF4-treated deciduous molars
Dow
nloa
ded
by [
The
Sta
te U
nive
rsity
of
New
Yor
k] a
t 07:
58 1
1 Se
ptem
ber
2015
ACTA ODONTOL SCAN) 55 (1997)
Dow
nloa
ded
by [
The
Sta
te U
nive
rsity
of
New
Yor
k] a
t 07:
58 1
1 Se
ptem
ber
2015
ACTA ODONTOL SCAi'iD 55 (1997) Retention of 7iF4 on deciduour teeth 75
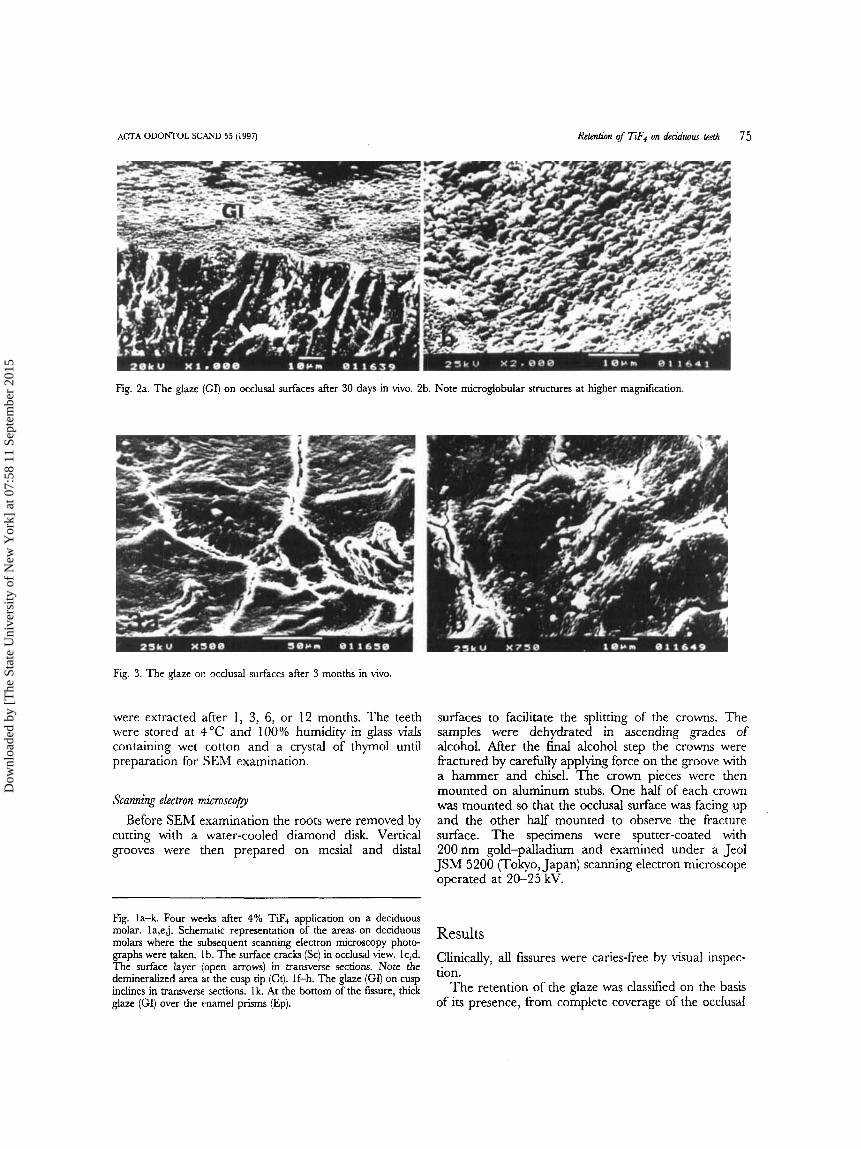
Fig. 2a. The glaze (GI) on occlusal surfaces after 30 days in vivo. 2b. Note microglobular structures at higher magnification.
Fig. 3. The glaze on occlusal surfaces after 3 months in vivo.
were extracted after 1, 3, 6, or 12 months. The teeth were stored at 4 "C and 100% humidity in glass vials containing wet cotton and a crystal of thymol until preparation for SEbl examination.
