Embed Size (px)
Citation preview
بسم هللا الرحمن الرحيم
Dr Ahmed Esawy
Postoperative Complications
of Transplanted Liver
Dr. Ahmed Esawy
MBBS M.Sc MD
Dr Ahmed Esawy
Postoperative Complications
Vascular Others
Biliary Parenchymal
Dr Ahmed Esawy
POSTOPERATIVE COMPLICATIONS OF LIVER TRANSPLANTATION
1- Vascular complications :
I- Arterial complications (i) Hepatic artery thrombosis.
(ii) Hepatic artery stenosis.
(iii) Hepatic artery pseudoaneurysm and
(iv) arteriovenous (HA and PV)
(v) arteriobiliary (HA and biliary tree) fistulae.
II- Venous complications: involve the inferior vena cava or the PV and consist of thrombosis or
stenosis) Dr Ahmed Esawy
2- Biliary complications : (i) Biliary duct obstruction (due to stricture
anastomotic or nonanastomotic.
(ii) Bile leak.
(iii) other rare biliary complications).
.
Dr Ahmed Esawy
3-Parenchymal complications
-Rejection Acute or Chronic rejection.
-Hepatic infarction
– Hepatic abscess
– Biloma
– Recurrence of malignancy
– Fatty liver
– Complication of biopsy
Dr Ahmed Esawy
4- Post-transplant lymphoproliferative disorders
5- Post-transplant malignancies.
6- Postoperative abdominal complications.
Hemorrhage
Bowel obstruction
7- Chest complications.
Pulmonary calcinosis
Edema
Pneumonia
Pulmonary infarction
8- Neurological complications.
Hemorrhage
Ischemia
Abscess and PTLD
Dr Ahmed Esawy
10- Infection and fever.
11- Recurrent liver disease.
12- Other long-term complications.
a-Arterial hypertension.
b-Diabetes mellitus
Dr Ahmed Esawy
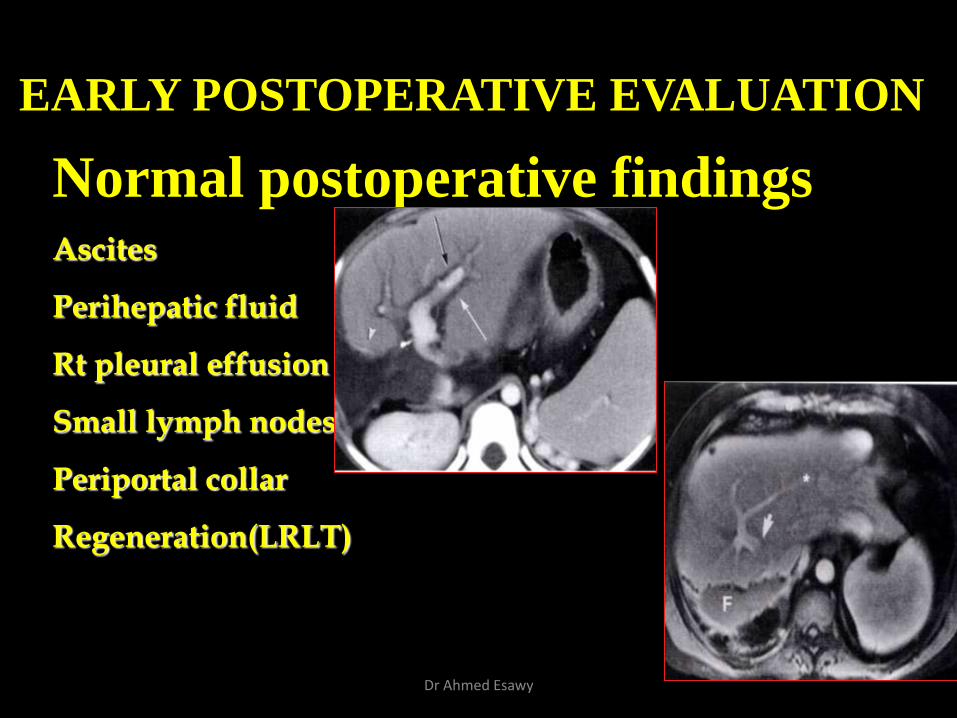
EARLY POSTOPERATIVE EVALUATION
Normal postoperative findings Ascites
Perihepatic fluid
Rt pleural effusion
Small lymph nodes
Periportal collar
Regeneration(LRLT)
Dr Ahmed Esawy
Vascular Complications
Hepatic artery Hepatic veins
Portal vein IVC
Dr Ahmed Esawy
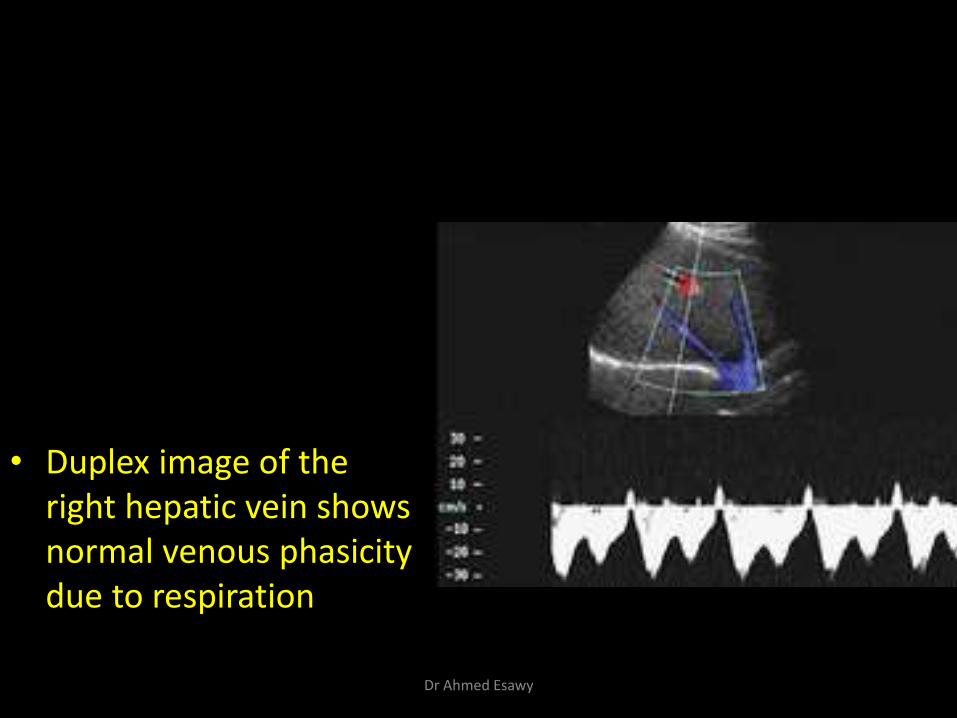
• Duplex image of the right hepatic vein shows normal venous phasicity due to respiration
Dr Ahmed Esawy
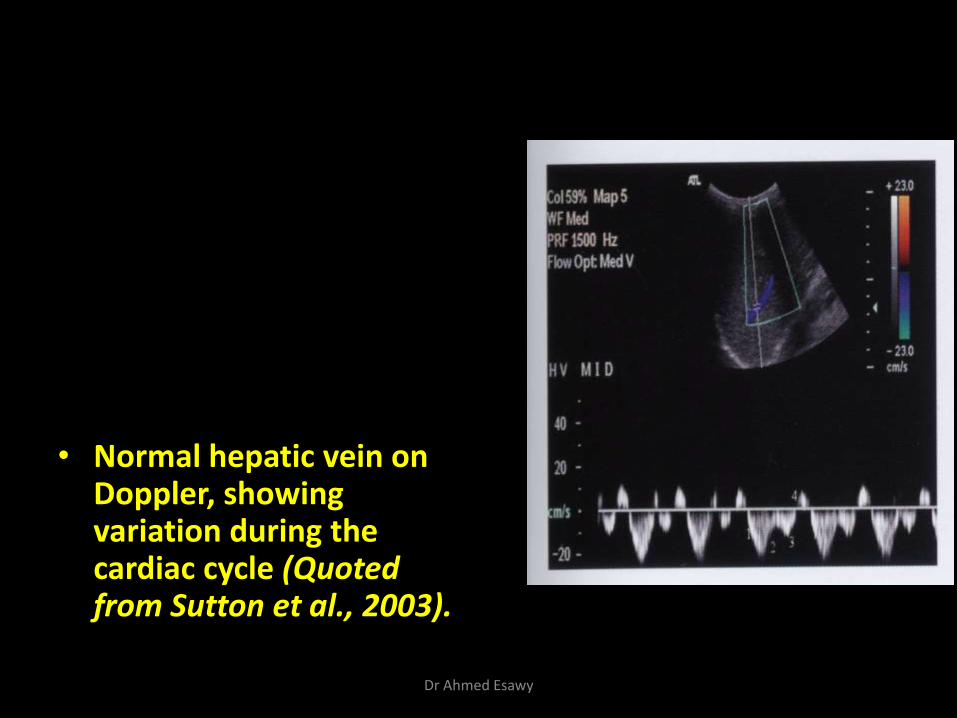
• Normal hepatic vein on Doppler, showing variation during the cardiac cycle (Quoted from Sutton et al., 2003).
Dr Ahmed Esawy
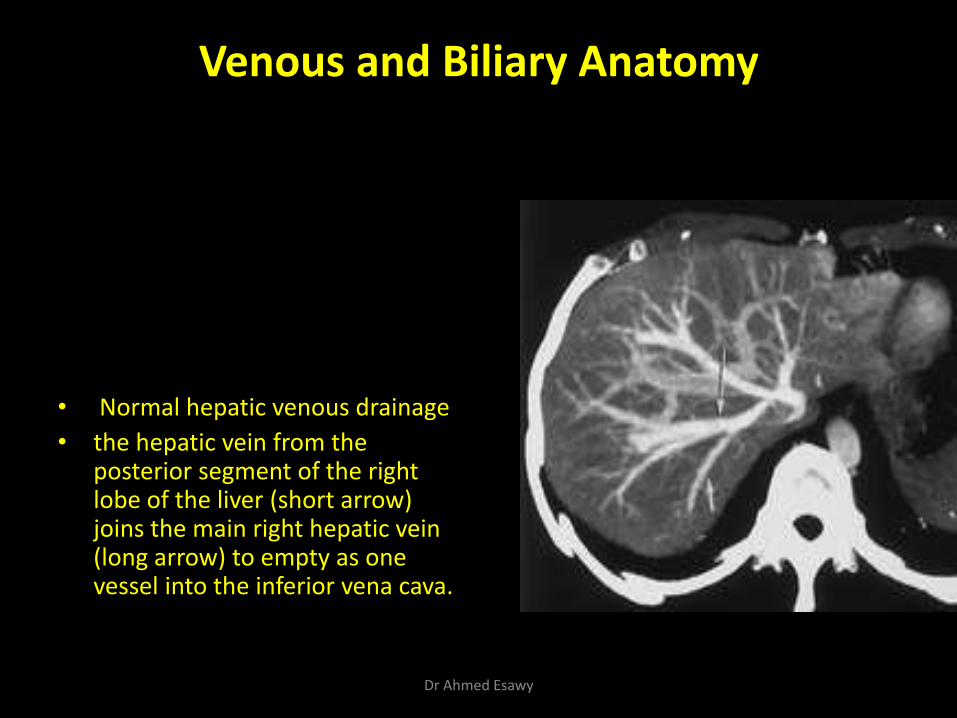
Venous and Biliary Anatomy
• Normal hepatic venous drainage
• the hepatic vein from the posterior segment of the right lobe of the liver (short arrow) joins the main right hepatic vein (long arrow) to empty as one vessel into the inferior vena cava.
Dr Ahmed Esawy
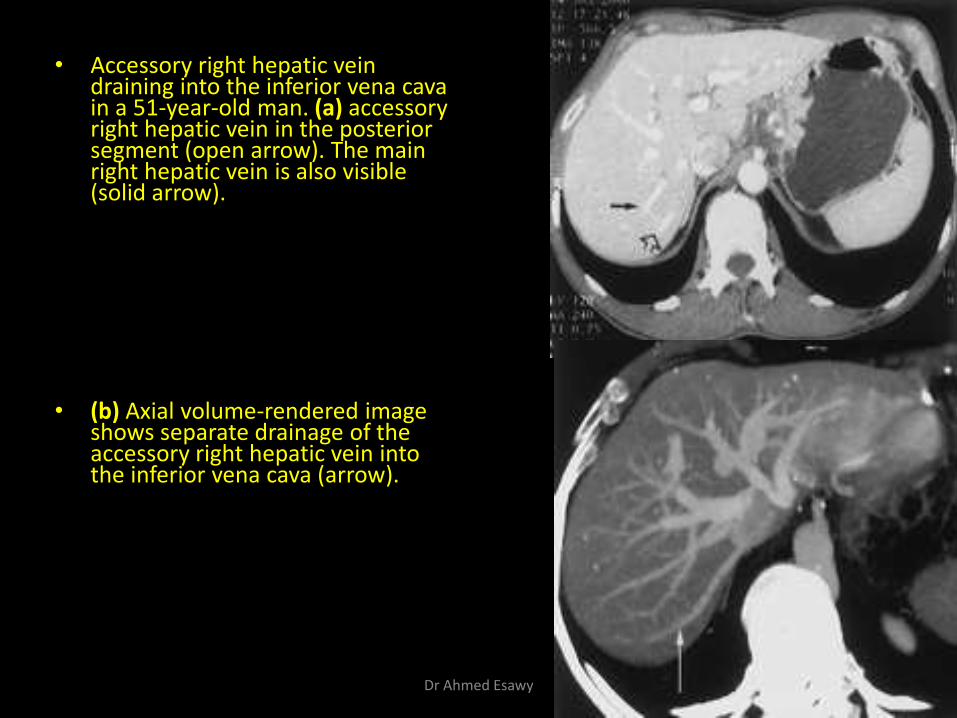
• Accessory right hepatic vein draining into the inferior vena cava in a 51-year-old man. (a) accessory right hepatic vein in the posterior segment (open arrow). The main right hepatic vein is also visible (solid arrow).
• (b) Axial volume-rendered image
shows separate drainage of the accessory right hepatic vein into the inferior vena cava (arrow).
Dr Ahmed Esawy
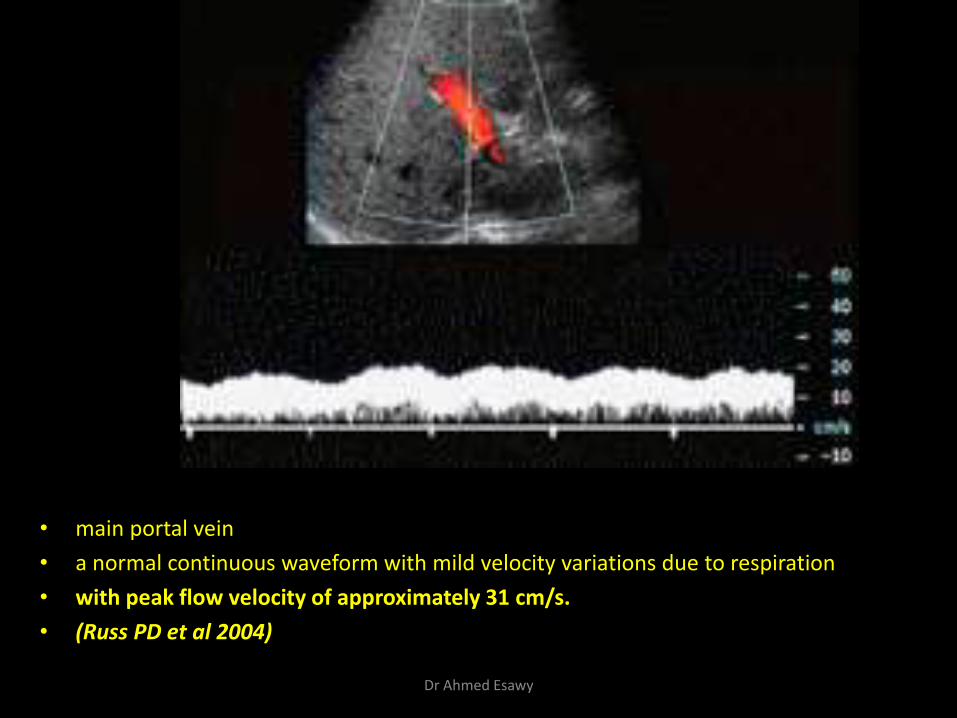
• main portal vein
• a normal continuous waveform with mild velocity variations due to respiration
• with peak flow velocity of approximately 31 cm/s.
• (Russ PD et al 2004)
Dr Ahmed Esawy
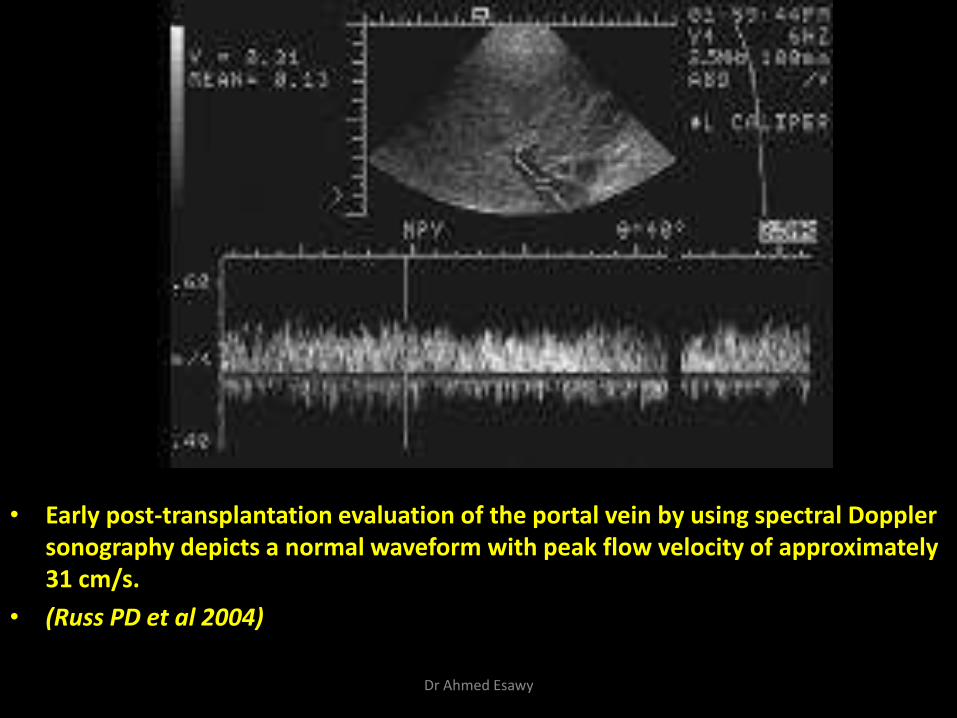
• Early post-transplantation evaluation of the portal vein by using spectral Doppler sonography depicts a normal waveform with peak flow velocity of approximately 31 cm/s.
