Embed Size (px)
DESCRIPTION
Citation preview

Community Health Workers – Overcoming Scalability Challenges
The Rwanda Expanded Impact Child Survival Project Experience
Presented by:Jennifer Weiss, MPH
Health Advisor, Concern WorldwideCORE Fall Meeting 2011

Project Overview
• Implemented from 2007 – 2011 in six districts in Rwanda
• Target population: 300,000 children under five
• Technical interventions: malaria, diarrhea, pneumonia

Project OverviewGoal: Reduce child mortality in six districts in Rwanda
Objective 1: Increase
access to first line treatment
Objective 2: Increase
coverage of preventative interventions
Objective 3: Increase
adoption of key family health
practices
Illustrative Activities:
• Expand CCM• Strengthen
service delivery (QI)
Illustrative Activities:
• Support health communication campaigns and National Health days
Illustrative Activities:
• Community mobilization
• Adapted Care Group model
Integrated Nutrition - CMAM

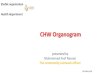
Rwanda MOH Community Health StructureDistrict Hospital: Community Health Supervisor
Health Facility: In-Charge of Community Health
CHW Cooperative and Cell-Coordinators
Village Level: 2 ‘binomes’ for c-IMI; 1 CHW for Maternal Health, and 1 Social Affairs Officer

40-80 Villages
Cell
Cell coordinator
In-charge Community Health
1 hour to 1 day walk
Existing Supervision and Reporting Structures
Sector

Opportunities for Improvement
• MOH has clearly defined Community Health structure that includes CHWs
• CHWs are officially recognized in the community, motivated, and provided incentives (Cooperatives)
• But …– Not well geared towards effective behavior change– Challenging reporting and supervision structures

Rwanda EIP Response (as it evolved)
World Relief CSP (2001-2006) used Care Group Model
WR began to incorporate Care Groups into EIP
(2007) under Community Mobilization activities
Rwanda MOH requirements on
limited number of CHWs per village
(2008)
15-20 member “Peer Support and
Collaboration Groups” formed
with 4 CHWs from each village (2009
– 2011)
CHW peer support groups no longer fit Care Group criteria but still maintains group solidarity, and responsibility for HH visits and behavior change

EIP Community Health Structure
In-Charge Community Health
Cell Coordinator
CHW Group
CHW Group
CHW Group
CHW Group

Outputs
• 660 peer support groups formed with 13,166 CHWs in 6 districts
• Average of 163,000 households visited on a monthly basis with key prevention messages

Results
• CHW Peer Support Group activities associated with:– Four-fold increase in the
number of households with kitchen gardens
– Twenty-five fold increase in the number of households with hand washing stations

Results• Statistically significant
increases in key behavior change indicators:– Hand washing – Point of use water treatment– Care seeking for and access
to malaria and pneumonia treatment
– Immunization, and Vitamin A
• Even with main project focus on CMM!

Outcomes – Supervision and Reporting
• Peer supervision helped to compensate for health facility staff challenges (HR, transport)
• Monthly meetings provided opportunity for facilitated supervision from In-Charge Community Health or Cell Coordinator
• Reporting burden on Cell Coordinator greatly reduced

Outcomes – CHW Activities
• Provided CHWs with greater social support (small groups vs. large cooperatives)
• Groups perceived as motivating factor– IGAs
• Home visits provided mechanism for BCC that previously did not exist
• Home visits also increased contact with families and provided opportunities for referrals and follow-up CCM care

Outcomes – Integration with MOH
• MOH stakeholders, CHWs, and beneficiaries viewed CHW peer support model as part of MOH-endorsed, cell-level CHW Cooperative structure at a smaller scale

Conclusions• CHWs working as group:– Provide greater peer support through social cohesion– Encourage joint problem solving– (In Rwanda), provide mechanism for BCC and home
visits that would not exist otherwise• Scale – working at district level first, in
collaboration with TWGs – Decentralization – districts chose to adopt– Transition to country ownership
• Sub-group cooperatives for IGAs that look very similar to “CHW peer support groups”?

Conclusions
• The CHW Peer Supervision Model provides a scalable model for meaningful engagement of CHWs at the village level - where it counts!