Embed Size (px)
Citation preview
Metabolic Emergencies Of Diabetes Mellitus
Guide –Dr B SrinivasCo Guide – Dr Arif Maldar
Presenter – Dr Ch Prudhvi Krishna
References
▪ ADA journals▪ William text book of endocrinology ▪ Monograms
What are metabolic emergencies in a diabetic person?
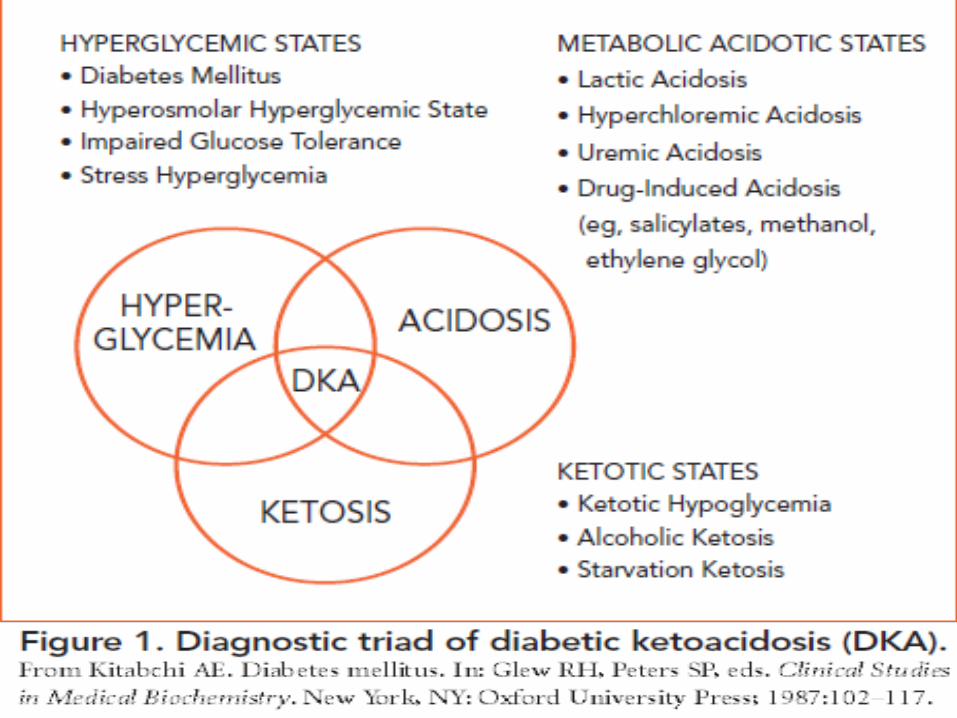
Diabetic ketoacidosis
Hyperglycemic Hyperosmolar state
Diabetic Hypoglycemia
Introduction
▪ Uncontrolled blood sugar often contributes to the incidence of metabolic emergencies of diabetes.
▪ Individuals who experience blood sugar levels that are too high or low may develop conditions that could lead to a coma.
▪ Hypoglycemia results from excessively low blood sugar levels caused by either insufficient food consumption or the presence of too much insulin.
Introduction
▪ DKA and HHS are life threatening emergencies results from excessively high blood sugar levels.
▪ It carries significant risk of death and/or morbidity especially with delayed treatment.
▪ The prognosis of DKA is worse in the extremes of age, with a mortality rates of 5-10%.
▪ With the new advances of therapy, DKA mortality decreases to < 1%.
▪ Before discovery and use of Insulin (1922) the mortality was 100%.
Introduction
