Embed Size (px)
Citation preview

ANATOMY AND PHYSIOLOGY OF CENTRAL NERVOUS SYSTEM
Dr. aparna jayara (p.g. 1st year)

Organs
CNS:• Brain• Spinal CordPNS:• Nerves

INTRODUCTION
Brain is a closed structureMost of it is brain tissue while
some of it is blood and CSFBrain comprises 80%Cerebral blood volume: 12%CSF contribute to 8% of the space
inside the skull vault.Any increase in 1 component must
be offset by equivalent decrease in other to prevent rise in ICT
Monro – Kellie doctrine

Brain
• It is one of the largest organs in the body, and coordinates most body activities.
• It is the center for all thought, memory, judgment, and emotion.
• Each part of the brain is responsible for controlling different body functions, such as temperature regulation and breathing.

Cerebrum
• It is the largest section of the brain• It is located in the upper portion of the brain and
is the area that processes thoughts, judgment, memory, problem solving, and language.
• The outer layer of the cerebrum is the cerebral cortex, which is composed of folds of gray matter.
• The cerebrum is subdivided into the left and right halves called cerebral hemispheres. Each hemisphere has 4 lobes.

Lobes of Cerebrum

Lobes of Cerebrum• 1. Frontal lobe: Most anterior portion of
the cerebrum, controls motor function, personality, and speech
• 2. Parietal lobe: The most superior portion of the cerebrum, receives and interprets nerve impulses from sensory receptors and interprets language.
• 3. Occipital lobe: The most posterior portion of the cerebrum, controls vision.
• 4. Temporal lobe: The left and right lateral portion of the cerebrum, controls hearing and smell

Cerebellum
• Second largest portion of the brain• Located beneath the posterior part of the
cerebrum• Aids in coordinating voluntary body
movements and maintaining balance and equilibrium
• Refines the muscular movement that is initiated in the cerebrum

Brain Stem
• Midbrain—acts as a pathway for impulses to be conducted between the brain and the spinal cord.
• Pons — means bridge—connects the cerebellum to the rest of the brain.
• Medulla oblongata—most inferior positioned portion of the brain; it connects the brain to the spinal cord.

Spinal Cord• Runs through the vertebral canal• Extends from foramen magnum to 2nd
lumbar vertebra• Regions
– Cervical – Thoracic – Lumbar– Sacral– Coccygeal
• Gives rise to 31 pairs of spinal nerves - all are mixed nerves

Meninges• Dura mater: outermost
layer; continuous with epineurium of the spinal nerves
• Arachnoid mater: thin and wispy
• Pia mater: bound tightly to surface

Blood Supply To The Brain

Arteries supplying the brain

2 sources of blood:ICA and VA

atlas
axis
Vertebro-basilar system CTA: CT angiography
C6
laterallyupwardbackward


Circle of Willis

Circle of Willis

Circle of Willis
oculomotor n.
abducens n.
optic chiasm
mamillary bodies
pituitary stalk

1. Circle of Willis encloses the optic chiasm, pituitary stalk and mamillary bodies.
2. Oculomotor nerve exits between the post. cerebral and sup. cerebellar arteries.
3. Vertebral arteries of the two sides unite to form the basilar artery at the ponto-medullary junction. The root of the abducens nerve and initial segment of the ant. inf. cerebellar artery can also be found here.

A1
A2



anterior cerebralmiddle cerebral
posterior cerebral


Venous drainage
3 set of veins drain from brain
1. Superficial cortical vein2. Deep cortical veins3. Dural sinuses
All ultimately drain into right and left IJV

• Almost the total volume of venous blood collected from the brain leaves the skull through the jugular foramen and the internal jugular vein.
• If the jugular foramen and/or the internal jugular vein is occluded, blood may escape through the diploic and emissary veins connecting the dural sinuses with the veins of the scalp skin.

Blood-brain barrier (BBB)The extracellular fluid of the CNS is separated from the blood by the BBB ensuring strictly controlled and mainly carrier protein assisted transport of macromolecules.Is formed by endothelial cells attached to one other by tight junctions, basement membrane, astrocytic endfeet.Protects the CNS from possibly toxic agents.

the Circumventricular organs
“Circumventricular” = around the ventriclesIncomplete or missing BBBHighly capillarized structuresSecretion of neurohormones or detection of hormones, glucose, ions, etc.


Subfornical organ sensory fluid regulation
Organum vasculosum
sensory, secretory detects peptides, fluid regulation
Median eminence secretory regulates the anterior pituitary through the release of neurohormones
Neurohypophysis secretorystore and secretes the hormones oxytocin and ADH into the blood, but does not synthesize either hormone
Subcommissural organ secretory secretes certain proteins into the cerebrospinal
fluid, its specific function is as yet unknown.
Pineal gland secretory stimulated by darkness to secrete melatonin and is associated with circadian rhythms
Area postrema sensory
the vomiting centre of the brain (can detect noxious substances in the blood and stimulate vomiting in order to rid the body of these toxic chemicals)

The cerebrospinal fluid (CSF)
• Provides mechanical protection for the brain and the spinal cord.
• When floating in the CSF brain weighs only 50g (!) according to the Archimedes’ principle.

