Embed Size (px)
Citation preview
Invisalign Clinical Best Practices
Protocol
Ask the Expert Call
Dr. René SterentalMarch 30th, 2007
What is the Clinical Best Practices Protocol?
The objective of the BP Protocol is to offer customers the best of what Align knows of how to treat cases with Invisalign.
The protocol is the result of combining the consensus opinions of leading edge user-doctors, research studies, and over 500K cases in treatment.
Implementation of the elements of this protocol through software automation renders them available to all user-doctors in a manner that is repeatable and scalable.
Elements of Invisalign Clinical Best Practices
Protocol
New Staging Protocol
New Attachment Protocol
New Staging Protocol
Sequential Staging (Old Protocol)
Simultaneous Staging (New Protocol)
Sequential Staging (Old protocol)
Individual Teeth: Complex movements required by one tooth (i.e.
rotation + extrusion) are performed separately, with the less predictable movement staged at the end of the treatment.
Staging of multiple teeth per arch : Some teeth start moving earlier in the setup and other
teeth start moving later. Intended to enhance intra-arch anchorage and/or to
avoid collisions between the teeth as they move.
Sequential Staging considerations (Old protocol)
Difficult movements are often left to the end of treatment and may be accelerated beyond the ideal clinical rate of movement required – applies to root movements.
Difficult for the clinician to estimate and request optimal velocity – can lead to request an excessive number of aligners by indiscriminate requests to reduce the velocity by increasing the overall number of stages.
