Embed Size (px)
DESCRIPTION
Review about hematopoetic stem cell transplantation
Citation preview
REVIEW ARTICLE: Haematopoietic stem cell
transplantation: Current status
By Dr. KUMARBHARGAV
7/14/2014 1

7/14/2014 2
Population of undifferentiated cells which are able to Divide for indefinite period.
Self renew. Generate a functional progeny of highly specialized
cells.
What is Stem Cell?
7/14/2014 3
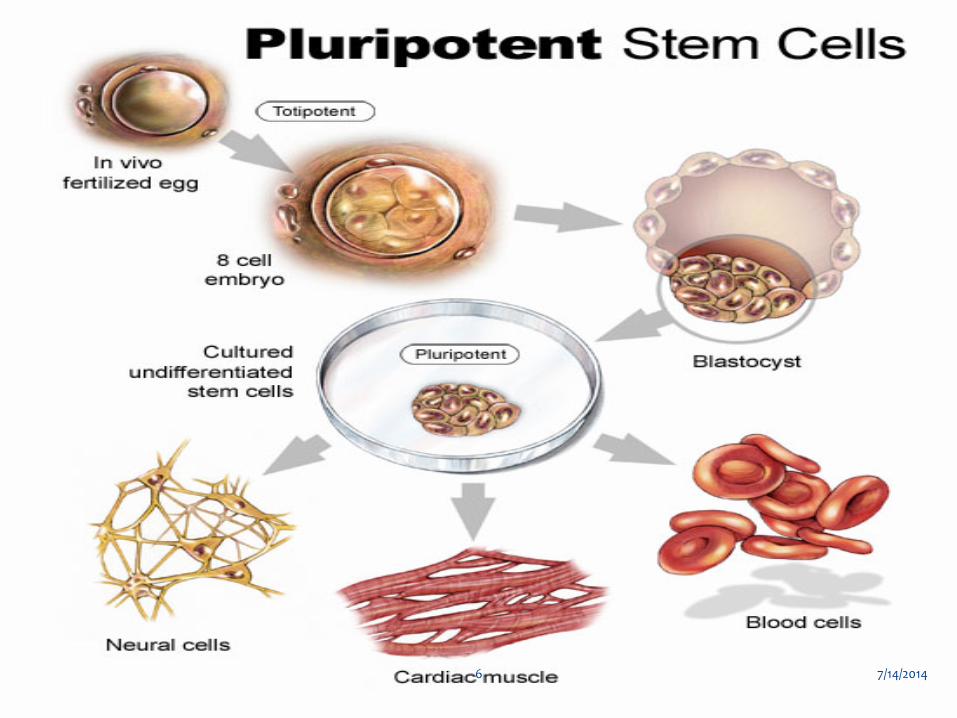
1.Embryonic stem cell (E S Cells ) : ∗ Are Pleuripotent.
∗ Can generate all tissues of body.
∗ Derived from embryos(blastocyst).
∗ Developed from in vitro fertilization.
Sources of stem cells
7/14/2014 4
7/14/2014 5
7/14/2014 6

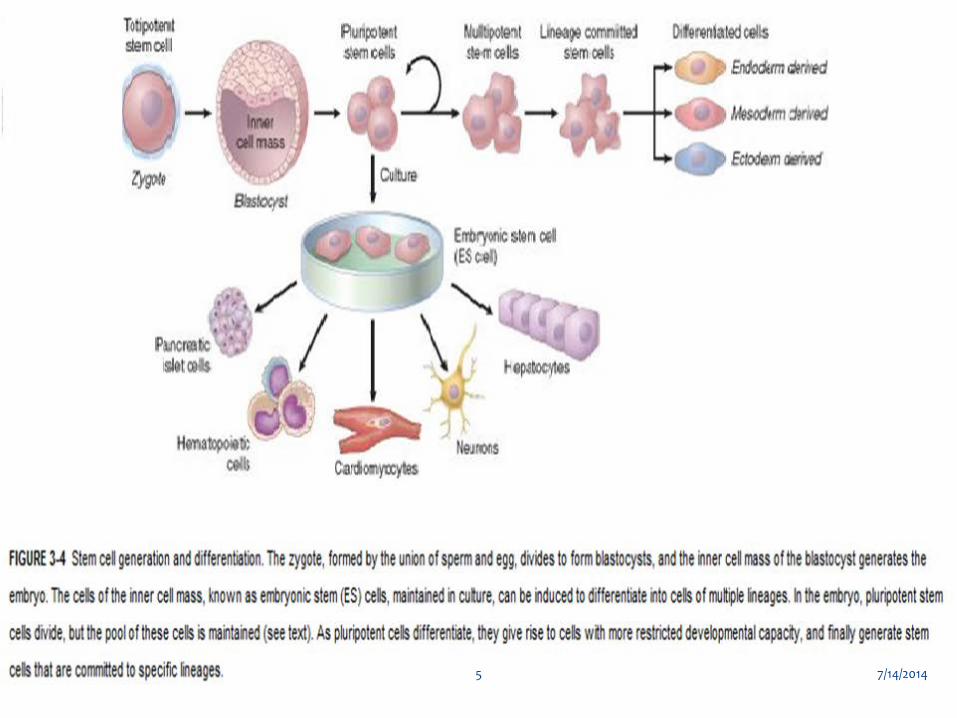
Pluripotent, embryonic stem cells originate as inner mass cells within a blastocyst. The stem cells can become any tissue in the body, excluding a placenta. Only the morula's cells are totipotent, able to become all tissues and a placenta 7/14/2014 7
2.Adult stem cells ( somatic cells ) : ∗ Undifferentiated cell found among differentiated cells
in a tissue or organ.
∗ Can renew it self in to specialized cells.
∗ e.g. Bone marrow , Skin , lining of G.I.T., pancreas , liver adipose tissues & many others
Sourses of stem cells
7/14/2014 8
7/14/2014 9

