Embed Size (px)
Citation preview

By- Dr. Armaan SinghBy- Dr. Armaan Singh
Clinical Anatomy of the Back

PROGRESS
TimeTime
Goh et al. Clin Biomech 1999;14:439

SPINEConsists of
• Cervical Vertebrae
• Thoracic Vertebrae
• Lumbar Vertebrae
• Sacrum

• The strength of the skeletal column is due to the size and shape of the vertebrae
• Its flexibility is due to the many joints that are close together
Spine

VERTEBRAL COLUMN• Lot of stress in variety of sports
• Cervical pathology
• Pain may be referred to upper limb
• Lumber pathology
• Lower limb

YOUNG SPINE
Normal curvature of infant’s spine
Normal lumbar curve of toddler’s spine

LOW BACK PAIN IN SPORTS• 70% of population will suffer from back pain
at some time
• 10% - 15% of sports injuries are spinal injuries
• 0.6% - 1% have neurological complications
Deyo & Tsui-Wu. Spine 1987;12:264-8

• Majority of sports injuries to lumbar spine
• Soft tissue and many are not reported
• Fractures
• Fracture dislocation
• Abrasions, bruising
• Contusions
Tall & De Vault. Clin Sports Med 1993;12:441-8
Low Back Pain in Sports

• Must know the sport
• Must understand the biomechanics and stresses involved in the sport
• Must examine the spine in the appropriate position
Low Back Pain in Sports

TYPICAL VERTEBRAE• Basic parts
• Body and neural arch
• Which consists of pedicles, lamina and spine
• The transverse processes arise from the pedicles
• Superior and inferior articular processes

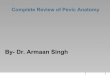
LUMBAR VERTEBRAE

LUMBAR VERTEBRAE• Body kidney shaped
• No articular facets for ribs
• Inferior facets face anterolateral
• Superior facets face posteromedial
• Intervertebral notch increase in size
• Accessory processes base of transverse process
• Mammillary process on posterior aspect of superior articular process

LUMBAR VERTEBRAE• Body is convex anteriorly
• Foramina on the posterior aspect are for the basic vertebral veins, which drain into the internal vertebral plexus
• The walls of the veins, which are valve less, have afferent nerve fibers
• Secondaries can spread from pelvis, prostate, adrenal glands lungs and breast

• The superior and inferior surfaces of the body are flat and covered by a thin layer of hyaline cartilage
• The body of the vertebra consists of trabecular or cancellous bone
Lumbar Vertebrae

TYPICAL LUMBAR VERTEBRAE• Superior and inferior articular
processes
• Arise from the junction of the pedicles and lamina
• Superior face posteromedially
• With rough mammillary processes on the posterior border
• Inferior face anterolaterally
• Accessory processes at the base of transverse process
• Prevents rotation

THE LUMBAR FACETS• Vary from the sagittal disposition at the first
and second, to almost coronal in the lower
• Facet tropism is when the facet on one side is in the sagittal plane and the other is in the coronal plane, which adds to rotational stress
• This change may occur in the lower thoracic vertebrae

PARS INTERARTICULARIS• Pars interarticularis
• Portion of lamina between superior and inferior articular processes
• Site of spondylolysis or spondylolisthesis

LUMBAR SPINE• Cancellous bone
• 50% compressive strength
• Facet joints 20% in standing upright position

LUMBAR VERTEBRAE

LUMBAR VERTEBRAE

LUMBAR SPINE• Cancellous bone
• 50% of the compressive
strength
• Facet joints, 20% of the strength in the standing upright position

ANTERIOR LONGITUDINAL LIGAMENT• Attached mainly to the bodies
• This ligament helps to prevent us from leaning too far back (hyperextension)

POSTERIOR LONGITUDINAL LIGAMENT• Attached mainly to the inter
vertebral discs
• This ligament helps to restrict forward bending (hyperflexion)

LIGAMENTUM FLAVA• Runs between the laminae
of the neural arches
• Helps to restrict hyperflexion
• It extends to the capsule of the facet joint
• It is highly elastic and ensures that the ligament does not buckle in extension