Simultaneous Staging (New protocol)
Different movements on individual teeth:
Complex movements required by one tooth (i.e. rotation + root uprighting) are performed at the same time.
This usually ensures that the less predictable root movement is performed at a reduced velocity since it is taking place along the greater number of stages required by the easier crown movement.
Simultaneous Staging (New protocol)
Staging of multiple teeth per arch:
All the teeth within each arch are moved together from the initial stage through the final stage.
The tooth that moves the most dictates the overall number of stages based on the maximum allowable tooth velocity.
Moving the other teeth simultaneously from the first to last stage reduces the velocity for all the other movements and increases their predictability without increasing the overall number of aligners.
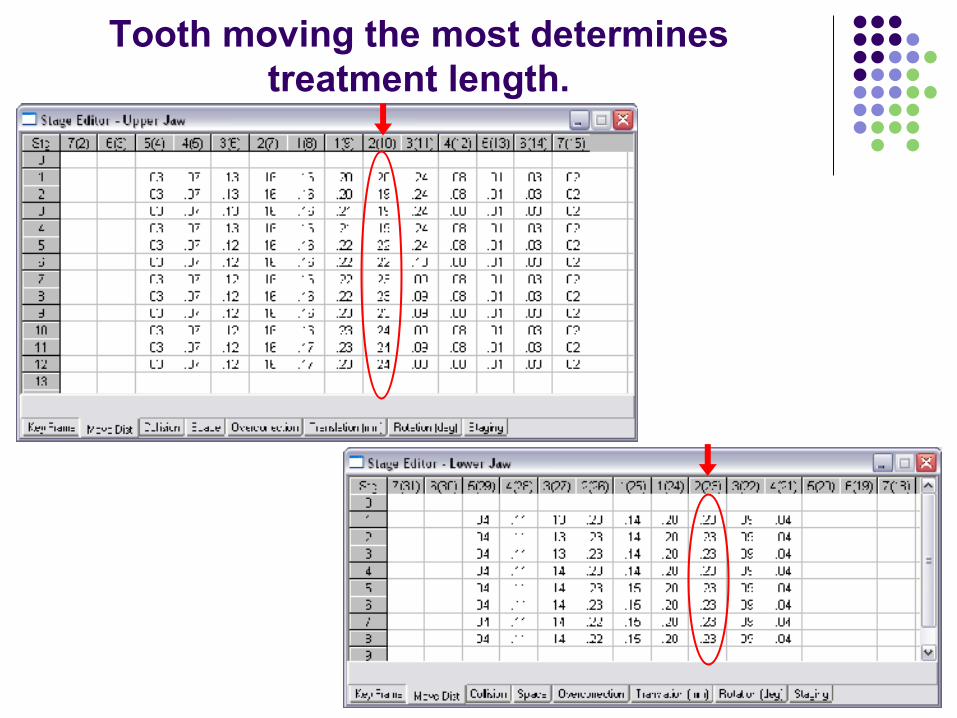
Tooth moving the most determines treatment length.
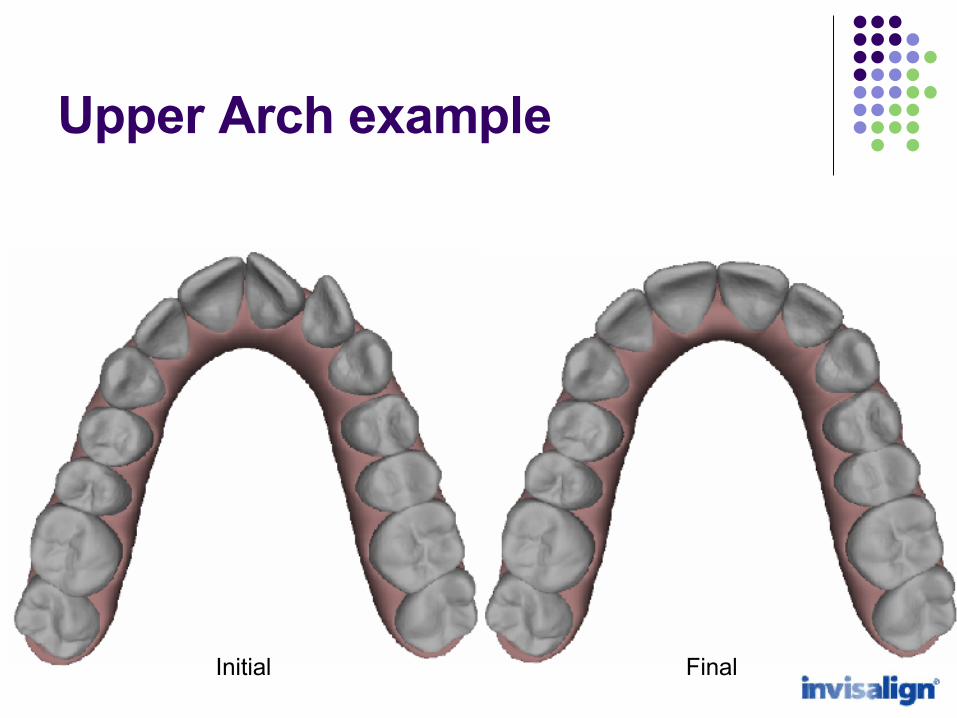
Upper Arch example
Initial Final
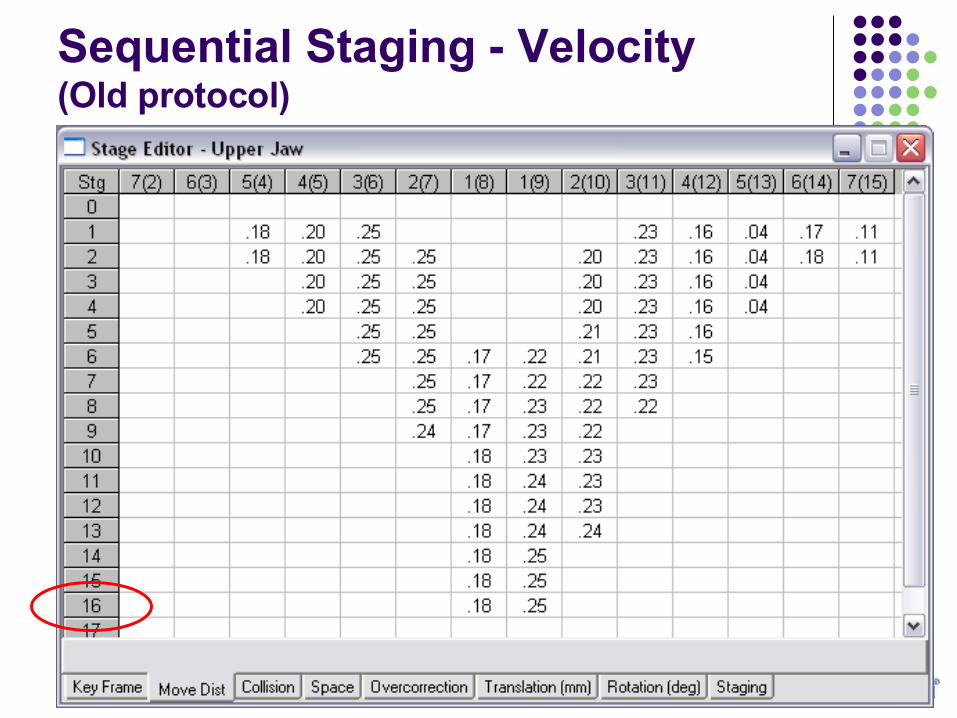
Sequential Staging - Velocity (Old protocol)
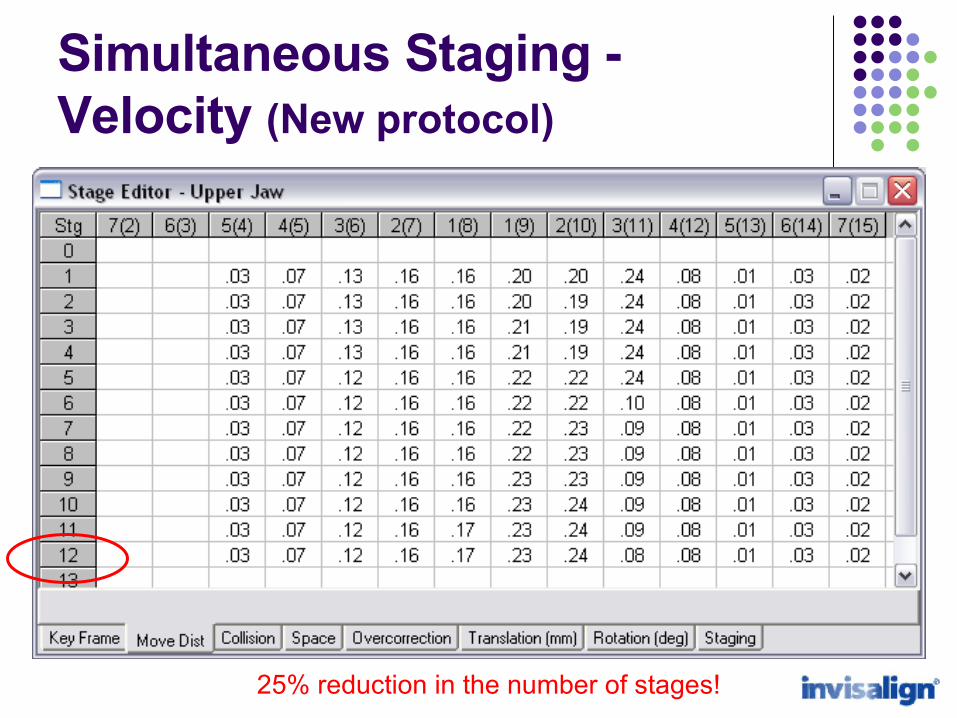
Simultaneous Staging - Velocity (New protocol)
25% reduction in the number of stages!

Lower arch example
Initial Final
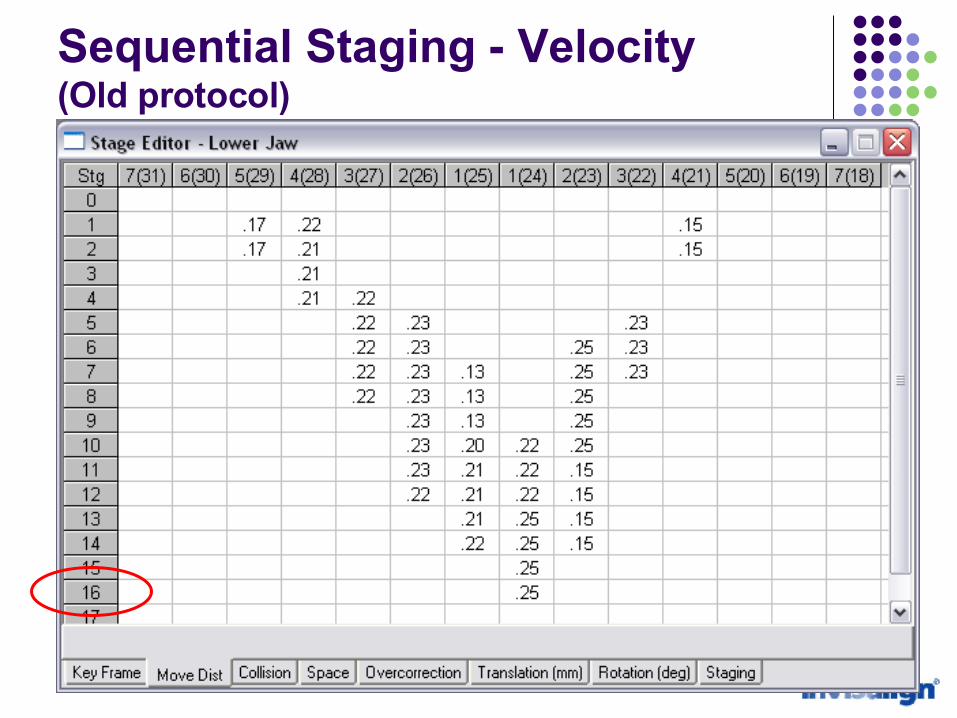
Sequential Staging - Velocity (Old protocol)
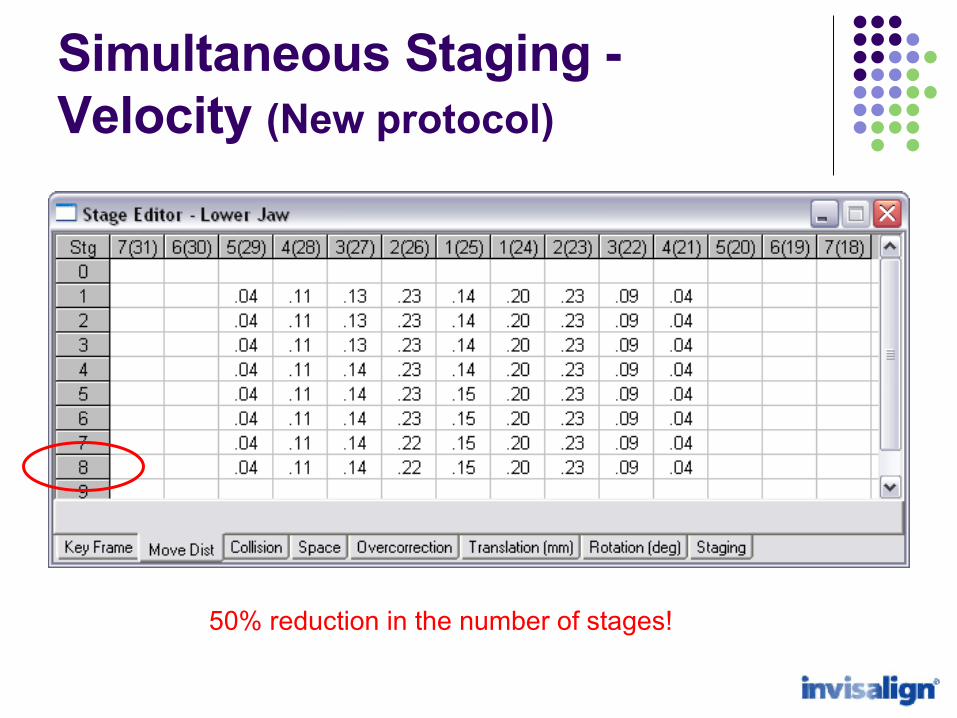
Simultaneous Staging - Velocity (New protocol)
50% reduction in the number of stages!
