Embed Size (px)
Citation preview

Constipation in Infants Constipation in Infants & Children& ChildrenDr. Vivek RegeDr. Vivek Rege
Pediatric Surgeon & Pediatric UrologistPediatric Surgeon & Pediatric Urologist
BhatiaHospitalBhatiaHospital
Saifee HospitalSaifee Hospital
Fortis HospitalsFortis Hospitals
B J Wadia Hospital for ChildrenB J Wadia Hospital for Children

October 2010 Dr. Vivek Rege 2
Physiology of defecationPhysiology of defecationAt birth passage of meconium- 24 hours: 87%At birth passage of meconium- 24 hours: 87%
48 hours: 99%48 hours: 99%
Breast fed infants - up to 5 stools /day(whey)Breast fed infants - up to 5 stools /day(whey)
Cows milk fed -Cows milk fed - firmer stools (casein) firmer stools (casein)
Formula fed - fat content dependant*Formula fed - fat content dependant*
At 16 weeks – about 2 stools /dayAt 16 weeks – about 2 stools /day
Weaning at 4 – 6 months – firmer stoolsWeaning at 4 – 6 months – firmer stools
*PUFA- softer/frequent*PUFA- softer/frequent
Standard fat: firmer, less freqStandard fat: firmer, less freq

October 2010 Dr. Vivek Rege 3
Anatomy & ContinenceAnatomy & Continence• Internal anal sphincter – involuntaryInternal anal sphincter – involuntary• External anal sphincter – voluntaryExternal anal sphincter – voluntary• Continence is combination of Continence is combination of
- Sensation within rectum- Sensation within rectum
- Good motility of colon- Good motility of colon
- Good function of sphincters- Good function of sphincters

October 2010 Dr. Vivek Rege 4
Anatomy & ContinenceAnatomy & Continence
• Presence of feces in rectum causes a Presence of feces in rectum causes a decrease in tone of the internal sphincterdecrease in tone of the internal sphincter
• Urge to defecate triggered by stool in Urge to defecate triggered by stool in contact with mucosa of lower rectumcontact with mucosa of lower rectum
• If no wish to evacuate- tightens ext. sph If no wish to evacuate- tightens ext. sph & gluteal muscles& gluteal muscles
• Wants to evacuate- relaxes ext. sph Wants to evacuate- relaxes ext. sph allows passage of fecesallows passage of feces

October 2010 Dr. Vivek Rege 5
Chronic ConstipationChronic ConstipationOccurrence of 2 or more of the followingOccurrence of 2 or more of the following
(last 2 months>4 yrs; last 1 month<4 yrs)(last 2 months>4 yrs; last 1 month<4 yrs)• Frequency of bowel movements < 3 / weekFrequency of bowel movements < 3 / week• More than 1 episode of fecal incontinence / weekMore than 1 episode of fecal incontinence / week• Large volume of stool in rectum or palpable in Large volume of stool in rectum or palpable in
abdomenabdomen• Passing of large diameter stools – may obstruct toiletPassing of large diameter stools – may obstruct toilet• Display of retentive behavior: posturing, withholding Display of retentive behavior: posturing, withholding
maneuvers, on toes, cornersmaneuvers, on toes, corners• Painful defecationPainful defecation

October 2010 Dr. Vivek Rege 6
Fecal IncontinenceFecal IncontinencePassage of stool in an inappropriate placePassage of stool in an inappropriate place• Organic: due to organic disease: NeurologicalOrganic: due to organic disease: Neurological
Sphincter Sphincter • Functional : non organic disease:Functional : non organic disease:
* Constipation associated functional incont.* Constipation associated functional incont.
* Non retentive – incontinence in children> * Non retentive – incontinence in children> 4 yrs with no c/o constipation 4 yrs with no c/o constipation

October 2010 Dr. Vivek Rege 7
Fecal ImpactionFecal ImpactionLarge fecal mass in rectum or Large fecal mass in rectum or
abdomen – unlikely to be passed on abdomen – unlikely to be passed on demanddemand
Pelvic Floor DysynergiaPelvic Floor DysynergiaInability to relax pelvic floor when Inability to relax pelvic floor when
attempting to defecateattempting to defecate