▪ HHS and DKA are not mutually exclusive but rather two conditions that both result from some degree of insulin deficiency.
▪ They can and often do occur simultaneously. In fact, one third of patients admitted for hyperglycemia exhibit characteristics of both HHS and DKA.
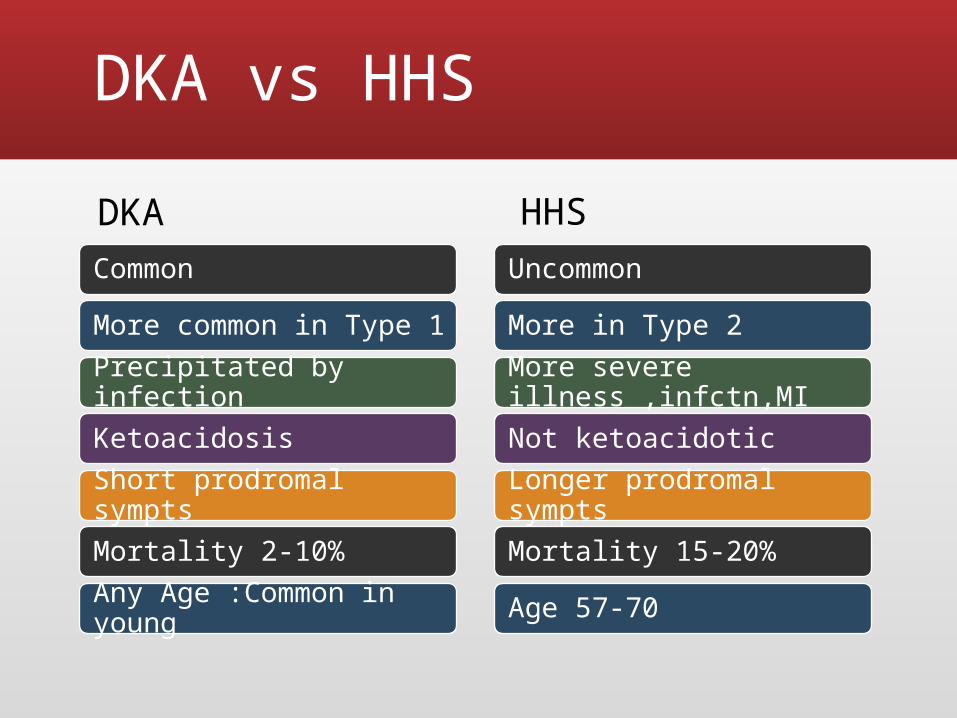
DKA vs HHS
CommonMore common in Type 1 Precipitated by infectionKetoacidosisShort prodromal symptsMortality 2-10%Any Age :Common in young
UncommonMore in Type 2More severe illness ,infctn,MINot ketoacidoticLonger prodromal symptsMortality 15-20%Age 57-70
DKA HHS
Precipitating events
Infection(Pneumonia / UTI / Gastroenteritis / Sepsis)
Inadequate insulin administration Infarction(cerebral, coronary, mesenteric,
peripheral) Drugs (cocaine, that affect carbohydrate
metabolism, such as corticosteroids, thiazides, sympathomimetic agents, and pentamidine)
Pregnancy.Harrison’s Principle of internal medicine 18th edition
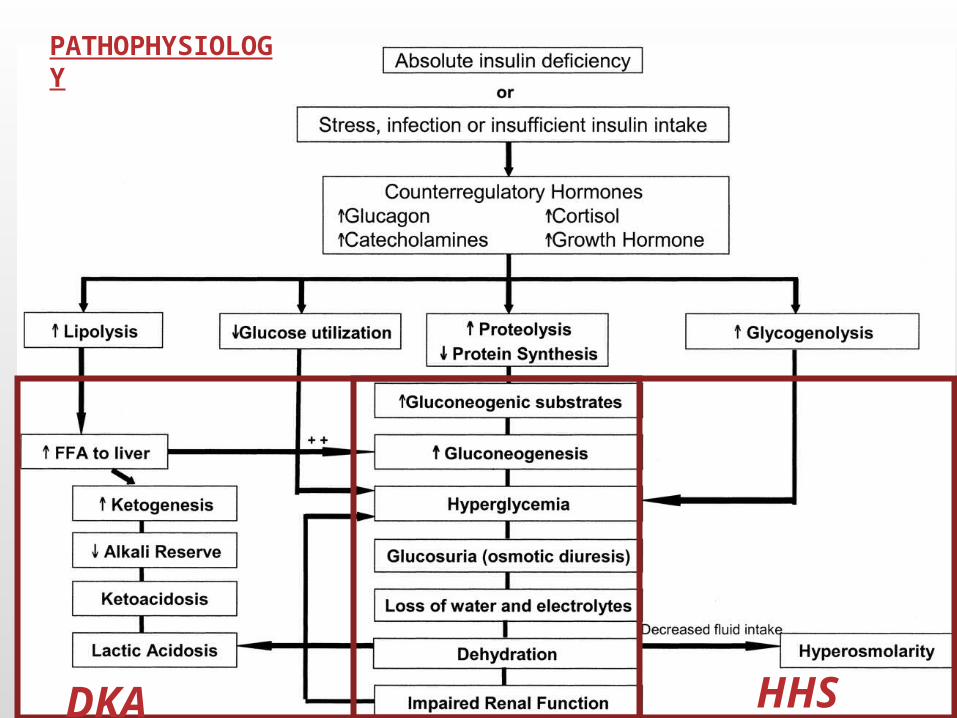
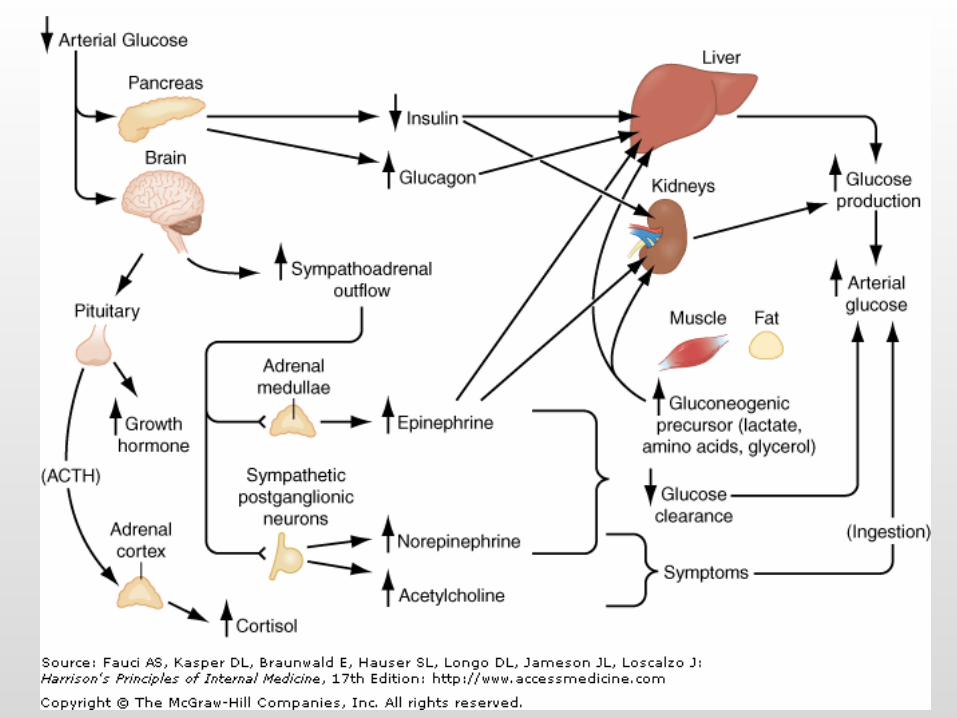
PATHOPHYSIOLOGY
DKA HHS
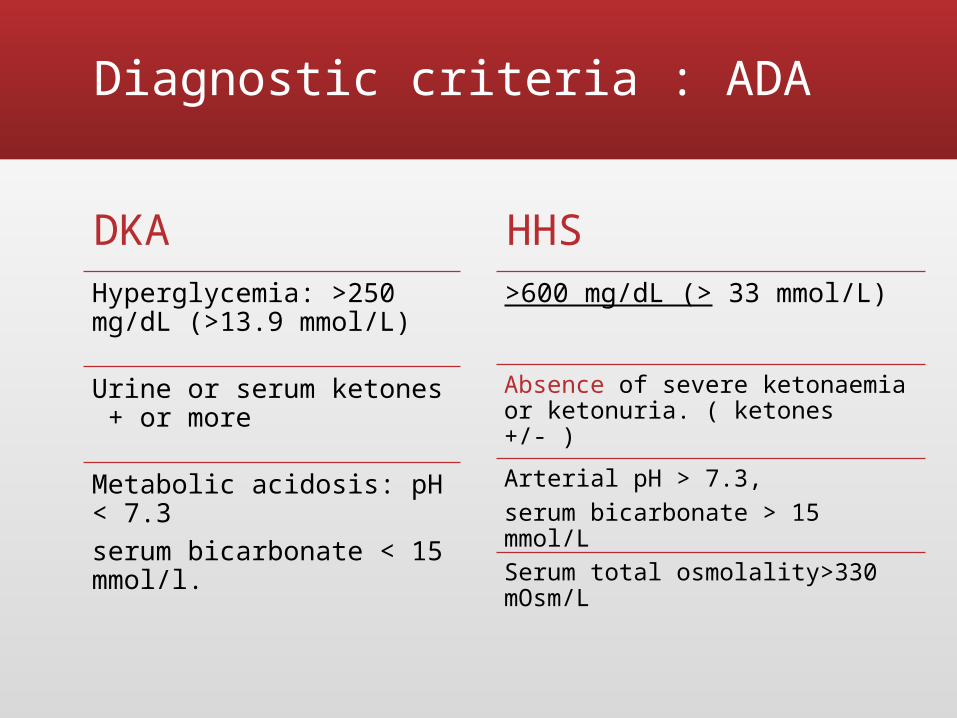
Diagnostic criteria : ADA
DKAHyperglycemia: >250 mg/dL (>13.9 mmol/L)
Urine or serum ketones + or more
Metabolic acidosis: pH < 7.3serum bicarbonate < 15 mmol/l.