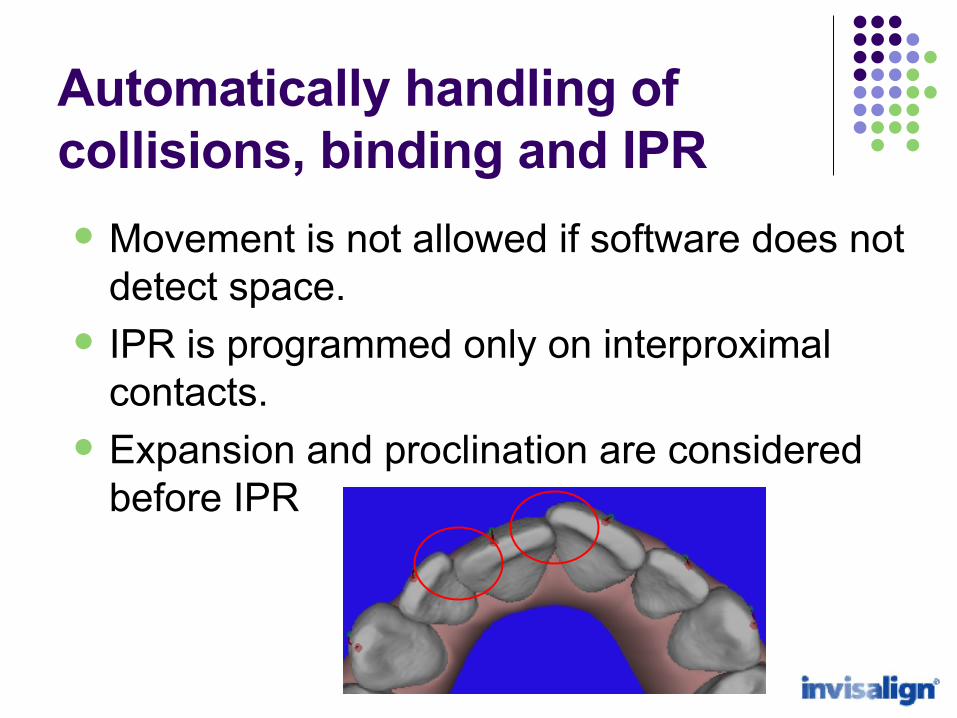
Automatically handling of collisions, binding and IPR
Movement is not allowed if software does not detect space.
IPR is programmed only on interproximal contacts.
Expansion and proclination are considered before IPR
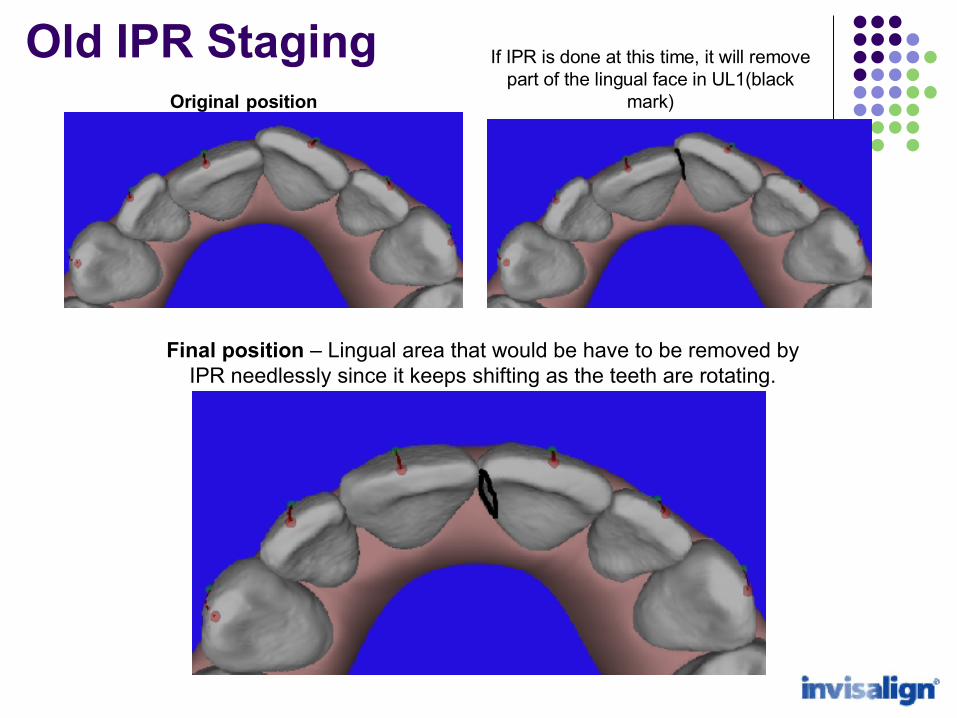
Original position
If IPR is done at this time, it will remove part of the lingual face in UL1(black
mark)
Final position – Lingual area that would be have to be removed by IPR needlessly since it keeps shifting as the teeth are rotating.