• Gives elasticity to the posterior aspect of the facet joints
• Helps form the posterior boundary of the intervertebral foramen
• The ligamentum flava is thicker in the lumbar region
Ligamentum Flava

SPINAL LIGAMENTS• Interspinous ligaments
• Strong supraspinous ligaments
• The inter-transverse ligaments join the transverse processes and are thin and membranous in the lumbar region

FIFTH LUMBAR VERTEBRAE• Larger, superior and inferior articular
facets in the same plane
• Fifth lumbar vertebrae has large transverse processes
• Arise from the body as well as the pedicles

ARTHRITIS OF SPINE• Painful
• Limitation of movement
• Extra projections
• Narrowing of disc spaces

VERTEBRAL JOINTS• Secondary cartilaginous joints between
the bodies
• Hyaline cartilage covering bodies
• Disc of fibrocartilage in between
• Synovial plane joints between the facets

INTERVERTEBRAL DISCS• Annulus fibrosis
• Concentric lamina run obliquely
• Type I collagen at periphery, type II near nucleus
• Weakest portion is the postero-lateral and posterior
• Periphery has a nerve supply

NUCLEUS PULPOSUS• Gelatinous, hydrophilic, proteoglycan gel in
collagen matrix
• Lies posterior in the disc
• There are no nerve endings in a mature disc
• Nerve endings are found in the posterior longitudinal ligament and the dura
• Nutrition of the disc is by diffusion via the central 40% of the cartilaginous end plate
• The discs are thicker in the cervical and lumbar sections of the vertebral column
• Where there is more movement. The largest disc is between L5 S1

NUCLEUS PULPOSUS• Hydration of the annulus and nucleus is
proportional to the applied compressional stress
• In vivo, there is a loss of 1 cm standing height over the course of the day
• A disc loaded in vitro for four hours by 100% body weight will lose 6% of the fluid from the nucleus and 13% from the annulus
• May be due to end plate fracture
• There is more rotational stress in the posterior part of the disc

NUCLEUS PULPOSUS• The position of the spine determines
where the compressional forces are greatest
• The posterior longitudinal ligament is thin and expanded at the level of the disc
• High compressional loading at L4,L5,S1 may be due to end platefracture and not to rupture of the annulus
• End plate failure is a possible precursor of disc degeneration

AXIAL LOAD AND END-PLATES

END-PLATE MECHANICS • Functionally, the vertebral end-plate
displays characteristics of a trampoline
• With the sub-end-plate trabecularbone acting as springs to sustainand dissipate axial load
• Despite the thinness of the vertebral end-plate
• The hydraulic nature of marrow and blood vessels within the vertebral body, act to dampen axial loads, unless the local point pressure is too high

END-PLATE MECHANICS • End-plate lesions can be induced experimentally
before a disc will prolapse through the anulus, suggesting a protective mechanism over annular injury and potentially cord or root compression
• Excessive loads may result in perforation of the end-plate, usually in the region of the nucleus and often in the path of the developmental notchord

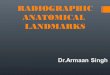
END-PLATE SUSCEPTIBILITY
Schmorl & Junghanns. The human spine in health and disease. New York: Grune & Stratton, 1965
Notochord

FACET JOINTS• L1,L2 Facets sagittal plane
• Lower joints in coronal plane
• Synovial plane joints
• Meniscoid structures
• Synovial membrane some contain fat
• Supplied by medial branch of dorsal ramus

• Narrowing of disc space, results in stress on facet joint
• Highest pressure during
• Combined
• Extension
• Rotation
• Compression
Facet Joints

FACET JOINT SYNDROME• Extension and rotation
• Pain rising from flexion
• Pain worse standing
• Lateral shift in extension
• Point tenderness over facet
• Referred leg pain

SEGMENTAL ROTATION
Singer et al. J Musculoskel Res 2001;5: 45-55

• Flexion limited by disc problems
• Lateral flexion
• Extension limited by facet joint problems
• Very little rotation
• Extension and rotation affect facet joints
MOVEMENTS OF LUMBAR SPINE