HHS>600 mg/dL (> 33 mmol/L)
Absence of severe ketonaemia or ketonuria. ( ketones +/- )
Arterial pH > 7.3, serum bicarbonate > 15 mmol/L
Serum total osmolality>330 mOsm/L
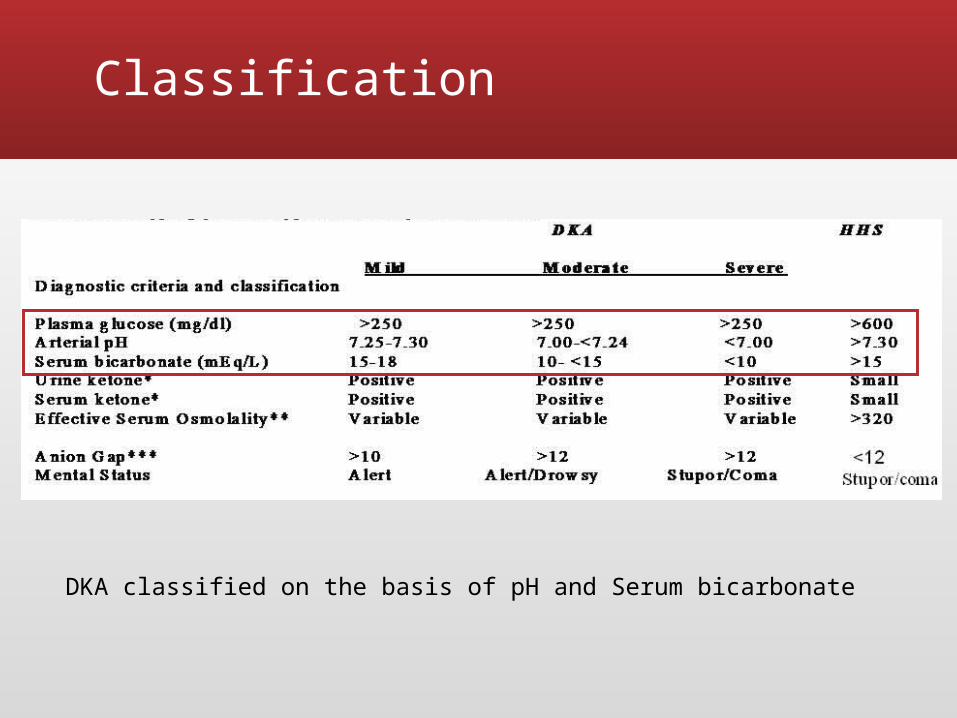
Classification
DKA classified on the basis of pH and Serum bicarbonate
Symptoms and signs of DKA
SymptomsExcessive thirst
Frequent urination
Nausea and vomiting
Abdominal pain
Weakness or fatigue
Shortness of breath
Confusion
SignsKussmal breathing ( Deep respirations )
Dry mucous membranes
Decreased skin turgor
Characteristic acetone (ketotic) Fruity breath odorTachycardia
Hypotension
Fever,cough,chills if associated with intercurrent infection
Symptoms and signs of HHS
▪ Usually presented dehydrated and stupor or coma.
▪ Loss of appetite and polyuria (several weeks)
▪ Profound dehydration▪ Hypotension ,▪ Tachycardia▪ Absence of nausea, vomiting, abdominal
pain
DIAGNOSIS Initial Evaluation
▪ Identify precipitating event leading to elevated glucose (pregnancy, infection, omission of insulin, myocardial infarction, central nervous system event)
▪ Assess hemodynamic status
▪ Examine for presence of infection
▪ Assess volume status and degree of dehydration
▪ Assess presence of ketonemia and acid-base disturbance
14th edition of Joslin's Diabetes Mellitus
DIAGNOSIS LAB INVESTIGATIONS
▪ Complete blood count
▪ Serum ketones/ Urine ketones and sugar