Old IPR Staging
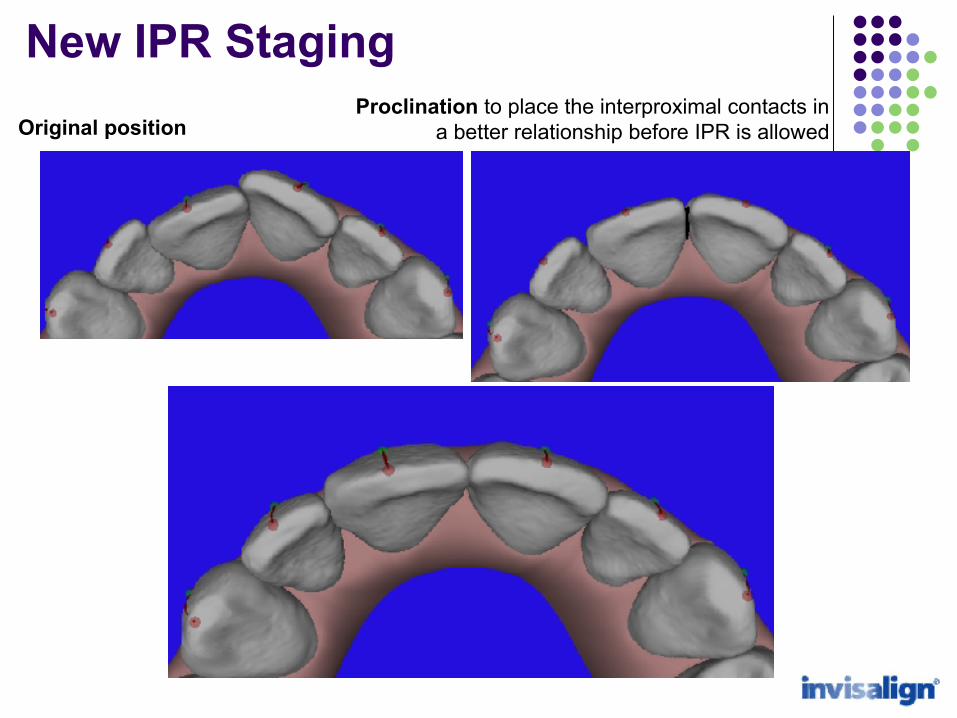
Original positionProclination to place the interproximal contacts in
a better relationship before IPR is allowed
Same final position after doing the IPR and retracting the teeth
New IPR Staging

New Attachment Protocol
Attachments can be…
Passive – Tooth doesn’t move: Intrusion Anchorage Aligner Retentiveness
Active – Tooth moves: Rotations of round teeth Root Control Extrusion
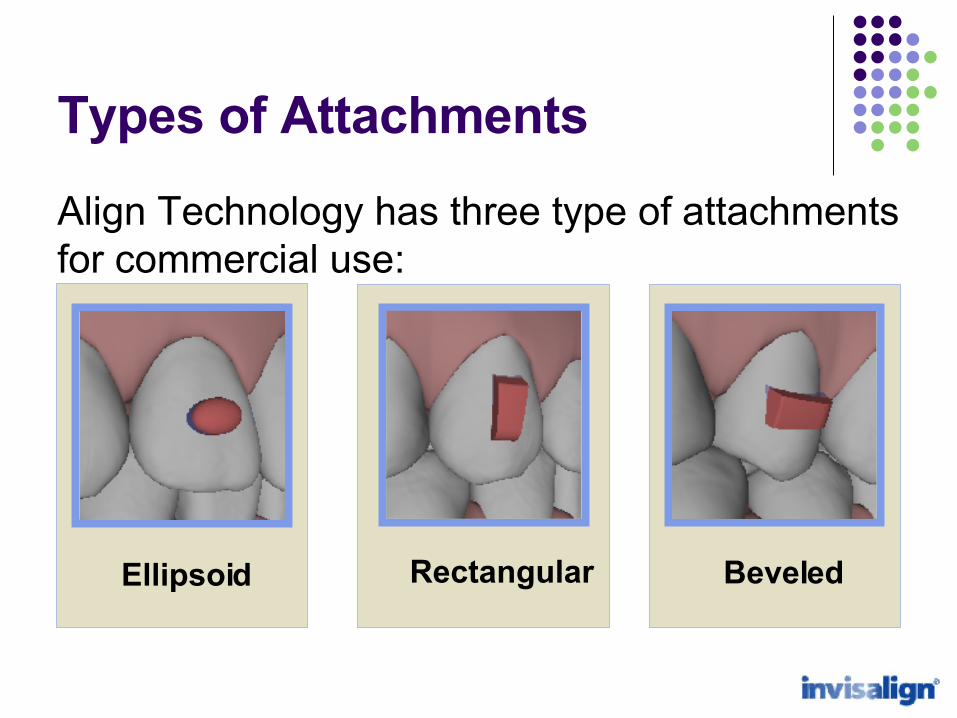
Types of Attachments
Align Technology has three type of attachments for commercial use:
BeveledEllipsoid Rectangular
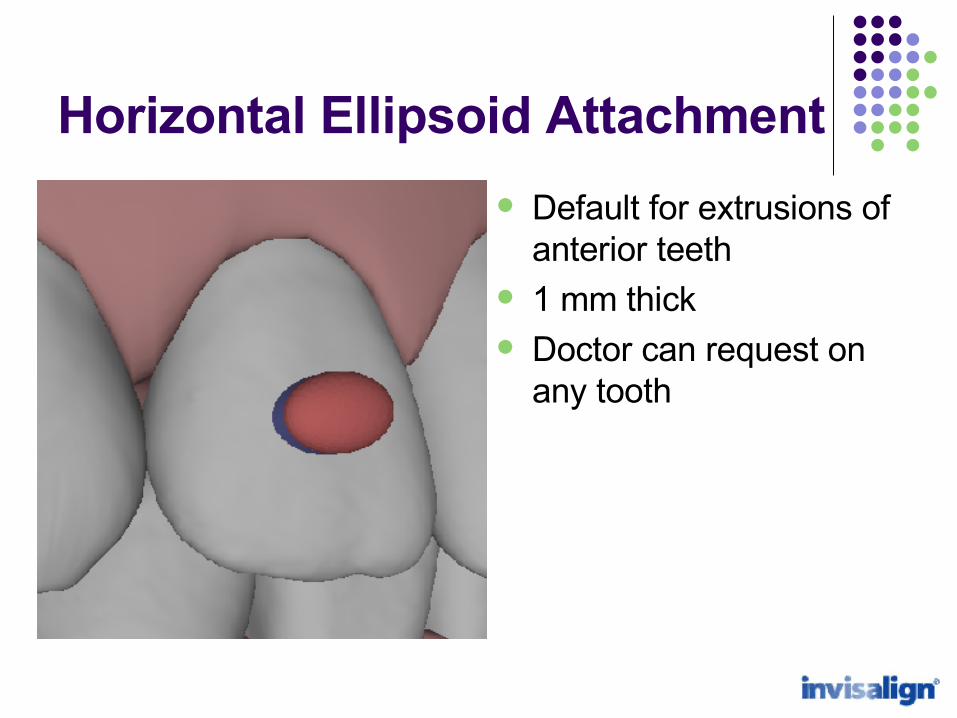
Horizontal Ellipsoid Attachment
Default for extrusions of anterior teeth
1 mm thick Doctor can request on
any tooth
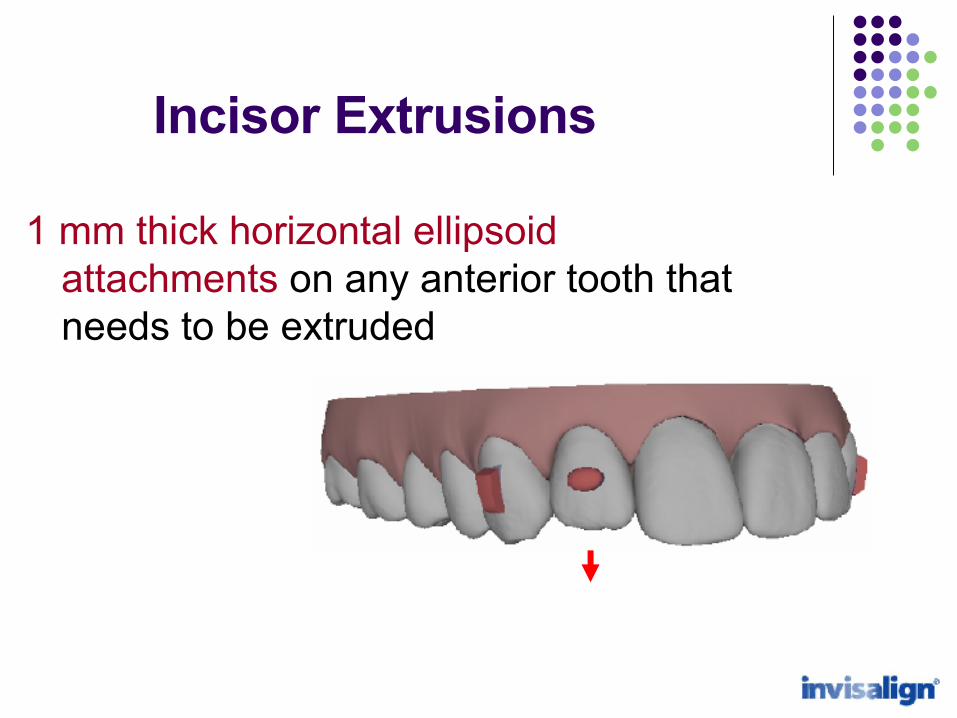
Incisor Extrusions
1 mm thick horizontal ellipsoid attachments on any anterior tooth that needs to be extruded
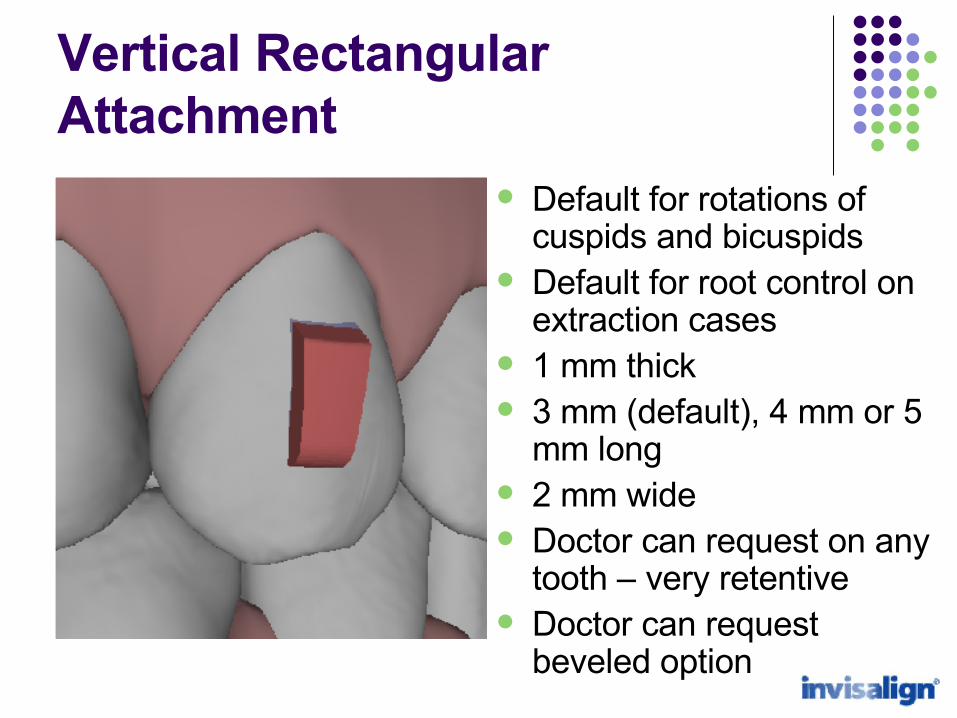
Vertical Rectangular Attachment
Default for rotations of cuspids and bicuspids
Default for root control on extraction cases
1 mm thick 3 mm (default), 4 mm or 5
mm long 2 mm wide Doctor can request on any
tooth – very retentive Doctor can request