• (Russ PD et al 2004)
Dr Ahmed Esawy
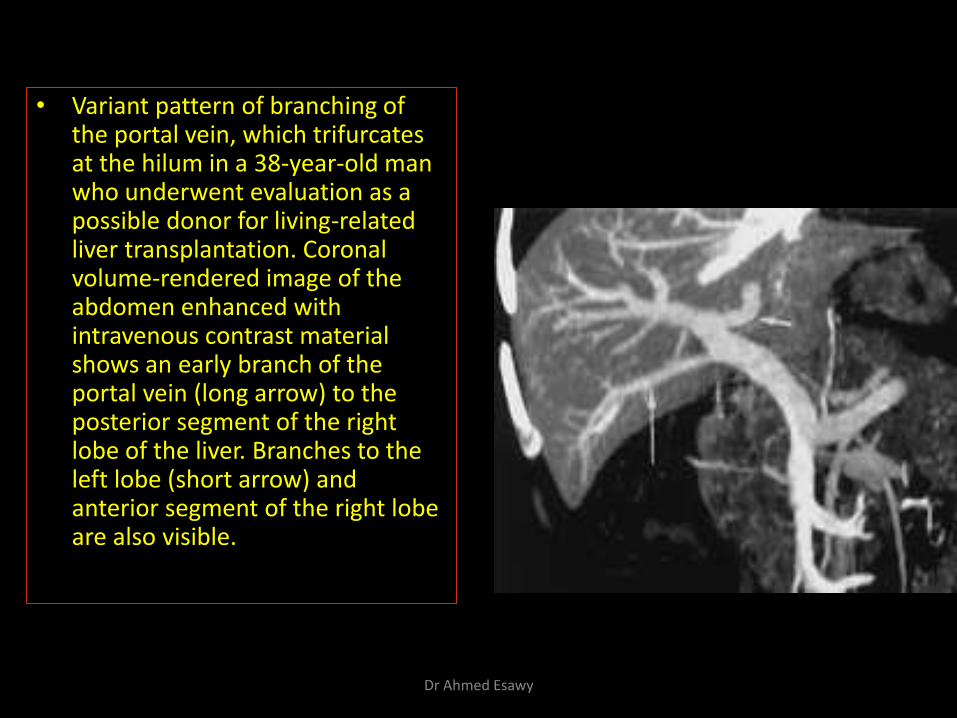
• Variant pattern of branching of the portal vein, which trifurcates at the hilum in a 38-year-old man who underwent evaluation as a possible donor for living-related liver transplantation. Coronal volume-rendered image of the abdomen enhanced with intravenous contrast material shows an early branch of the portal vein (long arrow) to the posterior segment of the right lobe of the liver. Branches to the left lobe (short arrow) and anterior segment of the right lobe are also visible.
Dr Ahmed Esawy
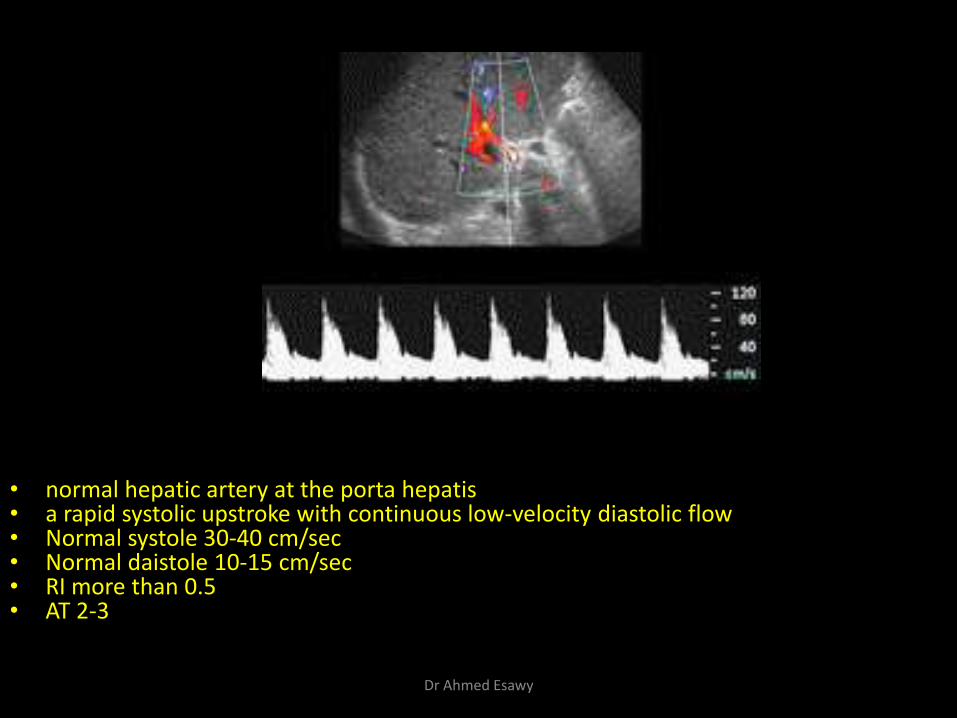
• normal hepatic artery at the porta hepatis • a rapid systolic upstroke with continuous low-velocity diastolic flow • Normal systole 30-40 cm/sec • Normal daistole 10-15 cm/sec • RI more than 0.5 • AT 2-3
Dr Ahmed Esawy
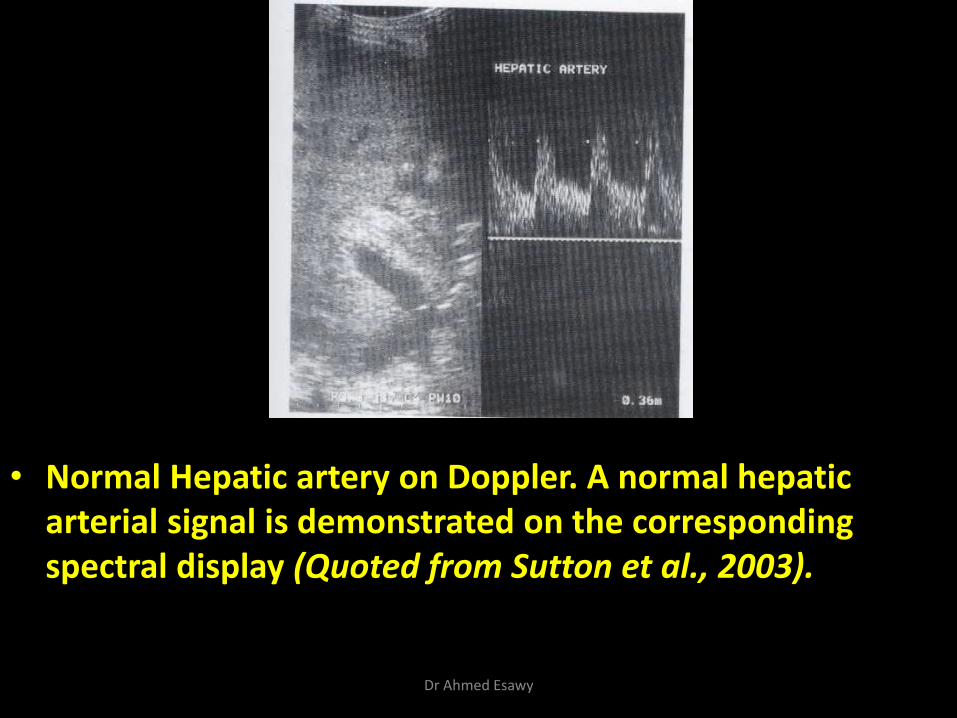
• Normal Hepatic artery on Doppler. A normal hepatic arterial signal is demonstrated on the corresponding spectral display (Quoted from Sutton et al., 2003).
Dr Ahmed Esawy
HEPATIC ARTERY
Dr Ahmed Esawy
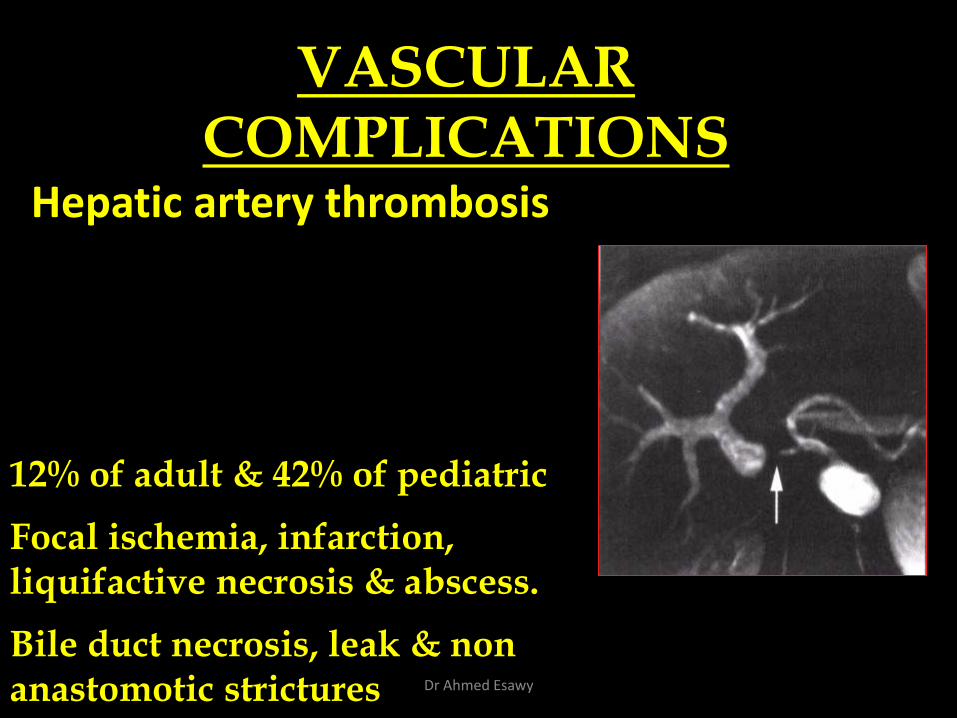
Hepatic artery thrombosis
VASCULAR COMPLICATIONS
12% of adult & 42% of pediatric
Focal ischemia, infarction, liquifactive necrosis & abscess.
Bile duct necrosis, leak & non anastomotic strictures Dr Ahmed Esawy
VASCULAR COMPLICATIONS
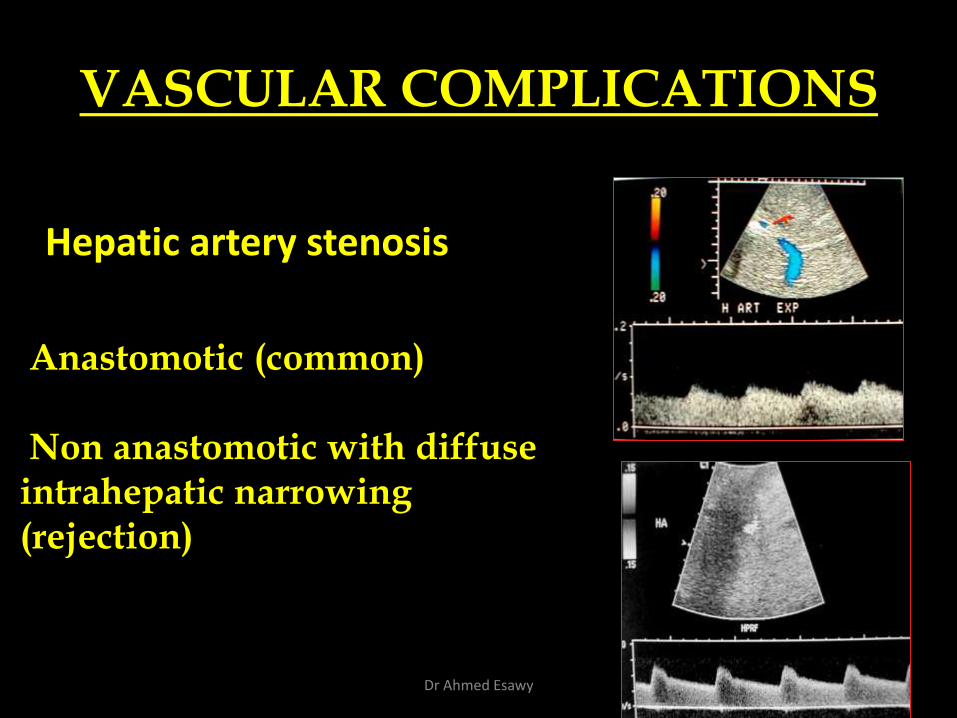
Hepatic artery stenosis
Anastomotic (common) Non anastomotic with diffuse intrahepatic narrowing (rejection)
Dr Ahmed Esawy
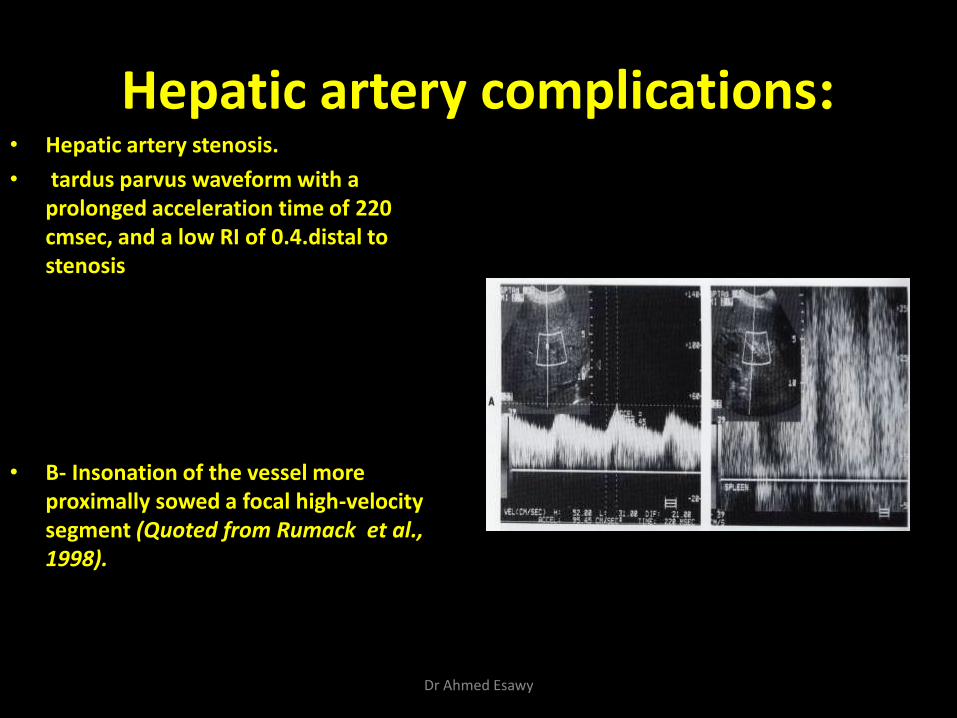
Hepatic artery complications: • Hepatic artery stenosis.
• tardus parvus waveform with a prolonged acceleration time of 220 cmsec, and a low RI of 0.4.distal to stenosis
• B- Insonation of the vessel more proximally sowed a focal high-velocity segment (Quoted from Rumack et al., 1998).
Dr Ahmed Esawy
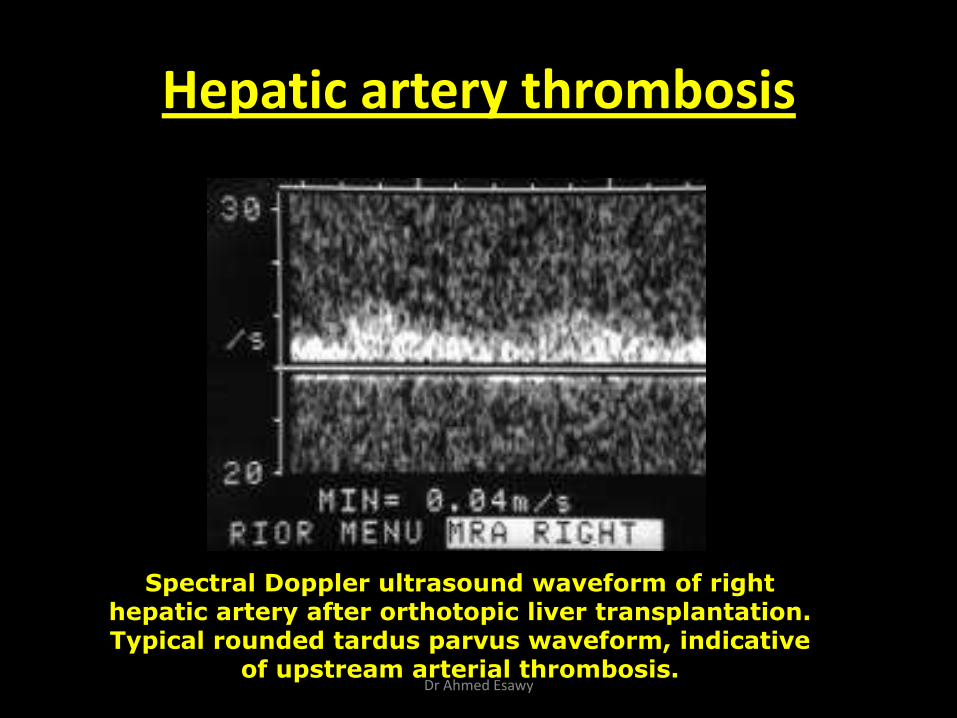
Hepatic artery thrombosis
Spectral Doppler ultrasound waveform of right hepatic artery after orthotopic liver transplantation. Typical rounded tardus parvus waveform, indicative
of upstream arterial thrombosis. Dr Ahmed Esawy
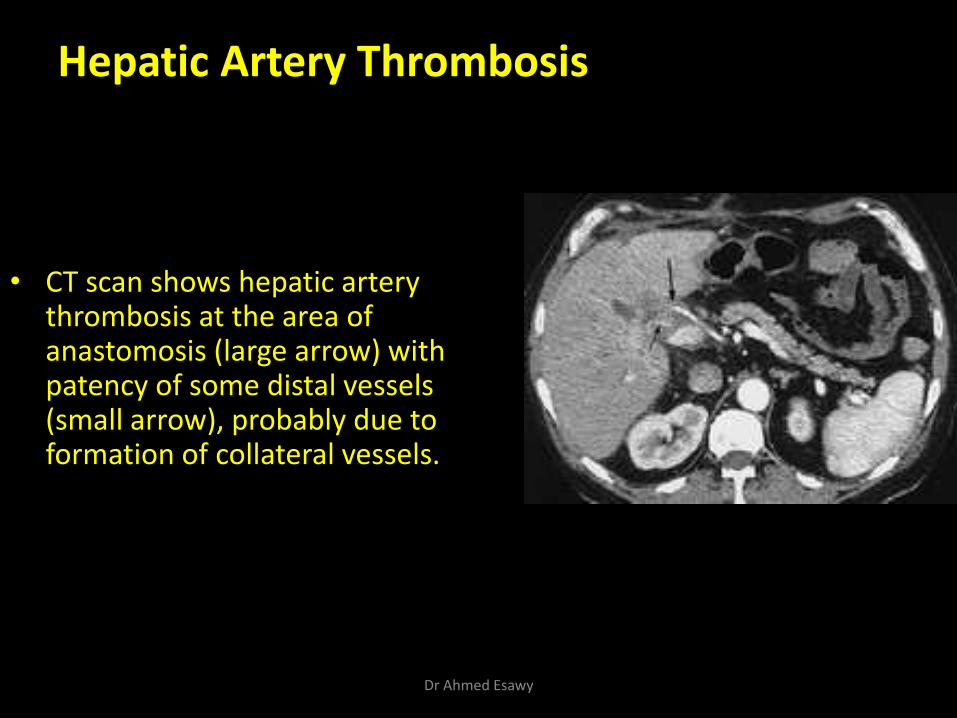
Hepatic Artery Thrombosis
• CT scan shows hepatic artery thrombosis at the area of anastomosis (large arrow) with patency of some distal vessels (small arrow), probably due to formation of collateral vessels.
