Embed Size (px)
Citation preview

CHILDHOOD DIABETES
BYDR.AKINBI
OLUBAYODE.O

DEFINATION
Diabetes mellitus - a chronic metabolic disorder of multiple aetiologies characterized by chronic hyperglcemia with disturbances of CHO, fat & protein metabolism resulting from defects in insulin secretion, action or both.

EPIDEMIOLOGY Most common endocrine-metabolic
disease in childhood and adolescents Incidence of diabetes is alarming and
increasing all over the globe Incidence of childhood diabetes ranges
from 3-50/100,000 worldwide.

DIAGNOSTIC CRITERIA THE A1C TEST-6.5% means diabetes-5-7-5.99% means prediabetes-less than 5.7% means normal THE FPG( fasting plasma glucose test)-126mg/dl means diabetes-100 – 125.99mg/dl means prediabetes-less than 100mg/dl means normal

DIAGNOSTIC CRITERIA THE OGTT ( oral glucose tolerance test)-200mg/dl means diabetes-140 -199,9mg/dl means prediabetesLess than 140mg/dl means normal


CLASSIFICATION T1DM. - Most common type of DM in C &
adolescents accounts for 90% of cases. Epidemic of T2DM now being observed in
most societies around the world. (↑obesity, ↑cal diet, sedentary life style)
Permanent neonatal diabetes Transient neonatal diabetes Maturity-onset diabetes of the young Secondary diabetes e.g, cystic fibrosis,
cushing syndrome

MODY Uncommon but distinct entity Presentation < 25yrs, often teenager Ass. with mutations of glucokinase gene
in chromosome 7 Not associated with immunologic or
genetic markers Insulin resistance is present

TRANSIENT NEONATAL DIABETES
Observe in both term and preterm babies, but more common in preterm.
Caused by immaturity of islet of β-cells Polyuria & dehydration are prominent,
but baby looks well and suck vigorously Highly sensitive to insulin Disappears in 4-6 weeks

PERMANENT NEONATAL DIABETES
A familial form of diabetes that appear shortly after birth and continue for life
The usual genetic and immunologic markers of type 1 diabetes are absent
Insulin requiring, but ketosis resistant Is often associated with other congenital
anomalies and syndromes e.g, walcott-Rallison syndrome

TYPE 2DIABETES Previously known as Adult-onset, NIDDM,
MODY Usually obese;↑ incidence because of↑
childhood obesity Not Insulin-Dependent (except during
stress etc for symptomatic hyperglycemia)
Not ketosis-prone (severe infectns, stress Insidious presentation usually- (routine
medical exam or for other problems

TYPE 2 DIABETES Minority of all DM pts in paediatric years
(10-20%) Inherited nature – stronger than T1DM Concordance for identical twins - >ter
(80-90%) No known HLA or ass. with autoimm
markers or dx.

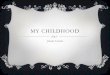
Hyperglycemia
Metabolic Defects in Type 2 Diabetes
Pancreas
Liver Muscle and Adipose
Hepatic Glucose Insulin Production - Resistance Glucose
Uptake Insulin
Resistance -
Progressive Insulin Secretory Defect

SCREENING FOR TYPE2 DM IN CHILDREN
Criteria: overweight (BMI > 85th %ile for age and sex,
weight for height > 85th %ile, or weight > 120% of ideal for height)
Plus any two of the following risk factors:

RISK FACTORS FOR TYPE 2• family history of type 2 diabetes in first- or
second-degree relative• race/ethnicity (American Indian, African-
American, Hispanic, Asian/Pacific Islander)• signs of insulin resistance (acanthosis
nigricans, hypertension, dyslipidemia, polycystic ovary syndrome

MANAGEMENT OF TYPE2 DM
Cornerstone - Modify diet ↑dly exercise Pharmacologic tx if BG is frequently
>200mg/dl, HbA1c > 8% Sulphonylurea- ↑ Insulin secretion
(cheap, convenient & effective in 3-7 days)
SE- refraction, hypoglcemia

MANAGEMENT OF TYPE2 DM
Metformin (glucophage) – biguanide -Now 1st line for T2DM -Mechanism- not fully known but 1oly
↓hepatic glucose production -SE- GIT symptoms, lactic acidosis -CI- liver, renal failure, metabolic acidosis

MANAGEMENT OF TYPE2 DM
Thiazolinediones- ↓peripheral insulin resistance in muscle & fat
Glucosidase inhibitors- competitive inhibitors of enzymes on intestinal brush border. Hence limit CHO absorption & minimize post prandial hyperglycemia

TYPE 1 DIABETES Autoimmune destruction of the beta cells
of the pancreas Insulin deficiency Insulin is necessary for survival
Diabetic Ketoacidosis (DKA) Usually an acute onset