beveled option
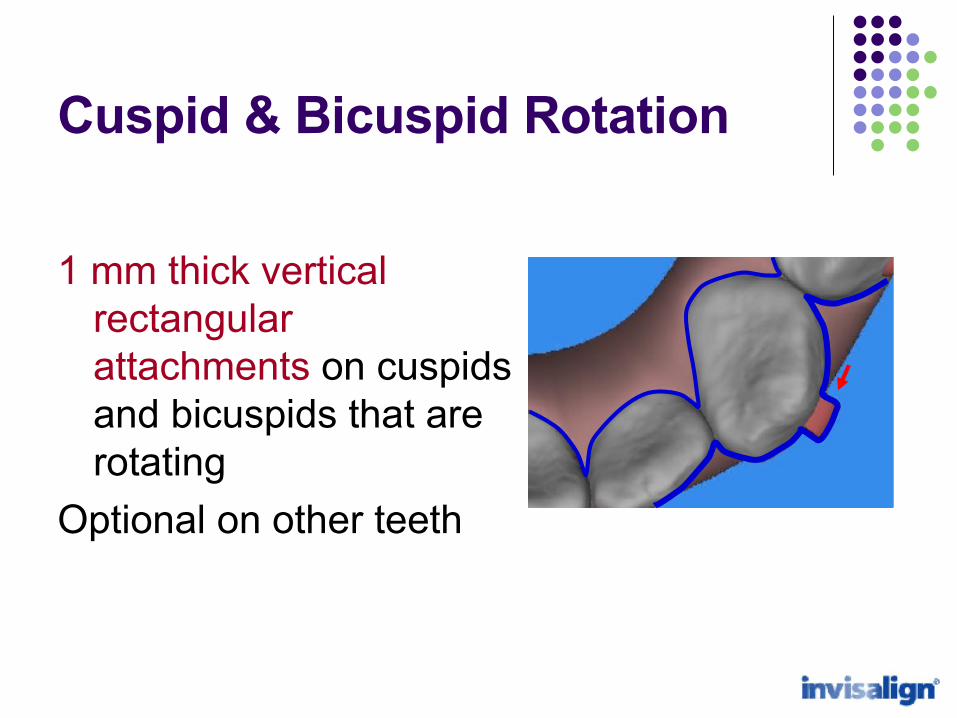
Cuspid & Bicuspid Rotation
1 mm thick vertical rectangular attachments on cuspids and bicuspids that are rotating
Optional on other teeth
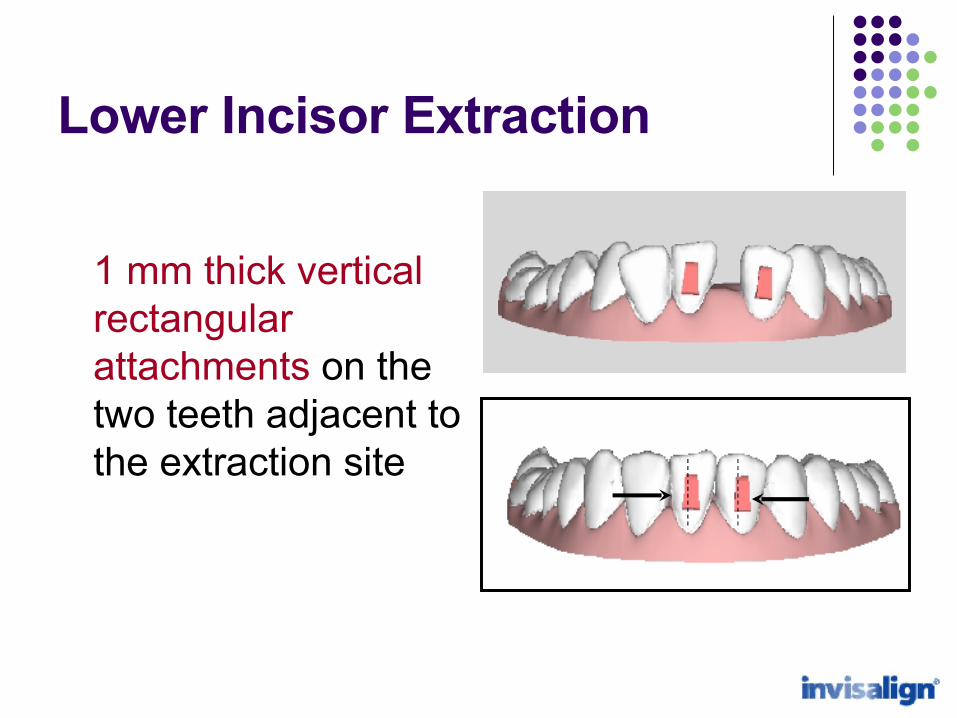
1 mm thick vertical rectangular attachments on the two teeth adjacent to the extraction site
Lower Incisor Extraction
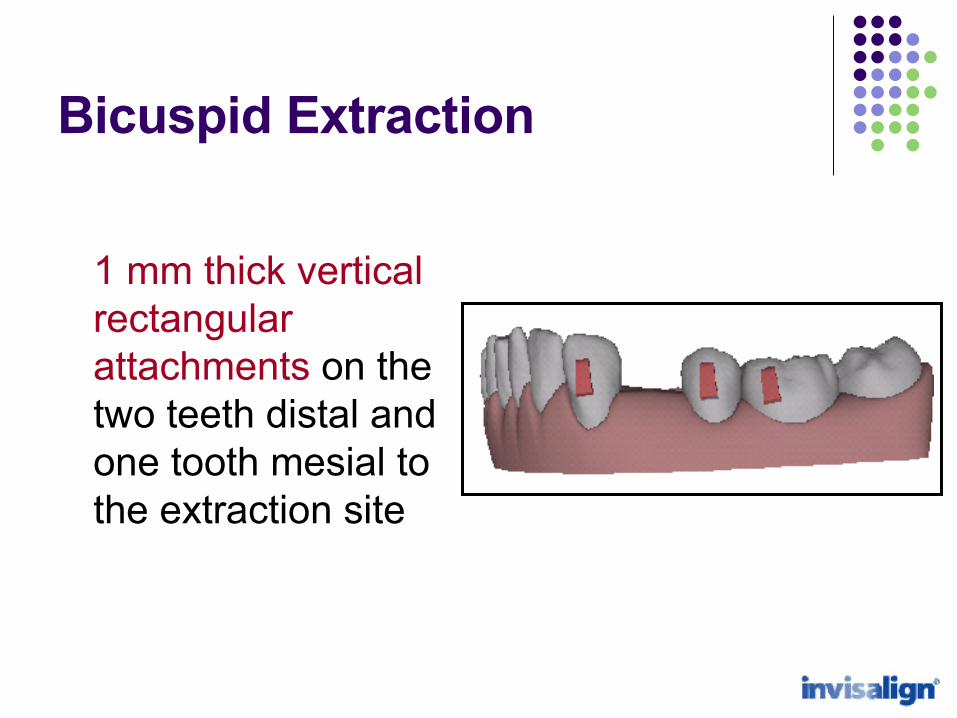
1 mm thick vertical rectangular attachments on the two teeth distal and one tooth mesial to the extraction site
Bicuspid Extraction
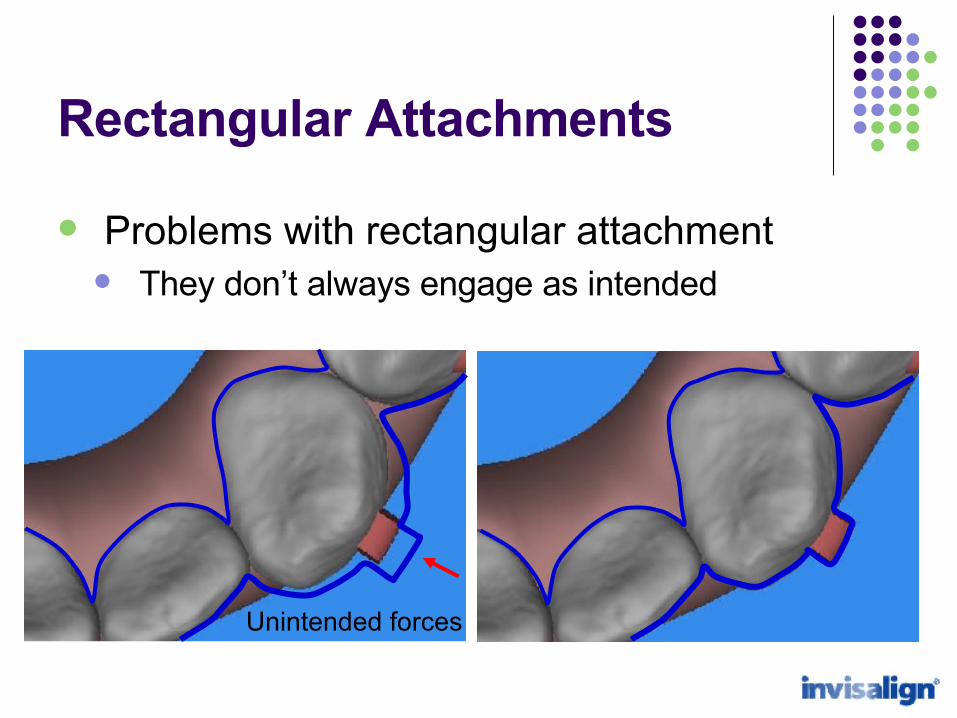
Rectangular Attachments
Problems with rectangular attachment They don’t always engage as intended
Unintended forces
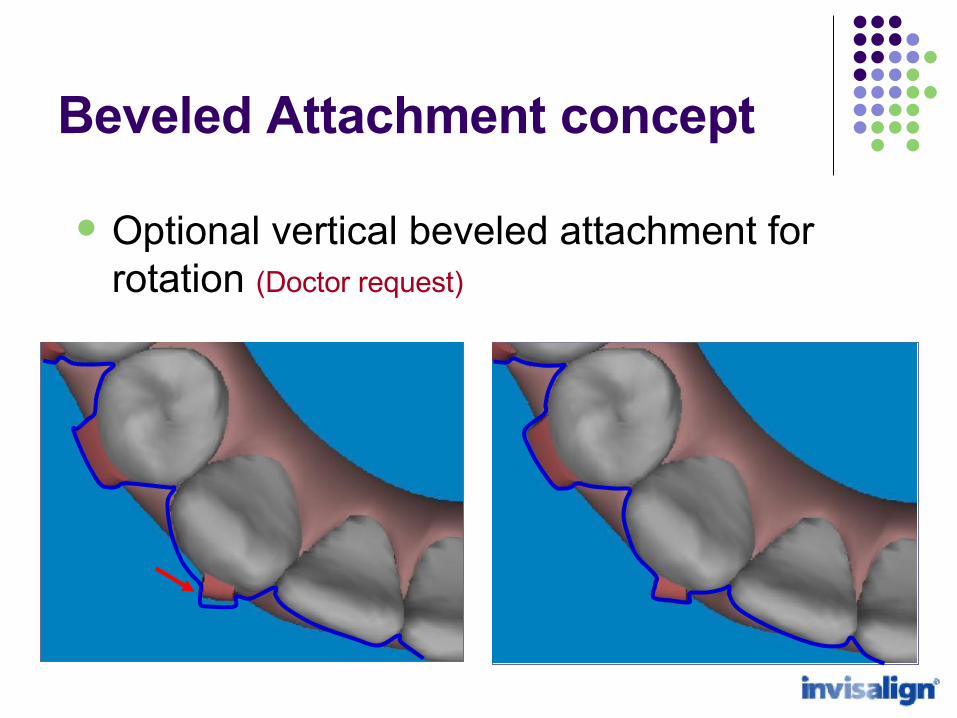
Optional vertical beveled attachment for rotation (Doctor request)
Beveled Attachment concept
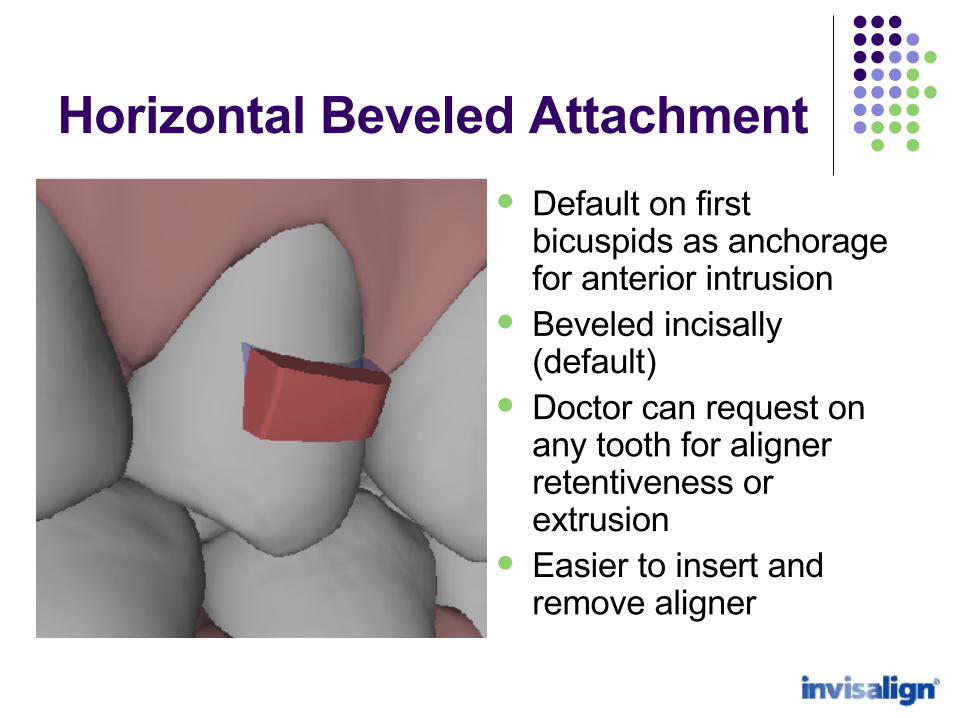
Horizontal Beveled Attachment
Default on first bicuspids as anchorage for anterior intrusion
Beveled incisally (default)
Doctor can request on any tooth for aligner retentiveness or extrusion
Easier to insert and remove aligner

Anterior Intrusion Anchorage provided by horizontal beveled
attachment on first bicuspids