Scanning electron microscopy Before SEM examination the roots were removed by
cutting with a water-cooled diamond disk. Vertical grooves were then prepared on mesial and distal
surfaces to facilitate the splitting of the crowns. The samples were dehydrated in ascending grades of alcohol. After the final alcohol step the crowns were fractured by carefully applying force on the groove with a hammer and chisel. The crown pieces were then mounted on aluminum stubs. One half of each crown was mounted so that the occlusal surface was facing up and the other half mounted to observe the fracture surface. The specimens were sputter-coated with 200nm gold-palladium and examined under a Jeol JSM 5200 (Tokyo, Japan) scanning electron microscope operated at 20-25 kV.
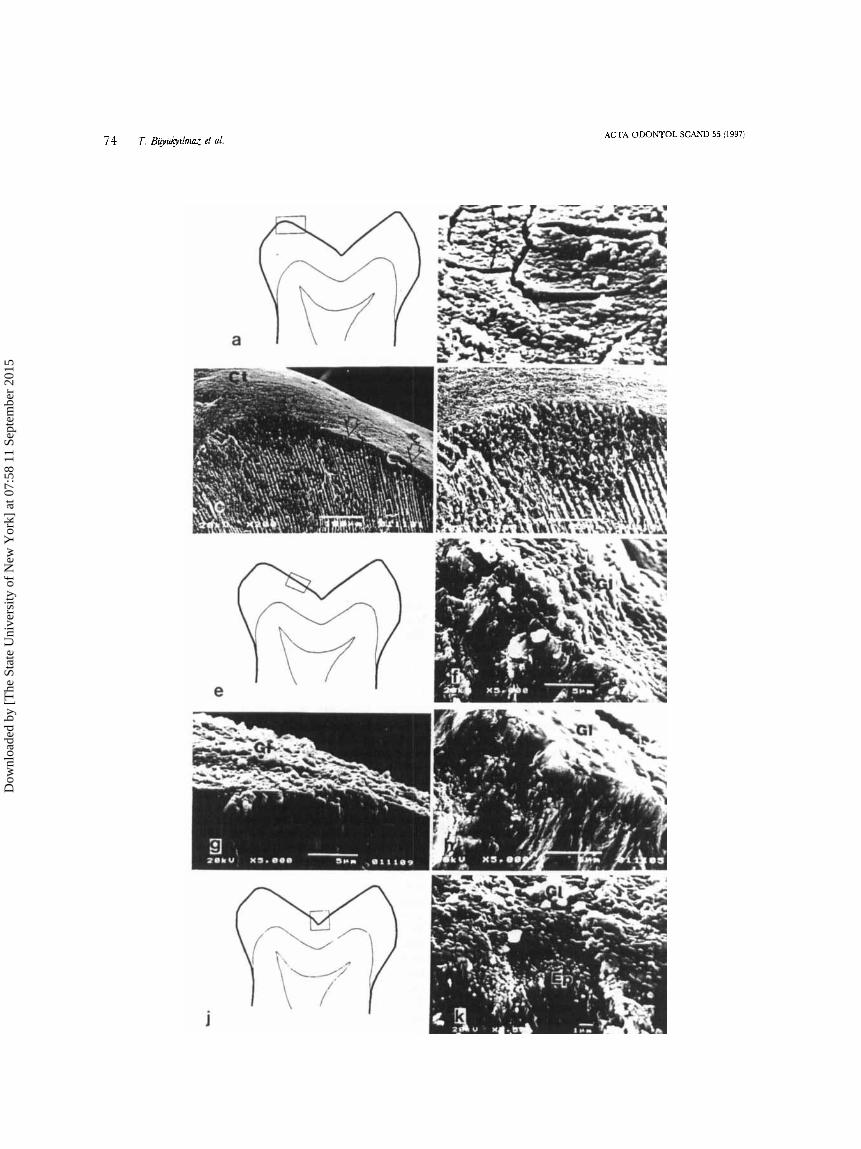
Fig. la-k. Four weeks after 4% TiF, application on a deciduous molar. la,ej. Schematic representation of the areas on deciduous molars where the subsequent scanning electron microscopy photo- graphs were taken. lb. The surface cracks (SC) in C J C C ~ U ~ ~ ~ view. lc,d. The surface layer (open arrows) in transverse sections. Note the demineralized area at the cusp tip (Ct). If-h. The glaze (GI) on cusp inclines in transverse sections. lk. At the bottom of the fissure, thick glaze (GI) over the enamel prisms (Ep).