▪ Calculate serum osmolality and anion gap
▪ Urinalysis and urine culture
▪ Consider blood culture
▪ Consider chest radiograph 14th edition of Joslin's Diabetes Mellitus
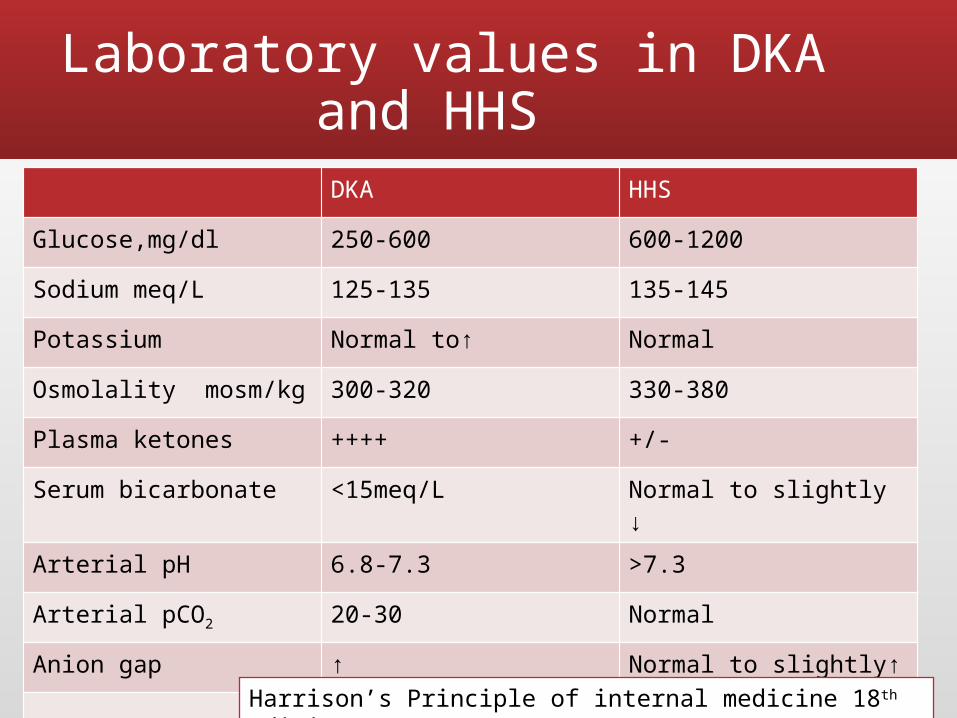
Laboratory values in DKA and HHS
DKA HHSGlucose,mg/dl 250-600 600-1200Sodium meq/L 125-135 135-145Potassium Normal to↑ Normal Osmolality mosm/kg 300-320 330-380Plasma ketones ++++ +/-Serum bicarbonate <15meq/L Normal to slightly ↓Arterial pH 6.8-7.3 >7.3Arterial pCO2 20-30 NormalAnion gap ↑ Normal to slightly↑
Harrison’s Principle of internal medicine 18th edition
14th edition of Joslin's Diabetes Mellitus
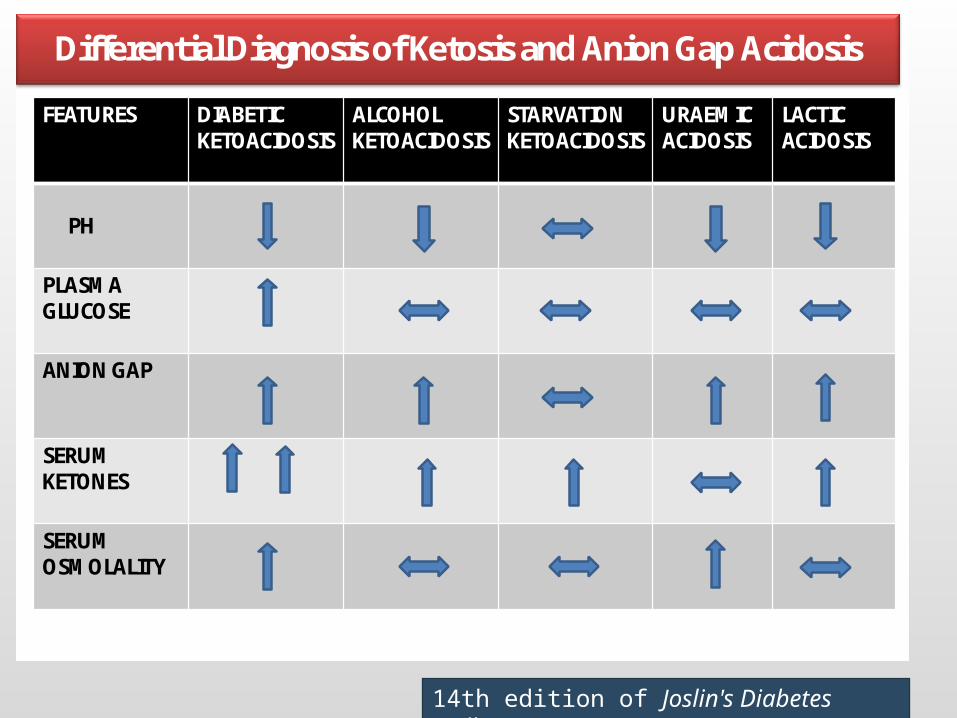
Differential Diagnosis of Ketosis and Anion Gap Acidosis
FEATURES DIABETIC KETOACIDOSIS
ALCOHOL KETOACIDOSIS
STARVATION KETOACIDOSIS
URAEMIC ACIDOSIS
LACTIC ACIDOSIS
PH
PLASMA GLUCOSE
ANION GAP
SERUM KETONES
SERUM OSMOLALITY
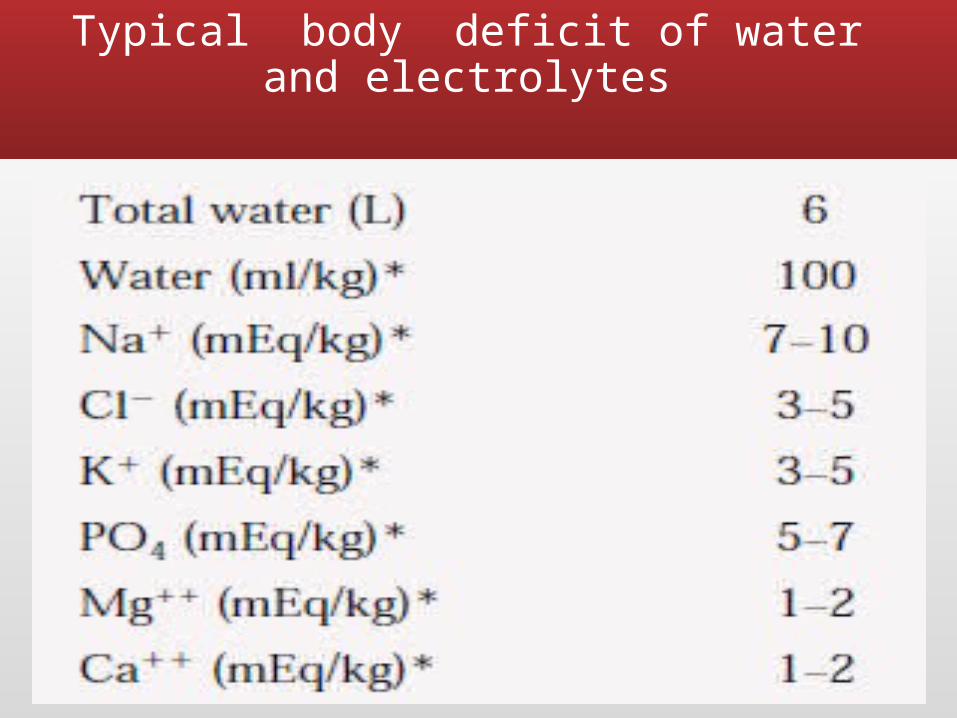
Typical body deficit of water and electrolytes

Management
Treatment Goals
▪ Restoration of volume deficits▪ Resolution of hyperglycaemia and
ketosis/acidosis▪ Correction of electrolyte abnormalities
(potassium level should be >3.3 mEq/L before initiation of insulin therapy; use of insulin in a patient with hypokalaemia may lead to respiratory paralysis, cardiac arrhythmias, and death)
▪ Treatment of the precipitating events and prevention of complications.