• Cerebrospinal fluid (CSF) is a clear fluid present in the ventricles of the brain, the central canal of the spinal cord, and the subarachnoid space.
• CSF is produced in the brain by modified ependymal cells in the choroid plexus (approx. 50-70%), and the remainder is formed around blood vessels and along ventricular walls.


Circulation of CSFLateral ventricles
interventricular foramen of Monroe
third ventricle
mesencephalic aqueduct (aqueduct of Sylvius)
fourth ventricle
spinal cord central canal; also, out the lateral apertures to the subarachnoid space
to the venous system

internal and external CSF spaces
internal = ventricles external = subarachnoidal space

Site of CSF resorption: arachnoid granulations in the superior sagittal sinus and lateral lacunae.

20 ml of fluid produced every hr in choroids plexus and reabsorbed by arachnoid villi
500ml/day, yet total csf volume is only about 150 ml

Brain Functions• Vision• Taste• Cognition• Emotion• Speech• Language• Hearing• Motor Cortex• Sensory Cortex• Autonomic Functions

CerebellumThe cerebellum is connected to the brainstem, and is the center for body movement and balance.
Click image to play or pause video

ThalamusThalamus means “inner room” in Greek, as it sits deep in the brain at the top of the brainstem.
The thalamus is called the gateway to the cerebral cortex, as nearly all sensory inputs pass through it to the higher levels of the brain.

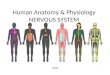
HypothalamusThe hypothalamus sits under the thalamus at the top of the brainstem. Although the hypothalamus is small, it controls many critical bodily functions:• Controls autonomic nervous system• Center for emotional response and behavior• Regulates body temperature• Regulates food intake• Regulates water balance and thirst• Controls sleep-wake cycles• Controls endocrine system
The hypothalamus is shaded blue. The pituitary gland extends from the hypothalamus.

Cerebral blood supply:Physiological considerations:
Brain accounts for 2% of body weight yet requires 20% of resting oxygen consumption
O2 requirement of brain is 3 – 3.5 ml/100gm/min
And in children it goes higher up to 5 ml/100gm/min
Brain has high metabolic rate
That’s why brain requires higher blood supply
55ml/100gm/min is the rate of blood supply
requires more requires
more substratete
substrate
requires mlacks of storage of
energy substrate

Cerebral blood supply
Cortical grey matter 75 – 80 ml/100gm/min
Subcortical white matter 20ml/100gm/min
CMRO2 : 5.5 ml/100gm/minFunctional requirement is
3.3 ml/100gm/minIntegrity required 02 is
2.2 ml/100gm/min
60% functional
40 % integrity

• High consumption bt low reserves responsible for unconsciousness within 10 sec of interruption of blood supply ( o2 tension dropping below 30mmhg, if sustained for 3-8 min can cause irrev. Injury to brain ( hippocampmpus and cerebellum being most sensitive)
• Main energy from glucose ( 5mg/100gm/min), 90% of which metabolized aerobically.

Regulation of cerebral blood flow
• CEREBRAL PERFUSION PRESSURE• CPP=MAP-ICP(CVP if it is greater than ICP)• Normally its is 80-100 mmhg, icp is normally less
than 10 mmhg, cpp is primarily dependent on MAP.
• CPP less tha 50 mmhg show slowing of EEG, those with CPP between 25 and 40 mmhg hav a flat EEG. Sustained <25 mmhg lead to irrev. Brain damage.

Regulation of cerebral blood flow


Autoregulation
• Cerebral vasculature rapidly (10-60s) adapts to change in CPP( decrease in cpp causes vasodilatation and vice versa)
• CBF remains const b/w MAP of 60-160 mmhg.• Beyond these limits , blood flow becomes
pressure dependent.

Factors regulating cerebral blood flow
• Hemodynamic autoregulation• Metabolic mediators and chemoregulation• Neural control• Circulatory peptides

Cerebral blood flow regulation
Arteriolar diameter as well as cerebral vascular resistance both vary with CPP but CBF remains constant in this range.

Cerebral blood flow regulation
2. Venous physiology:Venous system contains
most of the cerebral blood volume
Slight change in vessel diameter has profound effect on intracranial blood volume
But evidence of their role is less
Less smooth muscle content
Less innervations than arterial
system

Cerebral blood flow regulation
Pulsatile perfusion:Fast and slow components of myogenic response
bring a change in perfusion pressureCardiac output:Cardiac output may be responsible for improved
cerebral blood flowThey are indirectly related via central venous pressure and large cerebral vessel tone.