∗ Reprogrammed cells Known as iPS cells ,are able to generate cells from endodermal , mesodermal and ectodermal in origin.
∗ They function in vivo after genetic manipulation & Transplantation.
∗ More recently Pleuripotent iPS cells were generated by transfecting mouse hepatocytes,gastric cells & terminally differentiated mature B lymphocytes.
∗ iPS cells have been called ES cells without embryos.
Induced Pleuripotent Stem Cells
7/14/2014 10

7/14/2014 11
∗ Steps involved in therapeutic cloning, using embryonic stem cells (ES cells) for cell therapy. The
∗ diploid nucleus of an adult cell from a patient is introduced into an enucleated oocyte.
∗ The oocyte is activated, and the zygote divides to become a blastocyst that contains the donor DNA.
∗ The blastocyst is dissociated to obtain ES. ∗ These cells are capable of differentiating into various
tissues, either in culture or after transplantation into the donor.
∗ The goal of the procedure is to reconstitute or repopulate damaged organs of a patient, using the cells of the same patient to avoid immunologic rejection.
Therapeutic cloning
7/14/2014 12

7/14/2014 13
Lalit Kumar :REVIEW ARTICLE : Hematopoietic stem cell transplantation : Current Status
National medical journal of India Vol.20,No.3 ,2007
Review Article
7/14/2014 14
∗ HSCT is now established treatment for a number of
malignant and non malignant conditions. ∗ Bone-marrow or Peripheral Blood derived
allogeneic or autologous stem cells provides cure for many patients with critical diseases.
Abstract
7/14/2014 15

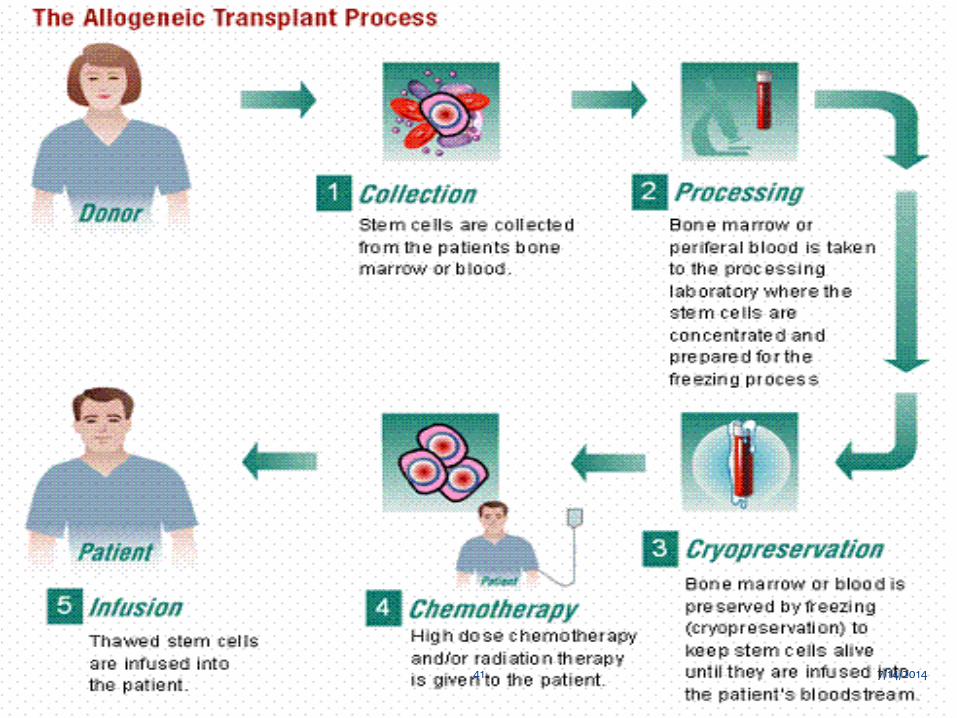
∗ Bone marrow transplantation refers to i.v.infusion
of haematopoetic progenitor cells to re-establish haematopoesis in pt. with a defective or damaged bone marrow.
Introduction
7/14/2014 16