October 2010 Dr. Vivek Rege 8
Pathophysiology of ConstipationPathophysiology of Constipation
• Repeated avoidance of defecation :Repeated avoidance of defecation :* Stretches the rectum* Stretches the rectum
* Decreases propulsive power * Decreases propulsive power
* Loss of sensory & motor function* Loss of sensory & motor function
• Longer feces remains in rectum – harder it becomesLonger feces remains in rectum – harder it becomes• Passage of hard & large stool – painful fissurePassage of hard & large stool – painful fissure• Cycle of avoiding bowel movement – fear of painCycle of avoiding bowel movement – fear of pain• Functional constipationFunctional constipation

October 2010 Dr. Vivek Rege 9
Pathophysiology of ConstipationPathophysiology of Constipation
• Self perpetuating & self aggravating diseaseSelf perpetuating & self aggravating disease• If not treated, allows larger & larger stool in If not treated, allows larger & larger stool in
rectosigmoid --- megasigmoidrectosigmoid --- megasigmoid• Dilatation of hollow organ produces poor peristalsisDilatation of hollow organ produces poor peristalsis• Passage of hard stools – pain & anal laceration – Passage of hard stools – pain & anal laceration –
reluctance to pass stool – constipation– fecal retention reluctance to pass stool – constipation– fecal retention – large hard stool – passage of hard stool– large hard stool – passage of hard stool

October 2010 Dr. Vivek Rege 10
Huge dilated Huge dilated SigmoidSigmoid

October 2010 Dr. Vivek Rege 11
Common age of occurrenceCommon age of occurrence
Infants : WeaningInfants : WeaningToddlers : acquiring toilet skillsToddlers : acquiring toilet skillsSchool ageSchool ageMost children are toilet trained (98%) by 4 yrsMost children are toilet trained (98%) by 4 yrs
Constipation difficult to treat, often Constipation difficult to treat, often requires prolonged support, requires prolonged support,
explanation and medical therapyexplanation and medical therapy

October 2010 Dr. Vivek Rege 12
Etiology of ConstipationEtiology of ConstipationOrganic FunctionalARM
Hirschsprung
Neuroenteric
Spinal Cord anomaly
Pelvic floor dysynergia
Metabolic : Thyroid, Calcium, C.F.
Toxic: lead, drugs(opiates, antidep)
Cows milk allergy

October 2010 Dr. Vivek Rege 13
Anatomical causesAnatomical causes• Anal StenosisAnal Stenosis• Anteposed anusAnteposed anus• Ectopic anal openingEctopic anal opening• Anal fissureAnal fissure• Anal strictureAnal stricture• Presacral mass - SCTPresacral mass - SCT

October 2010 Dr. Vivek Rege 14
Anteposed – stenosed anal opening - complaint is constipation

October 2010 Dr. Vivek Rege 15Stenosed anal opening seen anteriorly

October 2010 Dr. Vivek Rege 16
Incision taken after keeping a dilator inside ledge

October 2010 Dr. Vivek Rege 17
After cutting the muscle posteriorly mucosa identified and cut

October 2010 Dr. Vivek Rege 18
Mucosa now sutured to the skin to widen the anal opening to introduce size 13 dilator

October 2010 Dr. Vivek Rege 19
Anal openingAnal opening
FourchetteFourchette

October 2010 Dr. Vivek Rege 20
Suturing of the anal opening

www.addlifesurgikids.com
Three separate openings on perineumThree separate openings on perineum
Anal Anal openingopening

October 2010 Dr. Vivek Rege 22Recto Vaginal fistula –pre opRecto Vaginal fistula –pre op

October 2010 Dr. Vivek Rege 23
Post operative result after pull
thru with normal appearing anal opening in the right position

October 2010 Dr. Vivek Rege 24
Neuromuscular causesNeuromuscular causes
• Mental retardationMental retardation
• MyelomeningoceleMyelomeningocele
• Spinal trauma/surgerySpinal trauma/surgery
• Tethered cordTethered cord
• Muscular dystrophyMuscular dystrophy

Hirschsprung DiseaseHirschsprung Disease• Absence of Absence of GanglionGanglion cells from the bowel cells from the bowel
• Normal alternate segments contract and relax – Normal alternate segments contract and relax – peristalsis to push feces forwardperistalsis to push feces forward
• AganglionosisAganglionosis: contraction present but inability to : contraction present but inability to relax and push forwardrelax and push forward
• Obstruction of passage of feces – filling of rectum Obstruction of passage of feces – filling of rectum upwardsupwards
• Severity depends upon how long a segment of large Severity depends upon how long a segment of large intestine is involvedintestine is involved
October 2010 Dr. Vivek Rege 25