NERVE SUPPLY• Nerve supply
• Peripheral annulus
• Facet joint
• Nerve is medial branch dorsal ramus

BLOOD SUPPLY• Lumbar arteries
• Internal venous plexuses
• External venous plexuses
• Basivertebral veins
• Valveless

LUMBAR VERTEBRAE

CANCELLOUS BONE• Cancellous bone
• 50% compressive strength
• Facet joints 20% in standing upright position
Normal bone Osteoporotic bone

ANATOMICAL ABNORMALITIES• Spina Bifida Occulta
• Facet Tropism
• Kyphosis
• Scoliosis

ANATOMICAL ABNORMALITIES
Kyphosis Scoliosis

ANATOMICAL ABNORMALITIES• Hemi-vertebra
• Spina Bifida Occulta
• Facet Tropism
• Scoliosis
• Kyphosis

ANATOMICAL ABNORMALITIES• Unilateral lumbarisation
• Unilateral sacralisation

THE SPINE IN SPORTS• Spine injury epidemiology
• Contact vs. non-contact sports
• Spine injury mechanisms
• Overuse – overload – overlooked
• Vertebral end-plate injury
• Disc injury
• Future issues

EPIDEMIOLOGY
Cooke & Lutz. Phys Med Rehab Clinics N Am 2000;11:837

Cooke & Lutz. Phys Med Rehab Clinics N Am 2000;11:837-65
EPIDEMIOLOGY• Back pain in the community is 60% - 80%
• Recurrence of back pain is70% - 90%
• Progression to chronic back pain is 5% - 10%

LOW BACK PAIN IN SPORTS• Majority of sports injuries are to the
lumbar spine
• Many soft tissue injuries are not reported
• Fractures
• Fracture dislocation
• Abrasions, bruising
• Contusions
Tall & De Vault. Clin Sports Med 1993;12:441-8

CHRONIC LOW BACK PAIN• Local structures
• Muscles
• Ligaments
• Poor lifting techniques
• Joints
• Bones

BACK PAINLocal structures
• Muscles, ligaments
• Joints
Referred pain
• Abdominal organs
• Pelvic organs
Must out rule
• Infection
• Tumours

ACUTE LOW BACK PAIN• Non-specific low back pain
• Usually settles quickly
• History
• Examination
• Pain relief
• Stay as active as possible within limit of pain

ACUTE LOW BACK PAIN• Nerve root pain
• Leg pain worse than back pain
• Numbness and pins and needles
• Neurological signs
• Refer to specialist
• If it does not resolve in first 4 weeks

INVESTIGATE LOW BACK PAIN• Under 20 or over 55 years
• Non-mechanical pain
• Past history cancer
• Thoracic pain
• Steroids or HIV
• Unwell, weight loss
• Widespread neurology
• Structural deformity
• Gait disturbance or sphincter disturbance

CHRONIC LOW BACK PAINPain referred
• Abdominal organs
• Pelvic organs
Must out rule
• Infection
• Tumours

PAIN REFERRED

YOUNG ATHLETE• Junior rugby team 15 years of age
• M. Scheuermann
• 5 Spina bifida occulta
• The scrum half had degenerative facet joint changes

SACROILIAC JOINT – SCIATIC NERVE

SPINAL STENOSIS• Congenital or acquired
• Abnormally short pedicles or lamina
• Formation of osteophytes
• Osteo-arthritis of facet joints
• Pain aggravated by walking
• Relieved by rest

SPINAL STENOSIS

PREDISPOSING FACTORS• Intrinsic factors
• Anatomical abnormalities
• Biomechanical
• Extrinsic factors
• Sport
• Surfaces
• Equipment
• Training

PREDISPOSING FACTORS BACK PAIN• Poor posture
• Overweight
• Unfit

PREDISPOSING FACTORS• Poor core stability
• Weak abdominal muscles
• Weak gluteal muscles
• Muscle imbalance

PREDISPOSING FACTORS• Poor core stability
• Weak abdominal muscles
• Weak gluteal muscles
• Muscle imbalance
• Pronated or cavus feet