Dr Ahmed Esawy
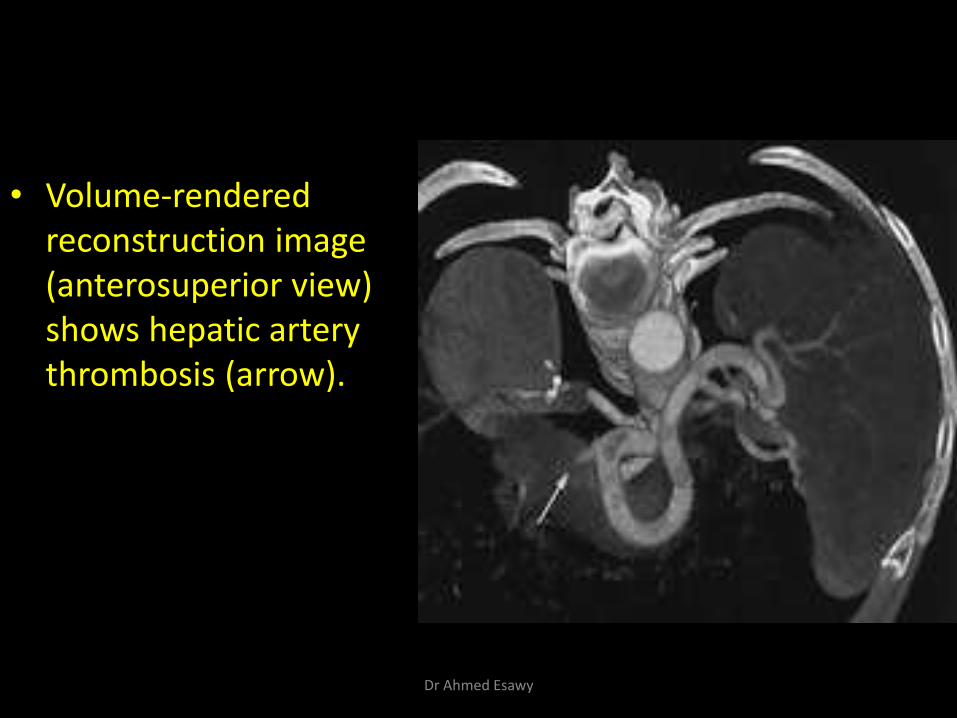
• Volume-rendered reconstruction image (anterosuperior view) shows hepatic artery thrombosis (arrow).
Dr Ahmed Esawy
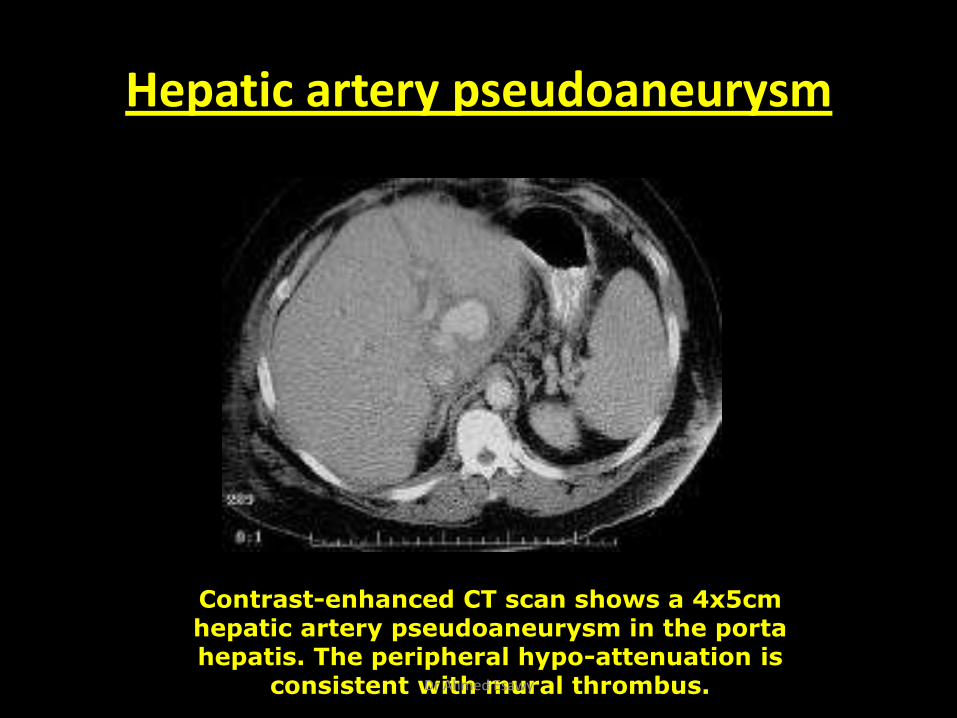
Hepatic artery pseudoaneurysm
Contrast-enhanced CT scan shows a 4x5cm hepatic artery pseudoaneurysm in the porta hepatis. The peripheral hypo-attenuation is
consistent with mural thrombus. Dr Ahmed Esawy
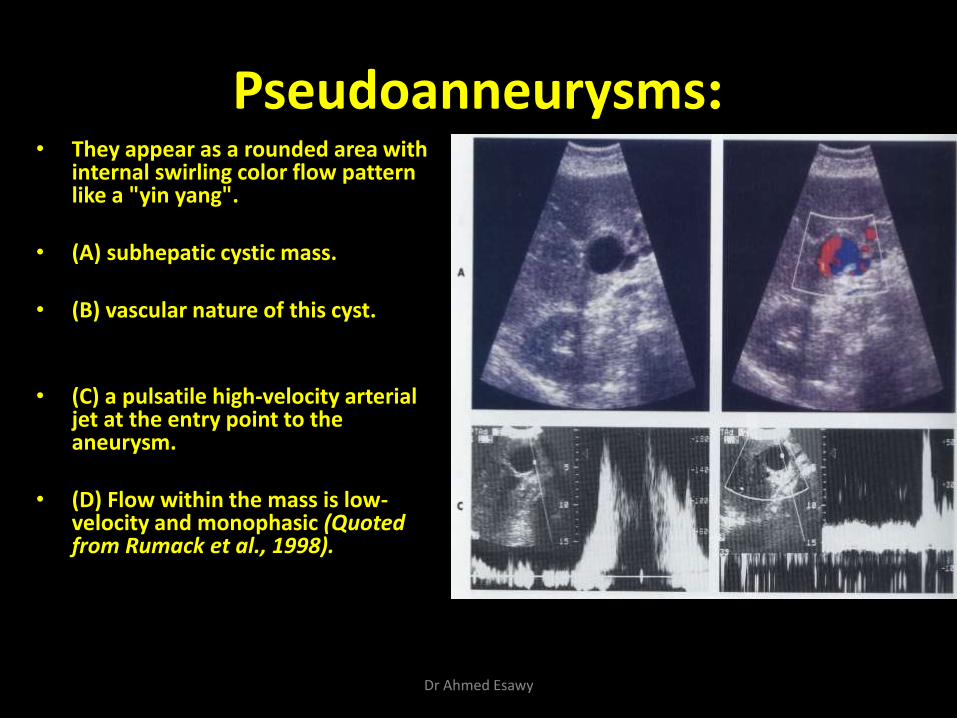
Pseudoanneurysms: • They appear as a rounded area with
internal swirling color flow pattern like a "yin yang".
• (A) subhepatic cystic mass.
• (B) vascular nature of this cyst.
• (C) a pulsatile high-velocity arterial jet at the entry point to the aneurysm.
• (D) Flow within the mass is low-velocity and monophasic (Quoted from Rumack et al., 1998).
Dr Ahmed Esawy
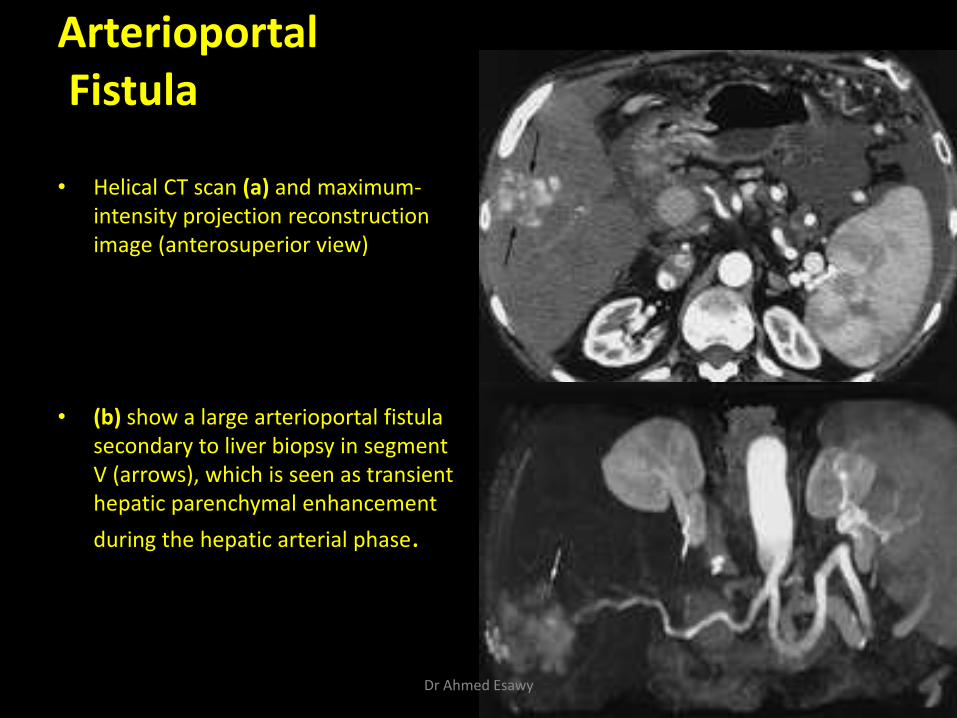
Arterioportal Fistula
• Helical CT scan (a) and maximum-
intensity projection reconstruction image (anterosuperior view)
• (b) show a large arterioportal fistula secondary to liver biopsy in segment V (arrows), which is seen as transient hepatic parenchymal enhancement
during the hepatic arterial phase.
Dr Ahmed Esawy
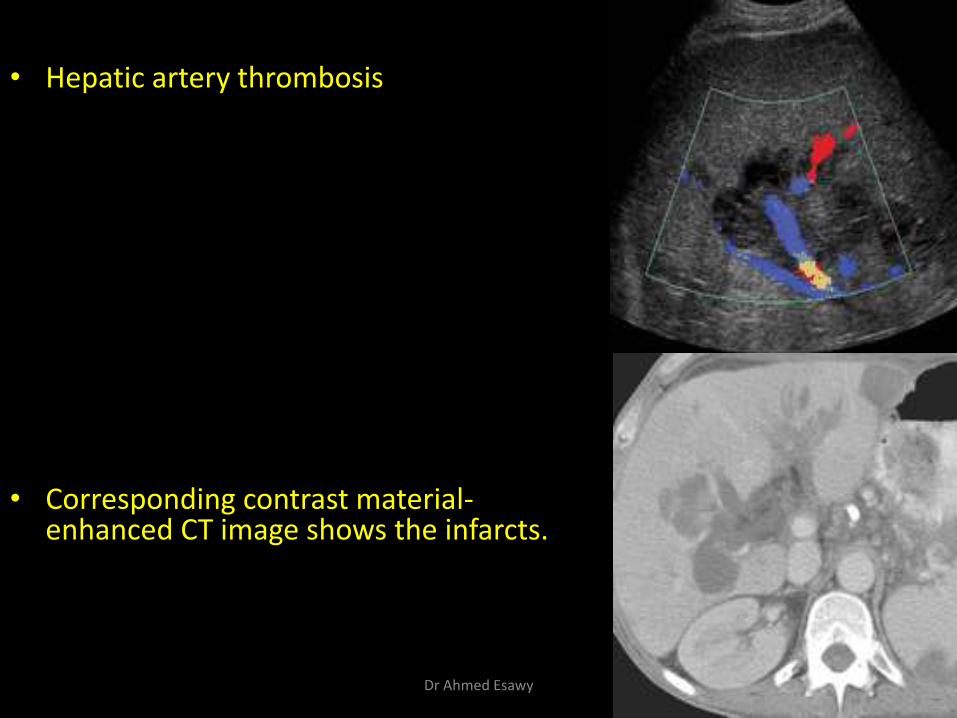
• Hepatic artery thrombosis
• Corresponding contrast material-enhanced CT image shows the infarcts.
Dr Ahmed Esawy
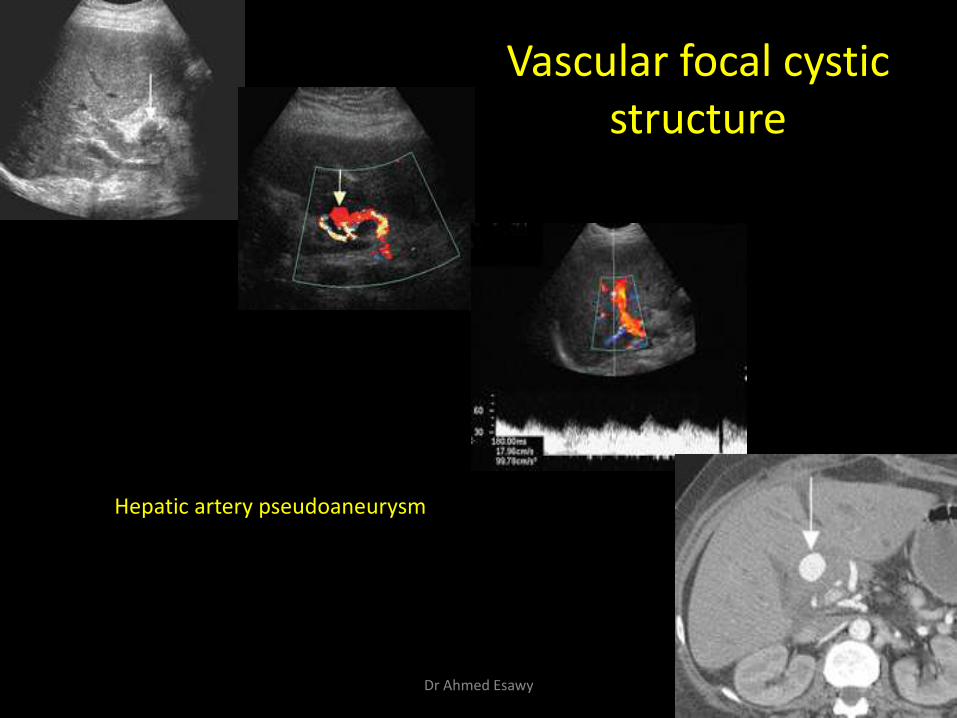
Vascular focal cystic structure
Hepatic artery pseudoaneurysm
Dr Ahmed Esawy

Hepatic infarction following hepatic arterial thrombosis
Dr Ahmed Esawy
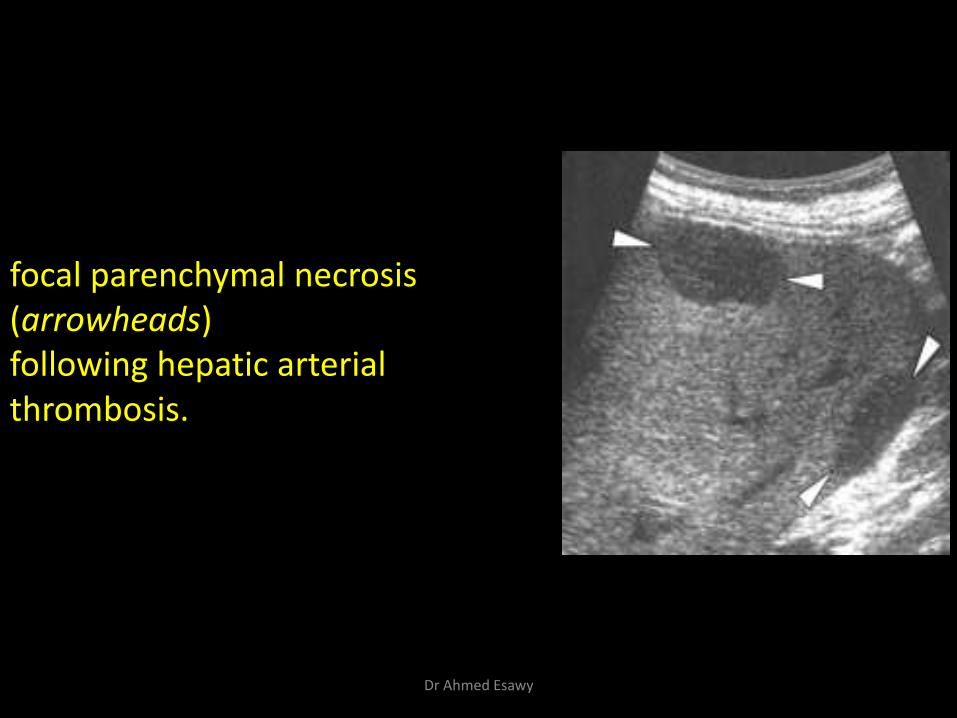
focal parenchymal necrosis (arrowheads) following hepatic arterial thrombosis.
