Embed Size (px)
Citation preview


Pandiammal 24 / F
C/o Swelling B/L neck - 5 months
No fever / pain
H/o weight loss and loss of appetite
Menstrual History
Amenorrhoea - 6 months
2 children LCB - 1 ½ years
Not sterilized

Hb - 10.2 gms
TC - 14200 cells / cumm
ESR - 60
Biopsy – Acute on chronic lymphadenitis
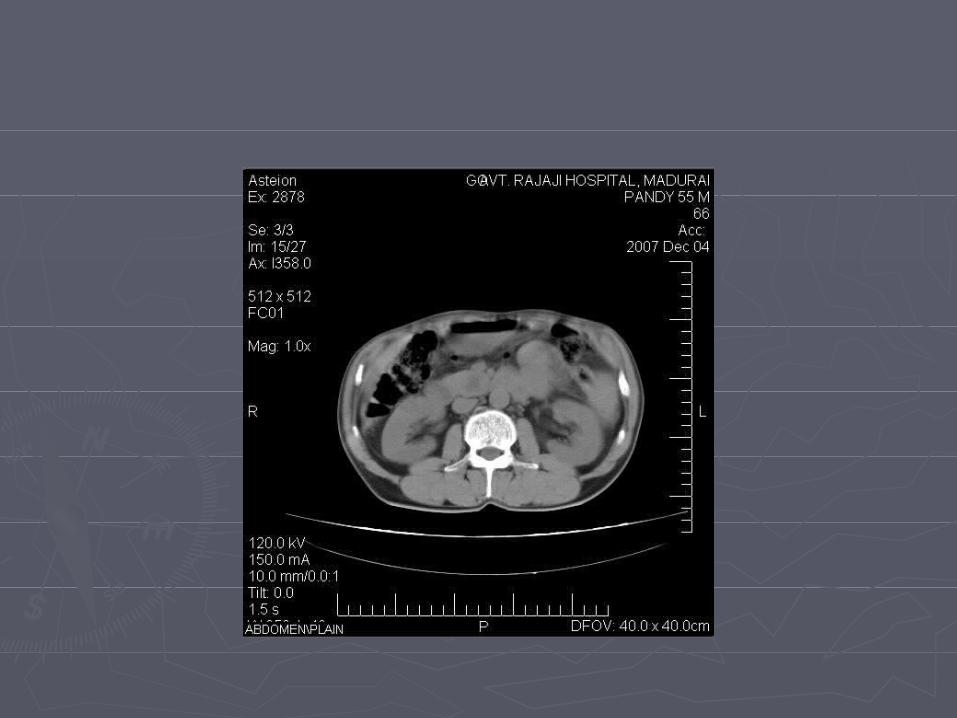
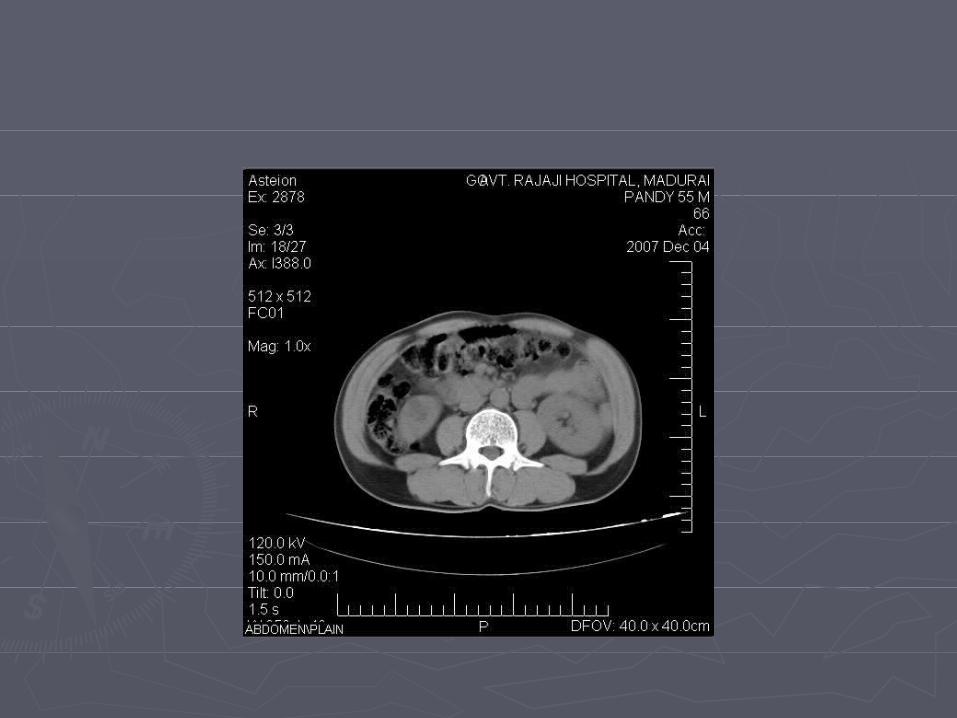
USG – multiple hypoechoeic lesions in B/L kidneys. R > L
Paraaortic, aortocaval nodes enlarged
CT

BIOPSY
LN with sinus histiocytosis exhibiting pagocytic activity.





