Embed Size (px)
Citation preview
- CyberKnife radiosurgery for single & ‘Oligo’ Vertebral metastasis in a reality.
- Ph II studies have shown significant benefit with higher dose SRS in terms of pain
control, requirement of re-RT
- Ph III studies with 400+ patients with high dose SRS (16Gy), initial results are
promising and shows positive outcome
- However, high dose SRS is also associated with high incidence of myelitis & vertebral
fracture
- Spinal AVMs: CyberKnife radiosurgery is the treatment of choice
Vertebral metastasis: CyberKnife
Vertebral metastasis
Spinal epndymoma / meningioma
Spinal metastasis
Spinal haemangioma/ haemangioblastoma
Spinal AVM
Spinal tumours: Radiosurgery
Conv RT: Bone metastasis
8Gy/1# OR 30Gy10#Wide marginAP/PA fieldOne vertebra other side in the field
Pain control rate 40-50%
Systemic review of randomized Pall RT trials: SFs Vs MFsSFs: 8Gy/1#MFs: 20Gy/5# OR 30Gy10# OR 40Gy/20#16 RCTs since 1986N=>5000Intention to treat & accessible pt analysis done
Chow E et al JCO 2007
Pall RT in bone metastasis
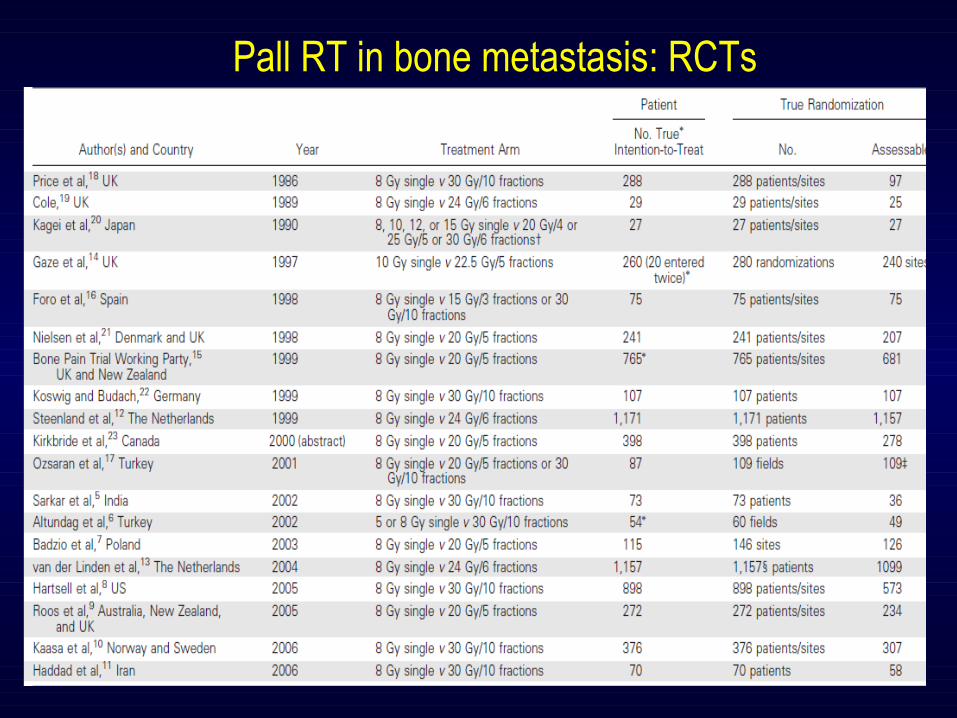
Pall RT in bone metastasis: RCTs
Pall RT in bone metastasisIntention to treat analysis:Overall response: SF= 58% (1468 / 2513 pt)MF= 59% (1466/ 2487 pt)ODD’s ratio= 0.99 (0.95-1.03)
Complete response:SF= 23% (545/2375 pt)MF= 24% (558/2351 pt)ODD’s ratio= 0.97 (0.88-1.06)
Increased risk in SF arm:Pathological #: 3.2% SF Vs 2.8% MF (p=0.75)Spinal cord compression: 2.8% SF Vs 1.9% MF (p=0.13)
Re-RT rate:SF= 20% Vs MF 8% (p=0.0001) Likelihood ratio 2.5
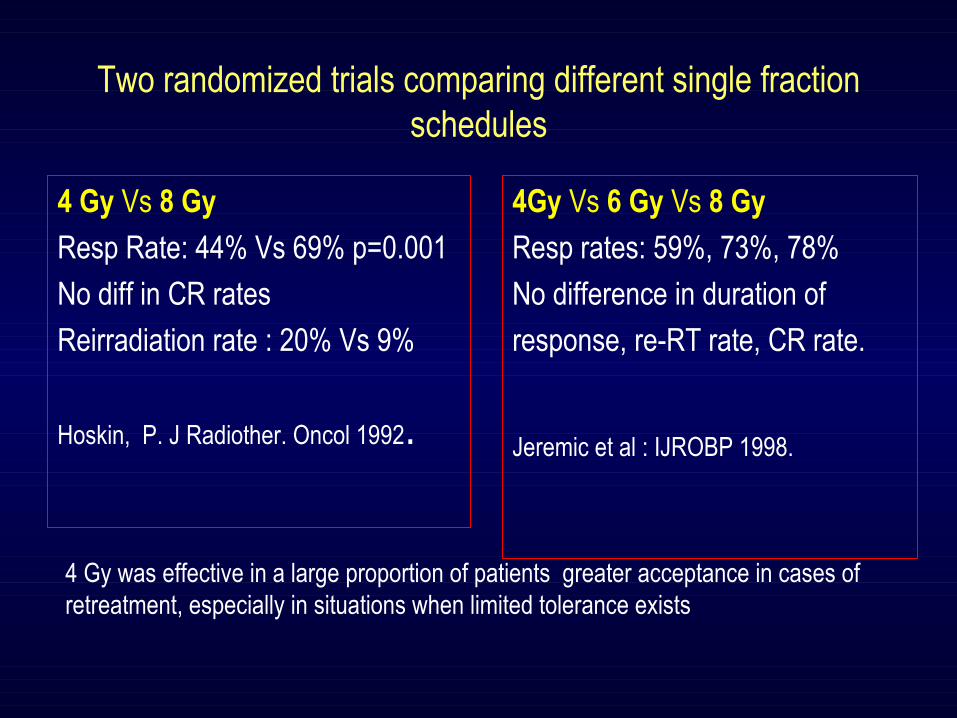
Two randomized trials comparing different single fraction schedules
4Gy Vs 6 Gy Vs 8 Gy
Resp rates: 59%, 73%, 78%
No difference in duration of
response, re-RT rate, CR rate.
Jeremic et al : IJROBP 1998.
4 Gy Vs 8 Gy
Resp Rate: 44% Vs 69% p=0.001
No diff in CR rates
Reirradiation rate : 20% Vs 9%
Hoskin, P. J Radiother. Oncol 1992.
4 Gy was effective in a large proportion of patients greater acceptance in cases of retreatment, especially in situations when limited tolerance exists
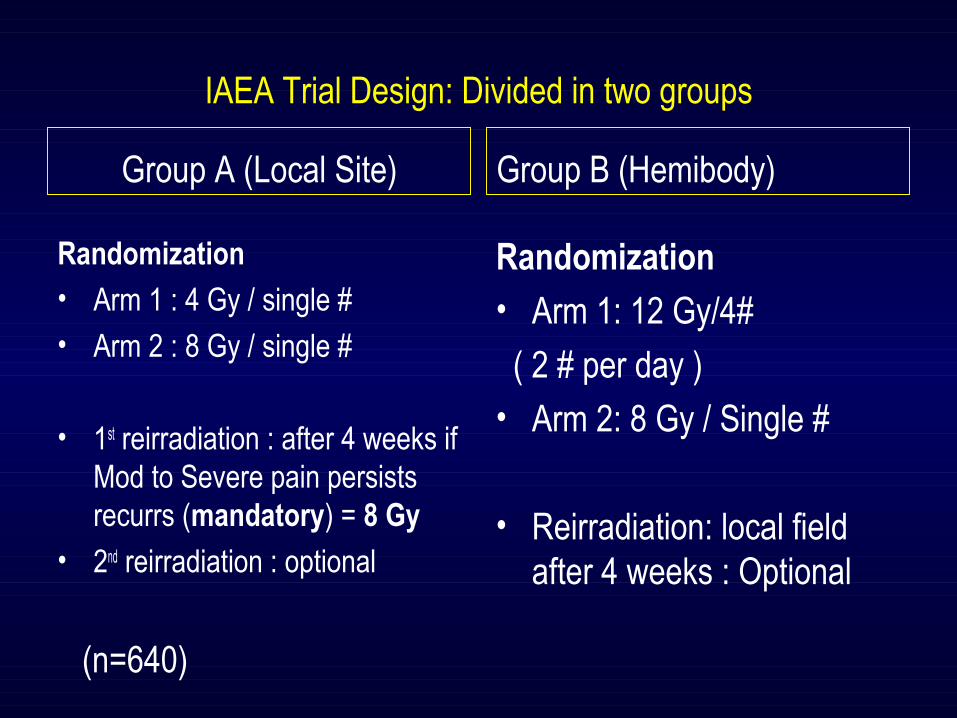
IAEA Trial Design: Divided in two groups
Group A (Local Site)
Randomization• Arm 1 : 4 Gy / single #• Arm 2 : 8 Gy / single #
• 1st reirradiation : after 4 weeks if Mod to Severe pain persists recurrs (mandatory) = 8 Gy
• 2nd reirradiation : optional
Group B (Hemibody)
Randomization• Arm 1: 12 Gy/4#
( 2 # per day )• Arm 2: 8 Gy / Single #
• Reirradiation: local field after 4 weeks : Optional
(n=640)
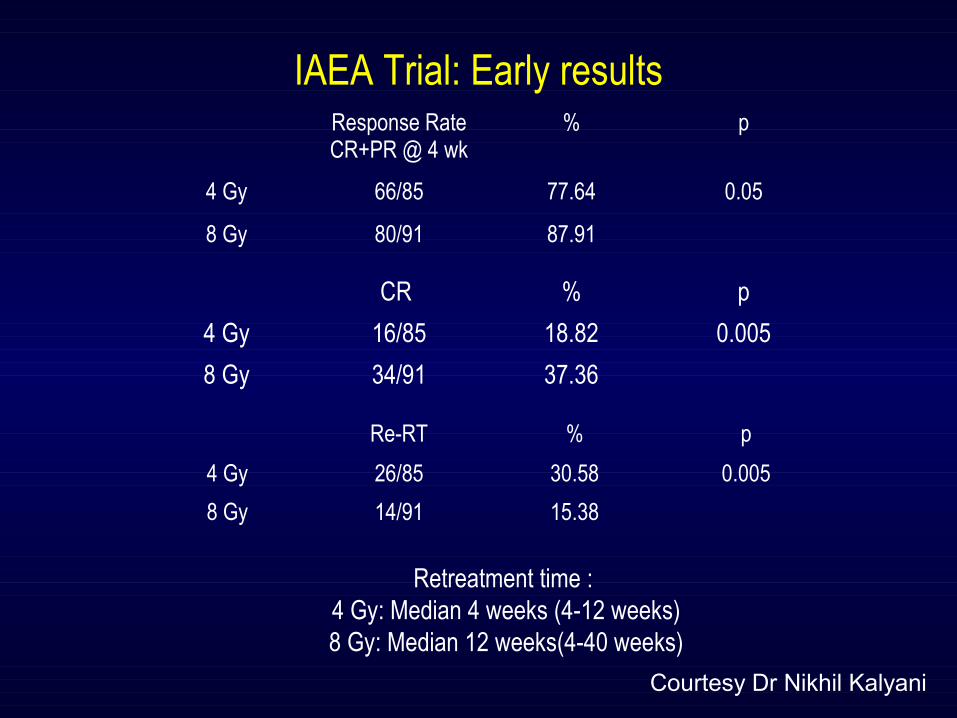
Response RateCR+PR @ 4 wk
% p
4 Gy 66/85 77.64 0.05
8 Gy 80/91 87.91
CR % p
4 Gy 16/85 18.82 0.005
8 Gy 34/91 37.36
Re-RT % p
4 Gy 26/85 30.58 0.005
8 Gy 14/91 15.38
Retreatment time : 4 Gy: Median 4 weeks (4-12 weeks)8 Gy: Median 12 weeks(4-40 weeks)
IAEA Trial: Early results
Courtesy Dr Nikhil Kalyani
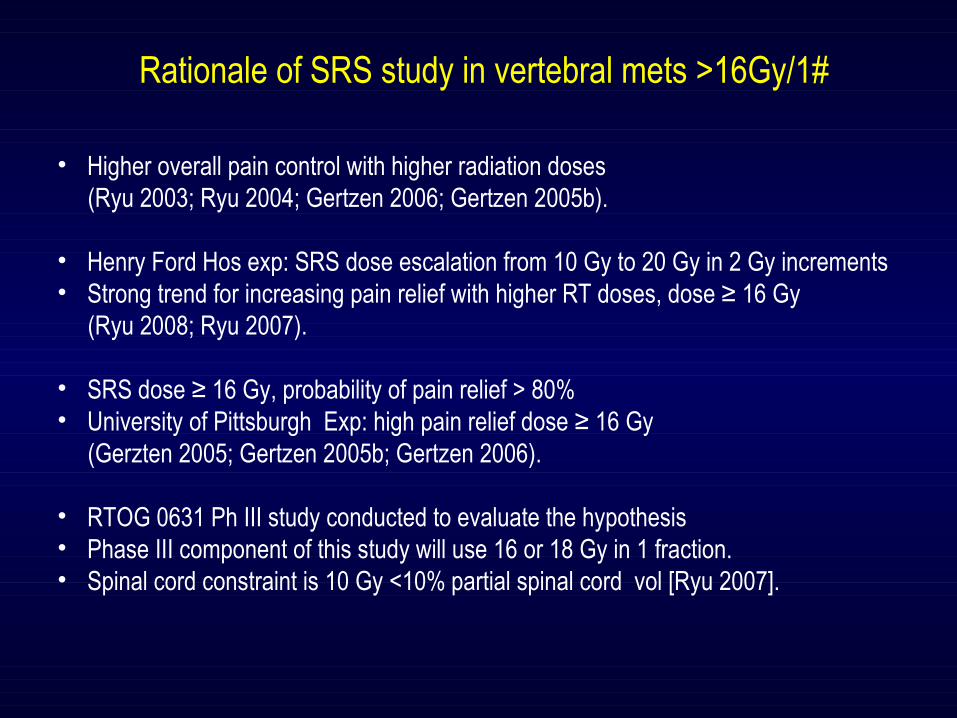
• Higher overall pain control with higher radiation doses (Ryu 2003; Ryu 2004; Gertzen 2006; Gertzen 2005b).