Dr Ahmed Esawy
PORTAL VEIN
Dr Ahmed Esawy
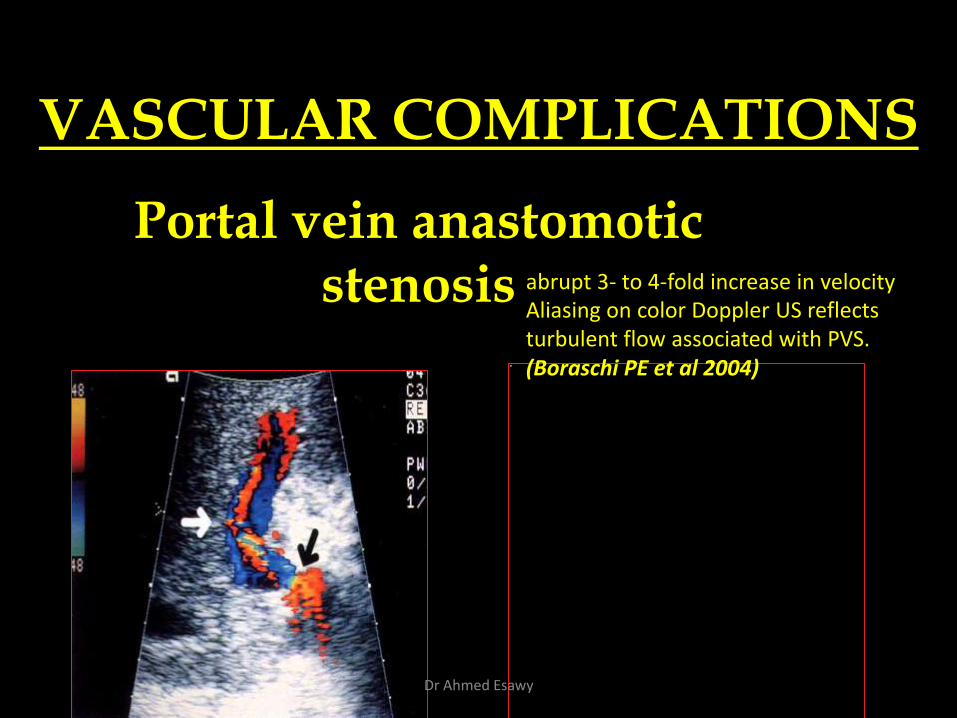
VASCULAR COMPLICATIONS
Portal vein anastomotic stenosis abrupt 3- to 4-fold increase in velocity
Aliasing on color Doppler US reflects turbulent flow associated with PVS. (Boraschi PE et al 2004)
Dr Ahmed Esawy
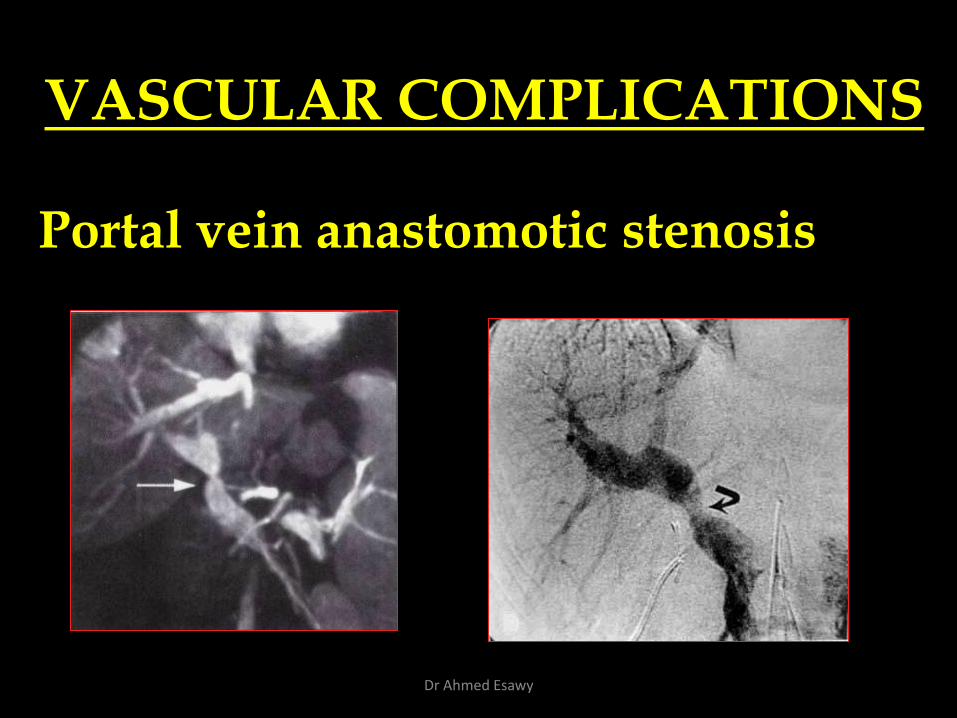
VASCULAR COMPLICATIONS
Portal vein anastomotic stenosis
Dr Ahmed Esawy
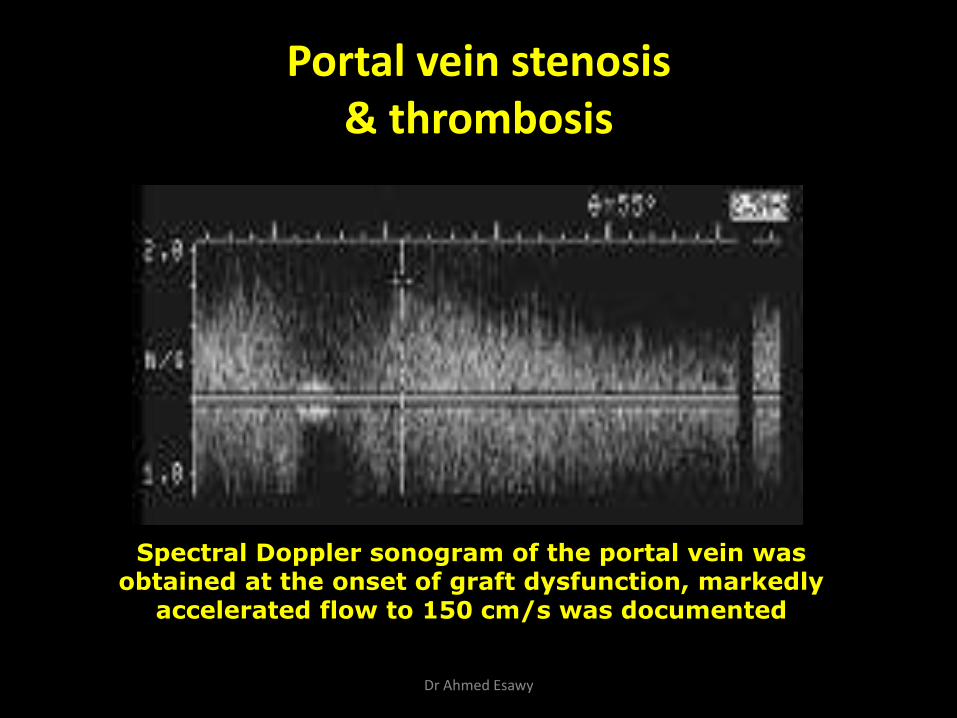
Portal vein stenosis & thrombosis
Spectral Doppler sonogram of the portal vein was obtained at the onset of graft dysfunction, markedly
accelerated flow to 150 cm/s was documented
Dr Ahmed Esawy
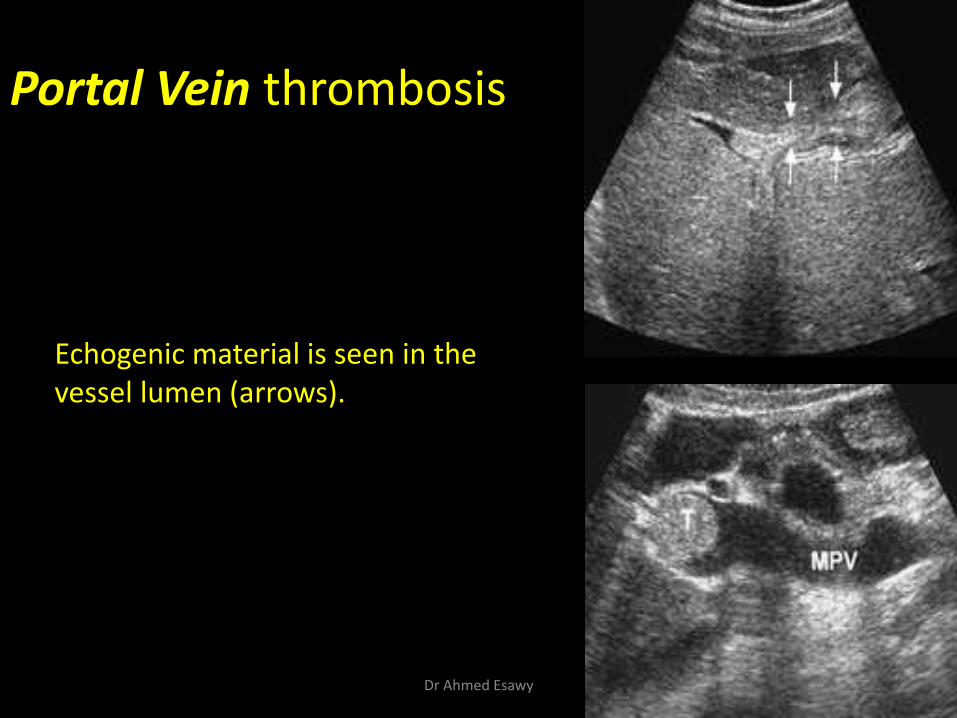
Portal Vein thrombosis
Echogenic material is seen in the vessel lumen (arrows).
Dr Ahmed Esawy
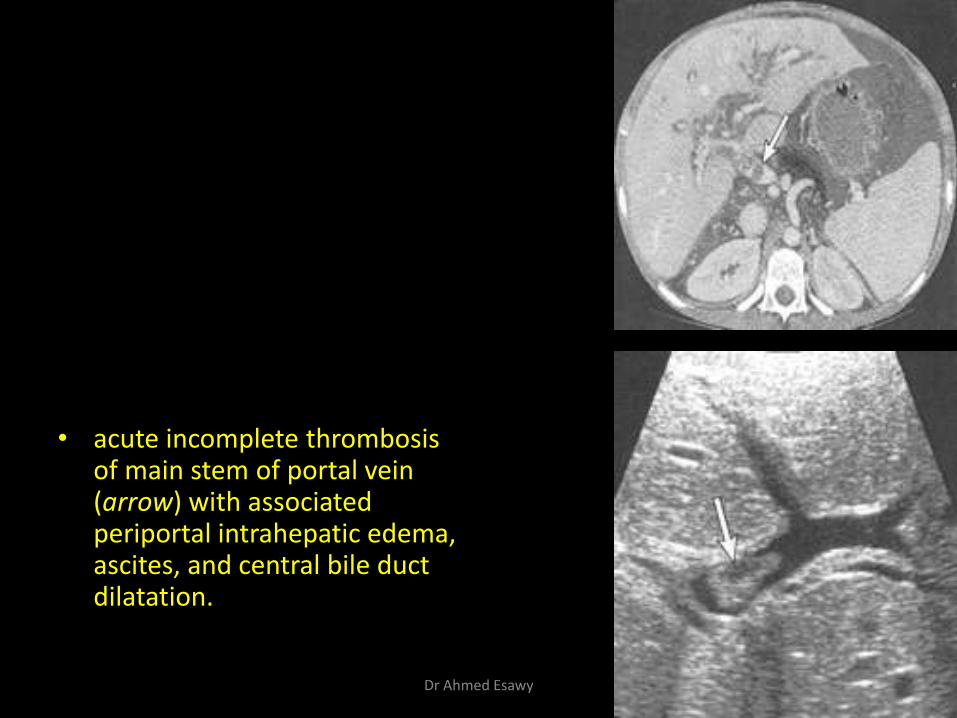
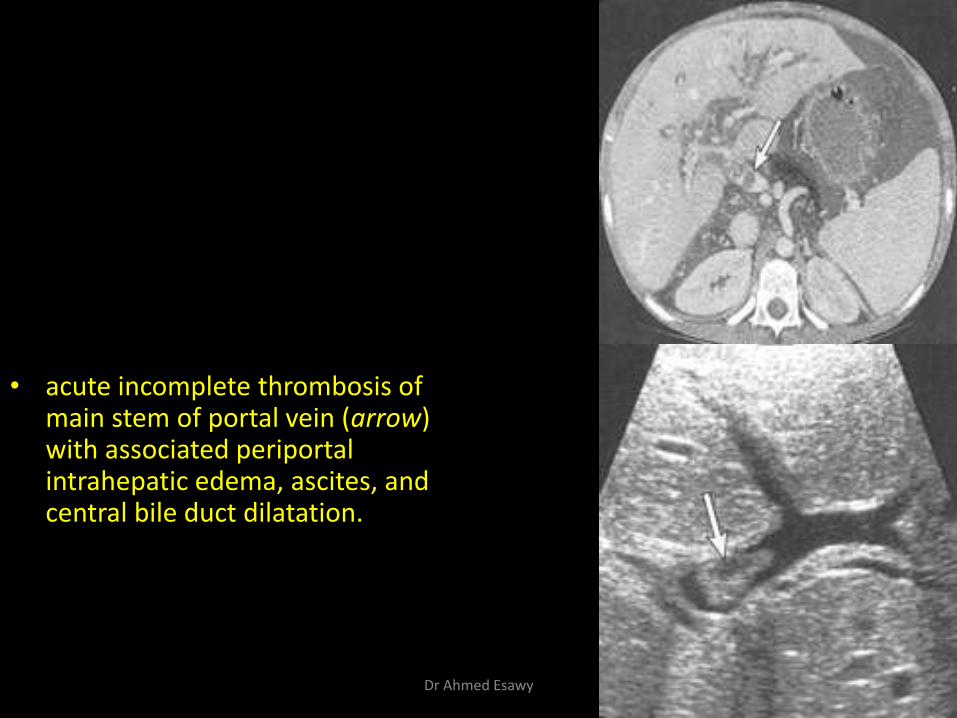
• acute incomplete thrombosis of main stem of portal vein (arrow) with associated periportal intrahepatic edema, ascites, and central bile duct dilatation.
Dr Ahmed Esawy
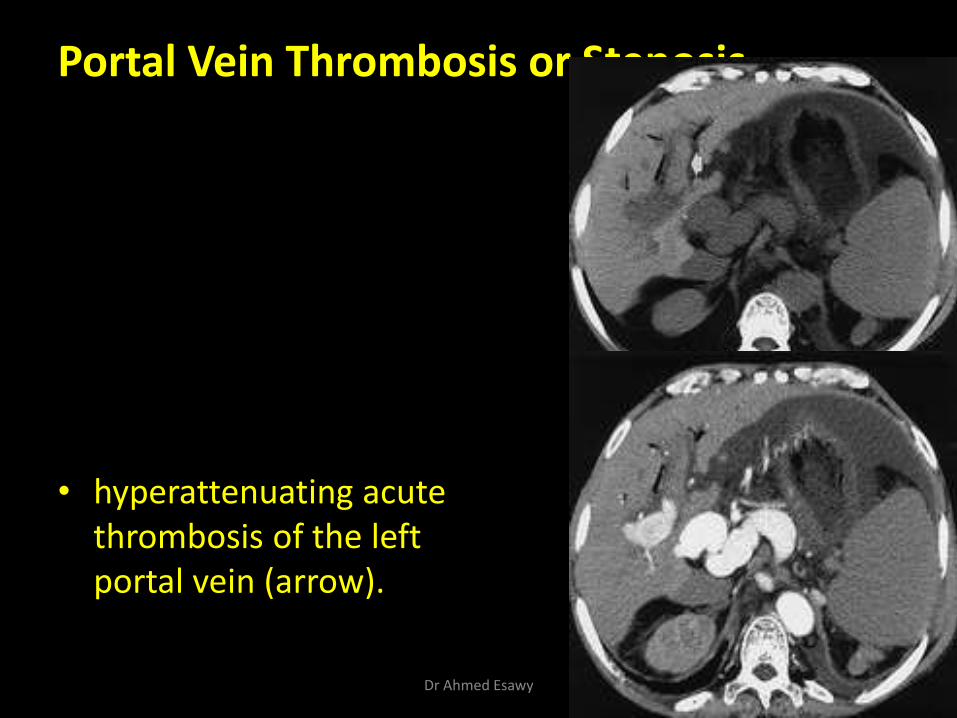
Portal Vein Thrombosis or Stenosis
• hyperattenuating acute thrombosis of the left portal vein (arrow).
Dr Ahmed Esawy
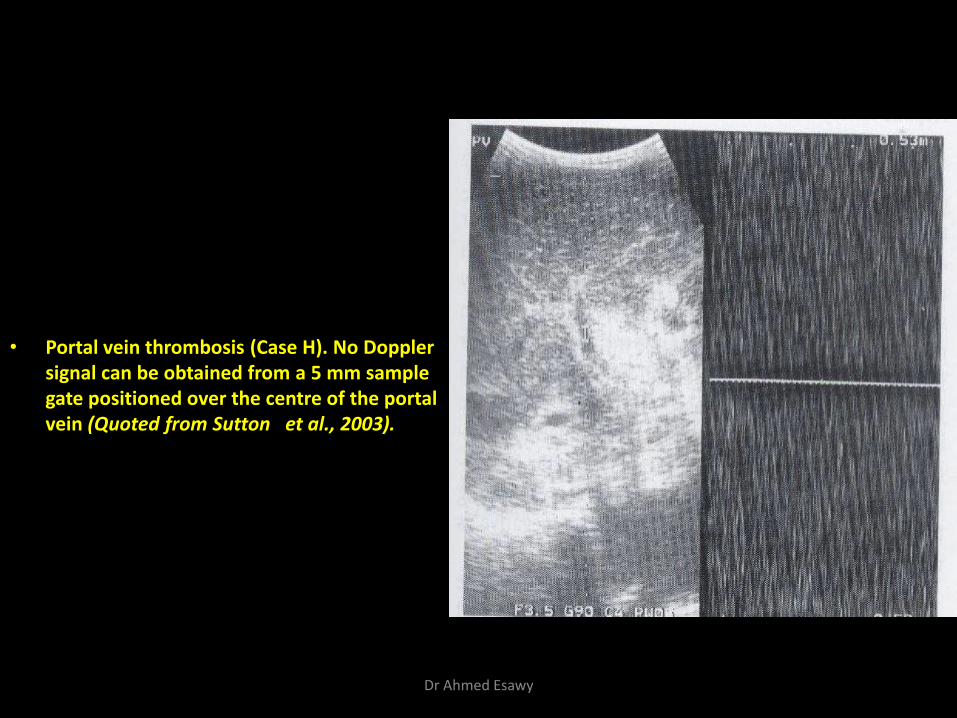
• Portal vein thrombosis (Case H). No Doppler signal can be obtained from a 5 mm sample gate positioned over the centre of the portal vein (Quoted from Sutton et al., 2003).