∗ Essential for Allogeneic HSCT.
∗ HLA identical donor is one that matches the
recipient’s HLA antigens:
∗ HLA-A,HLA-B,HLA-C,HLA-DR,HLA-DQ ( Also called 6/6 match ).
∗ At least 5/6 or 6/6 matching should be there.
HLA Typing
7/14/2014 17
∗ DNA based methods have now replaced serology for HLA Typing which includes: PCR amplification of specific HLA genes from genomic
DNA Sequencing-based typing or sequence specific
oligonucleotide probe hybridization( SSOPH ).
Methods
7/14/2014 18
∗ If multiple donors available then choice is based
upon Donor’s blood group Age Transfusion History CMV status For women donor parity
Contd…
7/14/2014 19
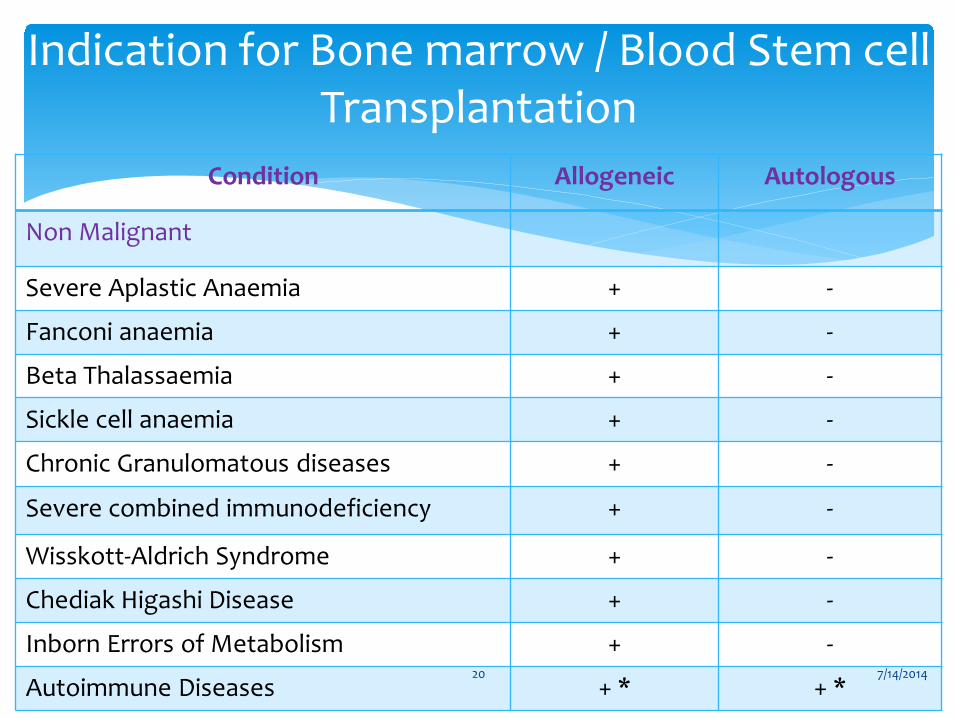
Condition Allogeneic Autologous
Non Malignant
Severe Aplastic Anaemia + -
Fanconi anaemia + -
Beta Thalassaemia + -
Sickle cell anaemia + -
Chronic Granulomatous diseases + -
Severe combined immunodeficiency + -
Wisskott-Aldrich Syndrome + -
Chediak Higashi Disease + -
Inborn Errors of Metabolism + -
Autoimmune Diseases + * + *
Indication for Bone marrow / Blood Stem cell Transplantation
7/14/2014 20