Results Clinically, all fissures were caries-free by visual inspec-
On the basis The retention Of the glaze was of its presence, from complete coverage of the occlusal
Dow
nloa
ded
by [
The
Sta
te U
nive
rsity
of
New
Yor
k] a
t 07:
58 1
1 Se
ptem
ber
2015
76 I.Btryul.1LRaTetai. ACTA ODONTOL SCAND 55 (1997)
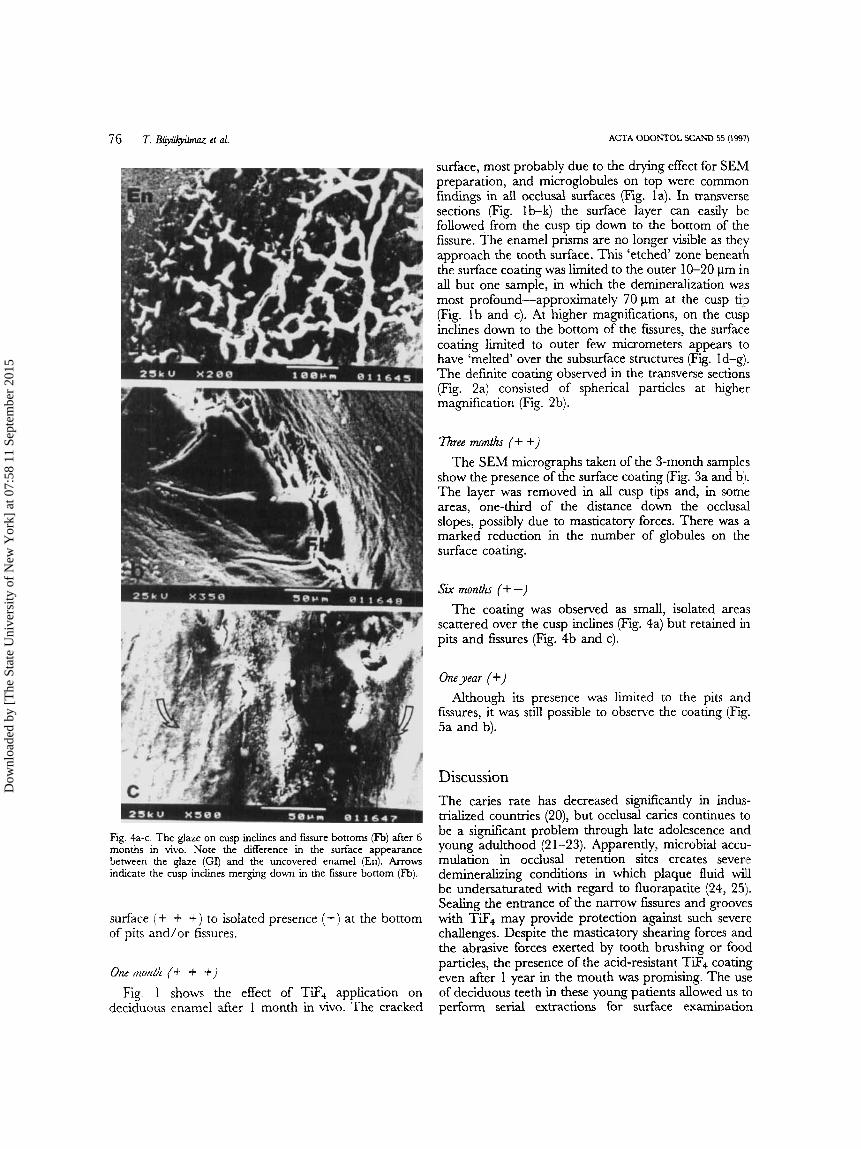
Fig. 4a-c. The glaze on cusp inclines and fwure bottoms (Fb) after 6 month in vivo. Note the difference in the surface appearance between the glaze (Gq and the uncovered enamel (En). Arrows indicate the cusp inclines merging down in the fmure bottom (Fb).
surface (+ + +) to isolated presence (+) at the bottom of pits and/or fissures.