• Henry Ford Hos exp: SRS dose escalation from 10 Gy to 20 Gy in 2 Gy increments• Strong trend for increasing pain relief with higher RT doses, dose ≥ 16 Gy (Ryu 2008; Ryu 2007).
• SRS dose ≥ 16 Gy, probability of pain relief > 80% • University of Pittsburgh Exp: high pain relief dose ≥ 16 Gy (Gerzten 2005; Gertzen 2005b; Gertzen 2006).
• RTOG 0631 Ph III study conducted to evaluate the hypothesis • Phase III component of this study will use 16 or 18 Gy in 1 fraction. • Spinal cord constraint is 10 Gy <10% partial spinal cord vol [Ryu 2007].
Rationale of SRS study in vertebral mets >16Gy/1#
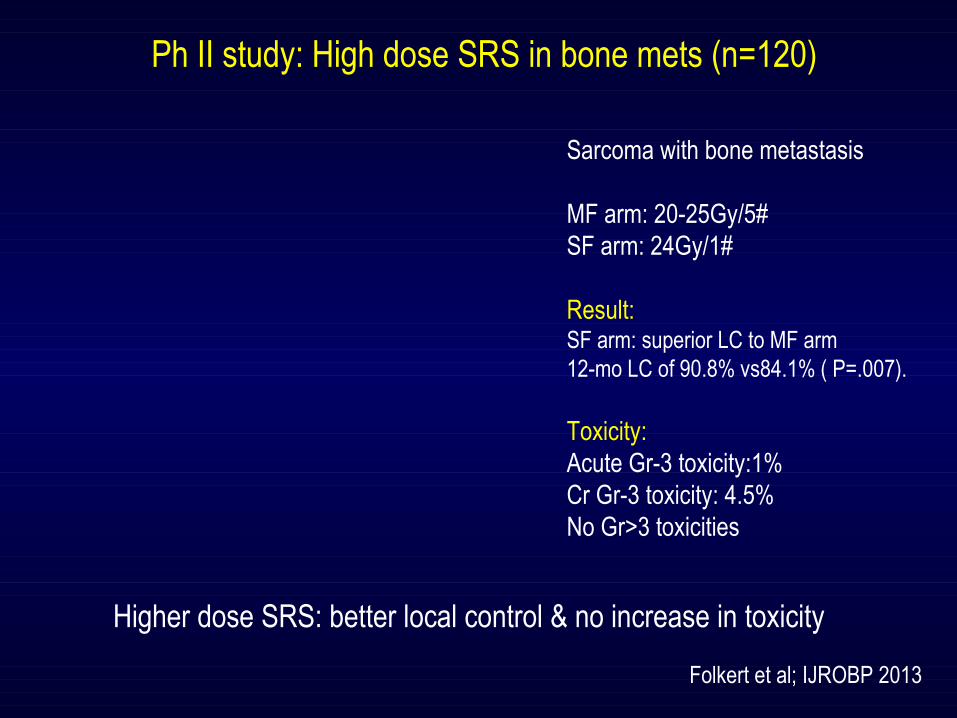
Ph II study: High dose SRS in bone mets (n=120)
Sarcoma with bone metastasis
MF arm: 20-25Gy/5#SF arm: 24Gy/1#
Result: SF arm: superior LC to MF arm12-mo LC of 90.8% vs84.1% ( P=.007).
Toxicity:Acute Gr-3 toxicity:1%Cr Gr-3 toxicity: 4.5%No Gr>3 toxicities
Higher dose SRS: better local control & no increase in toxicity
Folkert et al; IJROBP 2013
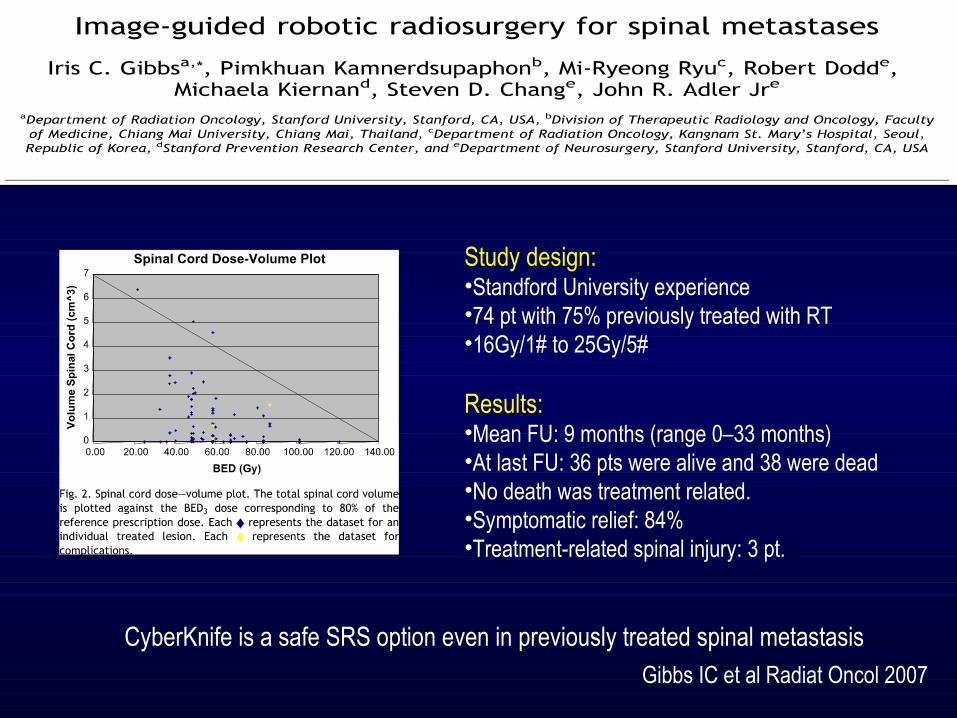
Study design:•Standford University experience•74 pt with 75% previously treated with RT•16Gy/1# to 25Gy/5#
Results:•Mean FU: 9 months (range 0–33 months)•At last FU: 36 pts were alive and 38 were dead•No death was treatment related. •Symptomatic relief: 84%•Treatment-related spinal injury: 3 pt.
Gibbs IC et al Radiat Oncol 2007
CyberKnife is a safe SRS option even in previously treated spinal metastasis
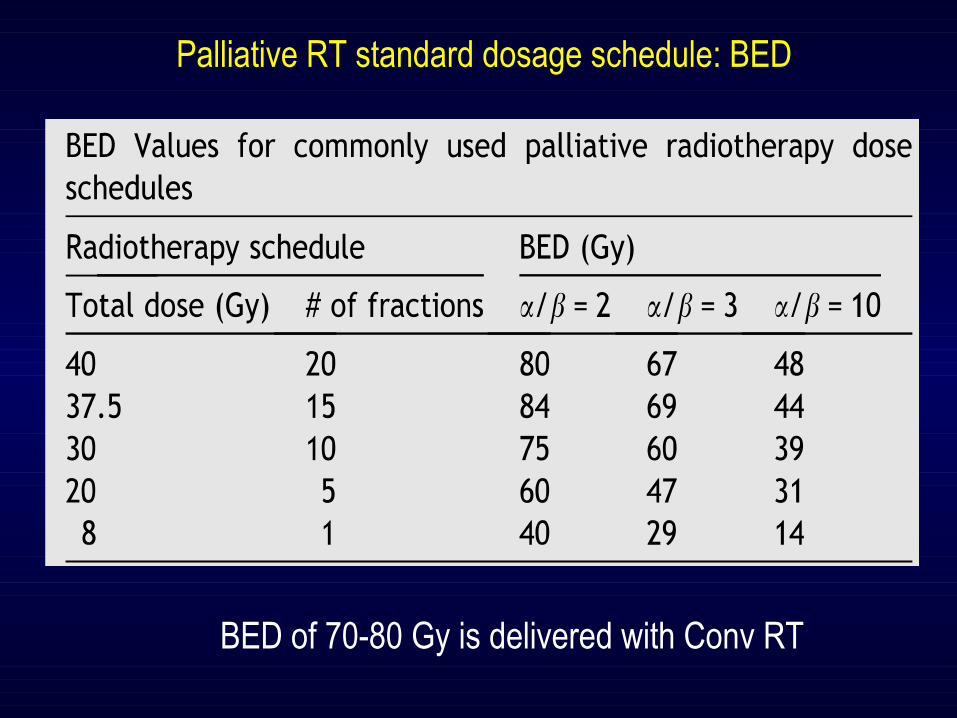
Palliative RT standard dosage schedule: BED
BED of 70-80 Gy is delivered with Conv RT
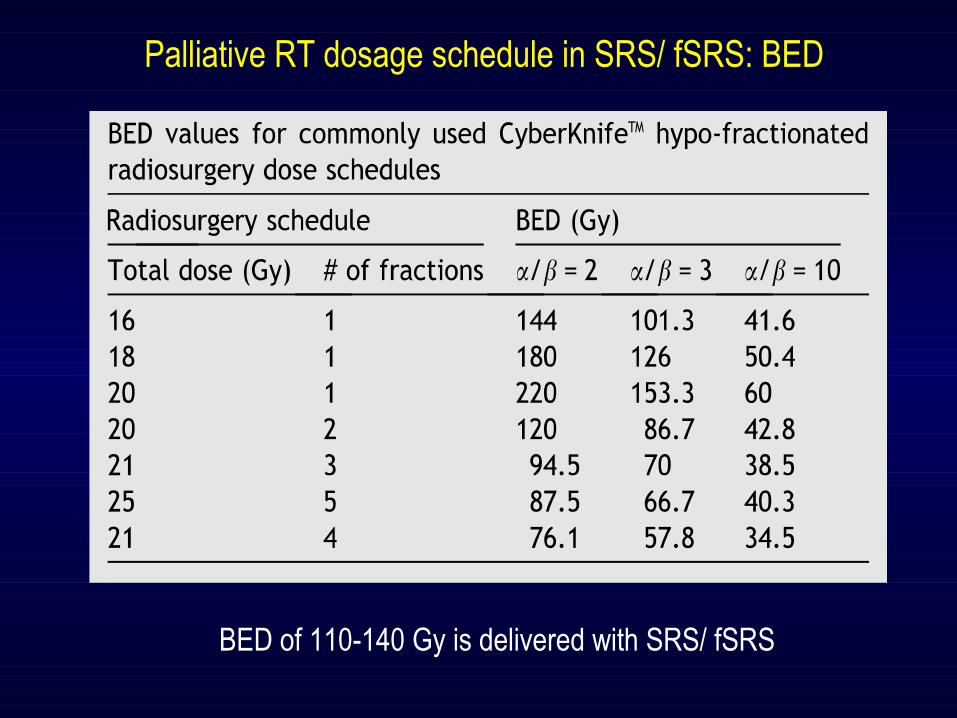
Palliative RT dosage schedule in SRS/ fSRS: BED
BED of 110-140 Gy is delivered with SRS/ fSRS
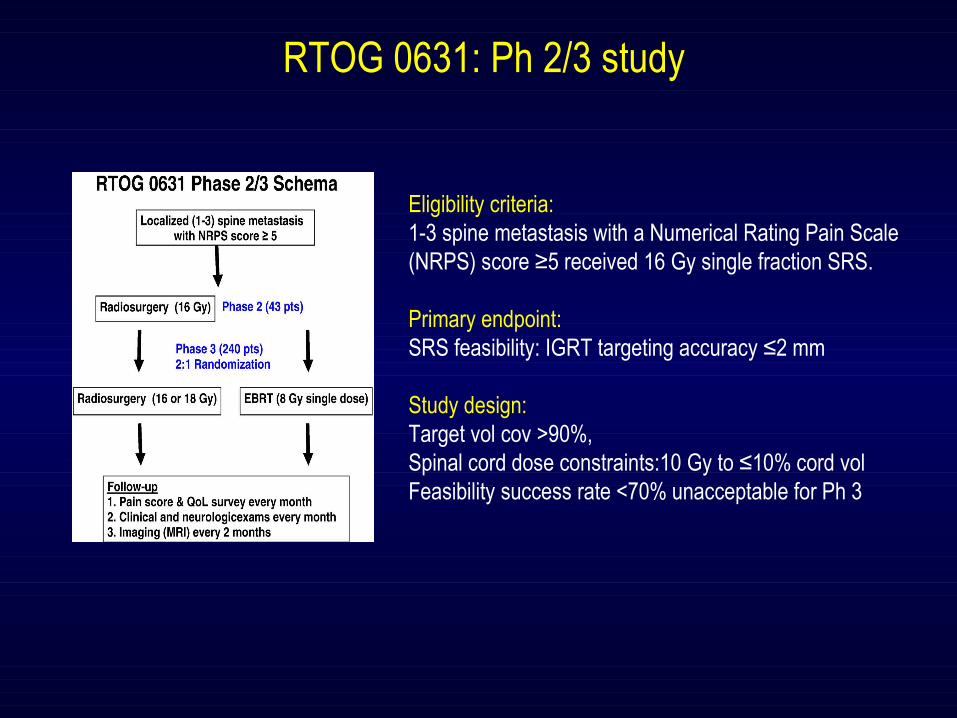
RTOG 0631: Ph 2/3 study
Eligibility criteria:1-3 spine metastasis with a Numerical Rating Pain Scale(NRPS) score ≥5 received 16 Gy single fraction SRS.