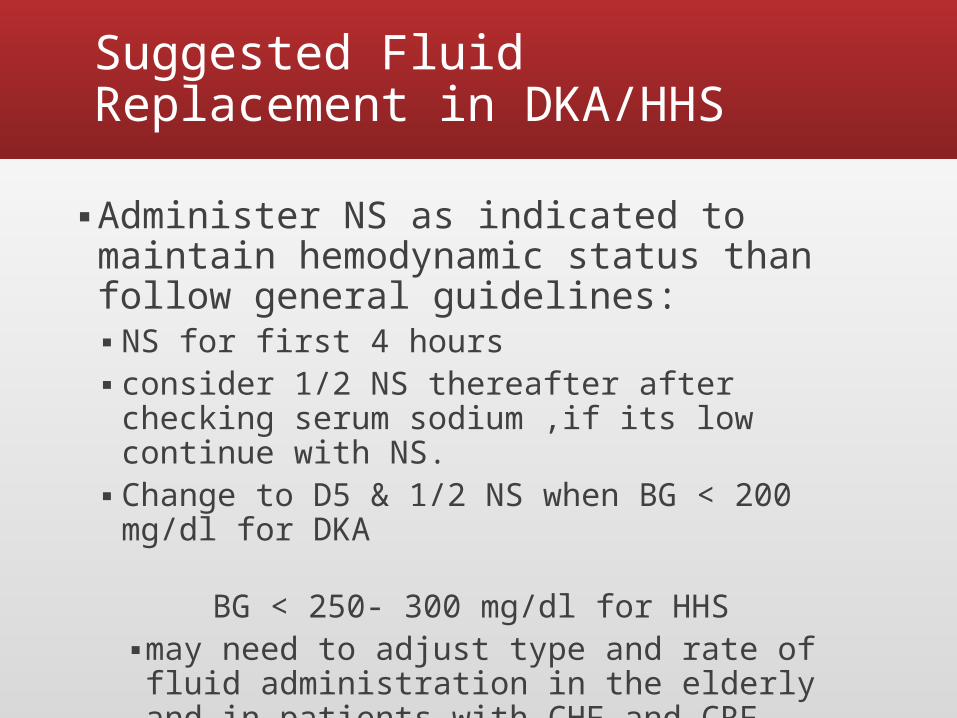
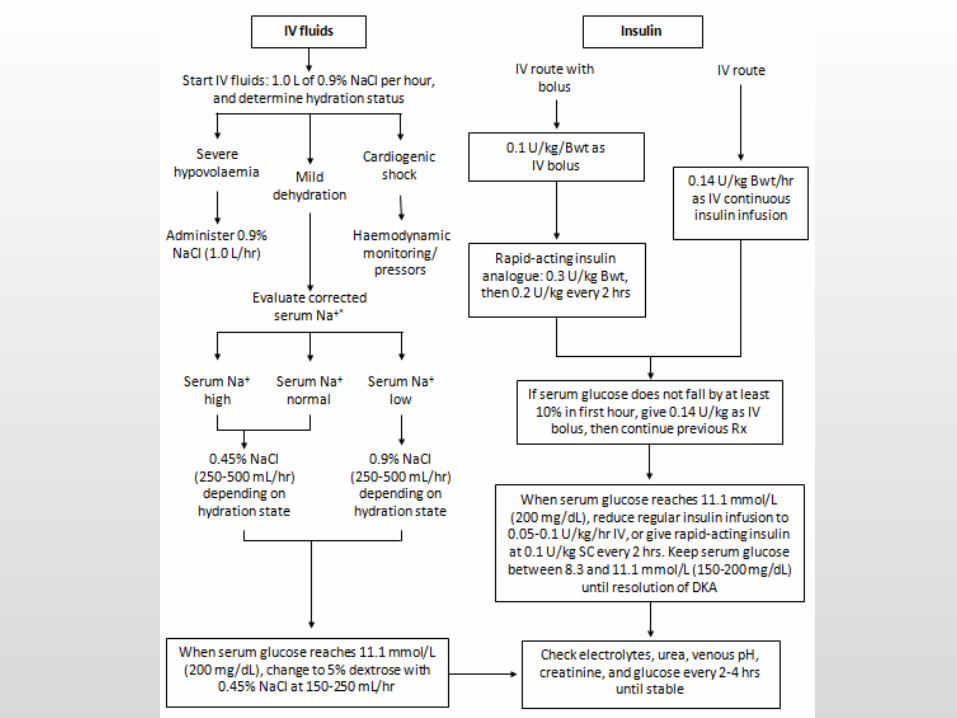
Suggested Fluid Replacement in DKA/HHS
▪ Administer NS as indicated to maintain hemodynamic status than follow general guidelines:▪ NS for first 4 hours ▪ consider 1/2 NS thereafter after checking
serum sodium ,if its low continue with NS.▪ Change to D5 & 1/2 NS when BG < 200 mg/dl
for DKA BG < 250- 300 mg/dl for HHS
▪ may need to adjust type and rate of fluid administration in the elderly and in patients with CHF and CRF
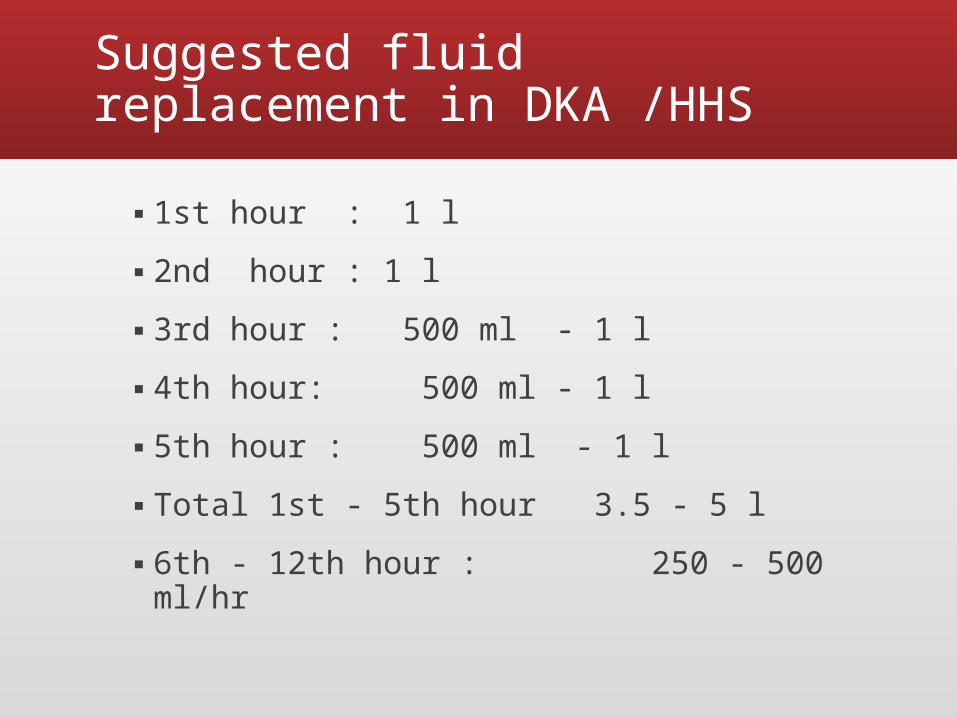
Suggested fluid replacement in DKA /HHS
▪ 1st hour : 1 l ▪ 2nd hour : 1 l ▪ 3rd hour : 500 ml - 1 l ▪ 4th hour: 500 ml - 1 l▪ 5th hour : 500 ml - 1 l▪ Total 1st - 5th hour 3.5 - 5 l ▪ 6th - 12th hour : 250 - 500 ml/hr
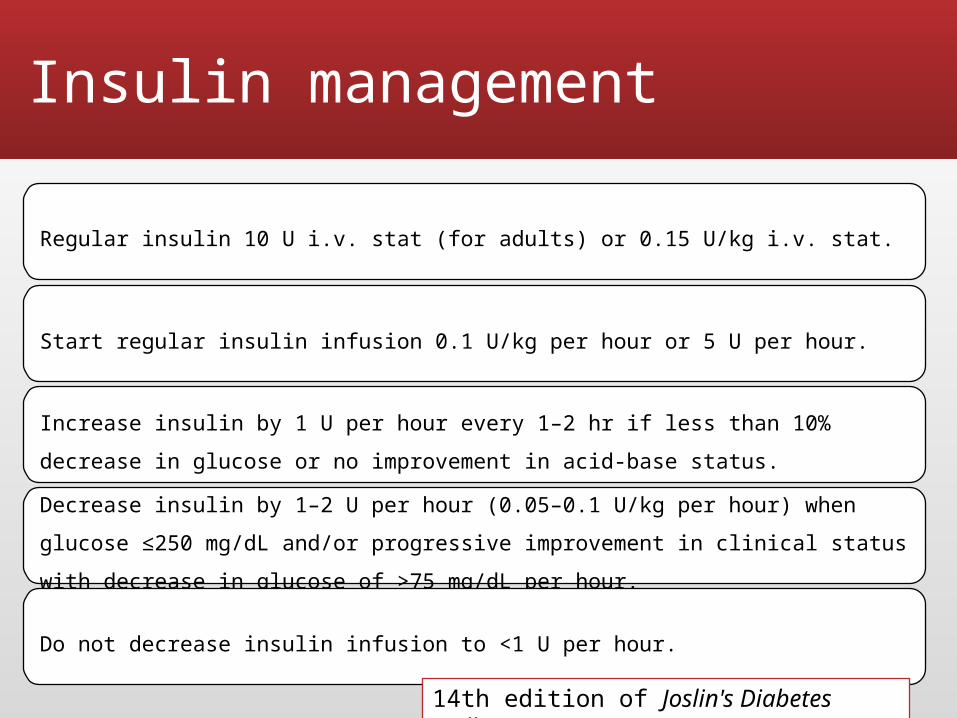
Insulin management
Regular insulin 10 U i.v. stat (for adults) or 0.15 U/kg i.v. stat.