Horizontal beveled attachments bilaterally on the first bicuspids to provide anchorage for anterior intrusion
Anterior Intrusion Anchorage
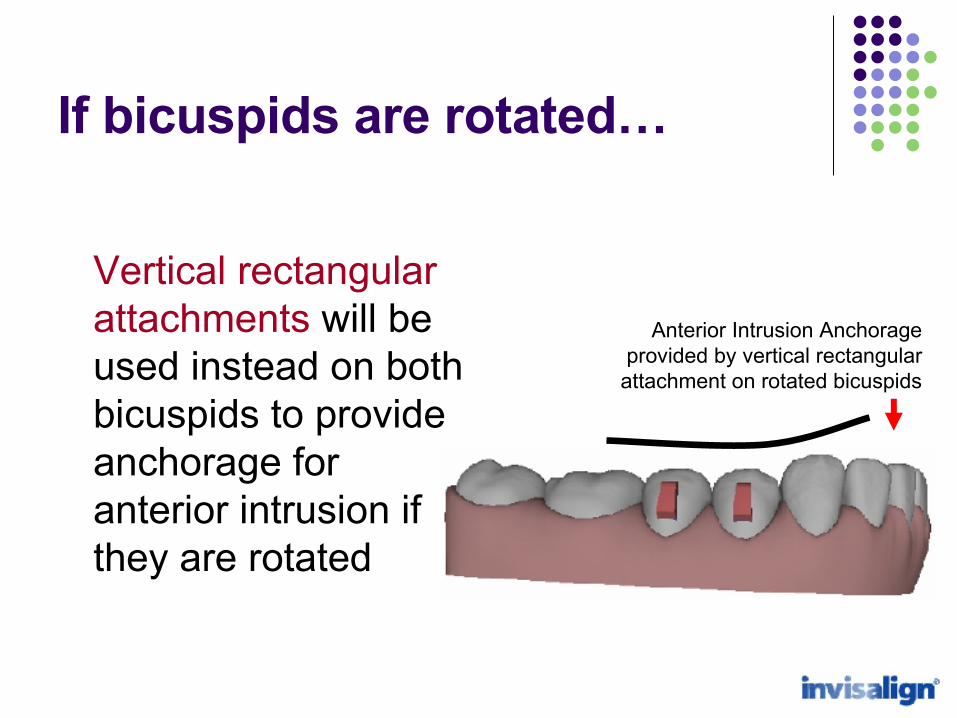
Vertical rectangular attachments will be used instead on both bicuspids to provide anchorage for anterior intrusion if they are rotated
Anterior Intrusion Anchorage provided by vertical rectangular
attachment on rotated bicuspids
If bicuspids are rotated…
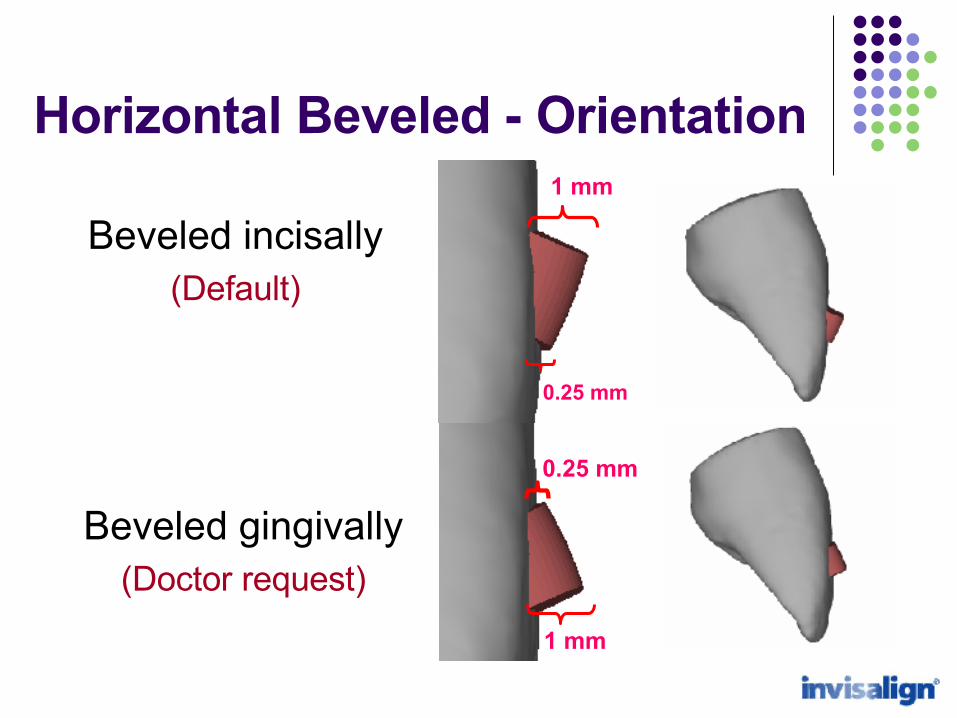
Beveled incisally(Default)
Beveled gingivally(Doctor request)
1 mm
0.25 mm
0.25 mm
1 mm
Horizontal Beveled - Orientation
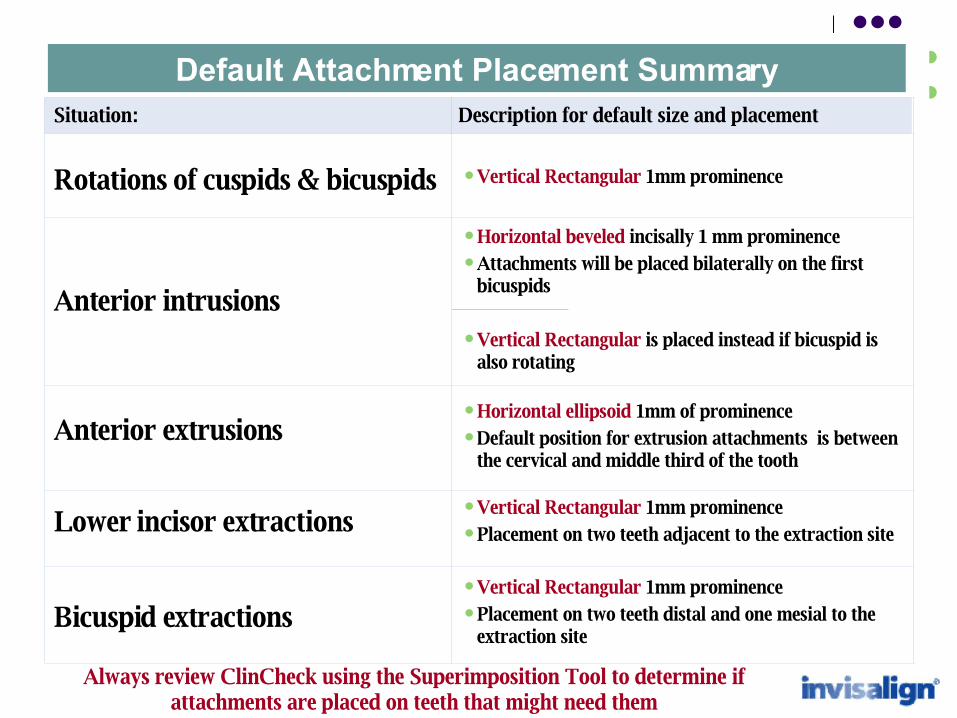
Vertical Rectangular 1mm prominence Placement on two teeth distal and one mesial to the
extraction site
Vertical Rectangular 1mm prominence Placement on two teeth adjacent to the extraction site
Horizontal ellipsoid 1mm of prominence Default position for extrusion attachments is between
the cervical and middle third of the tooth
Horizontal beveled incisally 1 mm prominence Attachments will be placed bilaterally on the first
bicuspids
Vertical Rectangular is placed instead if bicuspid is also rotating
Vertical Rectangular 1mm prominence