Primary endpoint: SRS feasibility: IGRT targeting accuracy ≤2 mm
Study design:Target vol cov >90%, Spinal cord dose constraints:10 Gy to ≤10% cord vol Feasibility success rate <70% unacceptable for Ph 3

RTOG 0631: Ph 2/3 study
74% procedure as per protocolONLY 10% unacceptable
Eligible criteria:•PS0-1•Age>18•NRPS >5
Plan:Arm 1: 16Gy/1# coverage >90%Arm 2: 8Gy/1#
End point:•Pain relief at least 3 points at 3 mo•QOL: FACT G / Brief pain inventory
RTOG 0631: Ph III study Eligibility criteria
PI: Samuel RyuPitsburg Hospital initiated
RTOG 0631, version date 4/21/14 14
metastasis is included in the target volume. In this study, the terms, GTV or CTV, are not used. The target as defined above will not be enlarged (i.e., no “margin” for presumed microscopic extension). This target volume ultimately becomes the radiosurgery planning target volume. The radiosurgery does not assume set-up errors. However, depending on the radiosurgery system, a beam aperture margin of 2-3 mm beyond the target volume is allowed to meet the adequate dose coverage of the target. This margin can be reduced to 0-1 mm at the area of spinal cord to meet the spinal cord dose constraints. The treatment plan is acceptable as long as ≥ 90% of the target volume receives the prescribed radiosurgery dose.
Examples of radiosurgery target volumes are illustrated in Figure 2. Solid black represents
the tumor that can be seen on the imaging studies.
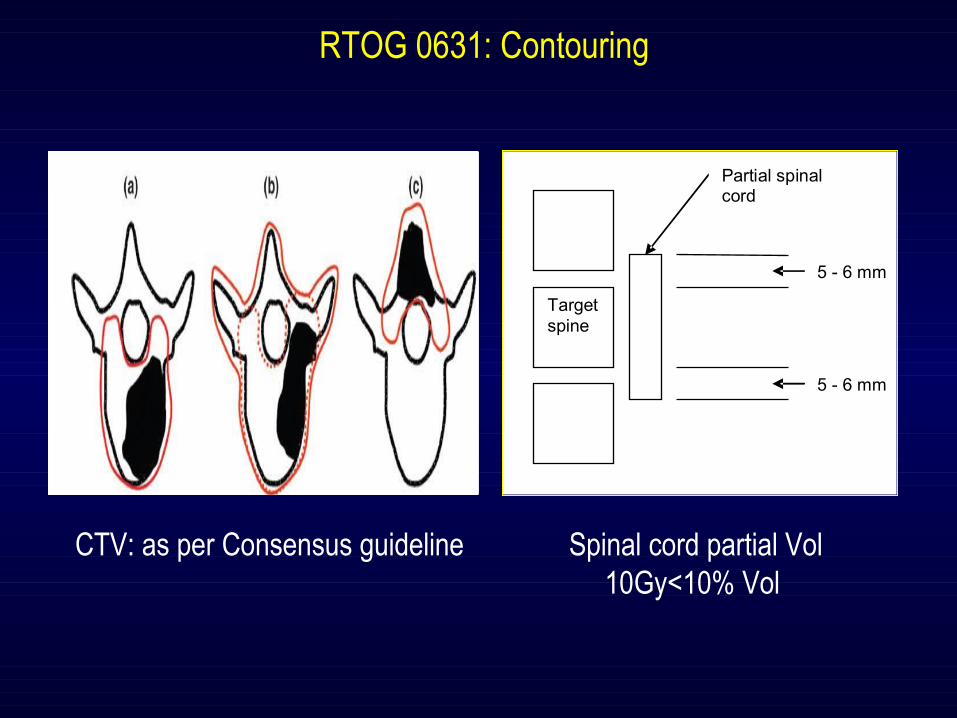
Most of the spine metastases involve the vertebral body and the gross tumor seen on MRI or CT scan, as shown in Figure 2a below. This is the most common type of spine metastasis. The radiosurgery target volume includes the involved vertebral body and both pedicles (solid red line).
Metastatic lesions can be more extensive, involving the pedicles [Figure 2b]. The target
volume can be more generous [dotted line of Figure 2b], or the target volume can include anterior and posterior elements of the spine [solid red line of Figure 2b]. The target volume may be chosen at the discretion of the treating Radiation Oncologist based on the extent of tumor involvement.
When the metastasis involves only the posterior element, the target volume includes the
spinous process and laminae [solid red line of Figure 2c]. In any circumstance, when there is an epidural or paraspinal soft tissue tumor component,
the visible epidural or paraspinal tumors are included in the target volume.
Figure 2: Diagram of Spine Metastasis and Target Volume
6.3.1.2 Spinal Cord Volume Two spinal cord contour sets are required for this protocol: the conventional and the partial
spinal cord volumes. The conventional spinal cord volume is contoured on the simulation CT based on the image
fusion with T2-weighted and T1-weighted MRI with contrast. It is recommended that a simulation CT be done with contrast, but this is not required. The conventional spinal cord should be contoured starting at least 10 cm above the superior extent of the target volume and continuing on every CT slice to at least 10 cm below the inferior extent of the target
RTOG 0631, version date 4/21/14 15
volume. This spinal cord volume is required to be consistent with image-guided radiotherapy volume definition of NRG Oncology protocols.
The partial spinal cord volume is specific to this study. The definition of partial spinal cord
volume is shown in Figure 3below. The spinal cord is contoured based on the image fusion with T2-weighted and T1-weighted MRI with contrast. It is recommended that a simulation CT image be done with contrast, but this is not required. The partial spinal cord should be contoured starting from 5-6 mm above the superior extent of the target volume to 5-6 mm below the inferior extent of the target volume. The spinal cord should be drawn on every slice of simulation CT. The variation of 5-6 mm is due to the pre-determined slice thicknesses of 2.5-3 mm by different CT manufacturers.
Three cord dose constraints are used in this study: 1) the dose constraints for the partial spinal cord is 10 Gy to no more than 10% of the partial spinal cord volume; or 2) the dose constraint for the conventional spinal cord is 10 Gy to the spinal cord volume less than 0.35cc; or 3) the maximum cord dose is 14 Gy for less than 0.03cc. These constraints are applied to the treated spine level. Any spinal cord dose exceeding these constraints is not acceptable and is a major deviation.
Figure 3: Diagram of Defining Partial Spinal Cord Volume
Radiosurgery is not recommended for any cases that do not meet the spinal cord constraints. Each CT slice within the radiosurgery plan should be checked to screen any unacceptably high radiation dose to the spinal cord at any particular slice. In this situation, the treating physician can make the decision of proceeding or stopping the radiosurgery or to perform re-planning. Critical organs including spinal cord, liver, kidneys, and lung should be analyzed for radiation dose distribution if any of them are transected by any radiation field. The dose-volume guidelines are described in Sections 6.3.2 and 6.4.
6.3.2 Dosimetry Intensity-modulated radiation therapy (IMRT) or other dose painting techniques will be used to
deliver highly conformal dose distributions. Non-coplanar beams can be employed. Non-opposing beams are preferable. Multiple beam directions or arcs of radiation will be used for geometrically complicated lesions. The beam arrangement should be placed mostly from the posterior direction to avoid the radiation beam entering through the lungs. Intensity-modulated arc therapy with either multiple static cones or dynamic conformal multileaf collimators (MLC) can be used. For arc rotational techniques, every effort should be used to limit the radiation through the lung.