October 2010 Dr. Vivek Rege 26
Functional causesFunctional causes• Poor diet & eating habitsPoor diet & eating habits• Faulty toilet trainingFaulty toilet training• Painful defecationPainful defecation• Poor toilet habits: hurry/too busyPoor toilet habits: hurry/too busy• Withholding behavior - avoidanceWithholding behavior - avoidance• Irregular therapy and/or follow upIrregular therapy and/or follow up

October 2010 Dr. Vivek Rege 27
MedicationsMedications• Anticonvulsants: PhenobarbAnticonvulsants: Phenobarb• DiureticsDiuretics• SucralfatesSucralfates• AntacidsAntacids• Iron preparationsIron preparations• AnticholinergicsAnticholinergics• Antitussive: CodeineAntitussive: Codeine

October 2010 Dr. Vivek Rege 28
Incidence of constipation & responseIncidence of constipation & responsePrevalence : ranges from 0.3 – 28%Prevalence : ranges from 0.3 – 28%School age : Boys > Girls ratio: 3 : 1School age : Boys > Girls ratio: 3 : 1Above 2 yrs : 95% Functional constipationAbove 2 yrs : 95% Functional constipationChild < 5 yrs presenting for constipation:Child < 5 yrs presenting for constipation:
50% take 1 yr for recovery50% take 1 yr for recovery65 – 70 % take 2 yrs for recovery65 – 70 % take 2 yrs for recovery
Child with constipation at 8 yrs: 30% continue to have severe Child with constipation at 8 yrs: 30% continue to have severe constipation beyond pubertyconstipation beyond puberty
80% children with functional constipation have success in 5 yrs80% children with functional constipation have success in 5 yrsLess success if : constipation begins before 1 yr OR associated Less success if : constipation begins before 1 yr OR associated
soiling at presentationsoiling at presentationRelapse after therapy: 30 – 50% and many do not improve on Relapse after therapy: 30 – 50% and many do not improve on
reaching puberty reaching puberty

October 2010 Dr. Vivek Rege 29
Suspect Organic ConstipationSuspect Organic Constipation
Children:Children:• Short segment HirschsprungShort segment Hirschsprung
• Metabolic: HypercalcemiaMetabolic: Hypercalcemia
HypothyroidHypothyroid
Diabetes InsipidusDiabetes Insipidus
Gluten EnteropathyGluten Enteropathy
Lead toxicityLead toxicity
Cystic FibrosisCystic Fibrosis
• Medications: OpiatesMedications: Opiates
BarbituratesBarbiturates
Tricyclic depressantsTricyclic depressants

October 2010 Dr. Vivek Rege 30
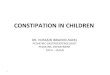
PresentationsPresentations• Delayed passage of meconium > 48 hrsDelayed passage of meconium > 48 hrs• Bottle fed infants – hard stools, diff. in passingBottle fed infants – hard stools, diff. in passing• Breast fed infants with very infrequent stoolsBreast fed infants with very infrequent stools• Weaning on to solids – infrequent stoolsWeaning on to solids – infrequent stools• Toilet training assoc. with withholding behaviour, Toilet training assoc. with withholding behaviour,
functional fecal retentionfunctional fecal retention• Behavioral problems: struggle over toilet training, Behavioral problems: struggle over toilet training,
child refuses to use potty despite trainingchild refuses to use potty despite training• 63% constipation & fecal soiling have had painful 63% constipation & fecal soiling have had painful
defecation before age of 3 yrs & secondary defecation before age of 3 yrs & secondary withholding pattern withholding pattern
Excessive straining to pass stool can lead to Prolapse

October 2010 Dr. Vivek Rege 32
History s/o Functional ConstipationHistory s/o Functional Constipation
• Large calibre ,infrequent stoolsLarge calibre ,infrequent stools
• Fecal soiling after child was toilet trainedFecal soiling after child was toilet trained
• Dietary details: low fibre diet, low vegetablesDietary details: low fibre diet, low vegetables• Details of toilet behaviour: Details of toilet behaviour: TimingTiming
PosturePosture
Restricted accessRestricted access
Toilet Toilet avoidance/refusalavoidance/refusal

October 2010 Dr. Vivek Rege 33
ExaminationExamination• Development within normal limits or notDevelopment within normal limits or not
• Nutritional assessmentNutritional assessment
• Physical examination: Physical examination: AbdomenAbdomen: Colonic mass, fecalomas,: Colonic mass, fecalomas,
SpineSpine: MMC, Occulta, Lower limb tone, power, saddle : MMC, Occulta, Lower limb tone, power, saddle areaarea
Perineum & PRPerineum & PR: Anal wink, cremasteric reflex: Anal wink, cremasteric reflex
Anal tone –sphincter,traumaAnal tone –sphincter,trauma
Rectum: ARM, Empty, stools, Rectum: ARM, Empty, stools, impacted with stool impacted with stool