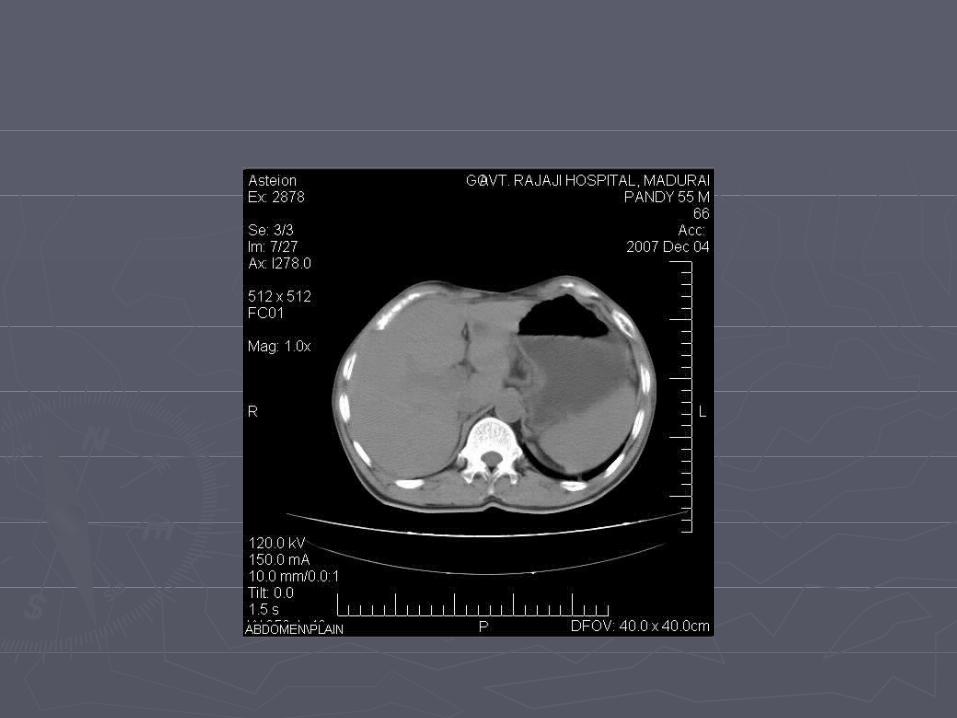

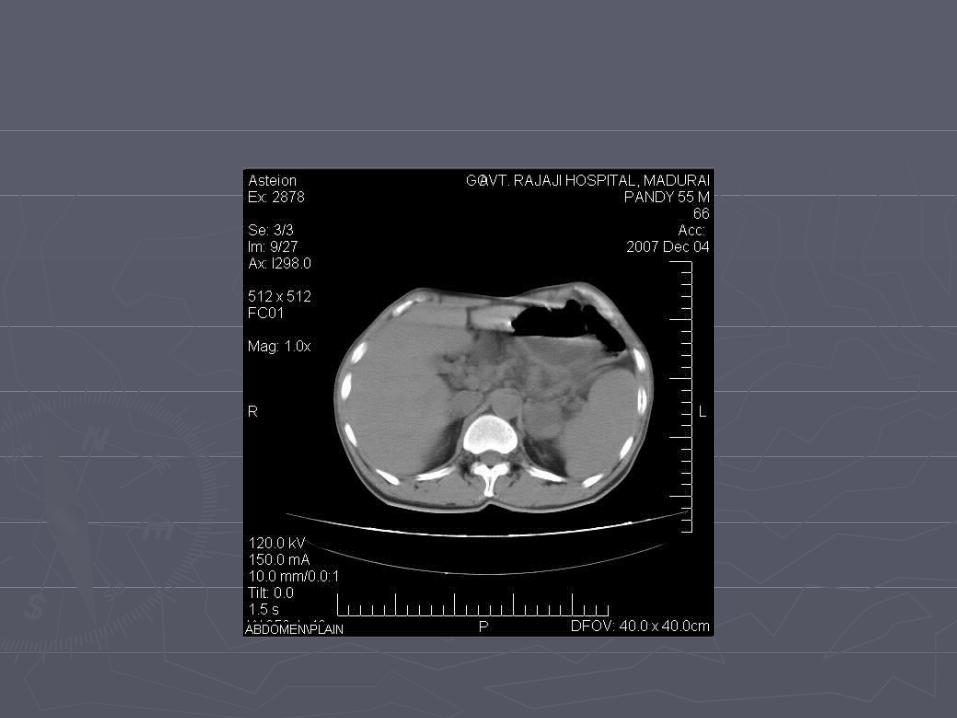





























ADRENAL METASTASIS
4th MC site next to lung, liver and bones
MC primary sites – Lung, Breast, Skin, Kidney, thyroid and colon
UL / BL
Small / large
US – Hetrogenous echogenicity
Echogenicity < than surrounding fat
CT - Small – gland contour maintained
Homogenous
Necrosis / Hge - rare

Large - Distortion of gland contour Lobulated / Irregular in shape heterogenous (necrosis / Hge) Invasion of kidneys
DD Adenoma, Lymphoma Carcinoma - rare Hge Pheochromocytoma
PANCREATIC METS
Best diagnostic clue - masses in pancreas without pancreatic / biliary duct obstuction
Type of spread – Hematogenous – MC
Lymphatic
Direct
Etiology
RCC - 30%
Br. Ca – 23%
Breast Ca
Soft tissue sarcoma
Colonic Ca

CT - Solitary (MC) / multiple
Discrete masses (MC) / Diffuse
Homo / heterogenous
Hypo / ISO attenuation
coexists with mets in Liver, LN, Adrenal gland
Ductal dilatation – Un common
DD - Pancreatic ductal Ca
Islet cell tumour
Mucinous cystic pancreatic tumour










![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://img.pdfslide.net/doc/110x75/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)