Cerebral blood flow regulation
Rheological factors:Related with blood viscosity.
Hematocrit has main influence on blood viscosity.
Flow is inversely related with hematocrit.In small vessels cells move faster than plasma.This reduces microvascular hematocrit and
viscosity FAHRAEUS LINDQVIST EFFECT

Metabolic and chemical regulation
1. Carbon dioxide
coupler between flow and metabolism
At normal conditions CBF has linear relationship with CO2 between 20 – 80 mm Hg
For every mm Hg change of PaCO2 CBF changes by 2 – 4 %

Metabolic and chemical regulation
Oxygen:Within physiological range PaO2 has no effect on
CBFHypoxia is a potent stimulus for arteriolar
dilatationAt PaO2 50 mmHg CBF starts to increase and at
PaO2 30 mm Hg it doubles

CO2 and Oxygen

Metabolic and chemical regulation
Temperature:Like other organs cerebral metabolism
decreases with temperatureFor every 1˚C fall in core body temperature
CMRO2 decreases by 7 %At temperature < 18 ˚C EEG activity ceases

Temperature

Pharmacology and autoregulation
Anaesthetic drugs can alter autoregulatory responses as seen with blood pressure and CO2 drug
CBF CMR
Preserve response to CO2
Preserve autoregulation
barbiturates ↓ ↓ yes yespropofol ↓ ↓ yes yesetomidate ↓ ↓ yes ….morphine ± ↓ …. yesfentanyl ± ± yes yesbenzodiazepines ↓ ↓ yes …ketamine ↑ ↑ yes yeslignocaine ↓ ↓ … …
response

Pharmacology and autoregulation
Inhalational agents affecting CBF
volatile anaesthetic CBF CMR
Preserve response to CO2
Preserve autoragulation
Xenon ↓ ↓ yes yesdesflurane ↑ ↓ yes yessevoflurane ↑ ↓ yes yesisoflurane ↑ ↓ yes yesenflurane ↑ ↓ yes yeshalothane ↑↑↑ ↓ yes yesnitrous oxide ↑ ↑ … …

EFFECTS @ DIFFERENT MACs

Pharmacology and autoregulationVasoactive agents:
Drugs that do not cross blood brain barrier do not affect CBF

Pharmacology and autoregulation
Dexmedetomidine: Causes 25% reduction in CBF primarily by
reducing CMR
ACE inhibitors, Angiotensin receptor antagonists, β blockers…….. Do not reduce CBF or alter autoregulation

Metabolic mediators and chemoregulation
Control CBF by acting as local vasodilatorsIons and chemicals
H+, K+, adenosine and phospholipid metabolites
Final common pathway is via NO

Neurogenic effects
Neurogenic effects: sympathetic tone shift the curve to right

Circulatory peptides:
Vasoactive peptides like angiotensin II do affect CBF.
Reactive oxygen moleculesAlteration to vasomotor functionVascular remodeling
De silva et al: effects of angiotensin II on cerebral circulation: role of oxidative stress; review article – front physiology ; jan 2013

To summarize

Clinical considerations
Hypertensive patients:Autoregulatory curve shifts to rightProtection from breakthrough but at the cost of
risk of ischemiaMay suffer cerebral ischaemia during
hemorrhage, shock or hypotension

Clinical considerations
Elderly patients:With age CBF decreasesYounger people have increased blood flow in
frontal areas…. Frontal hyperaemiaBut with age this increased flow reducesFlow in other areas are well maintained hence
blood is more uniformly distributedAutoregulatory failure occurs in morel elderly

Auto regulatory failure
For auto regulatory failure to occur vasomotor paralysis is the end point
• Acute ischemia• Mass lesions all lead to • Inflammation vasomotor• Prematurity paralysis• Neonatal asphyxia• Diabetes mellitus

Autoregulatory failure
Two stages before infarction:
a. Penlucida at flow 18 – 23 ml/100gm/min brain becomes inactive but function can be restored at any time by reperfusion
b. Penumbra at lower flow rates brain function can be restored by reperfusion but only within a time limit

Hemodynamic considerationsCerebral steal: it means blood is diverted from
one area to another if pressure gradient exists between the two circulatory beds
Vasodilatation in non ischemic brain takes blood from ischemic areas to normal areas causing more ischemia
Vasoconstriction results in redistribution of blood from normal to ischemic areas leading to inverse steal or ROBIN HOOD EFFECT

Hemodynamic considerations
Vessel length and viscosity At breakthrough point flow depends on vessel
length and viscosityAutoregulation has failed and it behaves like
fluid in a rigid tubePressure gradient across the ends are now same
so distal area have the lowest flowThis makes watershed areas more vulnerable to
ischemic changes

Considerations for ischemia
Consideration relevant to global ischemia
Prevent and treat hypotension as well asvasogenic & cytotoxic
edema
Induction of mild hypothermia for 24 hrs
Consideration relevant to focal ischemia
Barbiturate coma, volatile anesthetics (xenon),
calcium channel antagonists
PaCO2 and temperature

Therapies for enhancing perfusion
• Induced hypertension• Inverse steal• Hypocapnea• Hemodilution• Pharmacological agents
• Barbiturates, propofol
• Intra arterial delivery of drugs. Like mannitol and vasodilators

Thank You !!!