Start regular insulin infusion 0.1 U/kg per hour or 5 U per hour.
Increase insulin by 1 U per hour every 1–2 hr if less than 10% decrease in glucose or no improvement in acid-base status. Decrease insulin by 1–2 U per hour (0.05–0.1 U/kg per hour) when glucose ≤250 mg/dL and/or progressive improvement in clinical status with decrease in glucose of >75 mg/dL per hour.
Do not decrease insulin infusion to <1 U per hour.
14th edition of Joslin's Diabetes Mellitus
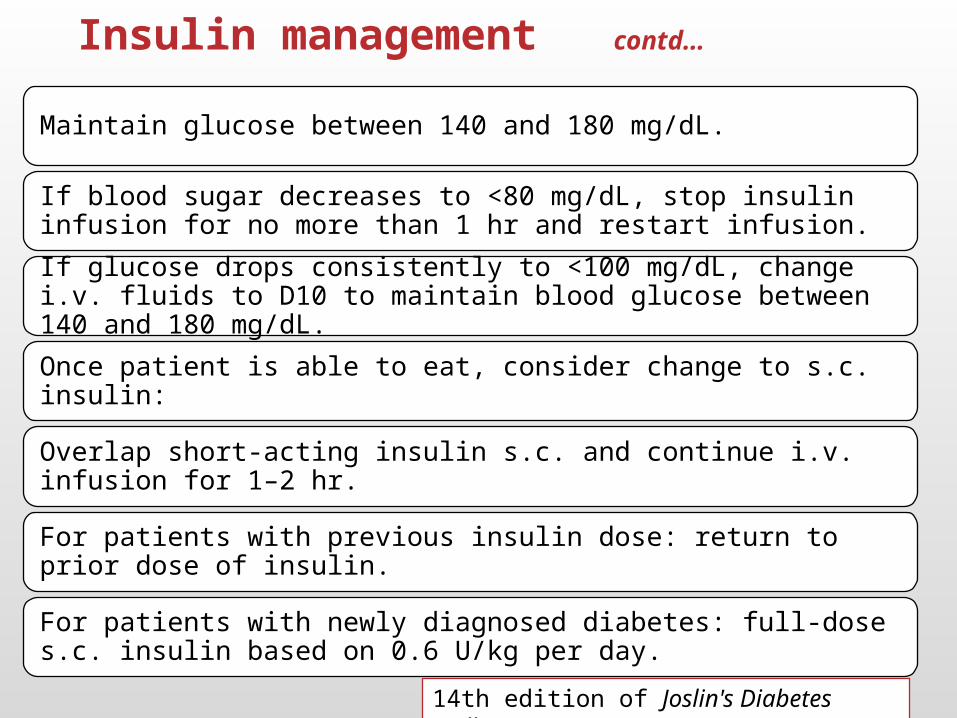
Insulin management contd…
Maintain glucose between 140 and 180 mg/dL.
If blood sugar decreases to <80 mg/dL, stop insulin infusion for no more than 1 hr and restart infusion.
If glucose drops consistently to <100 mg/dL, change i.v. fluids to D10 to maintain blood glucose between 140 and 180 mg/dL.
Once patient is able to eat, consider change to s.c. insulin:
Overlap short-acting insulin s.c. and continue i.v. infusion for 1–2 hr.
For patients with previous insulin dose: return to prior dose of insulin.
For patients with newly diagnosed diabetes: full-dose s.c. insulin based on 0.6 U/kg per day.