A common point should be defined, which is close to the center of the target volume for dose
normalization. Preferably, this point is placed at the treatment isocenter if a linac based delivery system is used. The plan should be normalized to the common point or isocenter or its vicinity suitable for dose normalization. Typically, this point will be the isocenter of the beam rotation; however, it is not a protocol requirement for this point to be the isocenter. Inhomogeneity
Target spine
Partial spinal cord
5 - 6 mm
5 - 6 mm
RTOG 0631: Contouring
CTV: as per Consensus guideline Spinal cord partial Vol10Gy<10% Vol
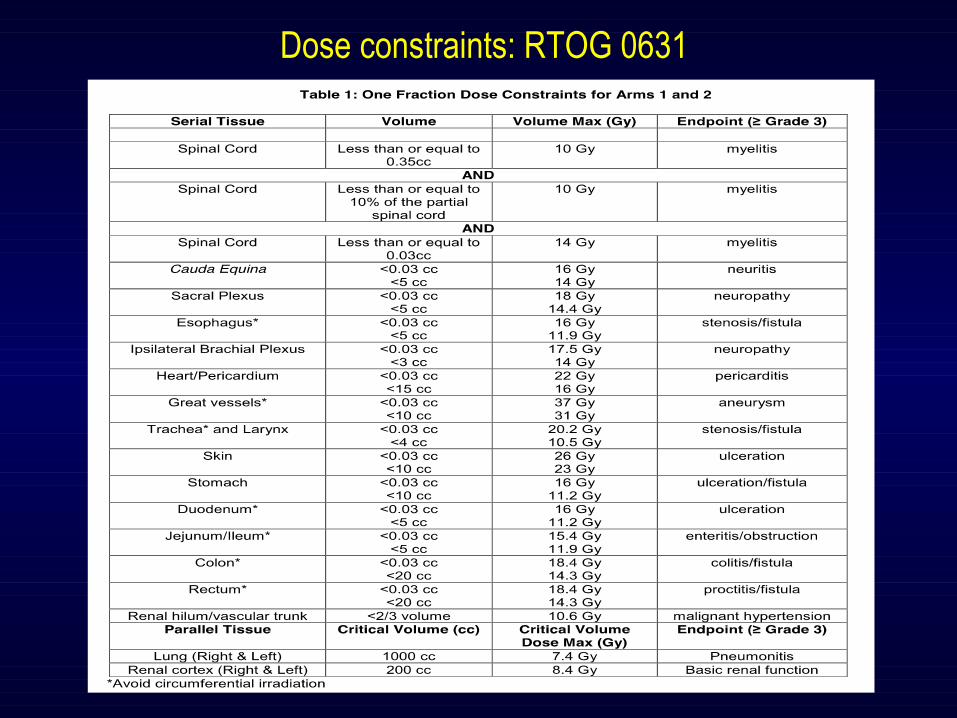
Dose constraints: RTOG 0631
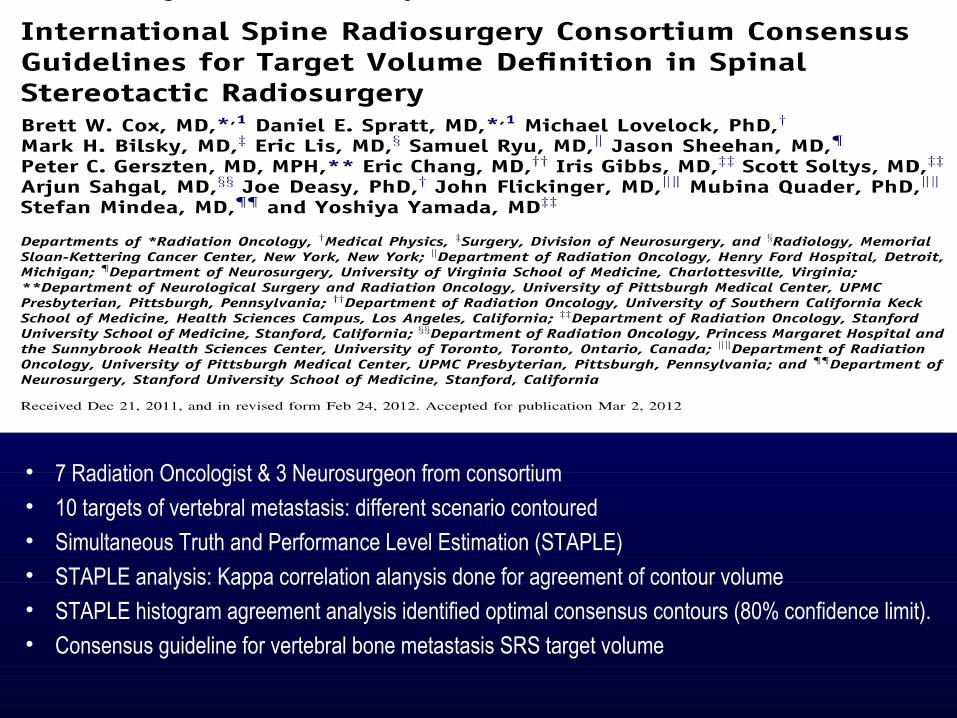
• 7 Radiation Oncologist & 3 Neurosurgeon from consortium• 10 targets of vertebral metastasis: different scenario contoured• Simultaneous Truth and Performance Level Estimation (STAPLE)• STAPLE analysis: Kappa correlation alanysis done for agreement of contour volume• STAPLE histogram agreement analysis identified optimal consensus contours (80% confidence limit).• Consensus guideline for vertebral bone metastasis SRS target volume
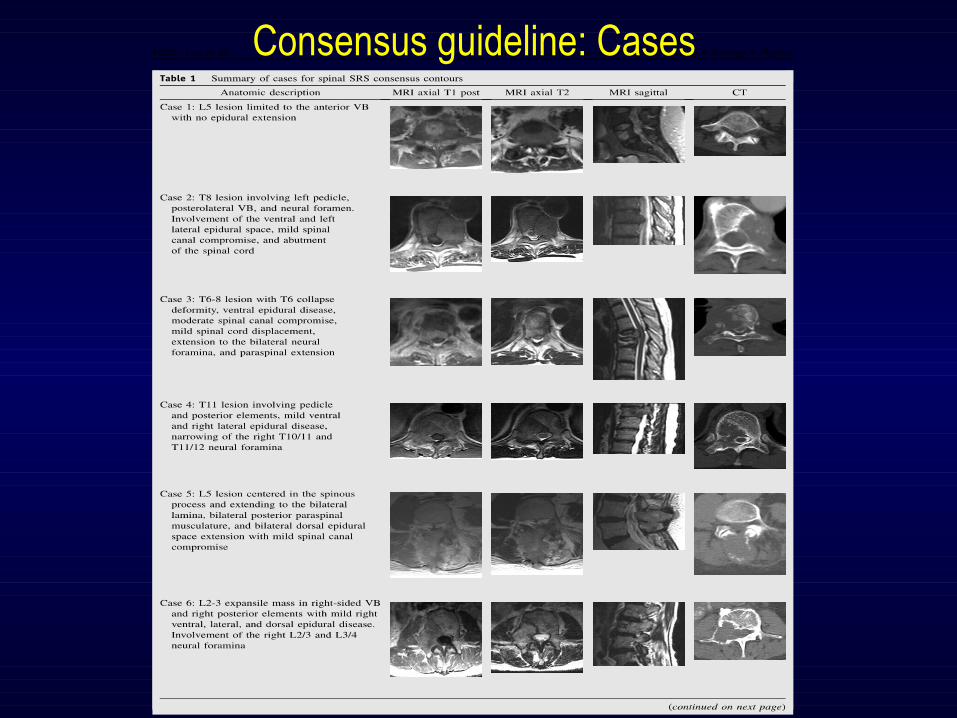
Consensus guideline: Cases
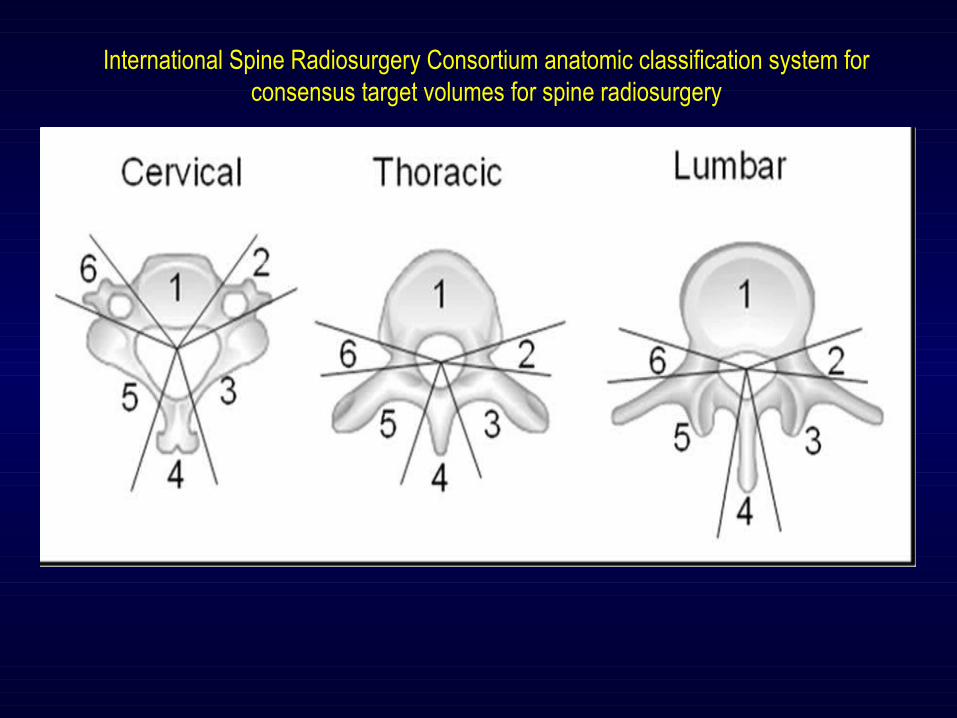
International Spine Radiosurgery Consortium anatomic classification system for consensus target volumes for spine radiosurgery
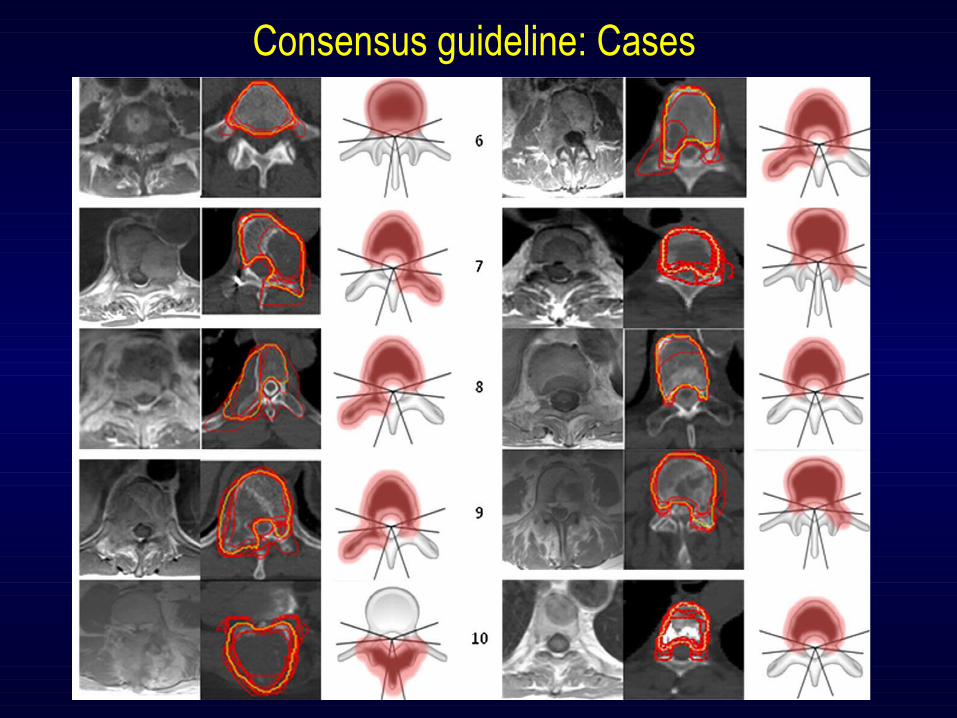
Consensus guideline: Cases
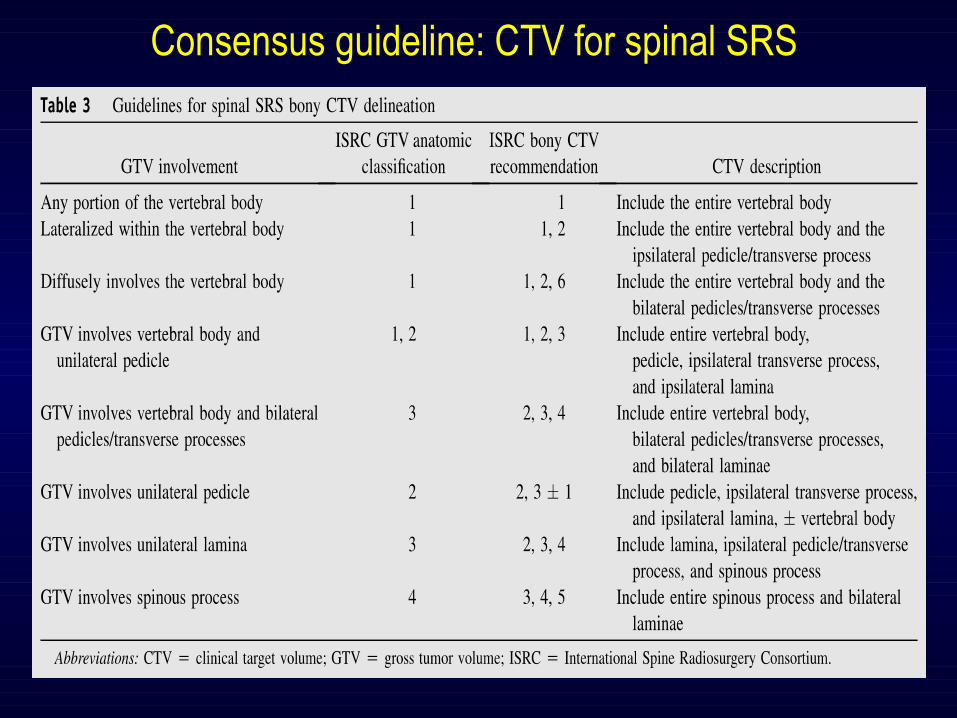
Consensus guideline: CTV for spinal SRS
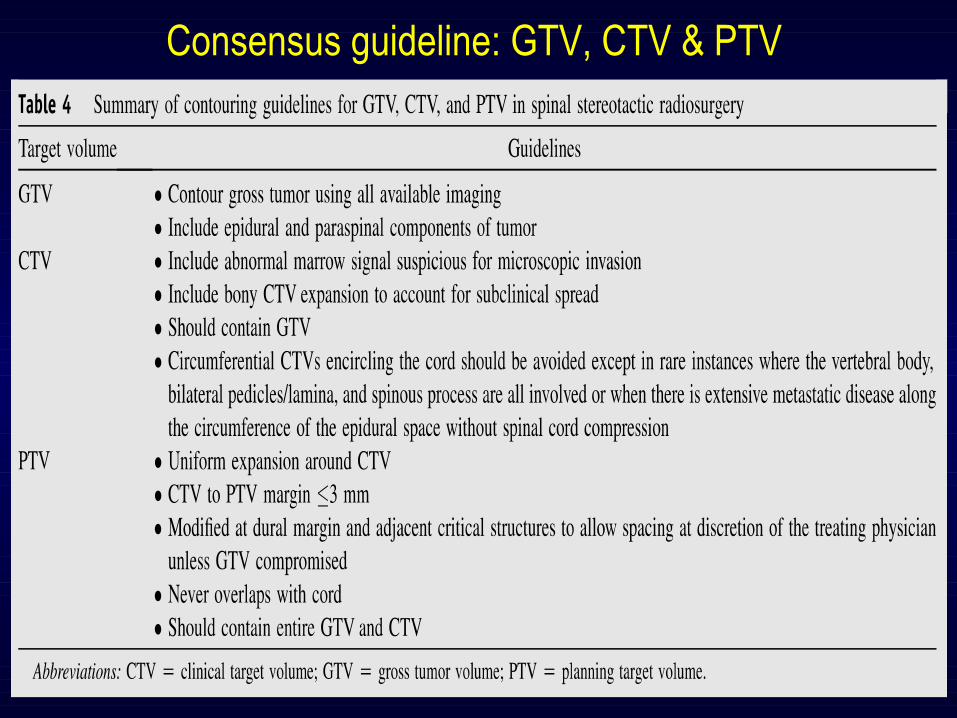
Consensus guideline: GTV, CTV & PTV
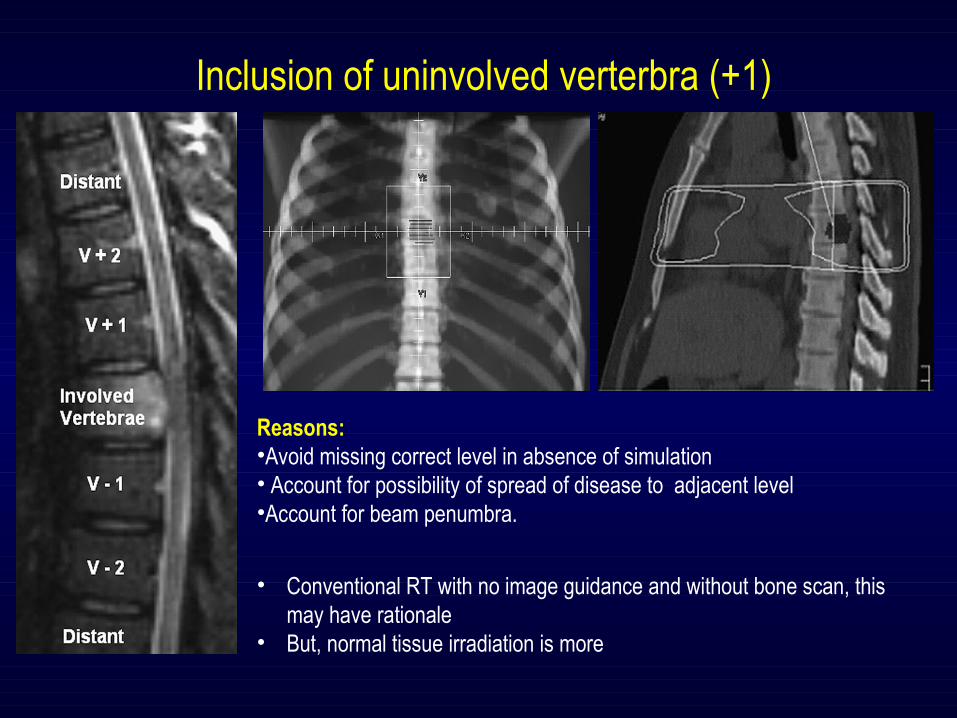
Inclusion of uninvolved verterbra (+1)
Reasons: •Avoid missing correct level in absence of simulation• Account for possibility of spread of disease to adjacent level•Account for beam penumbra.