Dr Ahmed Esawy
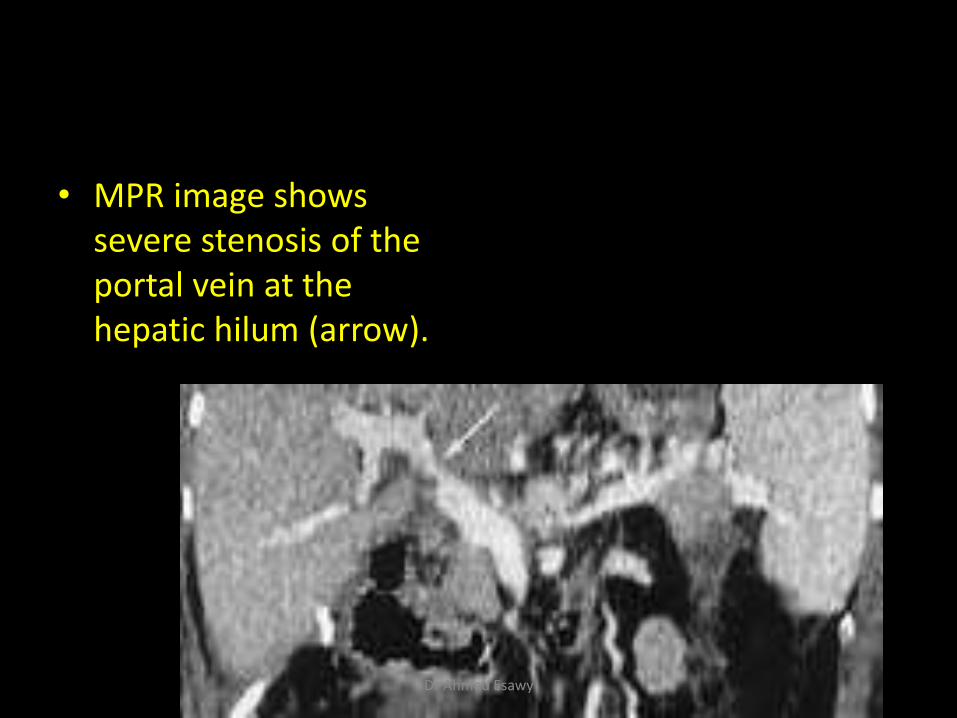
• MPR image shows severe stenosis of the portal vein at the hepatic hilum (arrow).
Dr Ahmed Esawy
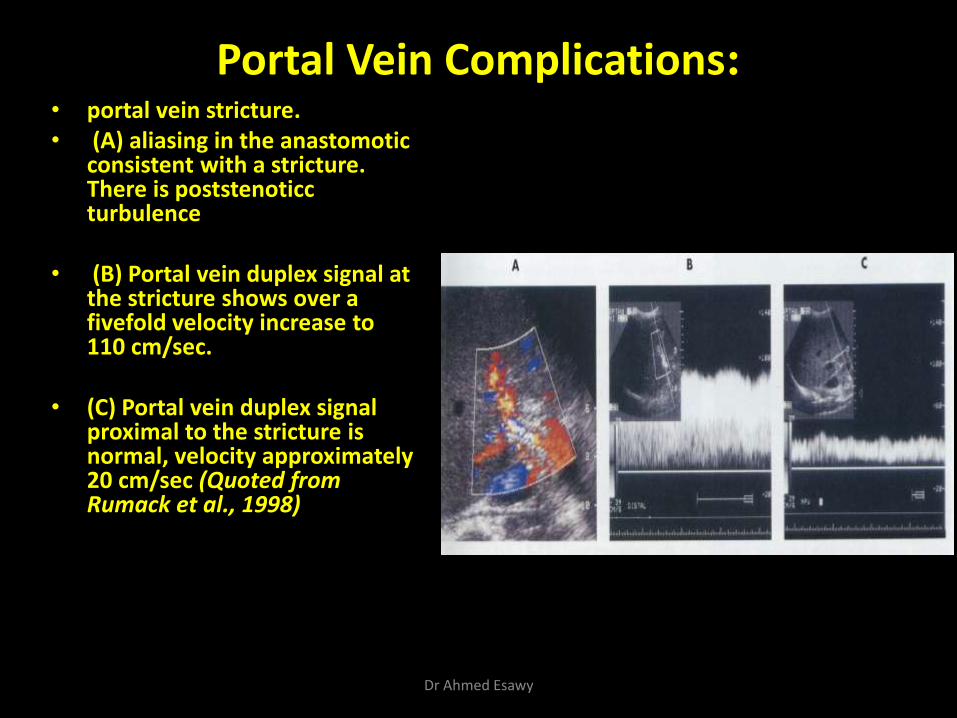
Portal Vein Complications: • portal vein stricture. • (A) aliasing in the anastomotic
consistent with a stricture. There is poststenoticc turbulence
• (B) Portal vein duplex signal at the stricture shows over a fivefold velocity increase to 110 cm/sec.
• (C) Portal vein duplex signal proximal to the stricture is normal, velocity approximately 20 cm/sec (Quoted from Rumack et al., 1998)
Dr Ahmed Esawy
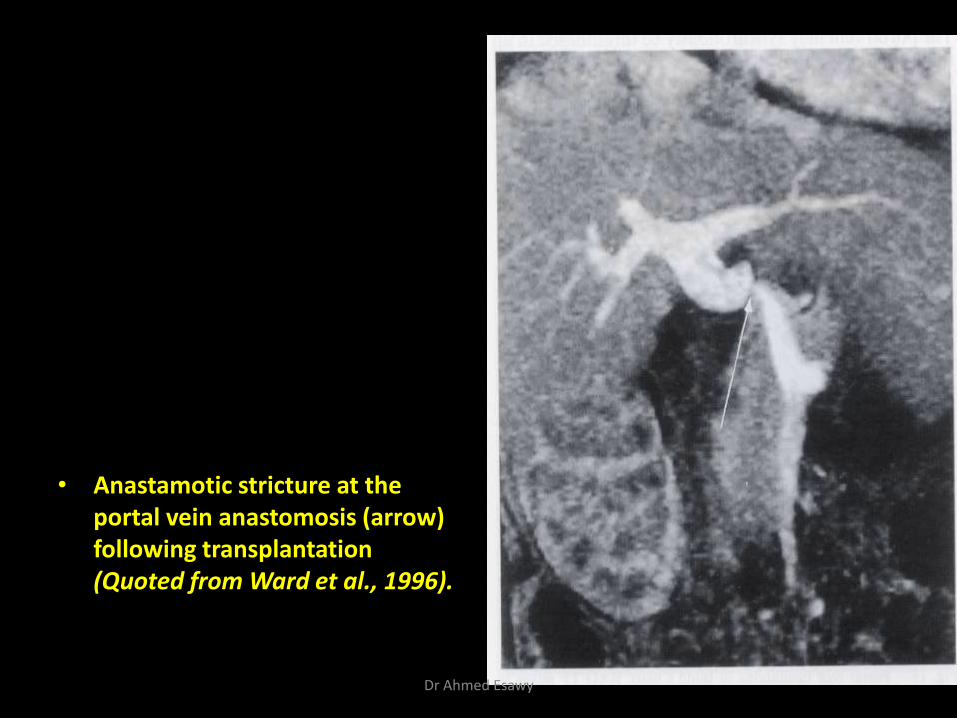
• Anastamotic stricture at the portal vein anastomosis (arrow) following transplantation (Quoted from Ward et al., 1996).
Dr Ahmed Esawy
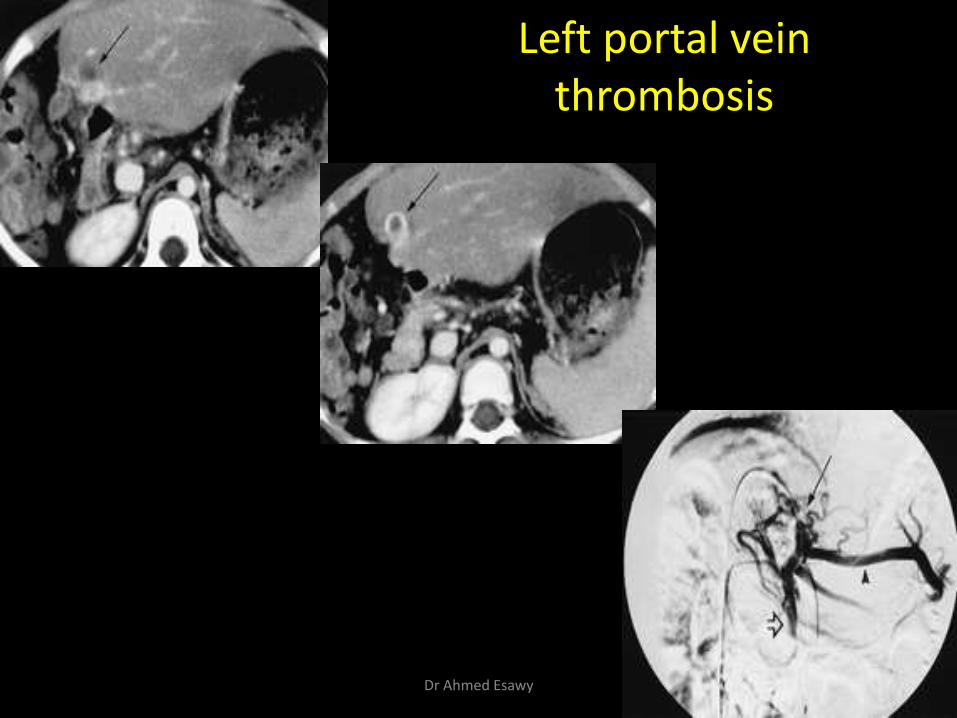
Left portal vein thrombosis
Dr Ahmed Esawy
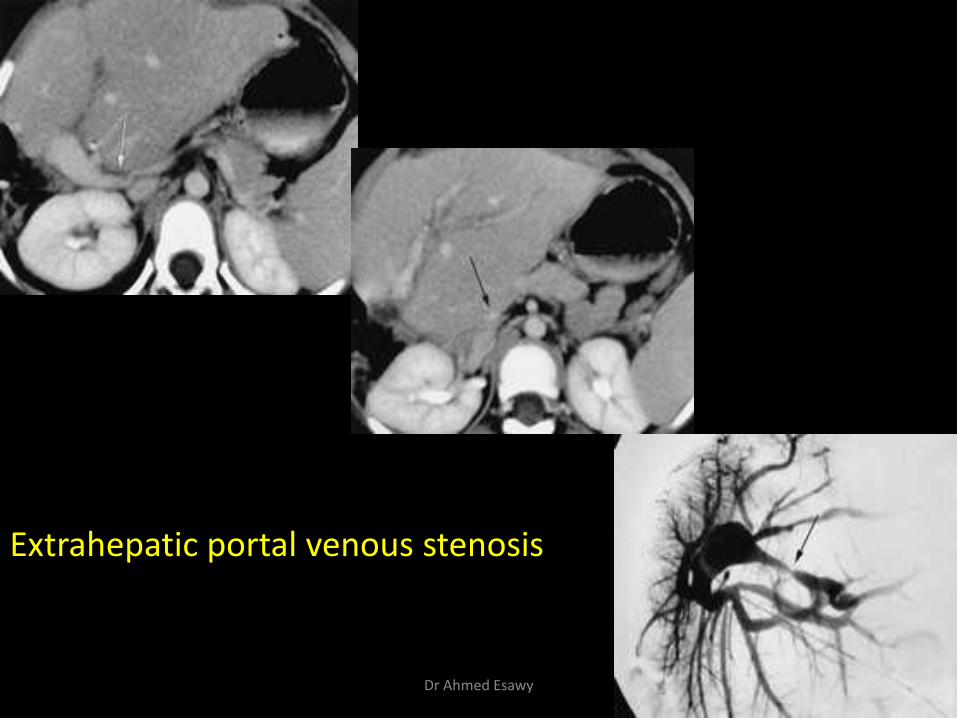
Extrahepatic portal venous stenosis
Dr Ahmed Esawy
• acute incomplete thrombosis of main stem of portal vein (arrow) with associated periportal intrahepatic edema, ascites, and central bile duct dilatation.
Dr Ahmed Esawy

Dr Ahmed Esawy
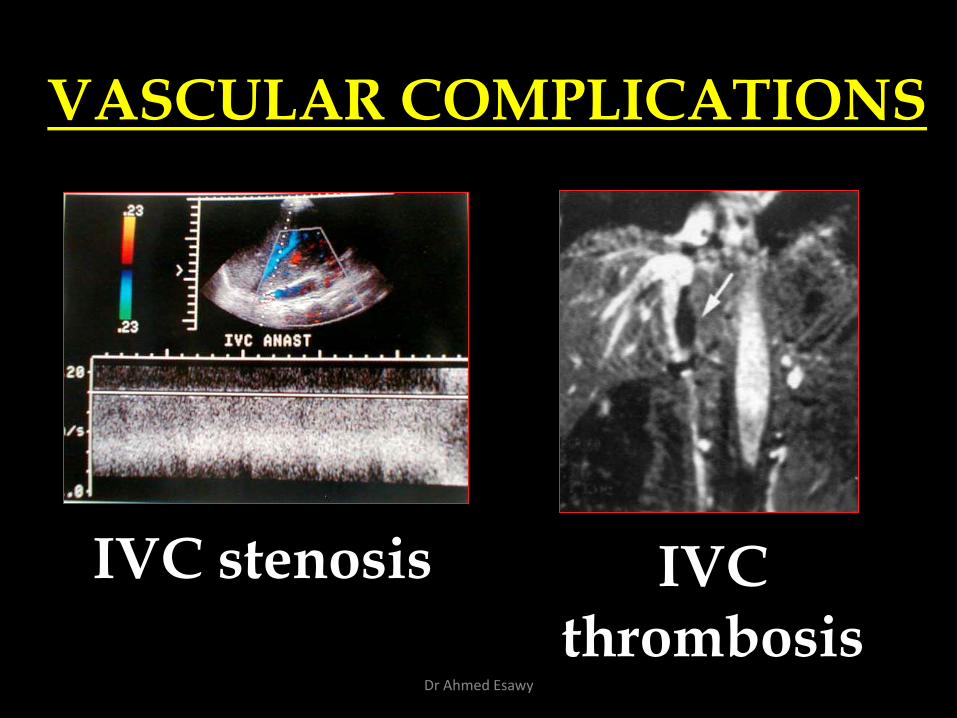
VASCULAR COMPLICATIONS
IVC stenosis IVC thrombosis
Dr Ahmed Esawy
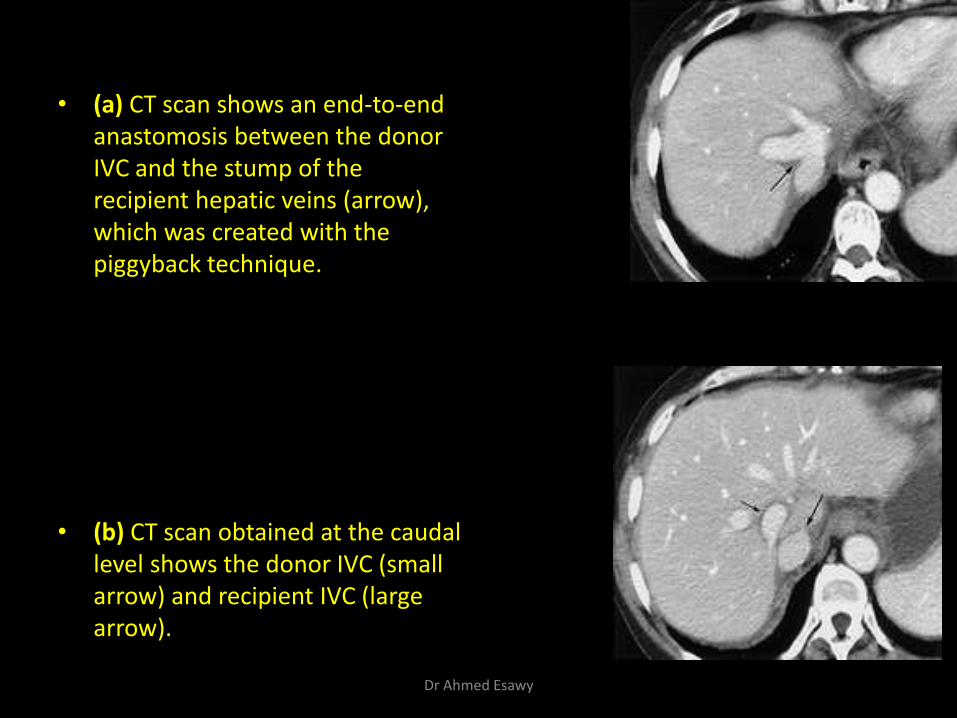
• (a) CT scan shows an end-to-end anastomosis between the donor IVC and the stump of the recipient hepatic veins (arrow), which was created with the piggyback technique.
• (b) CT scan obtained at the caudal level shows the donor IVC (small arrow) and recipient IVC (large arrow).