ozh! f?mlll (4- =+ 9)
Fig. 1 shows the effect of TiF, application on deciduous enamel after 1 month in vivo. The cracked
surface, most probably due to the drymg effect for SEA4 preparation, and microglobules on top were common h d m p in all occlusal surfaces (Fig. la). In transverse sections (Fig. Ib-k) the surface layer can easily be followed from the cusp tip down to the bottom of the fissure. The enamel prisms are no longer visible as they approach the tooth surface. This ‘etched‘ zone beneath the surface coating was limited to the outer 10-20 pm in all but one sample, in which the demineralkation was most profound-approximately 70 pm at the cusp tip (Fig. l b and c). At higher ma@ications, on the cuslp inclines down to the bottom of the fissures, the surface coating limited to outer few micrometers appears to have ‘melted’ over the subsurface structures (Fig. Id-g). The definite coating observed in the transverse sections (Fig. 2a) consisted of spherical particles at higher magdkation (Fig. 2b).
T h e e months (+ +) The SEM micrographs taken of the 3-month samples
show the presence of the surface coating (Fig. 3a and b:l. The layer was removed in all cusp tips and, in som’e areas, one-third of the distance down the occlusal slopes, possibly due to masticatory forces. There was .a marked reduction in the number of globules on the surface coating.
Sir months (+ -) The coating was observed as small, isolated areas
scattered over the cusp inclines (Fig. 4a) but retained in pits and fissures (Fig. 4b and c).
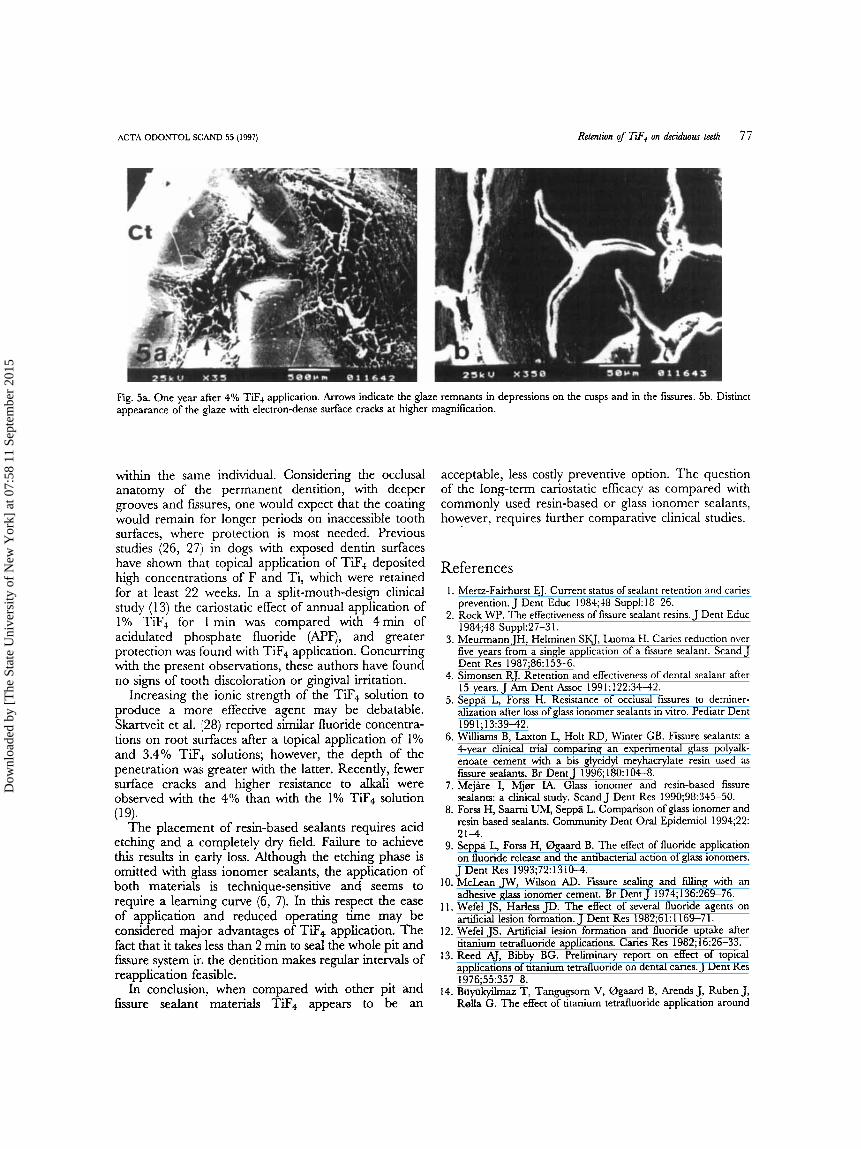
Oneyear (+) Although its presence was limited to the pits and
fEsures, it was still possible to observe the coating (Fig. 5a and b).