October 2010 Dr. Vivek Rege 34
Chronic Constipation with Chronic Constipation with Fecalomas palpableFecalomas palpable

October 2010 Dr. Vivek Rege 35
InvestigationsInvestigations• Plain X ray abdomen : if no retention/PR not donePlain X ray abdomen : if no retention/PR not done• USG: Rectal diameter >3 cmsUSG: Rectal diameter >3 cms• Barium Study: Hirschsprung suspicion: Barium Study: Hirschsprung suspicion: done properlydone properly• Anorectal ManometryAnorectal Manometry
Impaired sensation to rectal distensionImpaired sensation to rectal distensionAbnormal contraction Ext. sphincterAbnormal contraction Ext. sphincterAbnormal contraction pelvic floor musclesAbnormal contraction pelvic floor muscles
• Colonic transit time: radioopaque markers/ radioisotopeColonic transit time: radioopaque markers/ radioisotope• Rectal Biopsy: Suction – Acetyl Choline esterase studyRectal Biopsy: Suction – Acetyl Choline esterase study
Full thickness – HP AganglionosisFull thickness – HP Aganglionosis


October 2010 Dr. Vivek Rege 37
DifferentiationDifferentiationFeatureFeature FunctionalFunctional HirschspHirschsp
Starts from birthStarts from birth NoNo YesYes
Fecal soilingFecal soiling OftenOften RareRare
Fecal mass above rectumFecal mass above rectum NoNo YesYes
Retentive posturingRetentive posturing YesYes NoNo
Passage of large stoolPassage of large stool YesYes NoNo
Passage of flatusPassage of flatus YesYes NoNo
Painful defecationPainful defecation YesYes NoNo
October 2010 Dr. Vivek Rege 38
ManagementManagement
• Education: Child & parentsEducation: Child & parents
• Disimpaction of stoolsDisimpaction of stools
• Dietary changes adviceDietary changes advice
• MaintenanceMaintenance
• Behaviour modificationBehaviour modification
• Follow upFollow up

October 2010 Dr. Vivek Rege 39
EducationEducation
• Explain normal physiology of defecationExplain normal physiology of defecation• Use of the sphincters – voluntary & invol.Use of the sphincters – voluntary & invol.• Soiling: lack of conscious awareness of need to Soiling: lack of conscious awareness of need to
defecate due to chronic rectal distension with fecesdefecate due to chronic rectal distension with feces• Incontinence: due to involuntary relaxation of Incontinence: due to involuntary relaxation of
sphincter due to rectal distensionsphincter due to rectal distension• Importance of keeping rectum emptyImportance of keeping rectum empty• Painful bowel movements motivates fecal retentn.Painful bowel movements motivates fecal retentn.• Fecal retentn is NOT oppositional behaviourFecal retentn is NOT oppositional behaviour• Encopresis is NOT voluntaryEncopresis is NOT voluntary

DietDiet• Excess milk & bottle – lethal combinationExcess milk & bottle – lethal combination
• Food habits: Vegetables, Salads, Fruits & Dals Food habits: Vegetables, Salads, Fruits & Dals daily 2 – 4 helpingsdaily 2 – 4 helpings
• No junk foods: Wafers, Chips, Ruffles etcNo junk foods: Wafers, Chips, Ruffles etc
• No fried, pasta, burgers, pizza , noodles etcNo fried, pasta, burgers, pizza , noodles etc
• No gathya farsan, laddus, sweets, ghee etcNo gathya farsan, laddus, sweets, ghee etc
• Breakfast: MUST daily everydayBreakfast: MUST daily everyday
• Non veg substitutes only DalsNon veg substitutes only Dals
October 2010 Dr. Vivek Rege 40

Fecal Impaction Fecal Impaction
• Hard mass palpable in lower Hard mass palpable in lower abdomenabdomen
• Dilated rectum filled with large Dilated rectum filled with large amt. stool on rectal examinationamt. stool on rectal examination
• Excessive stool in the colon on Excessive stool in the colon on radiographyradiography
October 2010 Dr. Vivek Rege 41