Condition
Allogeneic
Autologous
Malignant
Chronic Myeloid Leukemia + + *
Acute Myeloblastic Leukemia + +
Acute Lymphoblastic Leukemia + * * -
Hodgkins Disease + * +
Non Hodgkins Lymphoma + * +
Chronic Lymphoblastic Leukemia + * + *
Myelodysplastic syndrome + + *
Multiple Myeloma ± + *
Neuroblastoma - +
Germ cell tumour of testis - + *
Ovarian Cancer - + *
Breast Cancer - + *
Renal Cell Cancer + * - 7/14/2014 21
Bone marrow
Peripheral blood
Umbilical cord blood
Fetal liver
placenta
Sources of Hematopoietic stem cells
7/14/2014 22
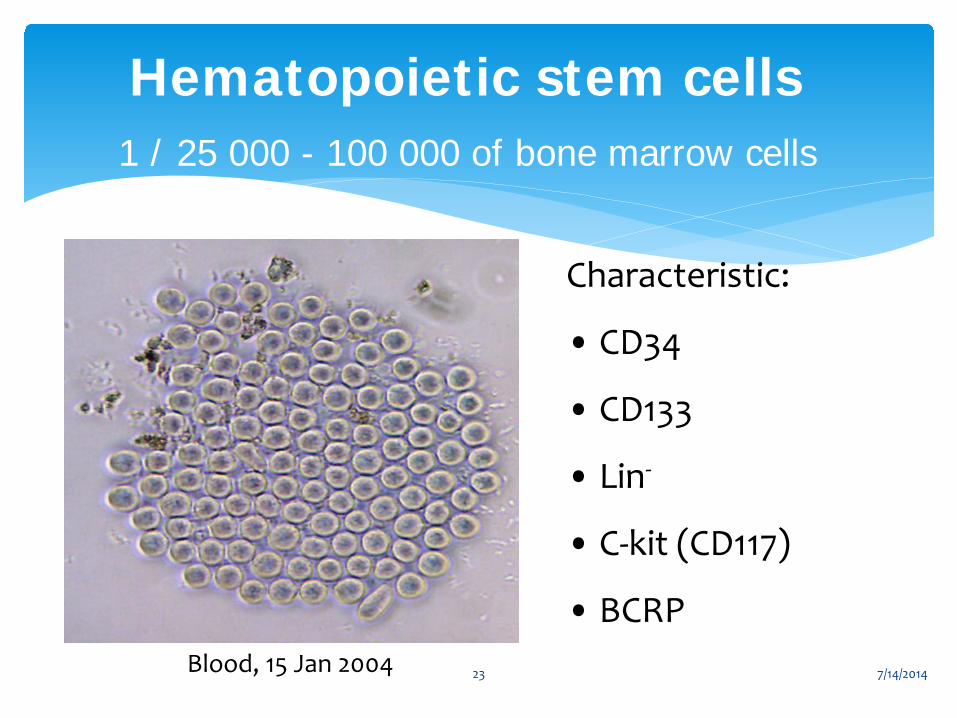
Hematopoietic stem cells 1 / 25 000 - 100 000 of bone marrow cells
Characteristic:
• CD34
• CD133
• Lin-
• C-kit (CD117)
• BCRP Blood, 15 Jan 2004 7/14/2014 23

Hematopoeitic Stem cell
7/14/2014 24

∗ Allogeneic HSCT
Syngeneic (from identical twins). from sibling/related donor. from unrelated donor.
∗ Autologous HSCT
Type of HSCT
7/14/2014 25
Harvesting Stem Cells
7/14/2014 26
Under Local anaesthesia by repeated aspiration
from the posterior illiac crest and is well tolerated. Anterior illiac crest or sternum can be used. It is necessary to remove mature erythrocytes from
the graft to avoid hemolytic transfusion reaction in allogeneic HSCT with major incompatibilities.
Bone Marrow
7/14/2014 27
∗ G-CSF in a dose of 10µg/kg/day in two divided doses S.C. for 4 to 5 days.
∗ On day 5 to 6 PB stem cells are collected by leukapheresis using apheresis (cell separator) machine.
∗ Which contains substantially more CD34+ cells and 10 times more lymphocytes than a BM harvest.
∗ These PB stem cells are cryopreserved at -80oC using 7.5% DMSO or liquid nitrogen.
Peripheral Blood
7/14/2014 28

7/14/2014 29

∗ At the time of delivery by clamping the cord and nicking the umbilical vein at the newborns first cry.
∗ Normal blood bags are used for collection.
∗ Volume 100 ml (60-140 ml).
∗ Samples sent to determine cell counts and for culture.
∗ Then cryopreserved in liquid nitrogen till further use.
Umbilical Cord
7/14/2014 30

7/14/2014 31
∗ 1 in 200 individuals1 may need a haematopoietic stem cells (HSCs) transplant by the age of 70 according to a scientific paper published in 2008
∗ It is once-in-a-life time chance2 to collect cord blood – a readily available source when needed in the future.
∗ 60% higher chance of locating a match versus bone marrow in a family.
Top 5 reasons why you should consider cord blood banking
7/14/2014 32