Discussion The caries rate has decreased si@icantly in indus- trialized countries (20), but occlusal canes continues to be a si@icant problem through late adolescence and young adulthood (2 1-23). Apparently, microbial accu- mulation in occlusal retention sites creates severie demineralizing conditions in which plaque fluid wikl be undersaturated with regard to fluorapatite (24, 25). Sealing the entrance of the narrow fissures and grooves with TiF, may provide protection against such severe challenges. Despite the masticatory shearing forces and the abrasive forces exerted by tooth brushing or food particles, the presence of the acid-resistant TiF, coating even after 1 year in the mouth was promising. The use of deciduous teeth in these young patients allowed us tlo perform serial extractions for surface examination
Dow
nloa
ded
by [
The
Sta
te U
nive
rsity
of
New
Yor
k] a
t 07:
58 1
1 Se
ptem
ber
2015
ACTA ODONTOL SCAND 55 (1997) Retention of Tfi4 on deduaus teeth 77
Fig. 5a. One year after 4% TiF+ application. Arrows indicate the glaze remnants in depressions on the cusps and in the fissures. 5b. Distinct appearance of the glaze with electron-dense surface cracks at higher magnification.
within the same individual. Considering the occlusal anatomy of the permanent dentition, with deeper grooves and fissures, one would expect that the coating would remain for longer periods on inaccessible tooth surfaces, where protection is most needed. Previous studies (26, 27) in dogs with exposed dentin surfaces have shown that topical application of TiF4 deposited high concentrations of F and Ti, which were retained for at least 22 weeks. In a split-mouth-design clinical study (1 3) the cariostatic effect of annual application of 1% TiF4 for I min was compared with 4min of acidulated phosphate fluoride (APF), and greater protection was found with TiF4 application. Concurring with the present observations, these authors have found no signs of tooth discoloration or gingival irritation.
Increasing the ionic strength of the TiF4 solution to produce a more effective agent may be debatable. Skartveit et al. 1p8) reported similar fluoride concentra- tions on root surfaces after a topical application of 1% and 3.4% TiF4 solutions; however, the depth of the penetration was greater with the latter. Recently, fewer surface cracks and higher resistance to alkali were observed with the 4% than with the 1% TiF4 solution
The placement of resin-based sealants requires acid etching and a completely dry field. Failure to achieve this results in early loss. Although the etching phase is omitted with glass ionomer sealants, the application of both materials is technique-sensitive and seems to require a learning curve (6, 7). In this respect the ease of application and reduced operating time may be considered major advantages of TiF4 application. The fact that it takes less than 2 min to seal the whole pit and fssure system in the dentition makes regular intervals of reapplication feasible.
In conclusion7 when compared with other pit and fmure sealant materials TiF4 appears to be an
(19).
acceptable, less costly preventive option. The question of the long-term cariostatic efficacy as compared with commonly used resin-based or glass ionomer sealants, however, requires further comparative clinical studies.
References 1. IMertz-Fairhurst EJ. Current status of sealant retention and caries
2. Rock WP. The effectiveness of fissure sealant resins. J Dent Educ
3. Meurmann JH, Helminen SKJ, Luoma H. Canes reduction over five years from a single application of a fissure sealant. Scand J Dent Res 1987;86:153-6.
4. Simonsen RJ. Retention and effectiveness of dental sealant after 15 years. J Am Dent Assoc 1991;122:3442.
5. Seppa L, Forss H. Resistance of occlusal fusures to deminer- alization after loss of glass ionorner sealants in vitro. Pediatr Dent 1991; 13:39-42.
6. Williams B, Laxton L, Holt RD, Winter GB. Fissure sealants: a 4-year clinical trial comparing an experimental glass polyalk- enoate cement with a bis glycidyl meyhacrylate resin used as fissure sealants. Br Dent J 1996; 180: 104-8.
7. Mejare I, Mjm IA. Glass ionomer and resin-based fusure sealants: a dmical study. Scand J Dent Res 1990;98:345-50.
8. Forss H, Saarni uh.i, Seppa L Comparison of glass ionomer and resin based sealants. Community Dent Oral Epidemiol 1994;22: 2 1 4 .