TYPE 1 DIABETES Accounts for > 90% of Childhood &
Adolescent DM. 3-50/100,000 C < 15yrs dev T1DM annually
with wide global variations in incidence Whites of N. European descent more likely
than Blacks, Asians. Can manifest at any age (approx 50% at >
18yrs) Bimodal peak age distribution: 5-7yrs &
puberty Worldwide↑ in No of young C being
diagnosed with T1DM especially in ↓ 5yrs

RISK FACTOR FOR TYPE1 Chronic Autoimmune dx – vast majority
(HLA DR3 & 4, B8,BW15 on chr 6) T-cell mediated autoimmune destruction
of pancreatic β-cells in genetically predisposed C. (Islet AB, Insulin AB)
Idiopathic - few

RISK FACTOR FOR TYPE1 Siblings 5-6%, Mother 3-4%, Father 6%,
5-10% both parents, Monozygotic twins 30-40%, general population 0.4%
Seasonal factors-new cases > in winter/autumn

PATHOPHYSIOLOGY OF TYPE 1 Insulinopenia→↓ glucose utiliztn (muscle, fat)
→post prandial hyperglcemia, at lower Insulin levels→ ↑hepatic glycogenolysis/ gluconeogenesis → fasting hyperglycemia → osmotic diuresis
→ glucosuria (> renal threshold-180mg /dl-10mM/L→calorie & E- loss →dehydratn

PATHOPHYSIOLOGY OF TYPE 1 →physiological stress →↑epinephrine,
cortisol, GH, glucagon→ worsens metabolic decompensation→↑ lipolysis & impaired lipid synthesis → ↑FFA, cholest, TGA → ketones- (βOH butyrate, acetoacetate, acetone) →buffer depleted →metabolic acidosis (DKA) –Kussmaul resp- deep, rapid resp to excrete excess CO2
→ ketonuria → ↑ H2O & E-loss →hyper osmolality
→dec cerebral O2 use →impaired consc, coma

MANAGEMENT Dreadful disease, requires team support:
paediatrician, nurse educator, dietician, mental health professional, social worker, peer discussion group, summer camps, role models, support groups
Aims of therapy: Provide N growth, puberty, psychomotor
development & well being Exercise is an integral component of
growth & dev. No sport is excluded.

MANAGEMENT Nutrition- 1 of cornerstone of mx No sp nutrition required other than for
optimal growth & dev. Same food type as for gen populatn
Regular eating pattern for Insulin regimen Individual nutritional reqment & meal
plan based on age, sex, wt, activity, preferences

MANAGEMENT Meal plan: 50% CHO- 70% as Complex eg
starch to prolong digestion & absorption for slow rise of BG
Avoid refined sugars, give high fiber diet eg veg, legumes, whole-meal bread, cereals diet & sugar- free carbonated drinks,
Lipids-30%- limit cholesterol; poly :unsat ≥2:1 –fat from plant( marg, veg oil to reduce LDL & cholest
20% protein (plant)- limit egg-yolk, give fish poultry, lean-cut meat

MANAGEMENT BG target: fasting/ preprandial – 70-
130mg/dl After meals < 180mg/dl Night: not < 60mg/dl (early morning
headache- suggestive of hypoglycemia in the night)

INSULIN Insulin is a hormone produced in the beta
cells of the Islets of Langerhans in the pancreas
FUNCTION: To allow glucose to pass into the cell To decrease physiological production of
glucose by the liver and muscle To turn off ketone production.

INSULIN Insulin: replacement required in T1DM,
even the small no of T2D are usually txed Wide variations in regimen Single dly injection (intermediate –
acting) rarely successful Multiple dly injections or continuous s/c
infusions – offers flexibility

TYPES OF INSULIN Rapid Acting:
Insulin lispro (Humalog) ® Insulin aspart (Novolog) ® Insulin glulisine (Apidra) ®
Short-acting: regular
Intermediate-acting: NPH (Neutral Protamine Hagedorn)
Long-acting: Insulin glargine (Lantus) ® Insulin detemir (Levemir

INSULIN ADMINISTRATION
Syringes: short needle, mixing insulins Pen injectors: flexibility Insulin Pumps; Continuous subcutaneous
insulin infusion (CSII) devices Insulin to Carbohydrate ratio
Unit: Grams of CHO Example: 1 unit : 15 grams of CHO

OUT-PATIENT MANAGEMENT
Goals Stabilize BG within target range Avoid metabolic decompensatn (DKA,
hypoglycemia) Ensure N growth & dev- physical &
emotnal Prevent long-term complicatn Preprandial BG- 80-120mg/dl 2hr pp < 180mg/dl Bedtime- 100-140mg/dl HbA1c within 1% of high normal for
method used

COMPLICATIONS OF DIABETES Macrovascular
Heart and blood vessels: High cholesterol Hypertension Atherosclerosis
Microvascular Retinopathy Nephropathy NeuropathyOthersKetoacidosis , infections, stroke, etc

THANK YOUMCI
www.mediconsultinitiative.com