14th edition of Joslin's Diabetes Mellitus
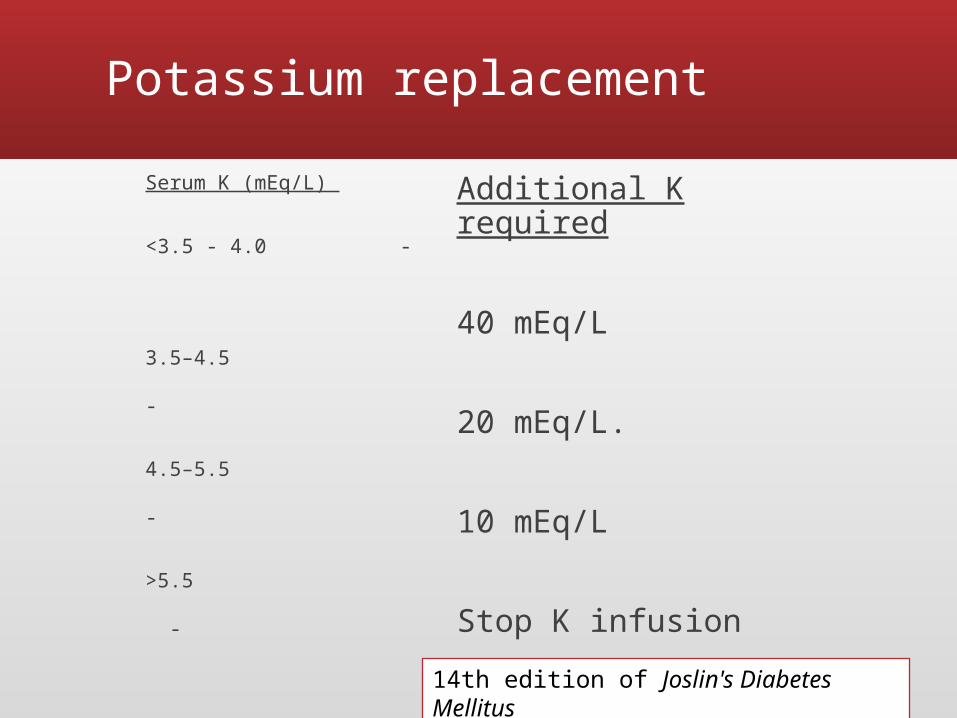
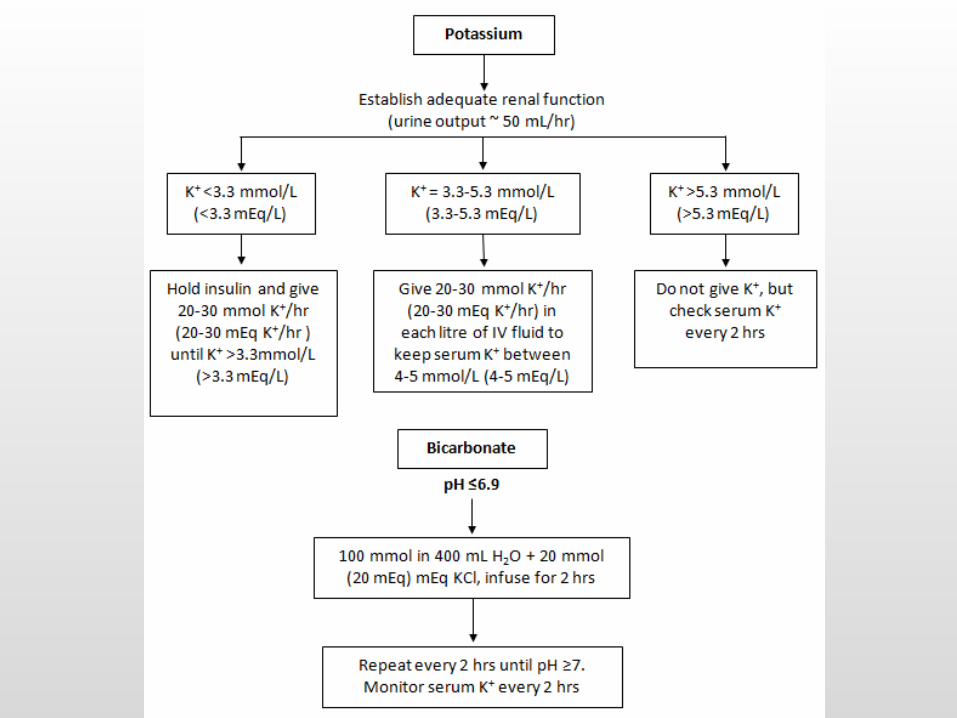
Potassium replacement
Serum K (mEq/L)
<3.5 - 4.0 -
3.5–4.5 -
4.5–5.5 -
>5.5 -
Additional K required
40 mEq/L
20 mEq/L.
10 mEq/L
Stop K infusion
14th edition of Joslin's Diabetes Mellitus
• Hypophasphatemia may develop during increased glucose usage.
• If serum level <1mg/dl then phosphate supplementation considered.
• No benefit demonstrated in RCT .
Phosphate
Bicarbonate
▪ Clinical trials do not support the routine use of bicarbonate replacement
• However, In the presence of severe acidosis (arterial pH <6.9), the ADA advises bicarbonate [50 mmol/L (meq/L) of sodium bicarbonate in 200 mL of sterile water with 10 meq/L KCl per hour for 2 h until the pH is >7.0].
Williams textbook of endocrinology 10th edition and ADA
Monitoring of RX
▪ Blood glucose hourly ▪ Electrolytes every 4 hours ▪ Blood gas analysis after fluid
management ▪ Ok to check venous pH if you can’t get
arterial line ( 0.03 unit less than arterial ).▪ Urine ketone bodies 8th hourly
Criteria for resolution
Management and monitoring should continue until resolution of DKA. ▪ Plasma glucose < 200 mg/dl ▪ Serum bicarbonate >18 mmol/L (>18
meq/L)▪ ABG pH >7.35▪ Anion gap < 10.
Complications of DKA▪ Infection
▪ Precipitates DKA▪ Leukocytosis can be secondary to
acidosis
▪ Shock
▪ Vascular thrombosis▪ Severe dehydration▪ Cerebral vessels▪ Occurs hours to days after DKA
▪ Pulmonary Edema▪ Result of aggressive fluid
resuscitation
▪ Cerebral Edema▪ First 24 hours due to aggressive
correction of hypoglycemia or administration of hypotonic solution
▪ c/p: Mental status changes▪ Tx: Mannitol
Prevention of DKA▪ Never omit insulin
▪ Prevent dehydration and hypoglycemia
▪ Monitor blood sugars frequently
▪ Sick day management -Monitor for ketosis, Be on non sugary fluids, increase insulin if sugars are very high.
▪ Provide supplemental fast acting insulin
▪ Maintain contact with medical team
Pitfalls in DKA▪ Plasma glucose is usually high but not always
▪ DKA can be present with RBS < 300 due to▪ Impaired gluconeogenesis
▪ Liver disease▪ Acute alcohol ingestion▪ Prolonged fasting▪ Insulin-independent glucose is high (pregnancy)
▪ Chronic poor control but taking insulin▪ Ketone in urine may be –ve in DKA, but always +ve in
blood▪ Due to measurement of acetoacetic acid in urine
not, betahydroxybuteric acid▪ Acetone in blood should be done in this case
Pitfalls in DKA
▪ High WBC may be present without infection▪ Infection may be present without fever▪ Blood urea and creatinine may be elevated with
prerenal azotemia secondary to dehydration.▪ Serum amylase is often raised even in the absence of
pancreatitis, In DKA its of salivary origin. Serum lipase should be obtained if pancreatitis is suspected.
Diabetic Hypoglycemia
Introduction
▪ Hypoglycemia is defined as blood sugar below 55 milligrams per deciliter (mg/dL) or 3 millimoles per liter (mmol/L).
▪ An estimated 6-10% of people with Type1DM die as a result of hypoglycemia each year.
▪ Occurs less frequently in Type2DM (People who are on insulin ).
Whipple traid: Symptoms consistent with hypoglycemia Low plasma glucose concentration Relief of those symptoms after the plasma glucose level is
raised
Causes
Common causes of diabetic hypoglycemia include:▪ Taking too much insulin or diabetes
medication▪ Not eating enough.▪ Postponing or skipping a meal or snack▪ Increasing exercise or physical activity
without eating more or adjusting your medications
▪ Drinking binge alcohol.