October 2010 Dr. Vivek Rege 42

October 2010 Dr. Vivek Rege 43
DisimpactionDisimpactionThree methods: Three methods: EnemasEnemas
SuppositoriesSuppositories
Oral agentsOral agents
• Enemas: rapid, invasive, traumaticEnemas: rapid, invasive, traumatic
• Combination: enema, suppositories, oral agentsCombination: enema, suppositories, oral agents
• Only oral agents: Polyethylene glycol solutionOnly oral agents: Polyethylene glycol solution

October 2010 Dr. Vivek Rege 44
DisimpactionDisimpactionRapid disimpaction:Rapid disimpaction:• 3 enemas/day for 3 days: Day 1: Phosphate enema3 enemas/day for 3 days: Day 1: Phosphate enema
Saline enema(500 – 1000ml)Saline enema(500 – 1000ml)
Day 2: Saline enema(500 – 1000 ml)Day 2: Saline enema(500 – 1000 ml)
Day 3: Saline enema(500 – 1000 ml)Day 3: Saline enema(500 – 1000 ml)• Plain x ray abdomen – if still impactedPlain x ray abdomen – if still impacted• Oral Golytely: NG Tube: 25ml/kg/hr – 4 hrsOral Golytely: NG Tube: 25ml/kg/hr – 4 hrs• Plain x ray abdomen – if still impactedPlain x ray abdomen – if still impacted• Oral laxative: Macrogol(3350) 2 -4 sachets/day, if still impactedOral laxative: Macrogol(3350) 2 -4 sachets/day, if still impacted• Manual evacuation under GA Manual evacuation under GA

October 2010 Dr. Vivek Rege 45
BeforeBefore AfterAfter

October 2010 Dr. Vivek Rege 46
Manual Evacuation Manual Evacuation of fecesof feces

October 2010 Dr. Vivek Rege 47
DisimpactionDisimpaction
Slow disimpaction:Slow disimpaction:• Oral: high dose mineral oil: 15 -30 ml/yr(240ml) to be given Oral: high dose mineral oil: 15 -30 ml/yr(240ml) to be given
for 3 – 4 daysfor 3 – 4 days
• Oral Senna: 15 ml: twice a day for 3 dosesOral Senna: 15 ml: twice a day for 3 doses
• Oral Magnesium Citrate: 30 ml/ yr/day for 3 daysOral Magnesium Citrate: 30 ml/ yr/day for 3 days
Constipation no impaction:Constipation no impaction:• Oral Lactulose dailyOral Lactulose daily
• No Paraffin for < 6 months-aspiration pneumoniaNo Paraffin for < 6 months-aspiration pneumonia
• No phosphate enemas: electrolyte imbalancesNo phosphate enemas: electrolyte imbalances
• Glycerine enemas, suppositoriesGlycerine enemas, suppositories

MaintenanceMaintenance
• Dietary interventionsDietary interventions
• Behavioral modificationsBehavioral modifications
• Oral laxativesOral laxatives
• Ensure bowel movements at normal Ensure bowel movements at normal intervals with good evacuationintervals with good evacuation
October 2010 Dr. Vivek Rege 48

October 2010 Dr. Vivek Rege 49
Behavior ModificationBehavior Modification• Regular toilet regimen: 2-3/day after mealsRegular toilet regimen: 2-3/day after meals
• Fixed time potty: morningFixed time potty: morning
• Proper posture: foot support, feet flatProper posture: foot support, feet flat
• Unhurried time on the pottyUnhurried time on the potty
• Reward system for passing stool without instr.Reward system for passing stool without instr.
• Diary of stool frequency, consistency, pain etcDiary of stool frequency, consistency, pain etc
• Positive reinforcementPositive reinforcement
No role of Bio feedback in therapy of constipationNo role of Bio feedback in therapy of constipation

Dietary ModificationsDietary Modifications• Vegetables at least 2 – 4 servings per dayVegetables at least 2 – 4 servings per day
• Salads raw at least 2 – 4 servings per daySalads raw at least 2 – 4 servings per day
• Whole grainsWhole grains
• Fruits – at least 2 -3 servings per dayFruits – at least 2 -3 servings per day
• Increased fiber contentIncreased fiber content
• Fluids – juices only apple, prune, pearFluids – juices only apple, prune, pear
October 2010 Dr. Vivek Rege 50

