Embed Size (px)
Citation preview

Dr. T. C. R. Rama Krishnan
DIABETES AND BRAIN

Case vignettes
Discussion
Pearls
Scheme of things

A 50 year old male who is a known diabetic came with acute onset of weakness of left sided limbs of 30 min duration
O/E
Left UMN facial palsy with Hemiplegia
CASE I


Capillary blood sugar: 40mg /dl

Serum glucose < 50 mg/dl
< 30 mg Confusion < 10 mg Seizures Coma Medullary phase of Hypoglycemia.
< 70 mg is the level at which counter regulatory hormones get activated
HYPOGLYCEMIA

Glucose is the exclusive fuel for the brain
Brain stores only trivial amounts of glucose as glycogen unlike liver and skeletal muscle
Hyperglycemia is better tolerated by the brain than hypoglycemia
Glucose sensor in the brain- STN
Basics

After food is ingested
Blood glucose level increases
Release of insulin from the pancreas
Glucose homeostasis

Insulin causes suppressing of glucose production in liver and storage of glucose as glycogen in the liver
Normally the liver contains sufficient glycogen stores to maintain the blood glucose concentration at 80-90 mg/dl for 24-36 hours

After that gluconeogenesis is the principal mechanism for maintaining glucose levels
Initially most of the gluconeogenesis takes place in the liver and subsequently in the kidney
50% of the glucose thus produced is utilized by the brain

Glucose reserve in the brain will sustain activity for about 30 min once blood glucose is no longer available.
If blood sugar falls to < 10 mg / dl & persists for minutes , recovery is delayed for weeks & may be incomplete

Neuroglycopenia is the term used to refer to symptomatic hypoglycemia
Sweating, tremor and the sensation of warmth is due to ANS activation
Even though the majority of symptoms of hypoglycemia are related to CNS dysfunction they are extremely varied, non specific and not always present even when blood glucose levels are very low

Decreased caloric intake Liver disease Uremia Infection and shock Burns Pregnancy Neoplasia
Risk factors for hypoglycemia

Acute Sub acute Chronic
Usually due to insulin or OHA
MC form and occurs in fasting state
Rare seen inobsessively controlled diabetics or due to insulin secreting tumor
Begins with vague symptoms
Symptoms seen in acute hypoglycemia are absent
Always consider in dementia
Clinical features of hypoglycemia

acute Subacute Chronic
Patients may recognize these symptoms
Usually accompanied by hypothermia
HbA1C levels are helpful in making the diagnosis
Attacks may end spontaneously or proceed to Sz and coma
Any unexplained hypothermia always check blood sugar
They usually arrive in the ED with coma
Always consider in stroke & seizures
responds well to treatment
Poor response to treatment

Symptoms of hypoglycemia will not be there if the person is on beta blockers or if they have autonomic neuropathy.
Use of Beta Blockers in patients on insulin or OHA is not advisable
Hypoglycemia Unawareness

Hypoglycemia is a medical emergency and should be considered in all patients with altered mental status of unknown origin
Exogenous glucose is harmful to brain during hypoxia or ischemia and caution must be exercised in giving glucose to them

A 54 yr old female not a known diabetic came with H/O involuntary movements involving Left sided limbs of 2 days duration
CASE II



Diagnosis left hemiballismus
Her blood sugar : 640 Ketones : Negative Serum Osmolarity : 311 mosm


A 64 years old Non – diabetic presented with visual disturbances - seeing continuous flashes of light in Left ½ of vision x 3d
O/E
Left homonymous hemianopia Confused No focal deficit
CASE III

Blood sugar 465 mg
HbA1C 15 %

DIAGNOSIS
Hyperglycemia induced seizures
He was treated with insulin , AED for short time
MRI repeated after 3 weeks was Normal


A 45 Year old diabetic presented with acute onset weakness of left sided limbs of 12 hrs duration
His CT Brain, MRI Brain ( DWI ) didn`t show any abnormality
CASE IV

His blood sugar was 472 mg/ dl and his HbA1C was 14%
We treated him with antiplatelets and control of sugar
He recovered completely in 4 days time Repeat MRI done after 4 days was also
normal

Hyperglycemia could be either associated with acidosis (DKA) or non – Ketotic Hyperosmolar coma ( Hyperosmolar Hyperglycemic state HHS )
Non ketotic coma may present with unexplained coma or seizures without any past history
Hyperglycemia