∗ Research showed that patients have a lower chance of complications in transplants when they receive stem cells from a relative3.
∗ Some of the most common cancers are treatable with a stem cell transplant.
∗ For instance, Lymphoma and Leukaemia are two of the top 10 common cancers for adults4 and among the top five most common childhood cancers5 in India.
Contd…
7/14/2014 33
Umbilical cord blood as a source of HSCT
for hematopoietic reconstitution
Advantages
Rapid procurement Less stringent HLA
matching Expanded donor pool Less graft-versus-host
disease
Disadvantage
Low cell dose Delayed engraftment Poor immune reconstitution Increased graft failure rate
Potential solution
Double Cord Transplantation Ex Vivo Expansion 7/14/2014 34

∗ Placenta and fetal liver are under trial phase but
could be great option in future.
Others
7/14/2014 35
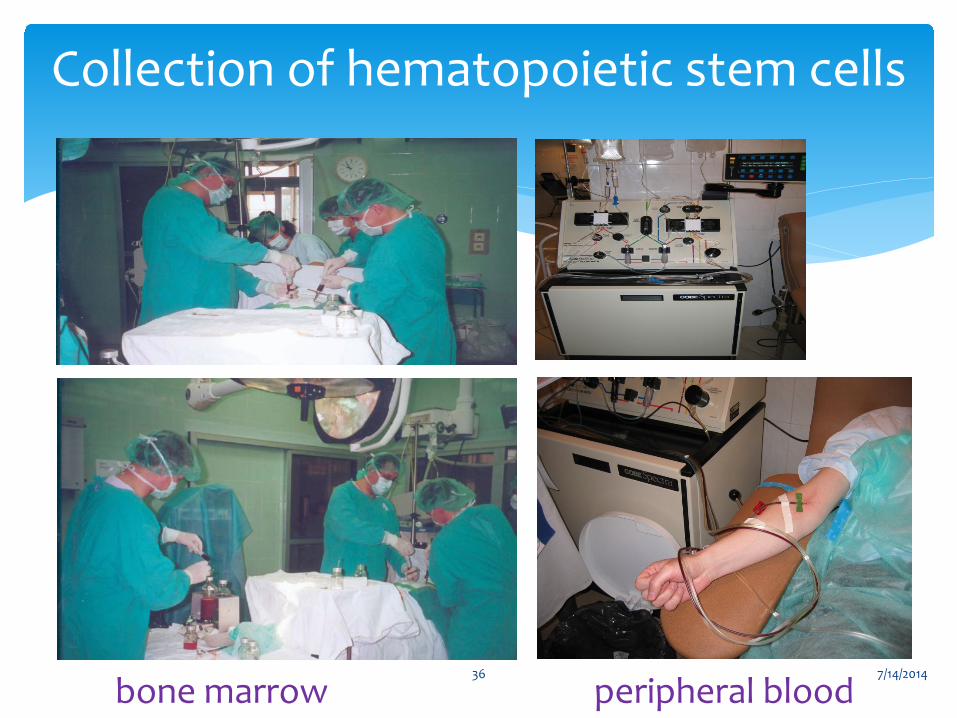
bone marrow peripheral blood
Collection of hematopoietic stem cells
7/14/2014 36

Approx. 3 × 10 ⁸ nucleated cells / kg of recipient's
body wt.—for bone marrow. 5 × 10 ⁸ mono nuclear cells / kg or
2 × 10 ⁶ / kg CD 34+ cells (markers of stem cells) – for
Peripheral blood. > 2-5 × 10 ⁷ / kg nucleated cells or 2-5 × 10 ⁵/ kg CD
34+ cells – For UCB.
Number of Stem Cells
7/14/2014 37
∗ Detailed general physical examination,Hb,CBC,Chest X-rays.
∗ Cardiac, renal, lung & liver function.
∗ Viral infection (Hepatitis B & C ,CMV)
∗ Details of chemotherapeutic drugs received in past.
∗ Fungal, tubercular infection.
∗ Allo-immunisation of platelets.
∗ We insert a central venous line (Hickman catheter) in all recipients 10 days prior to procedure.
Recipient’s and Donor Evaluation
7/14/2014 38
∗ BM is destroyed by High Dose Chemotherapy and/or total body irradiation
To Eradicate malignant or abnormal cells To create space within BM microenvironment to
allow engraftment of stem cells To provide immunosupression to prevent rejection. ∗ For autologous transplantation immunosupression
is not required.
Preparatory Regimen
7/14/2014 39
∗ 24 to 48 hrs of rest period is allowed after HDCT Stem cells are removed from deep freezer
Thawed at room temp. in water bath.
Reinfused in patient
∗ Prophylactic antimicrobials may be used.
∗ Allogeneic HSCT recipients also receive acute GVHD
prophylaxis with methotrexate and cyclosporins.
Stem Cell Infusion
7/14/2014 40
7/14/2014 41