PREDISPOSING FACTORS• Badly designed furniture
• No back support
• Poor posture at work

ACUTE LOW BACK PAIN

ANNULAR TEARS• Loaded compression with rotatory
component
• As little as 3 degrees of high torque rotation
• Facets protect disc
• As annulus fails, facets joints may be injured

ANNULAR BULGE

DISC LESION

YOUNG ATHLETE• Junior rugby team 15 years of age
• M. Scheuermann
• 5 Spina bifida occulta
• The scrum half had degenerative facet joint changes

SCHEUERMANN’S DISEASE
Greene et al. J Pediatr Orthop 1985;5:1

SPONDYLOLISTHESIS

PARS INTERARTICULARIS• Pars interarticularis, portion of lamina
between superior and inferior articular processes
• Site of spondylolysis or spondylolisthesis

SPONDYLOLISTHESIS

SPONDYLOLYSIS AND SPONDYLOLISTHESIS

PARS INTERARTICULARIS; FACET JOINT

SPONDYLOLISTHESISRAPID FLEXION AND EXTENSION
• Gymnastics, flips
• Vaulting
• Ballet, arabesque
• Lifting during dance
• Diving
• Butterfly swimming
• Decathlon
• Pole vaulting

ANKYLOSING SPONDYLITIS, INFECTION

465 ATHLETES LOW BACK PAIN (M318;F147)
male (39) female(14)
Spina Bifida Occulta (SBO)
6.6%(21) 4.1%(6)
Lumbarisation
3.5%(11) 1.4%(2)
Sacralisation
2.2% (7) 6.1% (9)
Spondylolisthesis (13)
30% had SBO; 21 of 56 had other pathology

MECHANISM OF INJURIES• Compression or weight loading
• Torque or rotation
• Tensile stresses produced by excessive motion of spine
• Hyperextension and flexion
Watkins & Dillin, 1985

COMPRESSION OR WEIGHT LOADING• Sports requiring
• Massive strength
• High body weight
• Weight lifter
• Hooker and No 8
• Wrestling
• Line back American football
Watkins & Dillin, 1985

WEIGHT LIFTING• 40 % weight lifters have
low back pain
• Greatest stress is when weight is lifted above the head
• Dangerous time is shift from spinal flexion to extension
Aggrawal et al. Br J Sports Med 1979;13:58-61

AXIAL COMPRESSIVE LOADING• Head on collisions
• Motor sports
• Boating accidents
• Wrestling
• Horseback riding
• Bicycling
• Bobsleigh

AXIAL COMPRESSIVE LOADING

AXIAL COMPRESSIVE LOADING

AXIAL COMPRESSIVE LOADING

COMPRESSION STRESS

ROTATIONAL STRESS

ROTATIONAL STRESS

SPONDYLOLISTHESISRAPID FLEXION AND EXTENSION
• Gymnastics, flips
• Vaulting
• Ballet, arabesque
• Lifting during dance
• Diving
• Butterfly swimming
• Decathlon
• Pole vaulting

AUSTRALIAN FOOTBALL LEAGUE
Seward & Orchard. 2000 AFL Injury Report, Australian Sports Commission

GOLF• Highest incidence of back injuries in
professional sports
• Torsional stress is lessened by spreading the stress over the entire spine
• Rigid abdominal control
• Parallel shoulders and pelvis
Watkins and Dillin, 1985

SUSTAINED POSTURES - HYPEREXTENSION

SUSTAINED POSTURES - HYPEREXTENSION

SUSTAINED POSTURES - HYPEREXTENSION

SUSTAINED POSTURES - FLEXION

SCOLIOSIS DUE TO UNILATERAL SPORTS• Racquet sports
• Fencing
• Sweep rowing
• Javelin
• Freestyle unilateral breathing

SCOLIOSIS DUE TO UNILATERAL SPORTS

RUNNING• Poor posture
• Poor abdominal
• Pronated feet
• Muscle imbalance
• Leg length discrepancy
• Osteoporosis

CRICKET• Bowlers
• Rotational forces
• Extension followed by rotation and flexion