Description for default size and placement
Bicuspid extractions
Rotations of cuspids & bicuspids
Anterior intrusions
Lower incisor extractions
Anterior extrusions
Situation:
Default Attachment Placement Summary
Always review ClinCheck using the Superimposition Tool to determine if attachments are placed on teeth that might need them
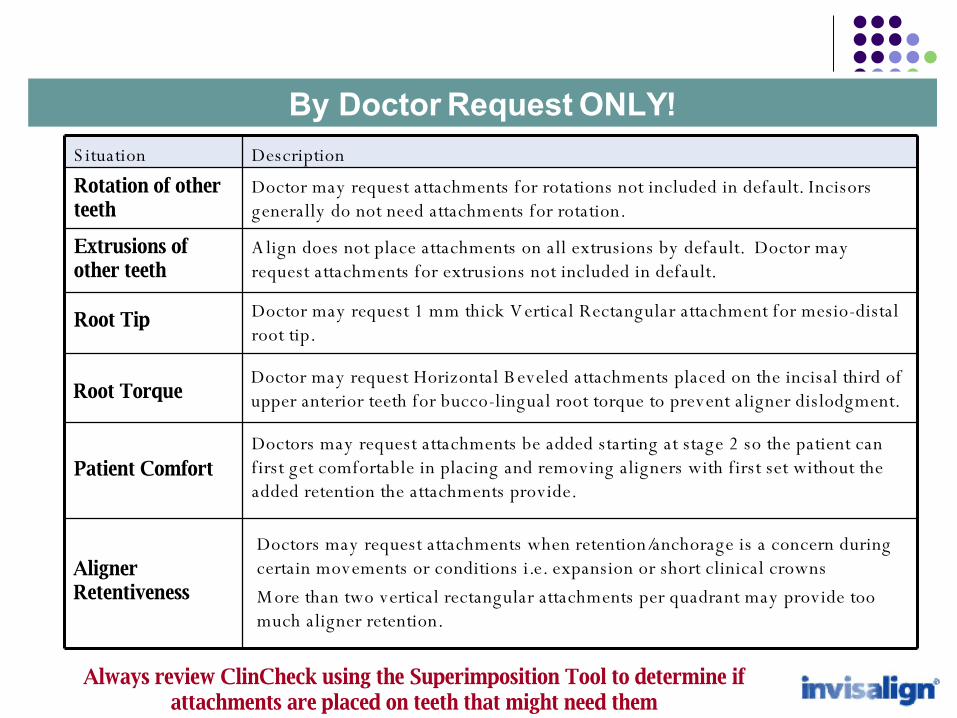
By Doctor Request ONLY!
Doctor may request 1 mm thick V ertical Rectangular attachment for mesio-distal root tip.
Root Tip
Doctors may request attachments when retention/anchorage is a concern during certain movements or conditions i.e. expansion or short clinical crowns
M ore than two vertical rectangular attachments per quadrant may provide too much aligner retention.
Aligner Retentiveness
Doctors may request attachments be added starting at stage 2 so the patient can f irst get comfortable in placing and removing aligners with first set without the added retention the attachments provide.
Patient Comfort
A lign does not place attachments on all extrusions by default. Doctor may request attachments for extrusions not included in default.
Extrusions of other teeth
Doctor may request attachments for rotations not included in default. Incisors generally do not need attachments for rotation.
Rotation of other teeth
DescriptionS ituation
Doctor may request Horizontal B eveled attachments placed on the incisal third of upper anterior teeth for bucco-lingual root torque to prevent aligner dislodgment. Root Torque
Always review ClinCheck using the Superimposition Tool to determine if attachments are placed on teeth that might need them
Making Invisalign work better…
Clean up your Treatment Preferences in order to get
consistent quality setups!
Clean up your Tx preferences!
Old Treatment preferences often conflict with the automated Best Practices Clinical Protocols.
View the initial ClinCheck set up with automated protocols for consistent quality.
If needed, modify the initial ClinCheck to address specific problems or preferences. Technicians will tend to use automated protocols
instead of complicated Tx preferences for initial setups.
Thank you!




























![Detection of Selfish Nodes in Networks Using CoopMAC Protoco[1]](https://img.pdfslide.net/doc/110x75/543ef2b4b1af9f780b8b4bf0/detection-of-selfish-nodes-in-networks-using-coopmac-protoco1.jpg)