Dr Ahmed Esawy
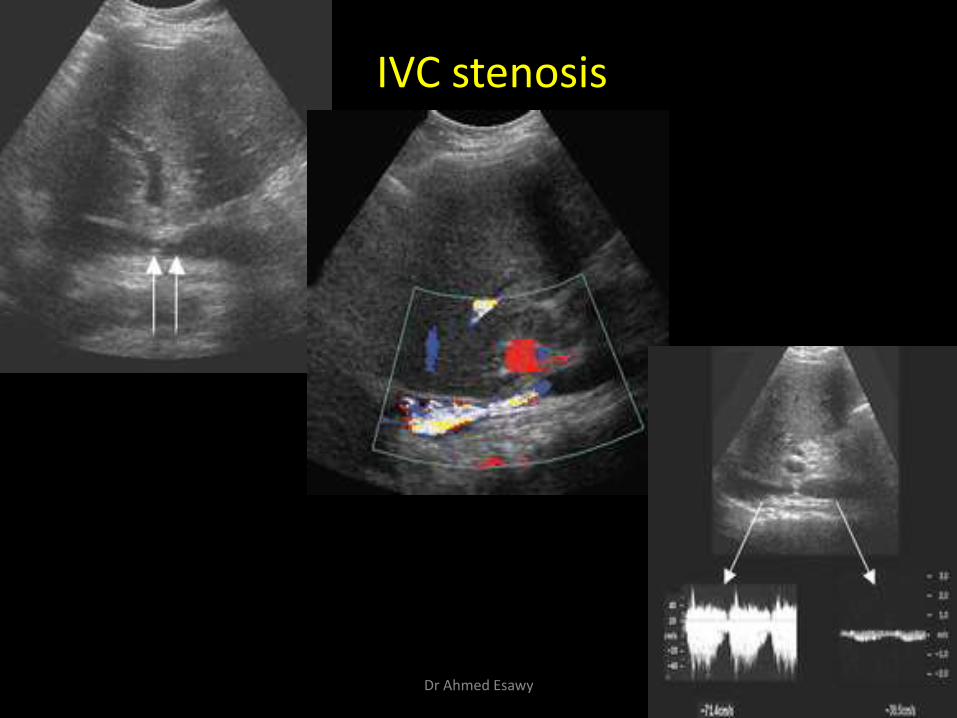
IVC stenosis
Dr Ahmed Esawy
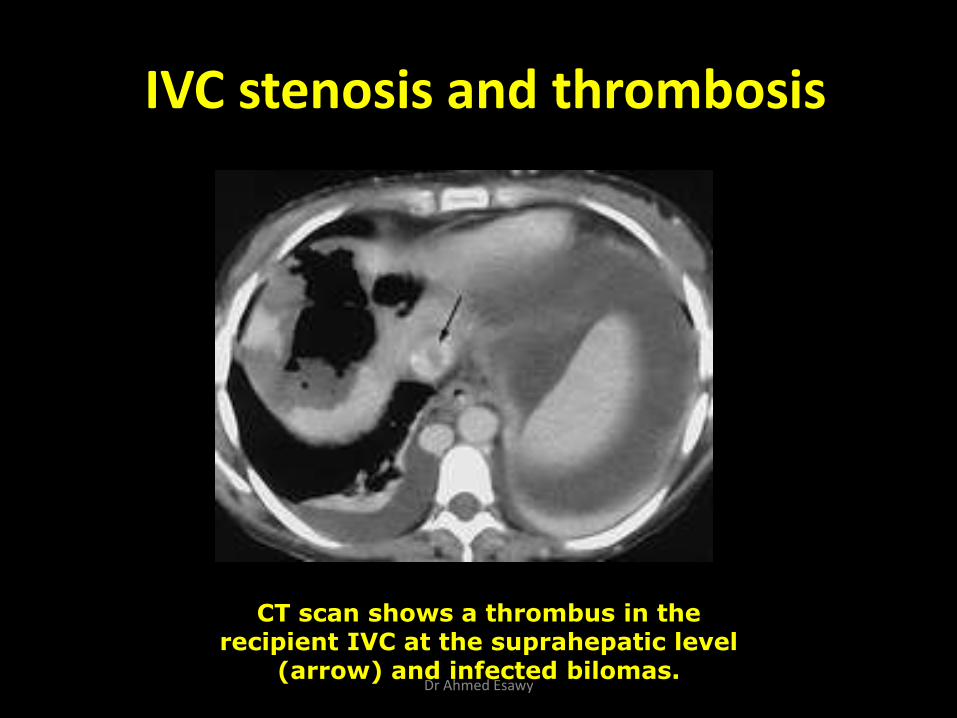
IVC stenosis and thrombosis
CT scan shows a thrombus in the recipient IVC at the suprahepatic level
(arrow) and infected bilomas. Dr Ahmed Esawy
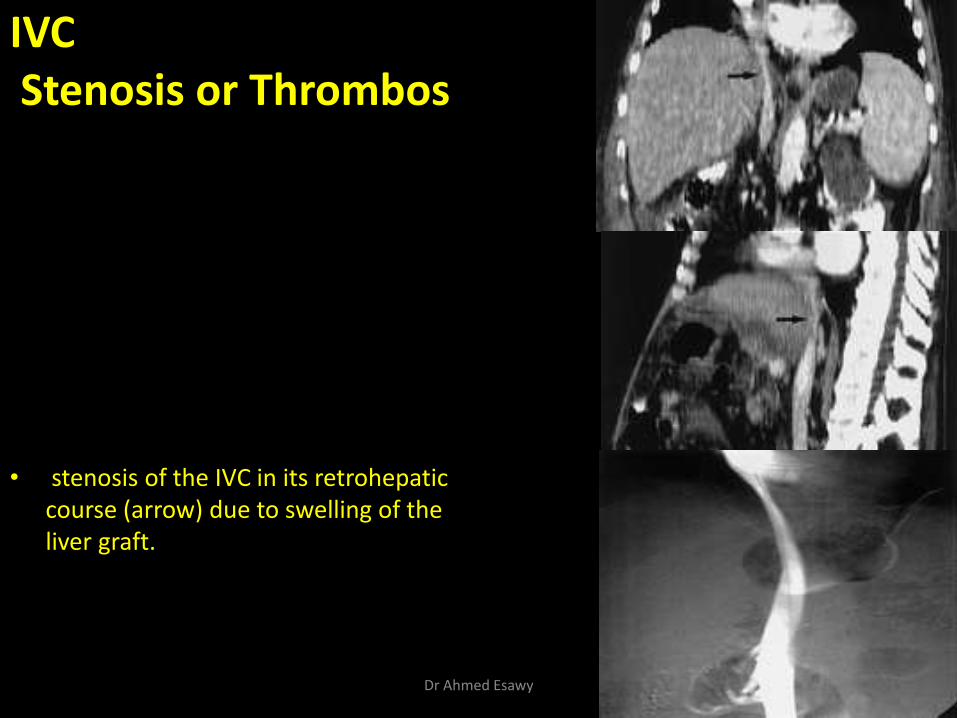
IVC Stenosis or Thrombos
• stenosis of the IVC in its retrohepatic course (arrow) due to swelling of the liver graft.
Dr Ahmed Esawy
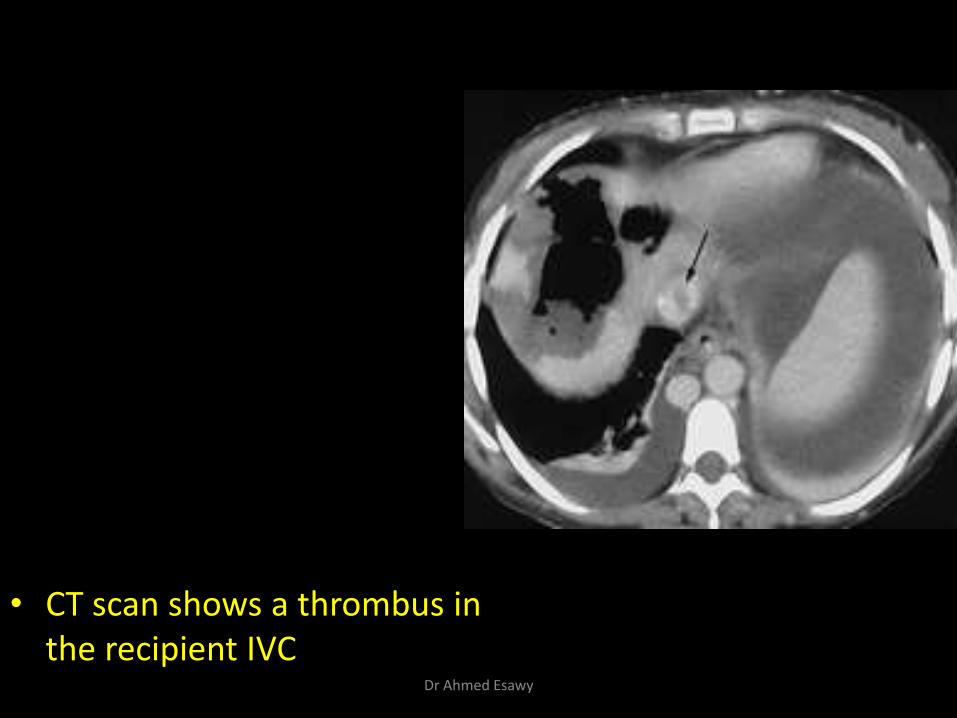
• CT scan shows a thrombus in the recipient IVC
Dr Ahmed Esawy
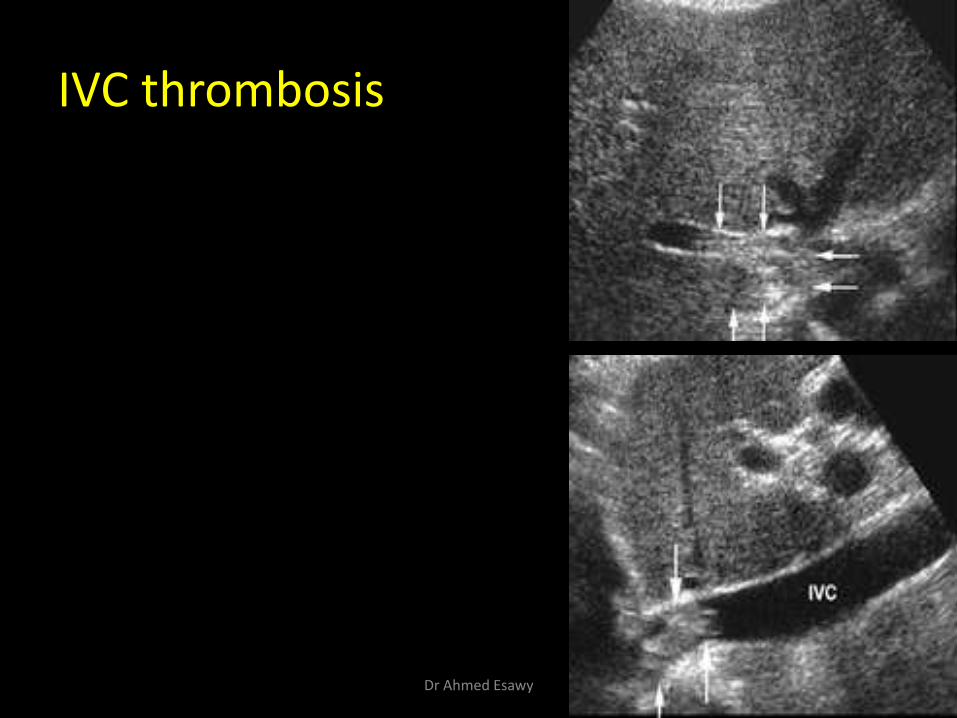
IVC thrombosis
Dr Ahmed Esawy
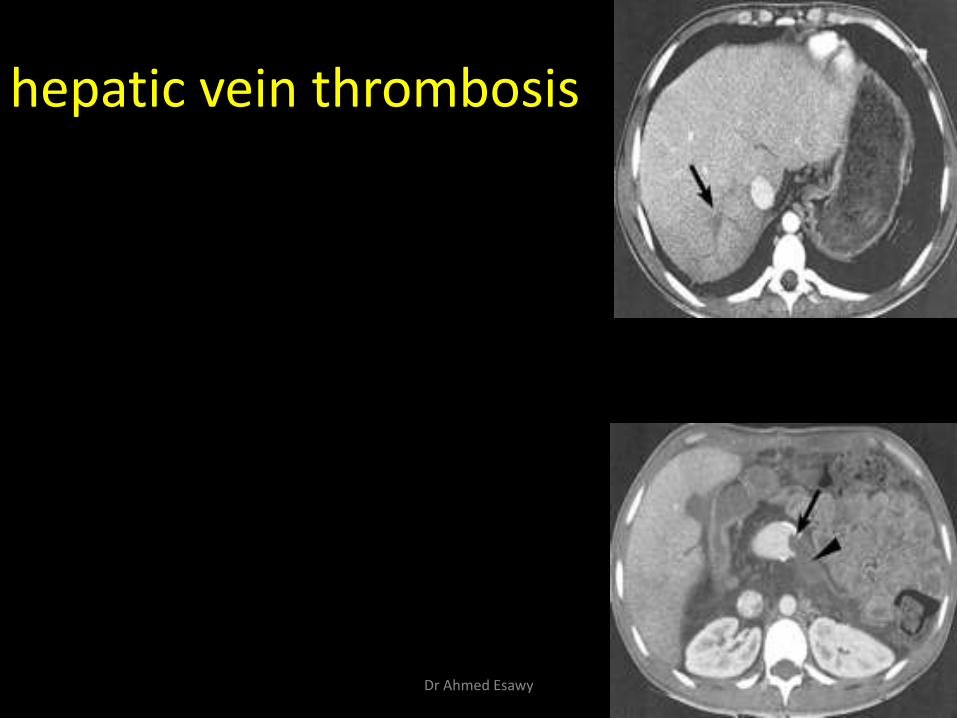
hepatic vein thrombosis
Dr Ahmed Esawy
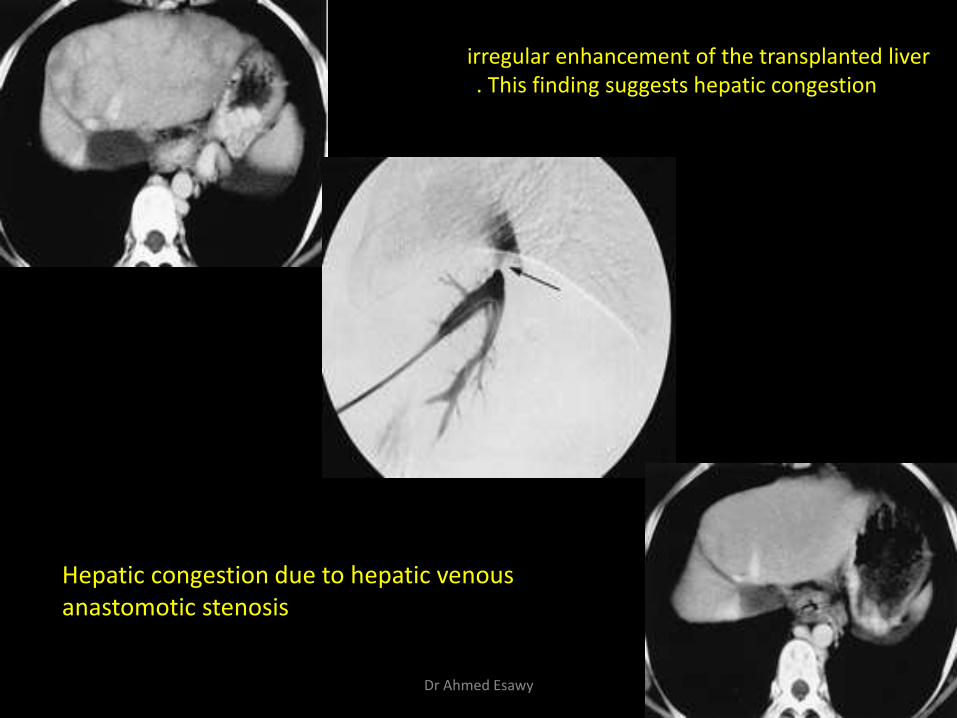
irregular enhancement of the transplanted liver . This finding suggests hepatic congestion
Hepatic congestion due to hepatic venous anastomotic stenosis
Dr Ahmed Esawy
2- Biliary complications : (i) Biliary duct obstruction (due to stricture
anastomotic or nonanastomotic.
(ii) Bile leak.
(iii) other rare biliary complications).