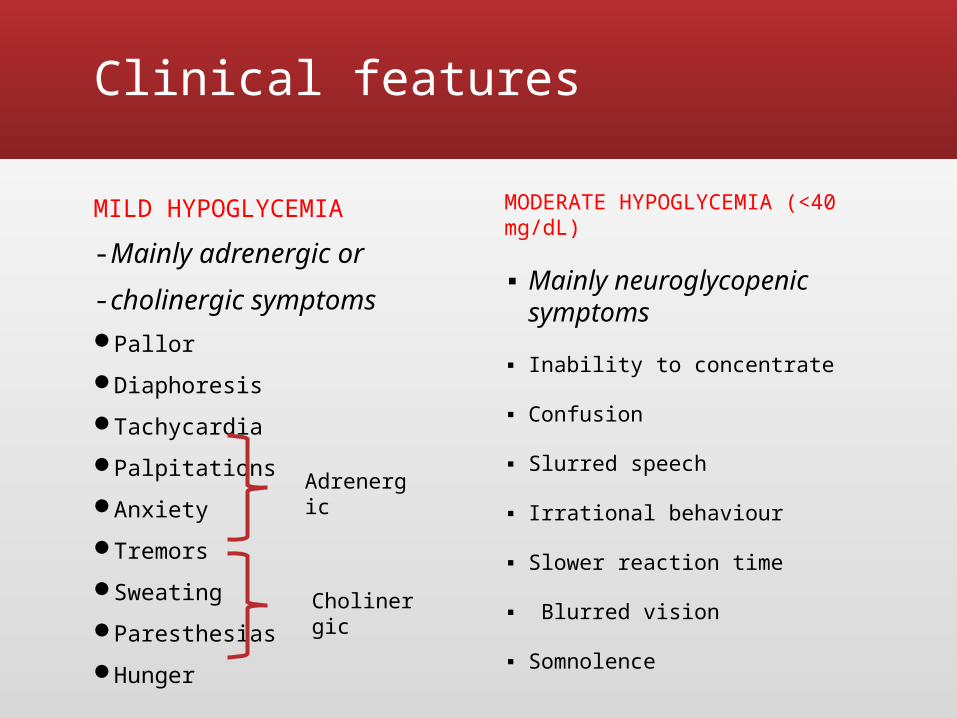
Clinical features
MILD HYPOGLYCEMIA - Mainly adrenergic or - cholinergic symptoms Pallor Diaphoresis Tachycardia Palpitations Anxiety Tremors Sweating Paresthesias Hunger
MODERATE HYPOGLYCEMIA (<40 mg/dL)
▪ Mainly neuroglycopenic symptoms
▪ Inability to concentrate
▪ Confusion
▪ Slurred speech
▪ Irrational behaviour
▪ Slower reaction time
▪ Blurred vision
▪ Somnolence
Adrenergic
Cholinergic
Clinical features
SEVERE HYPOGLYCEMIA (<20 mg/dL )▪ Associated with severe impairment of
neurologic function▪ Completely disoriented behavior▪ LOC▪ Coma▪ Seizures
Treatment
▪ MILD HYPOGLYCEMIA▪ Oral carbohydrates (at least 15gm)▪ Sources include
▪ Three glucose tablets (5g each)▪ 2 ½ cups of fruit juice▪ 1 cup of milk
▪ If patient is unable to take orally give IV dextrose
Treatment – Moderate to severe hypoglycemia.
▪ Dextrose - 50mL of 50% dextrose IV bolus after blood draw followed by 10% dextrose
▪ Glucagon – 1mg IM or SC can be given▪ Effective in treating hypoglycemia only if
sufficient liver glycogen present( absent in alcohol induced hypoglycemia)
▪ Patient is urged to eat as soon as possible
Prevention
▪ Patient education▪ Knowing signs and symptoms of hypoglycemia▪ Take meals on a regular schedule▪ Carry a source of carbohydrate▪ Self monitoring of blood glucose▪ Take regular insulin at least 30 min before eating
Thank you
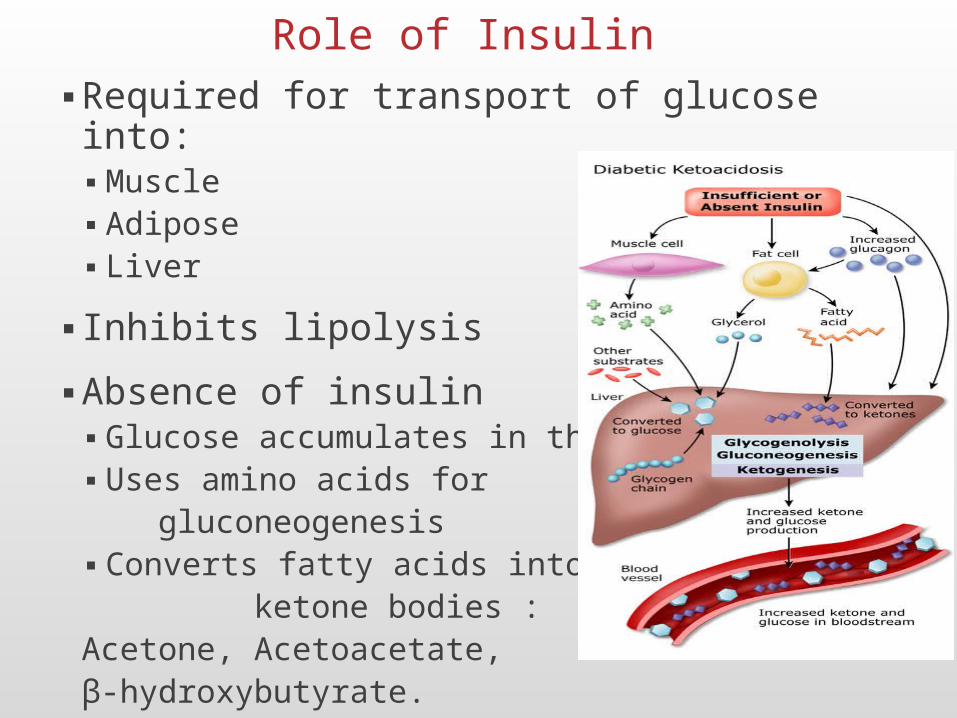
Role of Insulin▪ Required for transport of glucose into:
▪ Muscle▪ Adipose▪ Liver
▪ Inhibits lipolysis
▪ Absence of insulin▪ Glucose accumulates in the blood.▪ Uses amino acids for gluconeogenesis▪ Converts fatty acids into ketone bodies : Acetone, Acetoacetate, β-hydroxybutyrate.



























![Diabetis 1997[1]](https://img.pdfslide.net/doc/110x75/55cc55a6bb61eb3e4a8b4644/diabetis-19971.jpg)