• Conventional RT with no image guidance and without bone scan, this may have rationale
• But, normal tissue irradiation is more
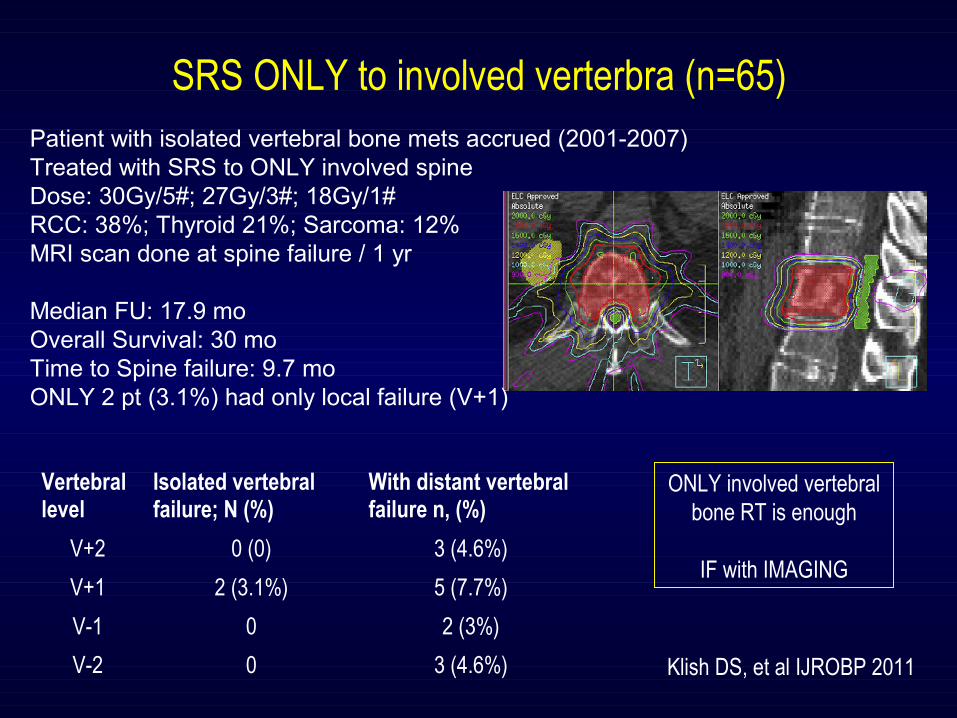
SRS ONLY to involved verterbra (n=65) Patient with isolated vertebral bone mets accrued (2001-2007)Treated with SRS to ONLY involved spineDose: 30Gy/5#; 27Gy/3#; 18Gy/1#RCC: 38%; Thyroid 21%; Sarcoma: 12%MRI scan done at spine failure / 1 yr
Median FU: 17.9 moOverall Survival: 30 moTime to Spine failure: 9.7 moONLY 2 pt (3.1%) had only local failure (V+1)
Vertebral level
Isolated vertebral failure; N (%)
With distant vertebral failure n, (%)
V+2 0 (0) 3 (4.6%)
V+1 2 (3.1%) 5 (7.7%)
V-1 0 2 (3%)
V-2 0 3 (4.6%) Klish DS, et al IJROBP 2011
ONLY involved vertebral bone RT is enough
IF with IMAGING
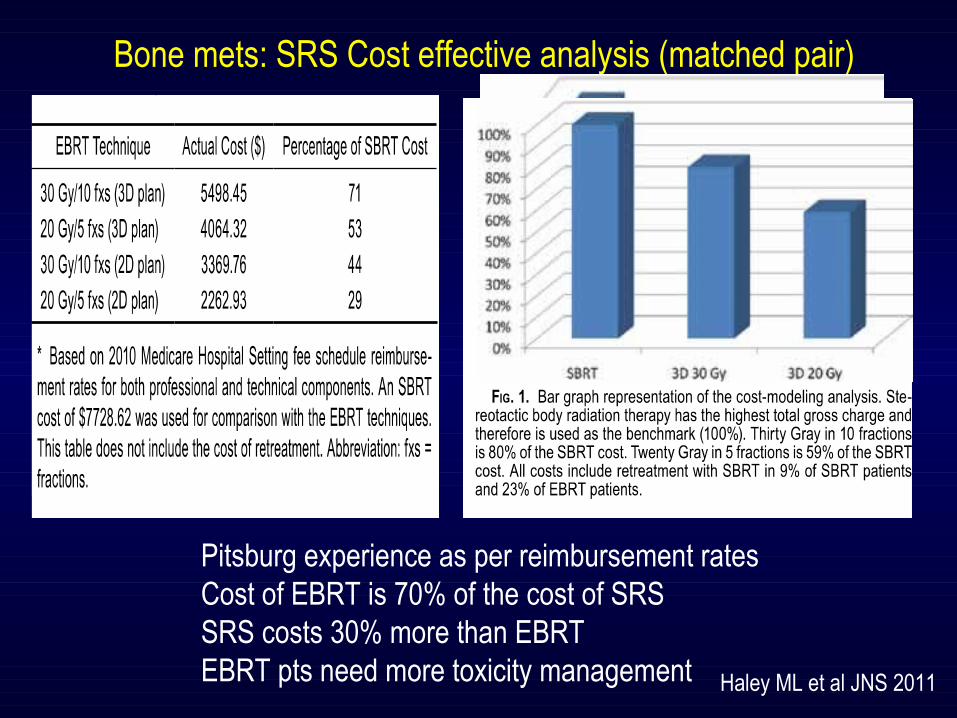
Pitsburg experience as per reimbursement ratesCost of EBRT is 70% of the cost of SRS SRS costs 30% more than EBRTEBRT pts need more toxicity management
Bone mets: SRS Cost effective analysis (matched pair)
Haley ML et al JNS 2011
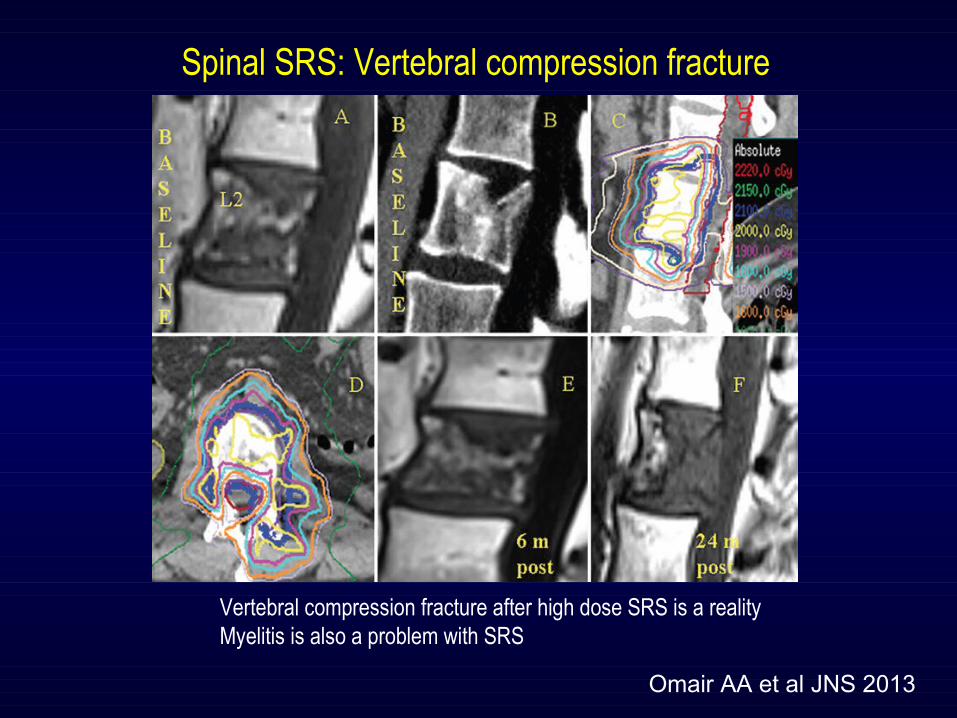
Spinal SRS: Vertebral compression fracture
Omair AA et al JNS 2013
Vertebral compression fracture after high dose SRS is a realityMyelitis is also a problem with SRS
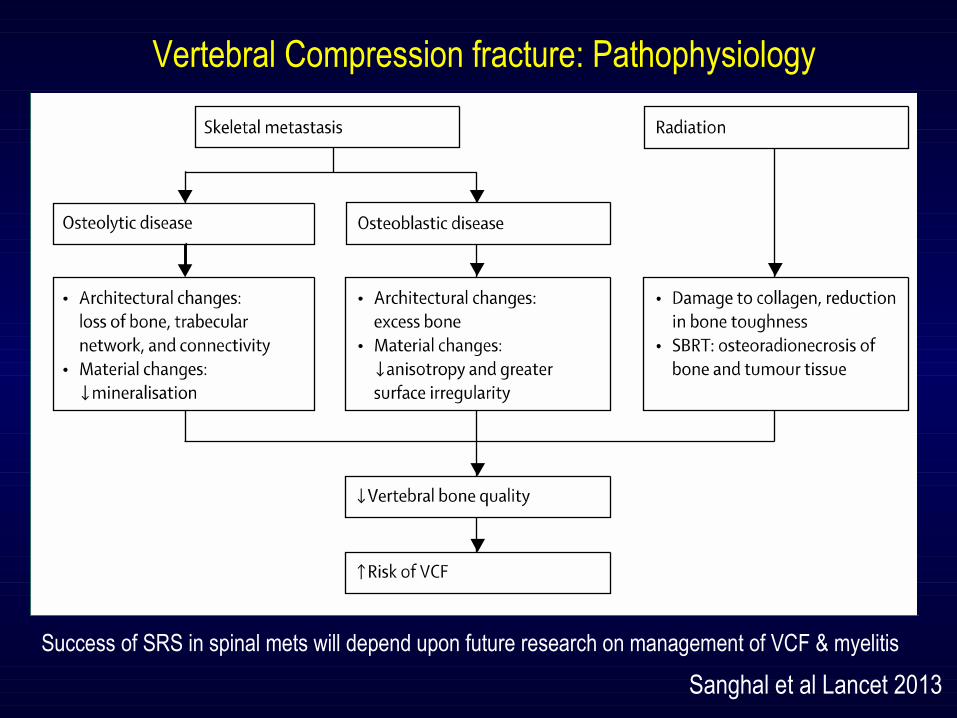
Sanghal et al Lancet 2013
Vertebral Compression fracture: Pathophysiology
Success of SRS in spinal mets will depend upon future research on management of VCF & myelitis
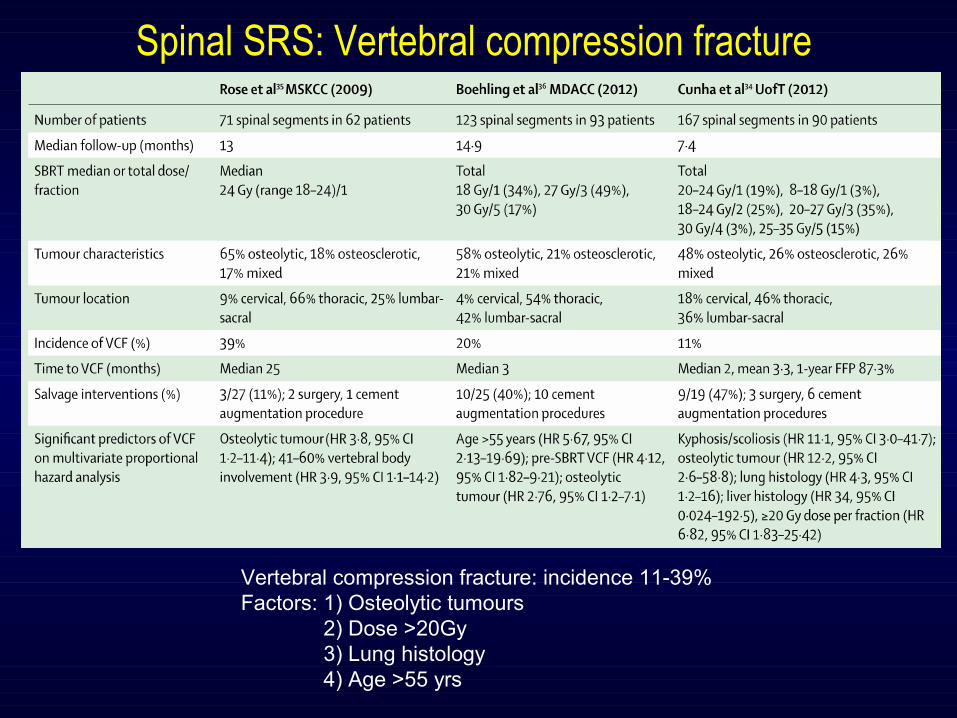
Spinal SRS: Vertebral compression fracture
Vertebral compression fracture: incidence 11-39% Factors: 1) Osteolytic tumours 2) Dose >20Gy 3) Lung histology 4) Age >55 yrs
Spinal SRS: Myelitis
•1996 and 2005 (n=1075) benign or malignant spinal
tumors were treated by CK.