(IV) dysfunction of the sphincter of Oddi
• (V) Bile duct Ischemia
Dr Ahmed Esawy
Biliary Tract Complications
Obstruction Dilatation
Leak Strictures
Bile Duct Ischemia
Dr Ahmed Esawy
Biliary Obstruction Strictures
T-tube stent dysfunction
kinking of extrahepatic ducts
cystic duct mucocele
biliary sludge or stones
BILIARY COMPLICATIONS
Dr Ahmed Esawy
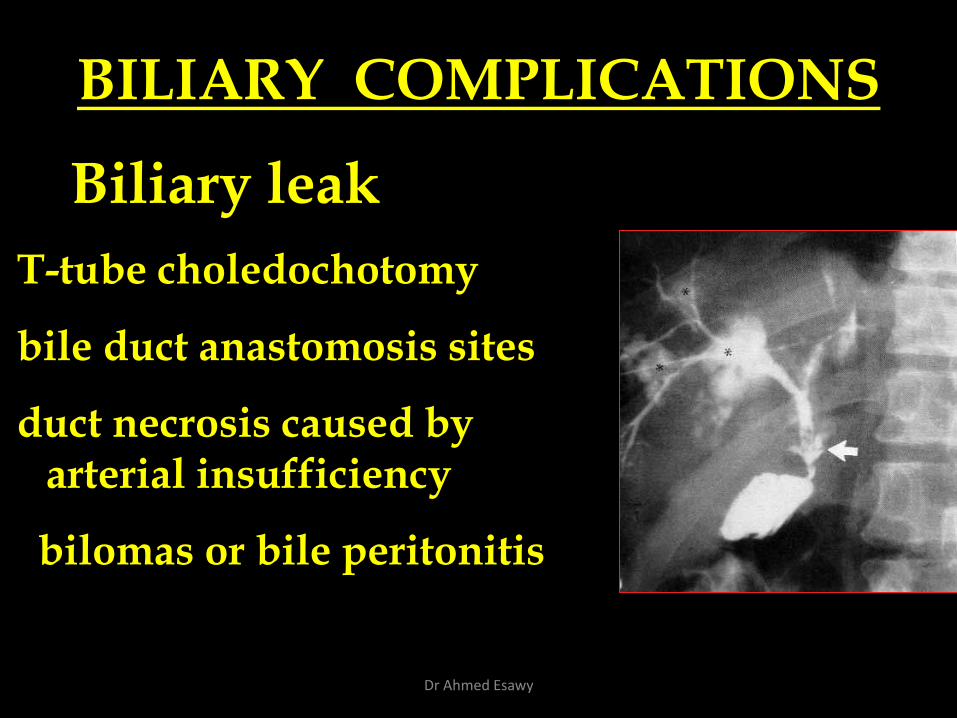
T-tube choledochotomy
bile duct anastomosis sites
duct necrosis caused by arterial insufficiency
bilomas or bile peritonitis
Biliary leak
BILIARY COMPLICATIONS
Dr Ahmed Esawy
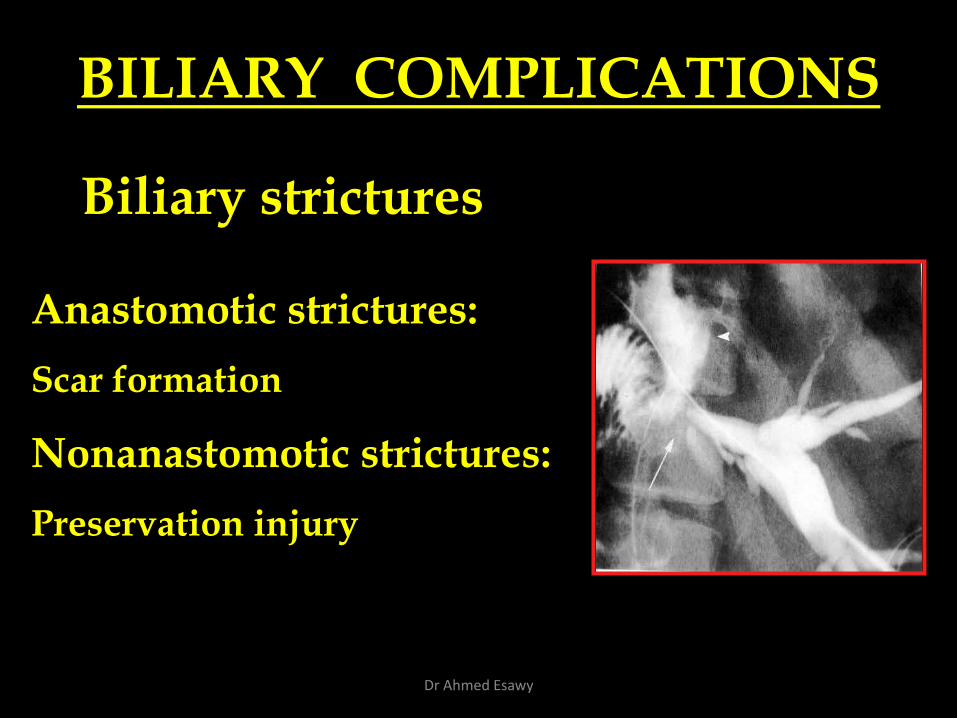
Biliary strictures
Anastomotic strictures:
Scar formation
Nonanastomotic strictures:
Preservation injury
BILIARY COMPLICATIONS
Dr Ahmed Esawy
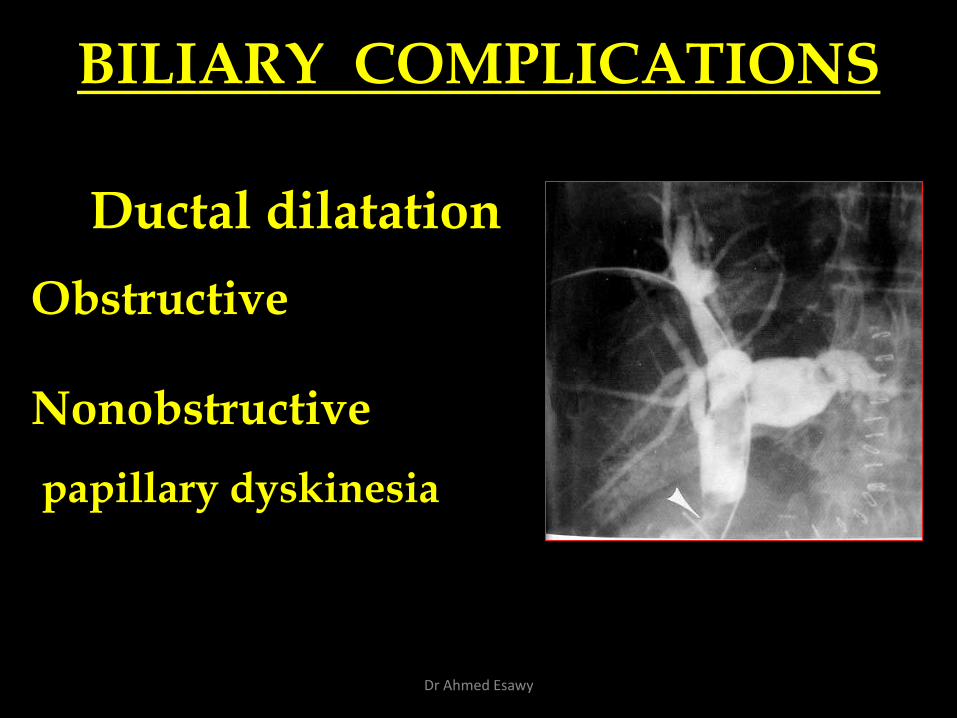
Ductal dilatation
Obstructive
Nonobstructive
papillary dyskinesia
BILIARY COMPLICATIONS
Dr Ahmed Esawy
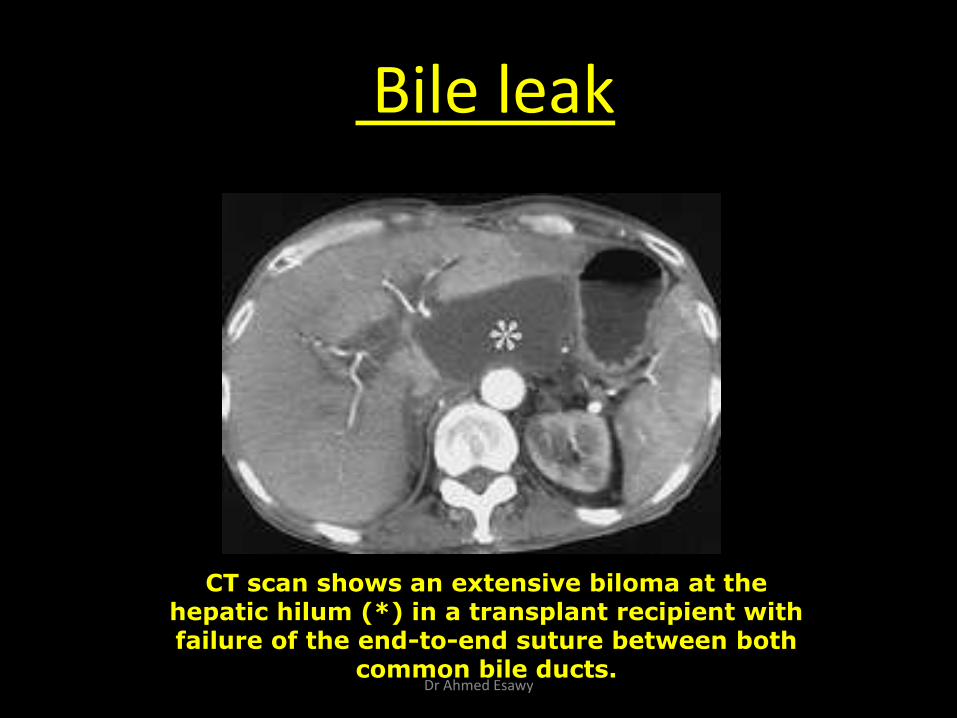
Bile leak
CT scan shows an extensive biloma at the hepatic hilum (*) in a transplant recipient with failure of the end-to-end suture between both
common bile ducts. Dr Ahmed Esawy
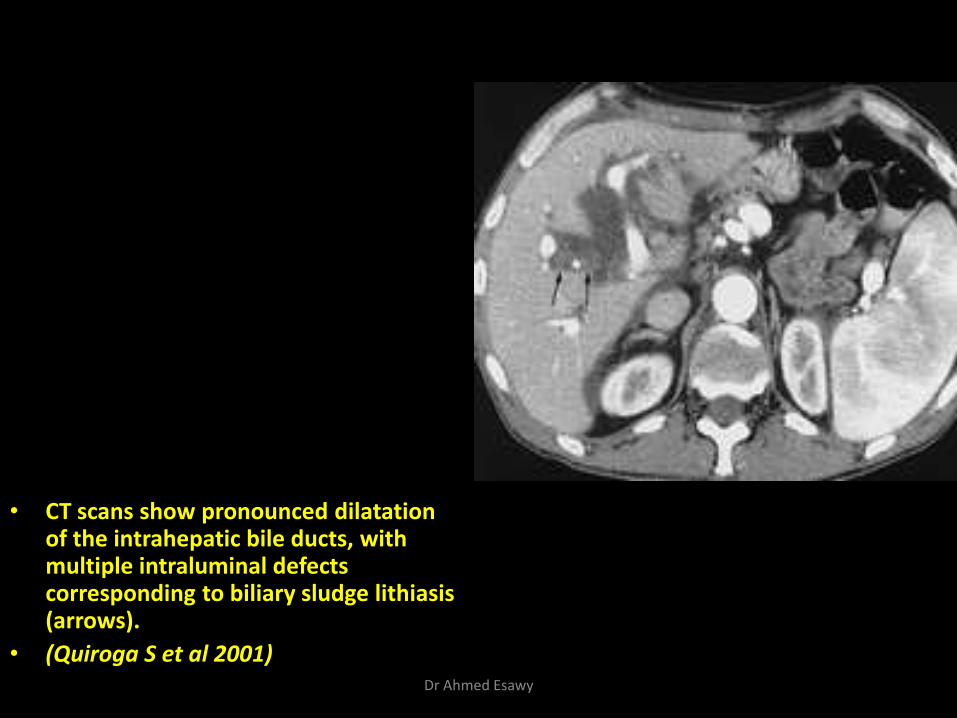
• CT scans show pronounced dilatation of the intrahepatic bile ducts, with multiple intraluminal defects corresponding to biliary sludge lithiasis (arrows).
• (Quiroga S et al 2001) Dr Ahmed Esawy
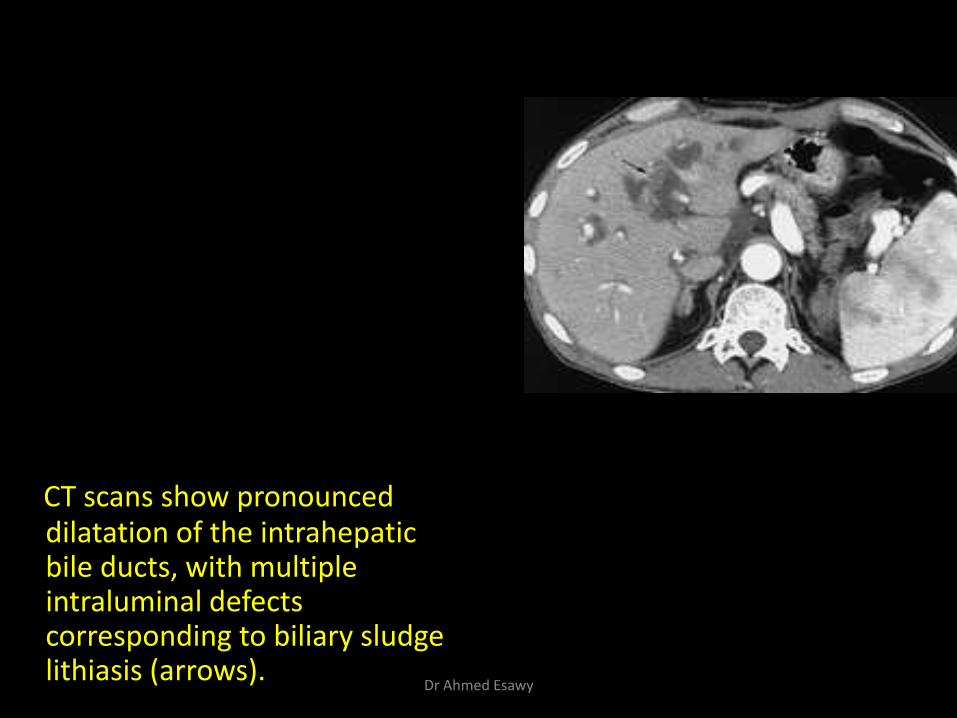
CT scans show pronounced dilatation of the intrahepatic bile ducts, with multiple intraluminal defects corresponding to biliary sludge lithiasis (arrows).
Dr Ahmed Esawy
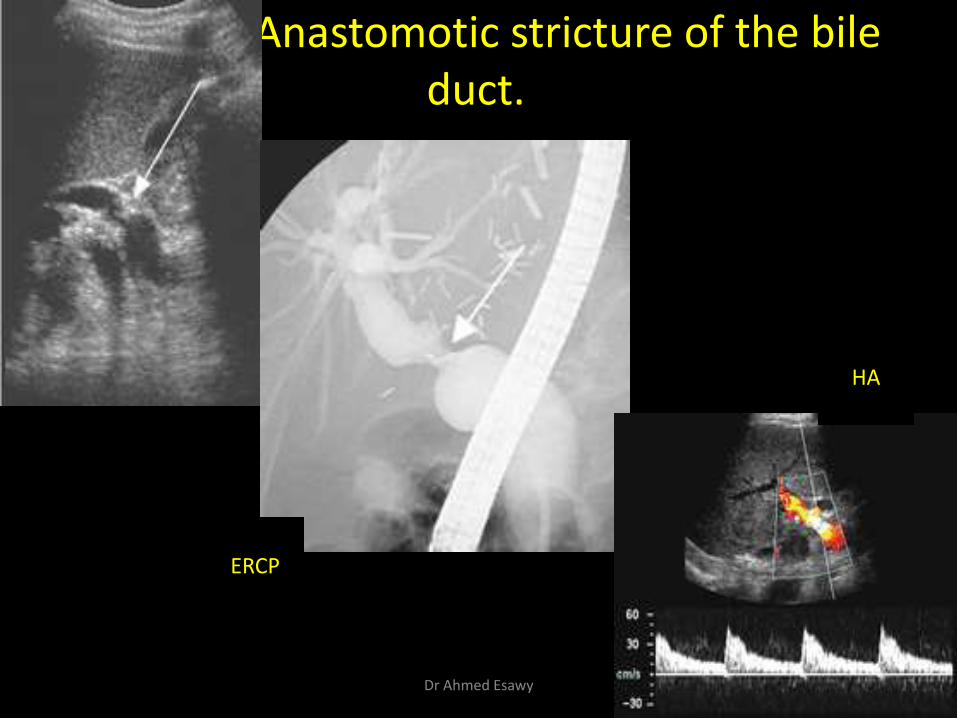
Anastomotic stricture of the bile duct.
ERCP
HA
Dr Ahmed Esawy
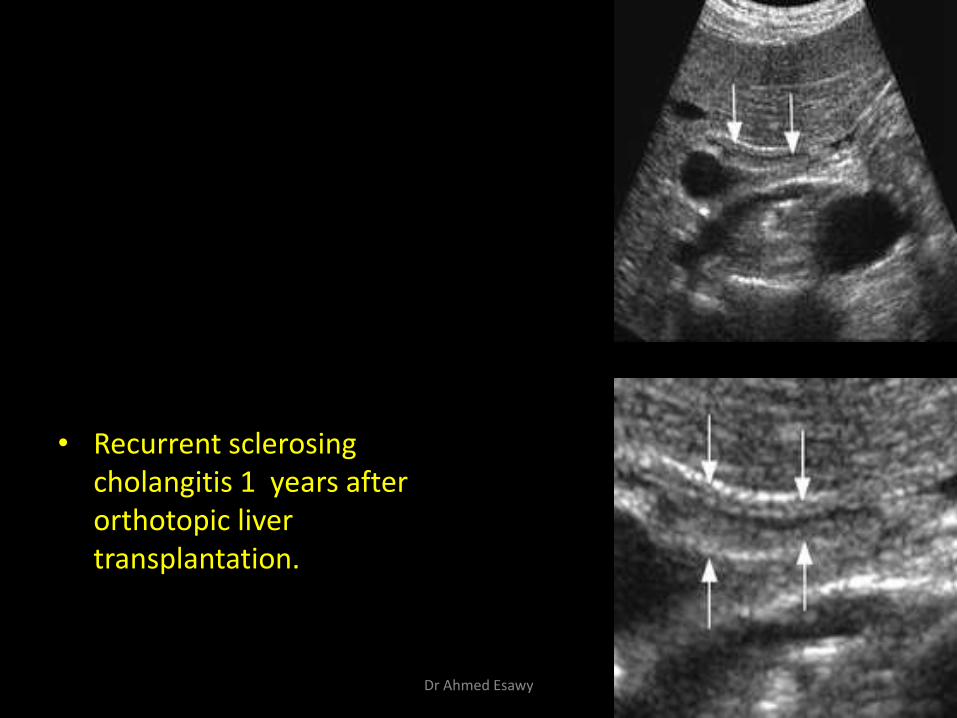
• Recurrent sclerosing cholangitis 1 years after orthotopic liver transplantation.
Dr Ahmed Esawy

• Intrahepatic bile duct dilatation in a 14-year-old boy 2 months after living related transplantation to treat biliary atresia.
Dr Ahmed Esawy

• Bile duct damage due to hepatic arterial thrombosis
Dr Ahmed Esawy

intrahepatic bile duct dilatation due to
anastomotic stricture, biliary stones
Dr Ahmed Esawy
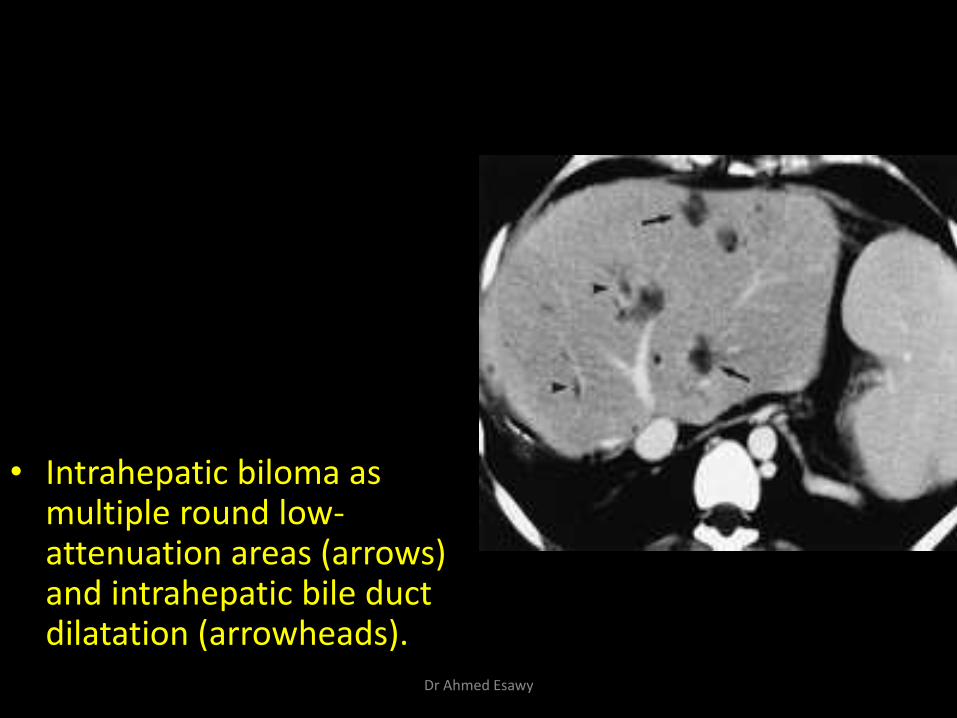
• Intrahepatic biloma as multiple round low-attenuation areas (arrows) and intrahepatic bile duct dilatation (arrowheads).
Dr Ahmed Esawy

• Biliary stone.
