Embed Size (px)
Citation preview

INTERESTING CASE OF DYSPNOEA
DR K.M.JEYABALAJI
PROF DR. P.VIJAYARAGHAVAN’S UNIT

HISTORY
A 38 YEAR OLD MALE PATIENT CAME WITH COMPLAINTS OF
PALPITATION
DYSPNOEA GRADE 3
BILATERAL LEG SWELLING
COUGH WITH EXPECTORATION
FOR PAST 10 DAYS

H/O PRESENTING ILLNESSPATIENT WAS APPARENTLY NORMAL 10 DAYS BACK
H/O BILATERAL LEG SWELLING -10 DAYS
H//O DIFF. IN BREATHING – 10 DAYS
H/O COUGH WITH SCANTY SPUTUM – 10 DAYS
NO H/O HEMOPTYSIS
NO H/O FEVER
NO H/O CHEST PAIN

PAST HISTORY:
KNOWN CASE OF OLD PT TREATED 5 YEARS BACK
NOT A KNOWN DM,SHT,ASTHMATIC, CAD
PERSONAL HISTORY:
SMOKER
NON ALCOHOLIC
FAMILY HISTORY:
HIS ELDER BROTHER DIED IN 30 YEARS DUE TO SUDDEN CARDIAC ARREST

EXAMINATION
Patient is
Concious
Oriented
Afebrile
Anaemic
No icterus, clubbing, cyanosis
Bilateral pitting pedal edema present

VITALS
Pulse- 86/min
BP- 110/80 mmHg
JVP- elevated – 12cm

EXAMINATIONCVS- s1,s2 +, mufflled
Apical impulse 6th intercostal space 1 inch lateral to mid clavicular line..
Hyperdynamic
Pan systolic murmur heard over tricuspid area
RS – trachea shifted to left, NVBS
P/A – soft, congestive hepatomegaly extending 2cm below Rt subcostal margin.

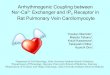
X ray

ECG

ECGRATE 120
AXIS – INDETERMINATE
RAE
T INVERSION IN V1-V6
POOR R WAVE PROGRESSION FROM V1-V6
QRS DURATION – 0.10 SEC.
VPC +

ECHO

CARDIAC MRI

4 CHAMBER VIEW




DIAGNOSIS
ARVD WITH RIGHT HEART FAILURE
SEVERE TRICUSPID REGURGITATION
OLD PULMONARY TUBERCULOSIS RT UL FIBROSIS

DISCUSSION
ARRHYTHMOGENIC RIGHT VENTRICULAR DYSPLASIA/CARDIOMYOPATHY (ARVD/C), FIRST DESCRIBED IN 1977 BY FONTAINE AND COWORKERS, IS A GENETIC FORM OF CARDIOMYOPATHY CHARACTERIZED PROTOTYPICALLY BY FIBROFATTY INFILTRATION OF THE RIGHT VENTRICLE


PREVALENCEARVD/C accounts for 20 percent of cases of sudden cardiac death.
The prevalence of ARVC in the general adult population is estimated to be approximately 1 in 2000 to 1 in 5000
Presentation is most common between the ages of 10 and 50 years, with a mean age at diagnosis of approximately 30 years
France - forensic autopsies on 1930 cases of unexplained SCD (mean age 34 years, males and females equally represented), 200 (10.4 percent) were associated with ARVC.
In a report from northern Italy evaluating the causes of SCD among 269 subjects under 35 years of age, ARVC accounted for 22 percent of deaths among the 49 athletes and 8 percent among the 220 non-athletes

DOMINANCE
Biventricular – Parallel involvement of both ventricles (112 patients (56 percent)
Classic – This pattern is defined by isolated RV disease or LV involvement in association with significant RV impairment (78 patients [39 percent]
Left dominant – Characterized by early and prominent LV manifestations and relatively mild right-sided disease (10 patients [5 percent])

GENETICS
SEVERAL GENES AND GENE LOCI ARE ASSOCIATED WITH ARVD/C, AND BOTH AUTOSOMAL DOMINANT AND RECESSIVE MODES OF INHERITANCE ARE DESCRIBED. IMPLICATED GENES INCLUDE
DESMOPLAKIN
JUNCTIONAL PLAKOGLOBIN (JUP)
THE CARDIAC RYANODINE RECEPTOR PLAKOPHILIN-2 (PKP2)
TRANSFORMING GROWTH FACTOR-B3.

NAXOS SYNDROME
AR ARVD – JUNCTIONAL PHAKOGLOBULIN MUTATION
CARDIOCUTANEOUS SYNDROME
ARVD
WOOLY HAIR
HYPERKERATOSIS OF PALMS AND SOLES

SYMPTOMS
Palpitations – 67 percent
Syncope – 32 percent
Atypical chest pain – 27 percent
Dyspnea – 11 percent
RV failure – 6 percent

The most common ventricular arrhythmia is sustained or nonsustained monomorphic VT that originates in the RV and therefore has a left bundle branch block (LBBB) pattern

The diagnosis of ARVD is confirmed if the patient has these characteristics:
Abnormal function of the right ventricle (RV)
Fatty or fibrous-fatty infiltrates of the right ventricle heart muscle (myocardium)
Abnormal ECG
Arrhythmias (supraventricular tachycardia, ventricular tachycardia or ventricular fibrillation, especially with exercise)
Family history of ARVD

ECG TASK FORCE CRITERIA
QRS prolongation, particularly in lead V1 versus V6 – This prolongation is consistent with delayed right ventricular activation.
Incomplete or complete right bundle branch block
Prolonged S wave upstroke (interval from the nadir of the S wave to the isoelectric baseline ≥55 msec) – (90-95%)
Epsilon wave – v1 (30%)
Inversion of T waves in the right precordial leads (V1, V2, and V3)
Ventricular ectopics in excess of 1000 per day.

ECG

ECHO
Right ventricular dilation.
Bulging of right ventricle during diastole.
Dyskinesia of inferobasal free wall during systole.
Dyskinesia of the apex.
Exaggerated trabecular pattern within right ventricle.
Structural abnormalities of the moderator band



MANAGEMENT ANTIARRYTHMIC DRUGS
BETA BLOCKERS, AMIODARONE, FLECAINIDE, PROPAFENONE.
RADIOFREQUENCY CATHETER ABLATION
ICD
ANTI FAILURE MANAGEMENT
ACE
BETA BLOCKER
DIURETICS
DIGOXIN

THANK YOU