•Six pts developed delayed myelopathy at a mean of 6.3
months after spinal SRS
• Three tumors were metastatic; 3 were benign.
•Three cases involved previous radiation therapy.
•Pts with myelopathy received spinal cord biological
equivalent doses >8 Gy.
Gibbs IC et al; Neurosurgery. 2009
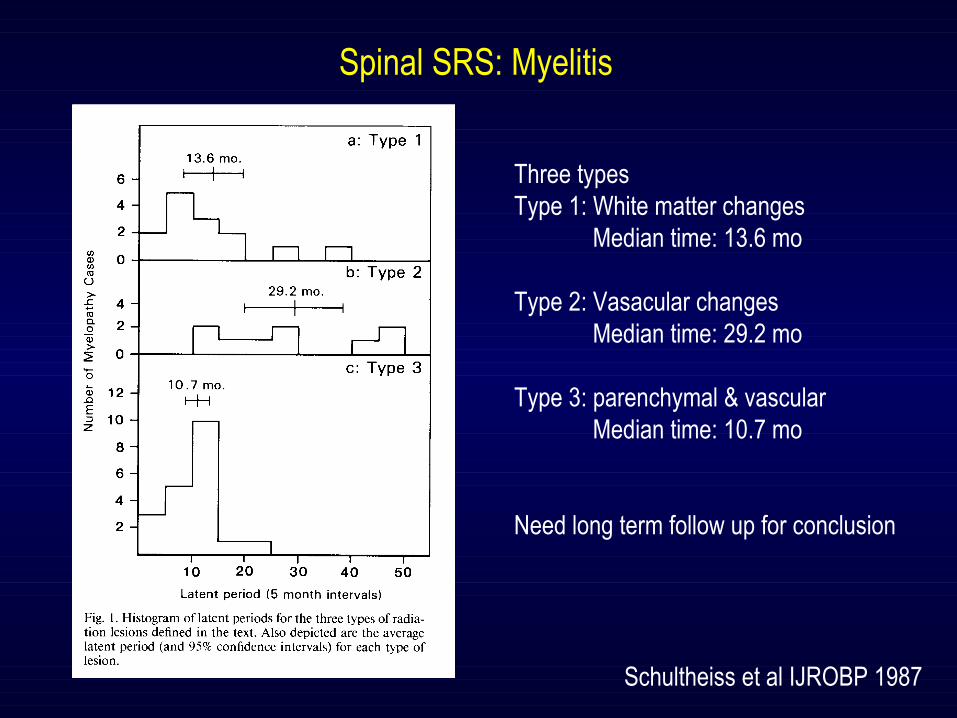
Schultheiss et al IJROBP 1987
Spinal SRS: Myelitis
Three typesType 1: White matter changes Median time: 13.6 mo
Type 2: Vasacular changes Median time: 29.2 mo
Type 3: parenchymal & vascular Median time: 10.7 mo
Need long term follow up for conclusion
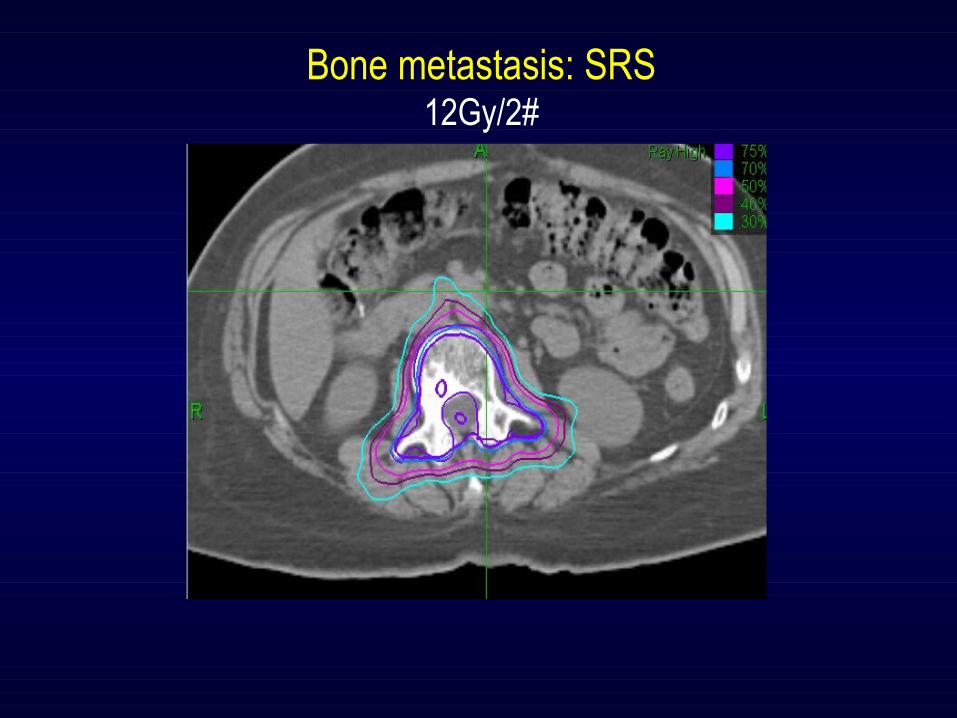
Bone metastasis: SRS12Gy/2#
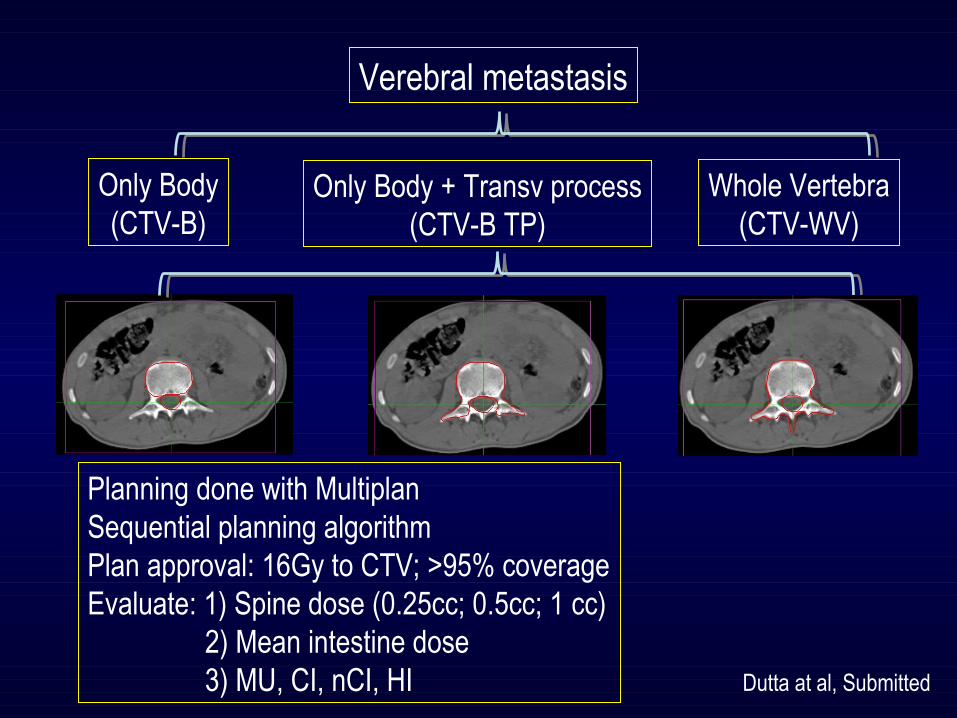
Verebral metastasis
Only Body(CTV-B)
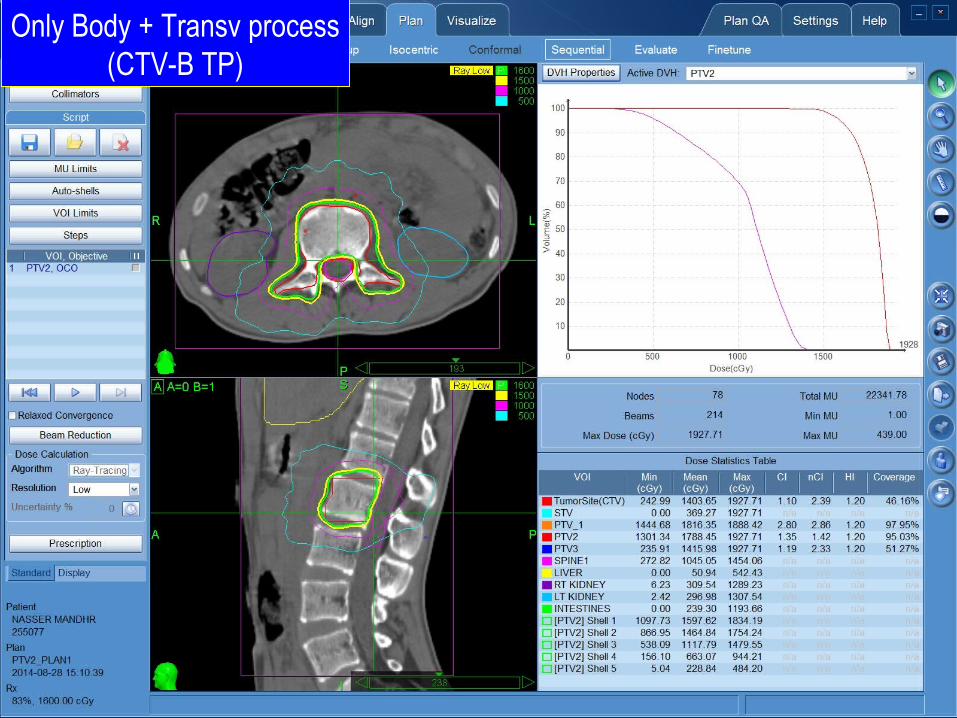
Only Body + Transv process(CTV-B TP)
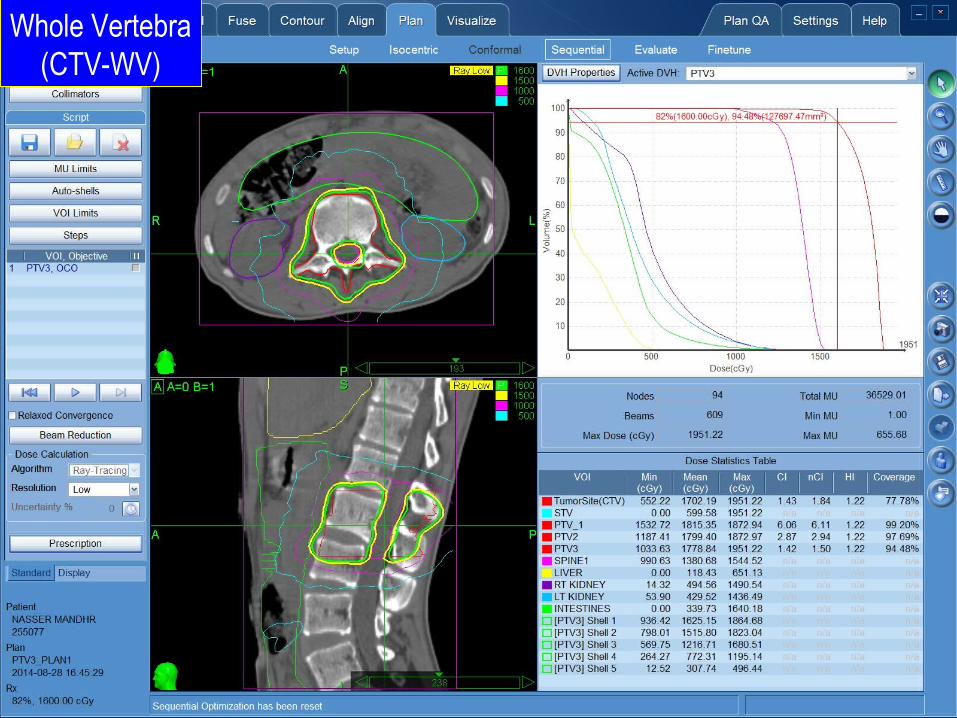
Whole Vertebra(CTV-WV)
Planning done with MultiplanSequential planning algorithmPlan approval: 16Gy to CTV; >95% coverageEvaluate: 1) Spine dose (0.25cc; 0.5cc; 1 cc) 2) Mean intestine dose 3) MU, CI, nCI, HI Dutta at al, Submitted
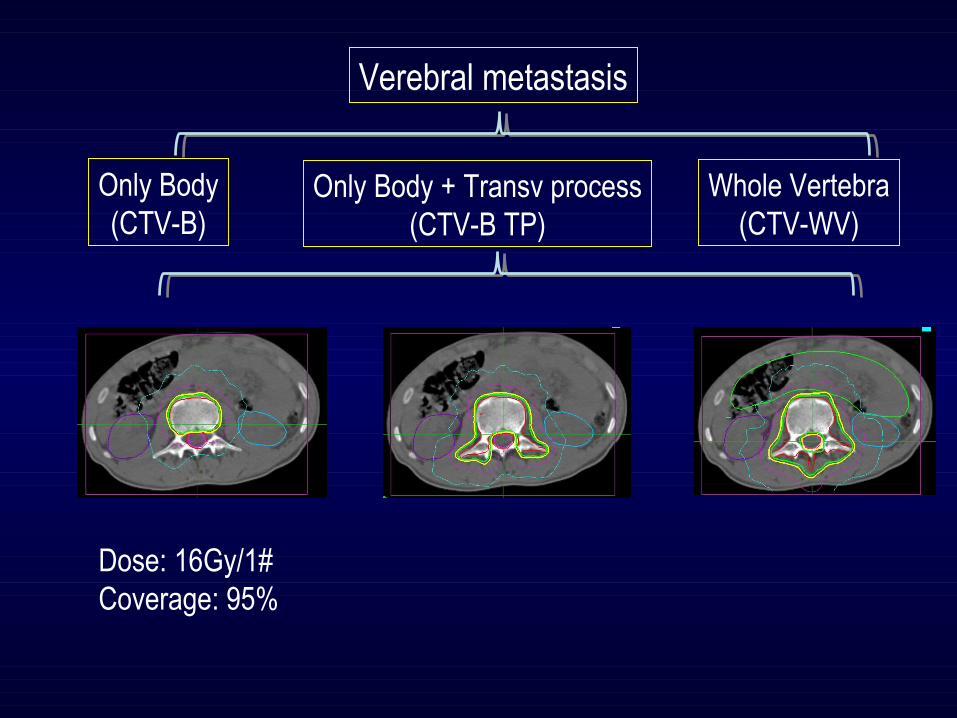