7/14/2014 42

Bone marrow transplantation unit
7/14/2014 43

Hematopoietic stem cell infusion
7/14/2014 44
7/14/2014 45
7/14/2014 46
7/14/2014 47
Non Malignant conditions
7/14/2014 48
7/14/2014 49
∗ Advances in care including New born screening , Early introduction of penicillins,pneumococcal vaccines & comprehensive care have resulted in marked improvement in life expectancy.
∗ However mean age of death of pt. is 42 year for male & 48 year for females.
∗ Hydroxyurea & chronic transfusion can ameliorates many complication but Allogeneic HSCT is only therapeutic option with curative intent.
Sickle Cell Anaemia
7/14/2014 50
∗ Allogeneic HSCT after myeloablative therapy has been performed in > 250 pts. (< 16 years ) with SCD.
∗ Outcome of HSCT with matched siblings is excellent with overall survival 93 – 97 % & event free survival is 85 %.
Contd…
7/14/2014 51
∗ Major indication of Allogeneic transplantation in India.
∗ Potentially curable with an allogeneic transplantation.
∗ Results are excellent if transplant done prior to complication of iron overload, Transfusion complication, and Allo-immunisation.
∗ Results from pesaro,Italy suggest > 85 % DFS for pts. Transplanted early & similar results are obtained at CMC vellore.
Thallaesemia Major
7/14/2014 52
∗ As soon as the child is diagnosed all siblings should be typed for HLA.
∗ If identical match is available than transplant should be done as soon as possible.
∗ For nursing convenience and post transplant care allo-SCT in India is generally performed after the child is more than 3 years of age
Contd..
7/14/2014 53