October 2010 Dr. Vivek Rege 51
MaintenanceMaintenance
Laxatives :Laxatives :
• Mineral oil: 1 – 3 ml/kg/day in 2 dosesMineral oil: 1 – 3 ml/kg/day in 2 doses
• Lactulose: 1 – 3 ml/kg/day in 3 dosesLactulose: 1 – 3 ml/kg/day in 3 doses
• Mag. Hydroxide: 1 – 3 ml/kg/day in 2 dosesMag. Hydroxide: 1 – 3 ml/kg/day in 2 doses
• Polyethylene Glycol: 1 g/kg/day in 2 doses ORPolyethylene Glycol: 1 g/kg/day in 2 doses OR
15 ml/kg/day in 2 15 ml/kg/day in 2 dosesdoses
• Sorbitol: 1 -3 ml/kg/day in 2 dosesSorbitol: 1 -3 ml/kg/day in 2 doses

October 2010 Dr. Vivek Rege 52
MaintenanceMaintenance
Stimulants:Stimulants:
• Senna : 2 – 6 yrs: 2.5 – 5 ml/day in 2 dosesSenna : 2 – 6 yrs: 2.5 – 5 ml/day in 2 doses
6 -12 yrs: 5 – 7.5 ml /day in 2 doses6 -12 yrs: 5 – 7.5 ml /day in 2 doses
• Bisacodyl(5mg): 1 – 3 Tab in 2 dosesBisacodyl(5mg): 1 – 3 Tab in 2 doses
GoalsGoals: Soft bowel movements: Soft bowel movements
Once or twice a day regularlyOnce or twice a day regularly

October 2010 Dr. Vivek Rege 53
Results & Follow upResults & Follow up
• Best results – combination of medications and Best results – combination of medications and behavioral modification(bm)behavioral modification(bm)
• Medications + bm: remission of enco: 3 -6 mon Medications + bm: remission of enco: 3 -6 mon
• Medications only: remission of enco: > 6 monMedications only: remission of enco: > 6 mon
• Weaning from laxatives – 6 monthlyWeaning from laxatives – 6 monthly
• Follow up takes 6 – 24 months for resultsFollow up takes 6 – 24 months for results

October 2010 Dr. Vivek Rege 54
Results & Follow upResults & Follow up
Long term : Impaction & EncopresisLong term : Impaction & Encopresis• Difficult to treatDifficult to treat• Relapse rate is highRelapse rate is high• Persistence after therapy: 52%: Const. + EncoprPersistence after therapy: 52%: Const. + Encopr
30%: Const. alone30%: Const. alone

October 2010 Dr. Vivek Rege 55
Results & Follow upResults & Follow up
Child < 5 yrs presenting for constipation:Child < 5 yrs presenting for constipation:50% take 1 yr for recovery50% take 1 yr for recovery65 – 70 % take 2 yrs for recovery65 – 70 % take 2 yrs for recovery
Child with constipation at 8 yrs: 30% continue to have Child with constipation at 8 yrs: 30% continue to have severe constipation beyond pubertysevere constipation beyond puberty
80% children with functional constipation have success in 80% children with functional constipation have success in 5 yrs5 yrs
Less success if : constipation begins before 1 yr OR Less success if : constipation begins before 1 yr OR associated soiling at presentationassociated soiling at presentation
Relapse after therapy: 30 – 50% and many do not improve Relapse after therapy: 30 – 50% and many do not improve on reaching puberty on reaching puberty

October 2010 Dr. Vivek Rege 56
Surgical TherapySurgical TherapyIndications:Indications:• No response to therapy: 3 – 6 monthsNo response to therapy: 3 – 6 months• Frequent soiling & distressFrequent soiling & distress• Family doc. feels s/s interfering with school & social Family doc. feels s/s interfering with school & social
relationshipsrelationships• Behavior anomalies: parental distressBehavior anomalies: parental distress
low self esteemlow self esteem
poor adherence to regimespoor adherence to regimes

October 2010 Dr. Vivek Rege 57
Surgical TherapySurgical Therapy
• Resection of sigmoid(dilated)Resection of sigmoid(dilated)
• Appendicostomy/Cecostomy: Antegrade Appendicostomy/Cecostomy: Antegrade enema with daily washouts for dryness enema with daily washouts for dryness for 24 hoursfor 24 hours

October 2010 Dr. Vivek Rege 58
ConclusionsConclusions
• Early regular, relaxed toilet trainingEarly regular, relaxed toilet training
• Proper care of diet & eating habitsProper care of diet & eating habits
• Early consultation for therapy if neededEarly consultation for therapy if needed
• Detailed history and thorough examinatnDetailed history and thorough examinatn
• Relevant investigationsRelevant investigations
• Systematic therapy with chartingSystematic therapy with charting
• Proper and prolonged follow upProper and prolonged follow up