9. Seppa L, Forss H, Bgaard B. The effect of fluoride application on fluoride release and the antibacterial action of glas ionomers. J Dent Res 1993;72:13104.
10. McLean JW, Wilson AD. Fissure sealing and f i g with an adhesive glass ionomer cement. Br Dent J 1974;136:269-76.
11. Wefel JS, Harless JD. The effect of several fluoride agents on artificial lesion formation. J Dent Res 1982;6 1 : 1 169-7 1.
12. Wefel JS. Artificial lesion formation and fluoride uptake after titanium tetrafluoride applications. Caries Res 1982; 16:26-33.
13. Reed AJ, Bibby BG. Preliminary report on effect of topical applications of titanium tetrafluoride on dental canes. J Dent Res 1976;55:357-8.
14. Biiyiikyllmaz T, Tangugsorn V, Bgaard B, Arends J, Ruben J, R0lla G. The effect of titanium tetrafluoride application around
prevention. J Dent Educ 1984;48 Suppl: 18-26.
1984;48 Suppl:27-3 1.
Dow
nloa
ded
by [
The
Sta
te U
nive
rsity
of
New
Yor
k] a
t 07:
58 1
1 Se
ptem
ber
2015
7% 7. B ~ + h u r et a&.
orthodontic brackets. Am J Orthod Dentofac Onhop 1994; 105:293-6.
15. Shrestha BM, Mundorff SA, Bibby BG. Enamel dissolution. I. Effects of various agents and titanium teduor ide . J Dent Res l972;5 I : 1561-6.
16. Gwinnett AJ, Buonocore MG, Sheykholeslam Z. Effect of fluoride on etched human and bovine tooth enamel surfaces as demonstrated by scanning electron microscopy. Arch Oral Biol 1972;117:271-8.
17. Wei SHY, Soboroff DM, Wefel JS. Effects of titanium tetrafluoride on human enamel. J Dent Res 1976;55:426-31.
18. Wefel JS, Harless JD. The effect of topical fluoride agents on fluoride uptake and surface morphology. J Dent Res 1981;60:
19. Biiyiikyilmaz T, Bgaard B, R d a G. The resistance of titanium tetrafluoride-treated human enamel to strong hydrochloric acid. Caries Res. In press.
20. Glass RL, editor. The first international conference on the declining prevalence of dental caries. J Dent Res 1982;61(Spec
21. Brunrlle 5.4, Carlos JP. Recent trends in dental caries in US children and the effect of water fluoridation. J Dent Res 1990;
1842-8.
ISS) 1301-83.
~ ~ ( S P C C Iss):723-7,
ACTA ODONTOL SCAND 55 [ 1997)
22. Ruiken IXMHM, Konig KG, Tmin GJ, Plasschaert AJM. Longi- tudinal study of dental caries development in Dutch children aged 8-12 years. Community Dent Oral Epidemiol 1986;14:53- 6.
23. BirkelandJiM, Bragelien J. Continual highly significant decrease in caries prevalence among 14-year-old Norwegians. Acta Odontol Scand 1987;45: 135-40.
24. Exterkate RAM, CateJ?vI ten. pH cycling, number of cycles and F treament on demineralization of sound enamel. Canes Res 1989;23:439-40.
25. h e n MJ. Chemical events during tooth dissolution. J Dent Res 1990;69(Spec Iss):57 5-80.
26. Tveit AB, Selvig KA, Tetdal B, Klinge B, Nilveus R. Long-tern1 retention of TiF, and SnF2 after topical application to dentin. Scand J Dent Res 1988;96:536-40.
27. Skartveit I.+ Tveit AB, Klinge B, Tetdal B, Selvig KA. In vivo uptake and retention of fluoride after a brief application of TiF+ to dentin. Acta Odontol Scand 1989;47:65-8.
28. Skartveit L, Tveit AB, Tetdal B, Selvig KA. Effects of TiF, solutions on root surfaces in vitro after different application periods. Acta Odontol Scand 1989;47:25-30.
Received for publication 7 August 1996 .Icceptrd 9 October 1996
Dow
nloa
ded
by [
The
Sta
te U
nive
rsity
of
New
Yor
k] a
t 07:
58 1
1 Se
ptem
ber
2015
Recommended

