∗ In young pt. with an HLA matched sibling donor ,allo – HSCT should be considered 1st line therapy as the complications are much less.
∗ In those older than 40 years, Immunosupression should be tried 1st .
∗ Recent study shows better outcome with Bone marrow than PBSC which mainly because of high GVHD in PBSC group.
Severe Aplastic Anaemia
7/14/2014 54
∗ Allogeneic HSCT from an HLA identical sibling must be
considered early in the course of disease.
∗ As pts. are prone to DNA damage because of sensitivity of hematopoietic tissues,pre-transplant conditioning with chemotherapeutic drug is used but not the radiation.
Fanconi Anaemia
7/14/2014 55
∗ A matched sibling donor transplant is the TOC for pts. With Severe combined immunodeficiency disease. Wiskott-Aldrich syndrome. Chediak-Higashi syndrome.
∗ About 74 % of pts. Are cured following HSCT.
Immunodeficiency Diseases
7/14/2014 56
∗ 1st successful BM transplantation of Hurlers syndrome was reported in 1981.
∗ Since than more than 300 transplants using BM & UCB have been done world wide.
∗ Following successful transplant life expectancy is increased,hepatospenomegaly gets resolved ,cardiac disease stabilized & there is improvement in the range of motion of joints, airway disease & hearing.
Inherited Metabolic disorders
7/14/2014 57
Malignant Conditions
7/14/2014 58
∗ High Dose Chemotherapy (HDCT) supported with autologous SCT is currently standard of care for relapsed HL & HL refractory to Primary therapy.
∗ In CIBMTR study,among 5219 pts.receiving
autotransplants for HD bt.1998 and 2006 3 year probabilities of survival were 78±1%,69±1% and 49±3% for pts. in CR,PR and with chemoresistant disease respectively.
Hodgkin's Lymphoma
7/14/2014 59
∗ Among 297 pts. Receiving HLA matched SCT
bet.1998 and 2006 3 year probabilities of survival were 39±5% with Myeloablative conditioning regimens and 38±5% with reduced intensity conditioning regimen.
Contd…
7/14/2014 60
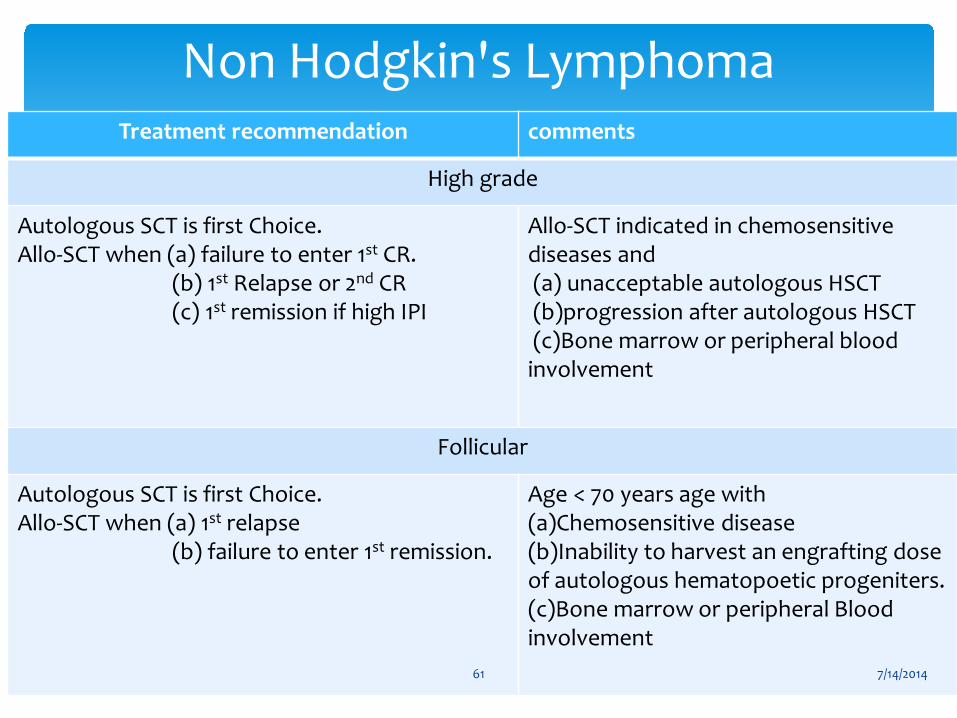
Treatment recommendation comments
High grade
Autologous SCT is first Choice. Allo-SCT when (a) failure to enter 1st CR. (b) 1st Relapse or 2nd CR (c) 1st remission if high IPI
Allo-SCT indicated in chemosensitive diseases and (a) unacceptable autologous HSCT (b)progression after autologous HSCT (c)Bone marrow or peripheral blood involvement
Follicular
Autologous SCT is first Choice. Allo-SCT when (a) 1st relapse (b) failure to enter 1st remission.
Age < 70 years age with (a)Chemosensitive disease (b)Inability to harvest an engrafting dose of autologous hematopoetic progeniters. (c)Bone marrow or peripheral Blood involvement
Non Hodgkin's Lymphoma
7/14/2014 61
∗ High Dose melphalan 200 mg/ m2 followed by ASCT associated with CR rates of 40-60% with improved overall & event free survival.
∗ Data on effectiveness of ASCT in pts. >65 years and
those with end stage renal disease is limited.
Multiple myeloma
7/14/2014 62