Verebral metastasis
Only Body(CTV-B)
Only Body + Transv process(CTV-B TP)
Whole Vertebra(CTV-WV)
Dose: 16Gy/1#Coverage: 95%

Only Body(CTV-B)
Only Body + Transv process(CTV-B TP)
Whole Vertebra(CTV-WV)
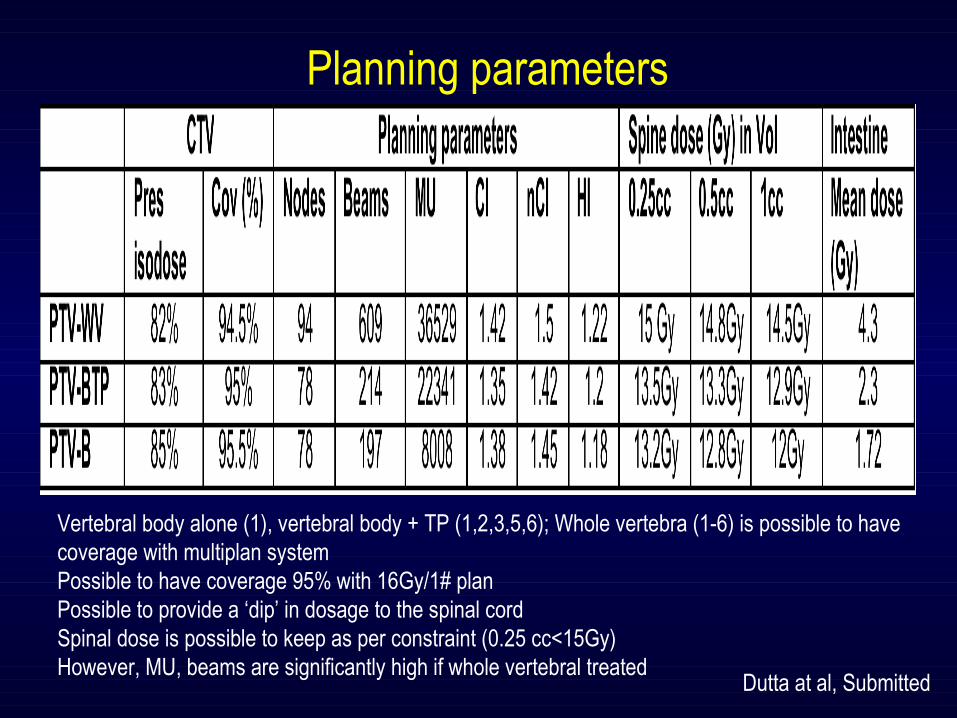
Planning parameters
Vertebral body alone (1), vertebral body + TP (1,2,3,5,6); Whole vertebra (1-6) is possible to have coverage with multiplan systemPossible to have coverage 95% with 16Gy/1# planPossible to provide a ‘dip’ in dosage to the spinal cordSpinal dose is possible to keep as per constraint (0.25 cc<15Gy)However, MU, beams are significantly high if whole vertebral treated
Dutta at al, Submitted
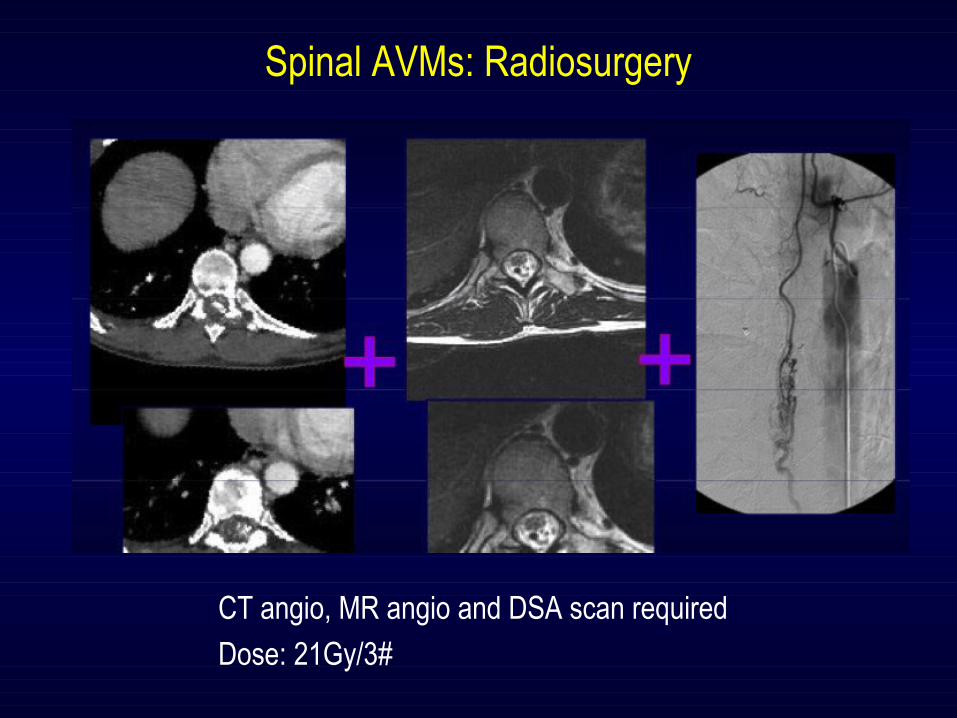
Spinal AVMs: Radiosurgery
CT angio, MR angio and DSA scan required
Dose: 21Gy/3#
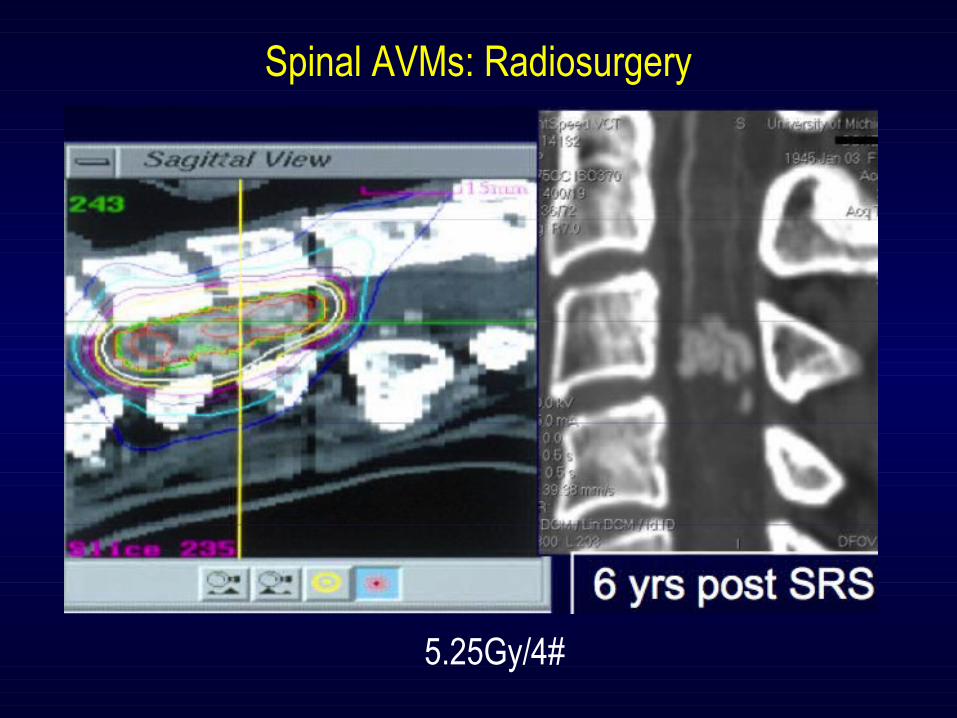
Spinal AVMs: Radiosurgery
5.25Gy/4#
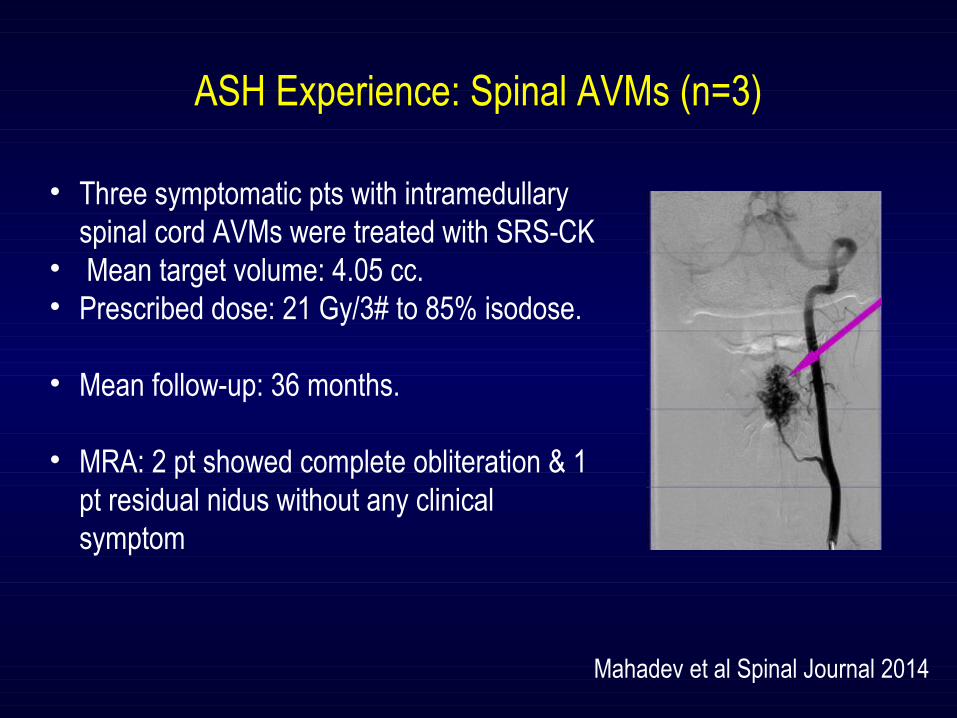
ASH Experience: Spinal AVMs (n=3)
Mahadev et al Spinal Journal 2014
• Three symptomatic pts with intramedullary spinal cord AVMs were treated with SRS-CK
• Mean target volume: 4.05 cc. • Prescribed dose: 21 Gy/3# to 85% isodose.