DKA Non ketotic hyperosmolar coma
Common in type I diabetics Feature of type II diabetes
Precipitated by infection Seen in older people commonly as first manifestation
Hyperventilation due to acidosis
Evolves more slowly than DKA
Ketone bodies are positive Clinical symptoms are due to hypertonicity, hypovolemia and cerebral dysfunction with seizures in some
DKA people who die are more often due to neurogenic dysfunction than CVS cause
Precipitated by infection, AGE, pancreatitis and treatment with steroids and phenytoin
Insulin is the corner stone of treatment

Main focus of treatment is correction of dehydration & electrolyte disturbance
Overly vigorous treatment with rapid correction of plasma osmolality can lead to the development of cerebral edema
Consider ICP management in DKA patients who deteriorate

56 year old male known case of uncontrolled diabetes –
Came with history of left side severe ear pain x 10 days
O/E
Left LMN facial palsy Swollen Left ear
CASE V


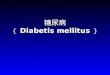
MRI brain



He was referred to ENT surgeon
He was treated with oral quinolones, strict sugar control
Local debridement of the wound was done
DIAGNOSIS Malignant Otitis Externa

72 year old male known diabetic came with deviation of angle of mouth towards right side of 2 days duration
Headache of severe degree interfering with sleep and ADL present
CASE VI

Day 1 Day 2 Day 3 Day 5 Day 7
Left LMN Facial Palsy
Left LMN Facial Palsy
Left LMN Facial Palsy
Operated Left LMN Facial Palsy
Proptosis Left abduction impaired
Left Complete Ophthalmoplegia
Right hemiplegia



DM WITH FUNGAL SINUSITIS
He underwent surgery along with Amphoterecin treatment, antibiotics and supportive measures
Unfortunately he succumbed to his illness
DIAGNOSIS

50 yr old known diabetic presented with acute onset binocular horizontal diplopia on looking to the right
O/E Right VI th nerve palsy
CASE VI


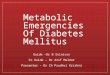
6O yr old diabetic presented with acute onset diplopia with drooping of eyelid
O/E right third nerve palsy
III rd NERVE PALSY

RT III rd NERVE PALSY

VII th NERVE PALSY

Treatment for diabetic cranial mono neuropathy is strict sugar control and physiotherapy
Most of them recover over a period of 6 – 12 weeks

A 50 year old diabetic presented with severe pain along the costal margin radiating from back to anterior aspect of 3 months duration
USG Abdomen CT Abdomen UGIE, Colonoscopy MRI Whole Spine all are normal


Can present with severe pain in a dermatomal pattern
Common in thoracolumbar region in diabetics
Diagnosis

A 40 years old male known diabetic came to us with numbness in the right hand since 1 month
Numbness occurred while mixing food and holding to objects
Numbness was more during night along with radiating pain from wrist to arm
CASE VII

No focal deficit
Tinel`s sign is negative
Phalen`s test positive
O/E


Blood sugar 236 mg/dl HbA1C 8.2% TSH - 1.23 , Free T4 1.35 NCS report showed Bilateral Carpal Tunnel
Syndrome
Investigation


Carpal tunnel Syndrome
Cock up splint at night CTS exercises Surgery for severe cases
Diagnosis & Management

Diabetic neuropathy is a length dependent process
Usually presents with lower limb sensory symptoms
Presentation with upper limb symptoms always consider Entrapment Neuropathy

A 54 years old diabetic female came to us with severe left shoulder pain and inability to lift the left shoulder overhead of 6 months
O/E
Left shoulder abduction restricted Wasting of left arm muscles present Sensation impaired over Left Axillary nerve
area
CASE VIII


She was treated with pregabalin, physiotherapy
Diagnosis

A 56 year old male who is a known case of diabetic came to us with low back pain radiating to left lower limb
Pain is severe in nature interfering with ADL Numbness and burning pain in feet present
O/E Wasting of left thigh Left KJ absent, Left AJ + Sensory - Normal
CASE IX

He was treated with
IV Methyl Prednisolone for 3 days
Pregabalin, Duloxetene and supportive measures
Diagnosis

Consider hypoglycemia in any altered mental status in a diabetic
HHS can present for the first time with seizures or focal deficit or with delirium
Always rule out aneurysm in IIIrd nerve palsy
Facial palsy is not always as simple as it looks
Take home message

Shoulder pain in a diabetic is not always periarthritis shoulder
Sciatica if not responding to treatment consider Lumbosacral Plexopathy
Diabetic neuropathy is more of a sensory neuropathy
If patient present with predominant weakness or if NCS shows demyelinating pathology consider CIDP

Thank you