Acute Myeloid Leukemia
7/14/2014 63
E. Donnall Thomas The Nobel Prize, 1990
first succsessful HSCT in treatment of acute leukemias Thomas ED, Lochte HL, Lu WC, Ferrebee JW. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N. Engl. J. Med. 1957; 257: 491 7/14/2014 64
∗ About 80 % of children with good risk ALL are now cured with standard chemotherapy.
∗ Therefore ,allogeneic HSCT is usually reserved for Children < 15 year with t(4;11) & philadelphia
chromosome t (9;22). Young adults bet. 15 and 21 years who have high
leukocyte count at diagnosis.
Acute Lymphoblastic Leukemia
7/14/2014 65
∗ Allogeneic HSCT is the treatment of choice for pts. With international prognostic Scoring system (IPPS) intermediate – 2 & high risk MDS.
∗ However its use is limited because of higher median age at the time of dignosis (70 years).
Myelodysplastic Syndrome
7/14/2014 66
∗ Imatinib Mesylate is now TOC for all newely diagnosed pt.
∗ Allogeneic HSCT is considered for Who failed to achieve CR after 3 months of Imatinib
therapy Who failed to achieve complete cytogenetic
response after 12-18 months of Imatinib therapy. Who relapse after initial response. With advanced disease (accelerated phase/blast
crisis)
Chronic Myeloid Leukemia
7/14/2014 67
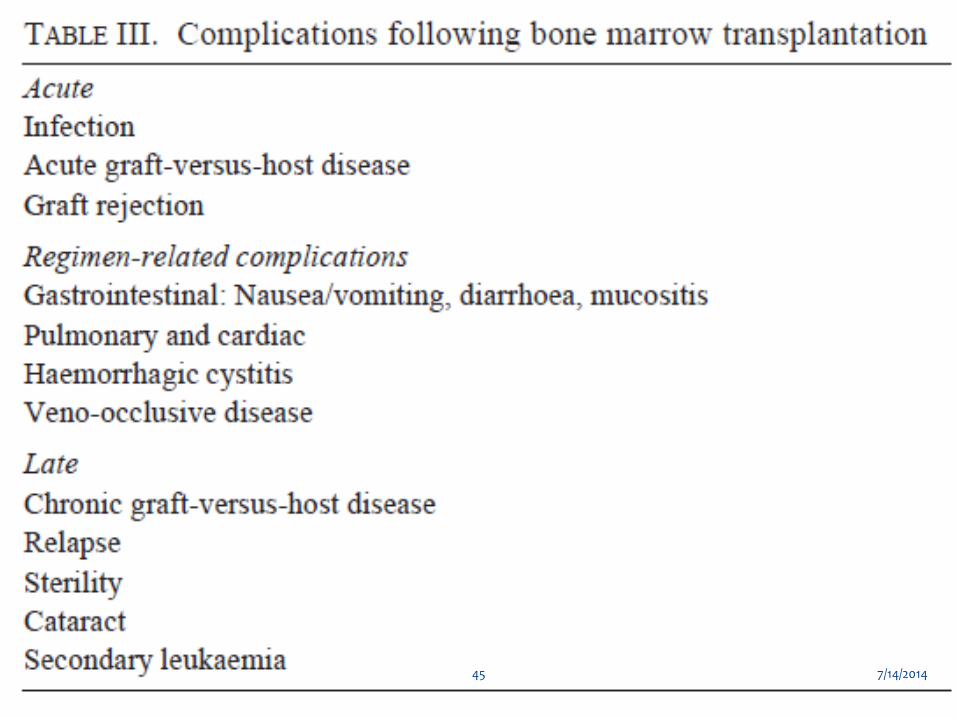
∗ Allogeneic HSCT is associated with significant
morbidity & mortality due to regimen related toxicities ,GVHD & infection.
∗ At present with HSCT experience is small but it appears that allogeneic HSCT could be considered in selected young pts. Using reduced intensity conditioning.
Chronic Lymphocytic Leukemia
7/14/2014 68

Double or Tandem Transplant
7/14/2014 69

∗ Second Transplant within 1-6 months of recovery from the 1st transplant has been attempted to improve CR rates & survival.
∗ Studies suggest higher CR rates, improved overall & event free survival with double transplant compared to single transplant.
Double or Tandem Transplant
7/14/2014 70
∗ Kumar et al have most recently reported results of meta-analysis of six randomized trials .
∗ Response rate was significantly better with double transplant.
∗ But at present it should be considered as experimental approach for younger pt.
Contd…
7/14/2014 71
∗ First BM Transplantation was done in March 1983 at Tata Memorial Hospital ,Mumbai.
∗ Next centre to start BMT/SCT was CMC Vellore where the first Allogeneic BMT was done in 1986.
∗ AIIMS New Delhi is the third largest centre in the country.
Where Does India Stand ?
7/14/2014 72

7/14/2014 73

∗ SCT especially Allogeneic SCT should be offered where benefits outweigh the risks.
∗ Non Transplant Therapy should be compared to SCT before making any recommendation.
∗ Counseling of pt. & Pt’s preference is extremely important as SCT involves considerable expence,often prolonged morbidity & even fatality.
∗ In India ,where the cost is usually borne by the pt. & family ,economic factors need consideration.
Take Home Message
7/14/2014 74

∗ Early Transplants offers better results than SCT performed in advanced disease.
∗ In those disorders where Non Transplant therapy offers similar outcomes . SCT is offered only when there is failure of alternate therapy.
∗ In hematological malignancies cytogenetics & molecular prognostic markers usually guide the timing of transplantation.
Contd…
7/14/2014 75

7/14/2014 76
∗ National Medical Journal of India Vol.20 N0.3 , 2007
∗ Recent advances in Hematology-3.
∗ Robbins 8th edition.
∗ Internet references.
References :
7/14/2014 77

Thank you all for listening
7/14/2014 78








![Alevilikte Cem · 2019. 10. 23. · Remzi Kaptan Alevilikte Cem [3] Remzi Kaptan, 1976 yılında K. Mara'ta doğdu. Temel çalıma alanı bata Alevilik olmak üzere dinler ve inançlardır](https://img.pdfslide.net/doc/110x75/60ac8191ce777602a204d55d/alevilikte-2019-10-23-remzi-kaptan-alevilikte-cem-3-remzi-kaptan-1976-ylnda.jpg)


