• Mean follow-up: 36 months.
• MRA: 2 pt showed complete obliteration & 1 pt residual nidus without any clinical symptom
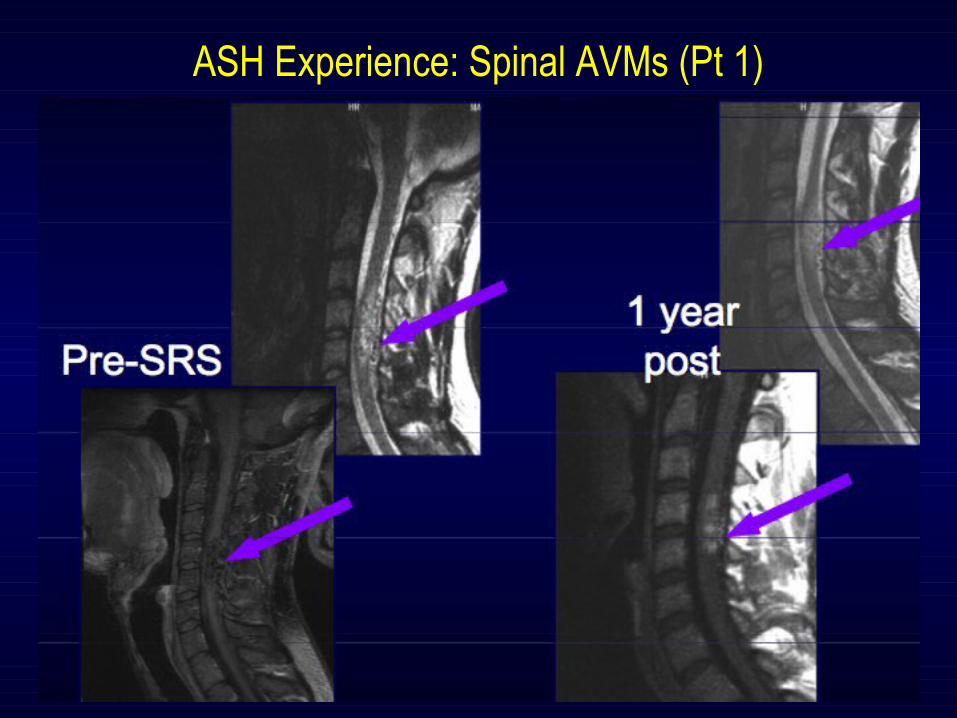
ASH Experience: Spinal AVMs (Pt 1)
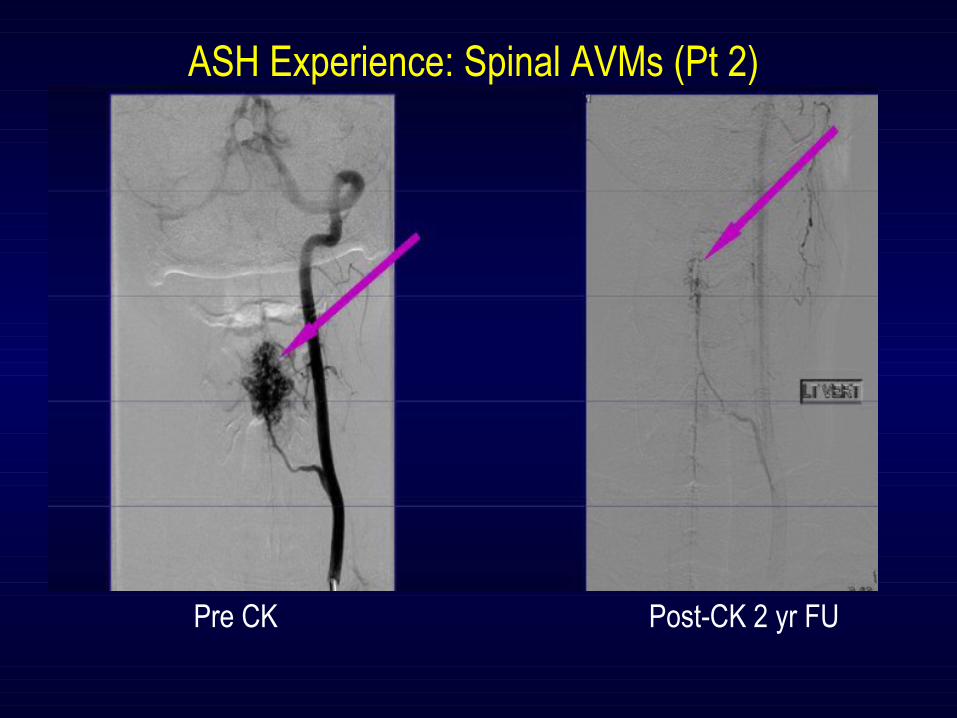
Pre CK Post-CK 2 yr FU
ASH Experience: Spinal AVMs (Pt 2)
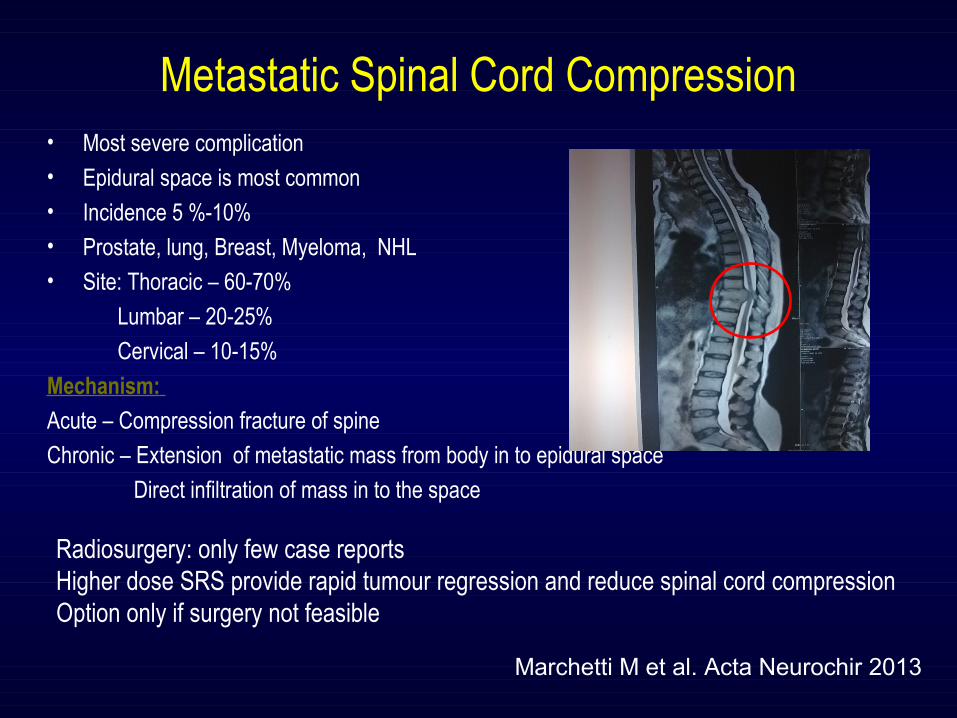
Metastatic Spinal Cord Compression• Most severe complication• Epidural space is most common• Incidence 5 %-10% • Prostate, lung, Breast, Myeloma, NHL • Site: Thoracic – 60-70%
Lumbar – 20-25%
Cervical – 10-15%
Mechanism:
Acute – Compression fracture of spine
Chronic – Extension of metastatic mass from body in to epidural space
Direct infiltration of mass in to the space
Marchetti M et al. Acta Neurochir 2013
Radiosurgery: only few case reportsHigher dose SRS provide rapid tumour regression and reduce spinal cord compressionOption only if surgery not feasible
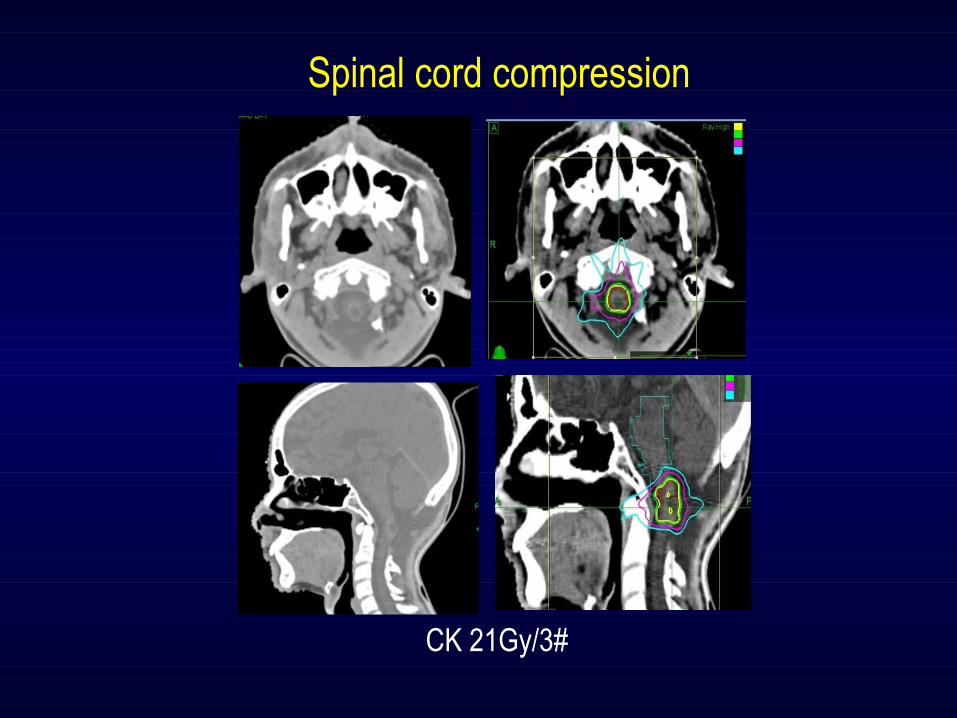
Spinal cord compression
CK 21Gy/3#
Take home message
High dose SRS is NOT yet the standard of care in spinal lesionsHowever, early data is promisingHigher dose may have longer pain control
RTOG 0631 Ph III study will provide us level I evidence, but need long term follow up
High dose SRS for vertebral body mets only in ‘oligo’ metsSlow growing tumours: Thyroid, sarcoma, RCCContouring of vertebra: as per guidelineContouring is critical as ‘rapid dose fall off”PTV margin <3mmDose: 16Gy to >90% coverageSpine dose is the constraint
CVF & myelitis is the main complications and should inform pts
Conclusions - SRS for solitary & ‘Oligo’ Vertebral metastasis in a reality. Ph II studies have shown
significant benefit with higher dose SRS in terms of pain control, requirement of re-RT- Ph III studies with 400+ patients with high dose SRS (16Gy), initial results are
promising and shows positive outcome- However, high dose SRS is also associated with high incidence of myelitis & vertebral
fracture
- Spinal metastasis & spinal cord compression, where surgery is morbid SRS reduces
the tumour mass and hence compressive symptoms
- Primary spinal cord tumours (ependymoma, PXA, Pilocytic astrocytoma): role of SRS
is not yet defined and hence should be done only in investigational situation- Spinal AVMs: SRS is the treatment of choice
- There is no ‘head to head’ comparative study of different RT delivery machines