Dr Ahmed Esawy
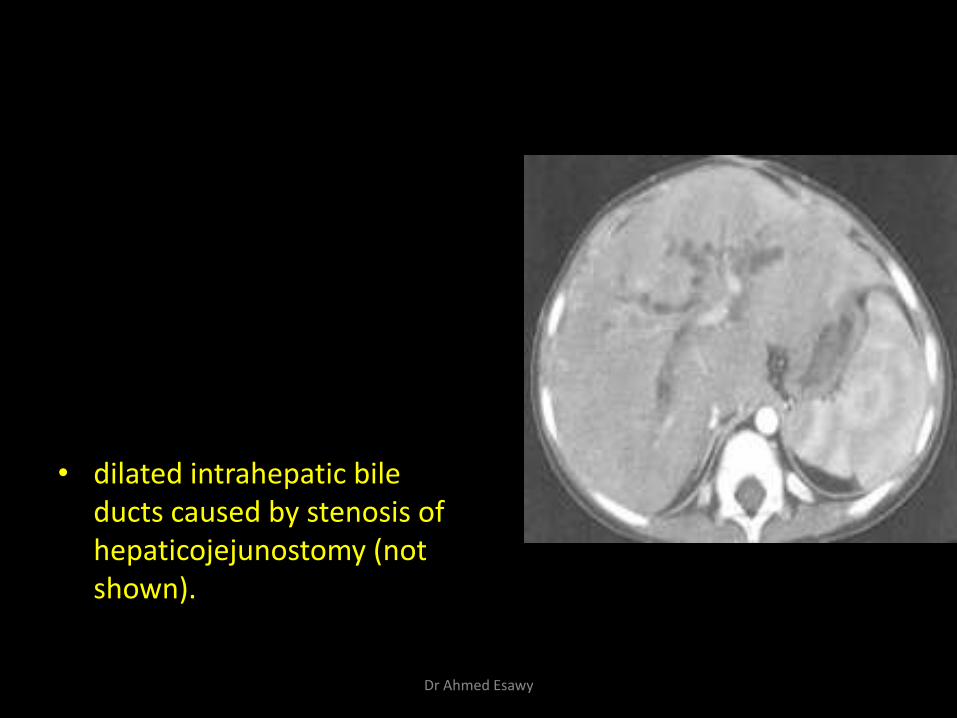
• dilated intrahepatic bile ducts caused by stenosis of hepaticojejunostomy (not shown).
Dr Ahmed Esawy
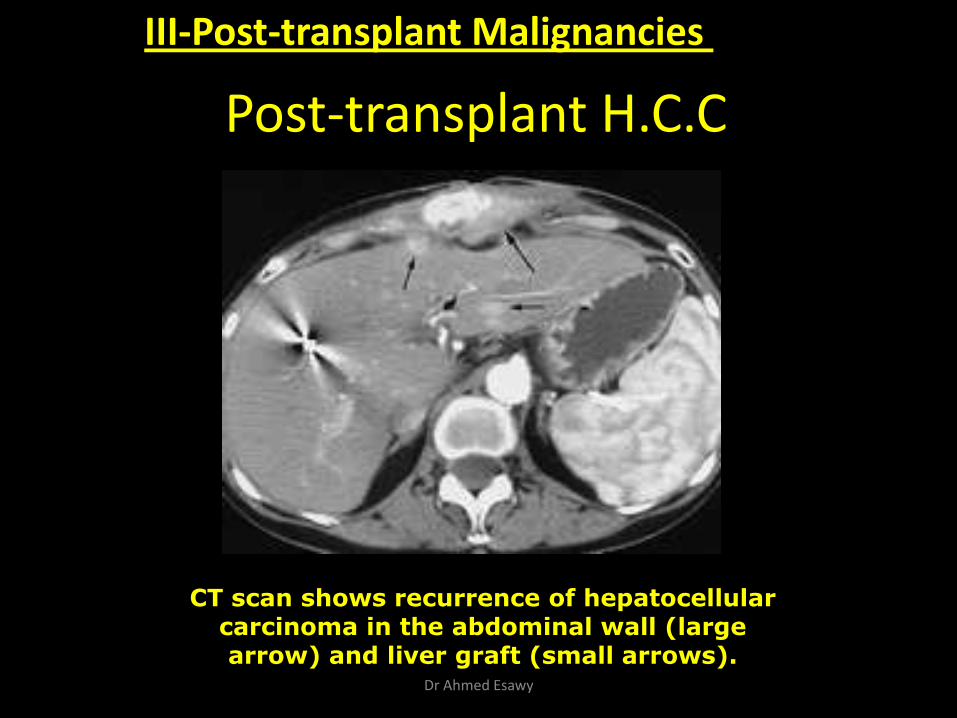
Post-transplant H.C.C
CT scan shows recurrence of hepatocellular carcinoma in the abdominal wall (large arrow) and liver graft (small arrows).
III-Post-transplant Malignancies
Dr Ahmed Esawy
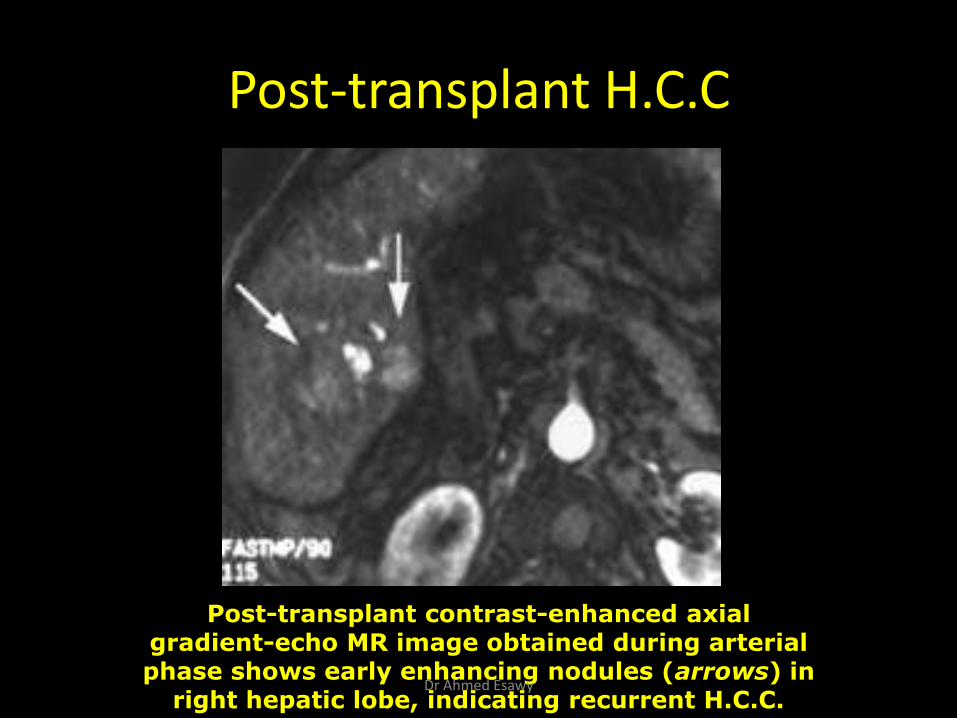
Post-transplant H.C.C
Post-transplant contrast-enhanced axial gradient-echo MR image obtained during arterial phase shows early enhancing nodules (arrows) in
right hepatic lobe, indicating recurrent H.C.C. Dr Ahmed Esawy
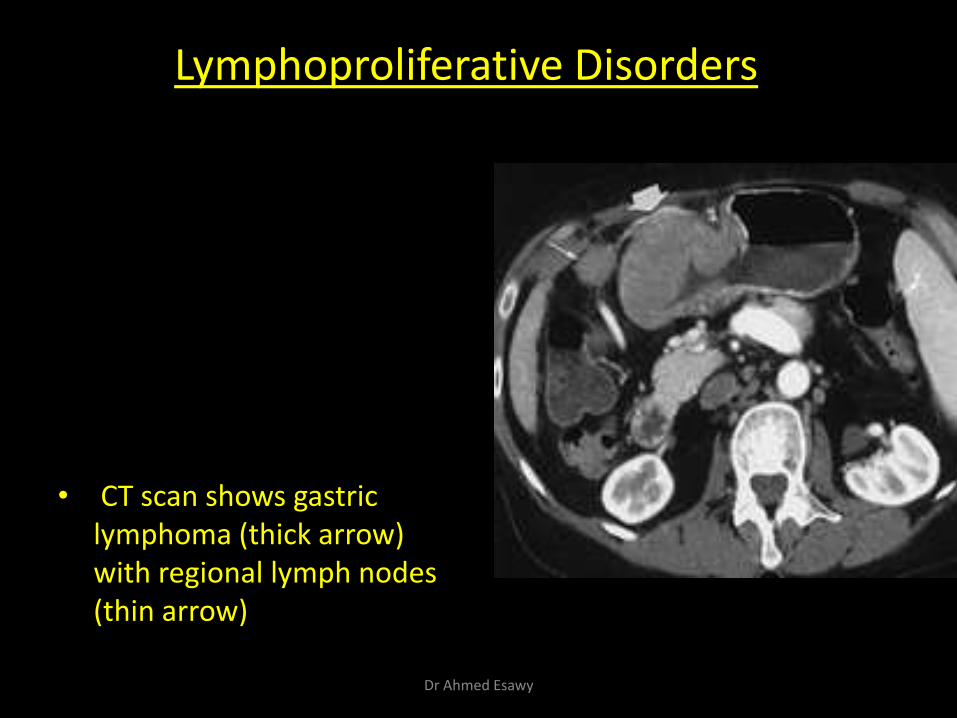
• CT scan shows gastric lymphoma (thick arrow) with regional lymph nodes (thin arrow)
Lymphoproliferative Disorders
Dr Ahmed Esawy
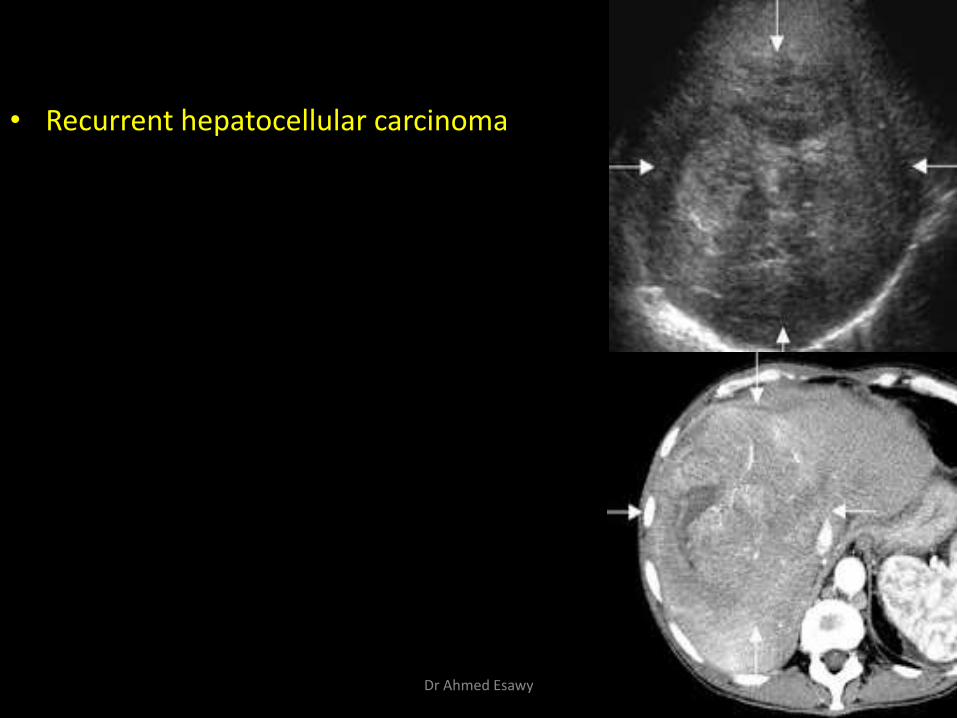
• Recurrent hepatocellular carcinoma
Dr Ahmed Esawy
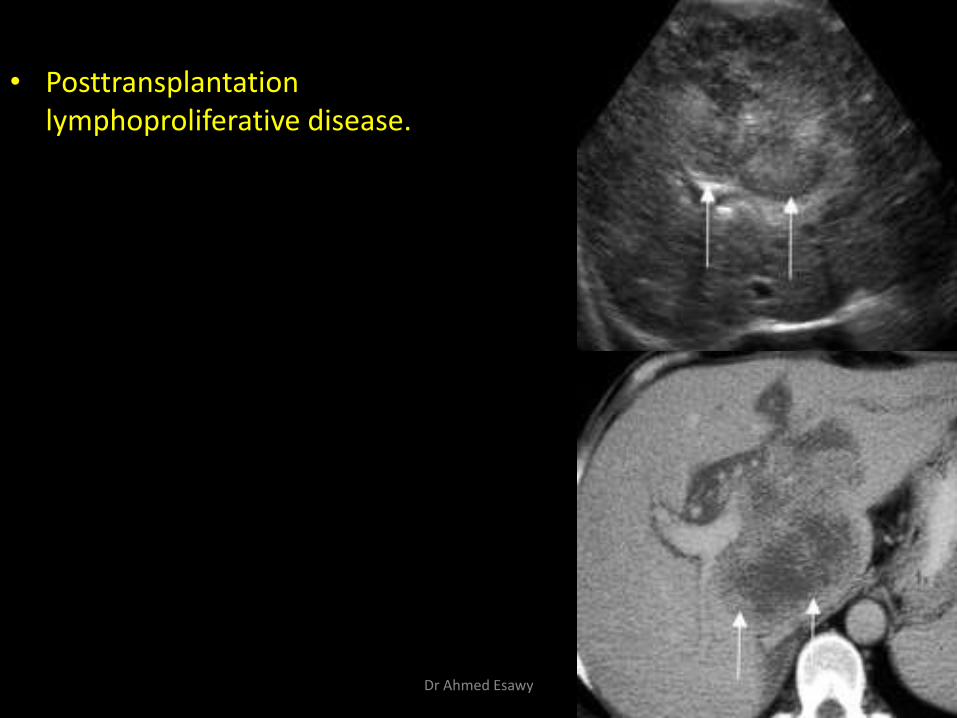
• Posttransplantation lymphoproliferative disease.
Dr Ahmed Esawy

• Nodal and splenic PTLD.
Dr Ahmed Esawy
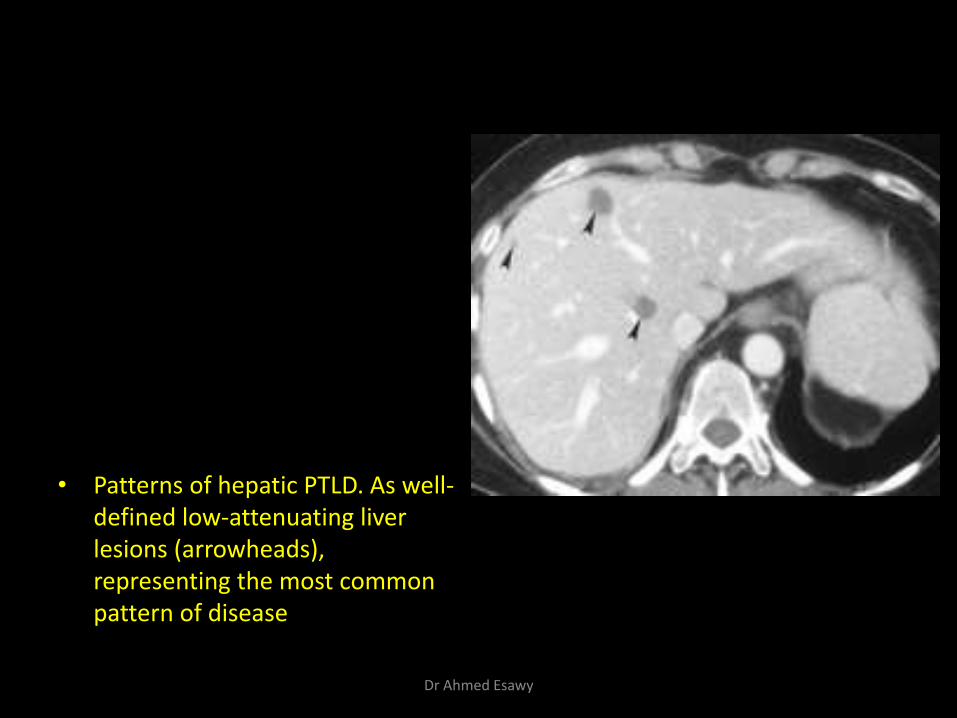
• Patterns of hepatic PTLD. As well-defined low-attenuating liver lesions (arrowheads), representing the most common pattern of disease
Dr Ahmed Esawy
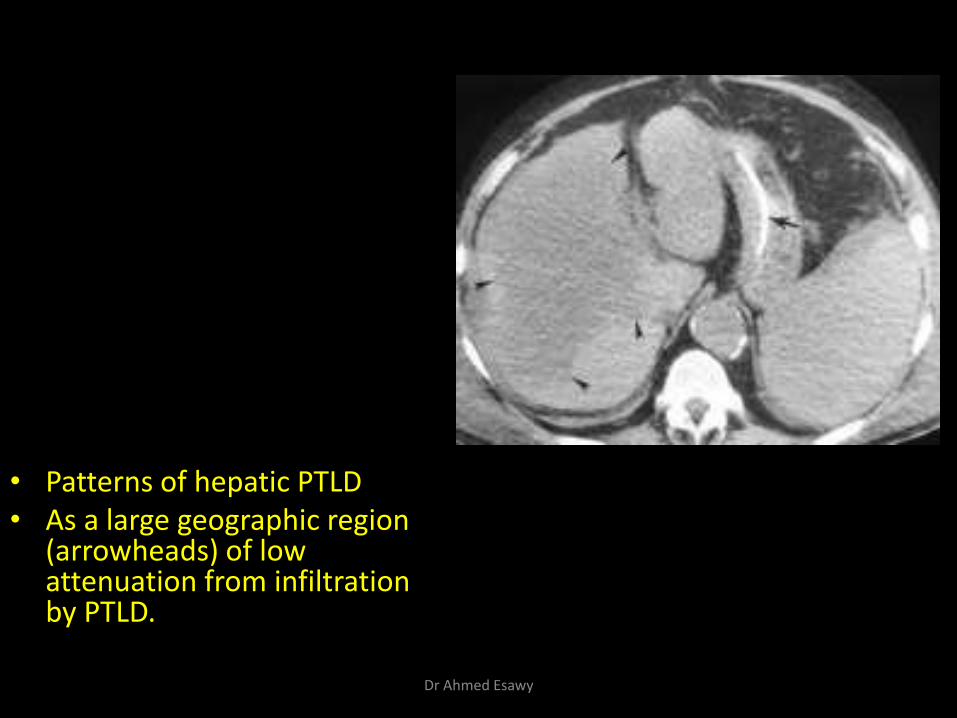
• Patterns of hepatic PTLD • As a large geographic region
(arrowheads) of low attenuation from infiltration by PTLD.
Dr Ahmed Esawy
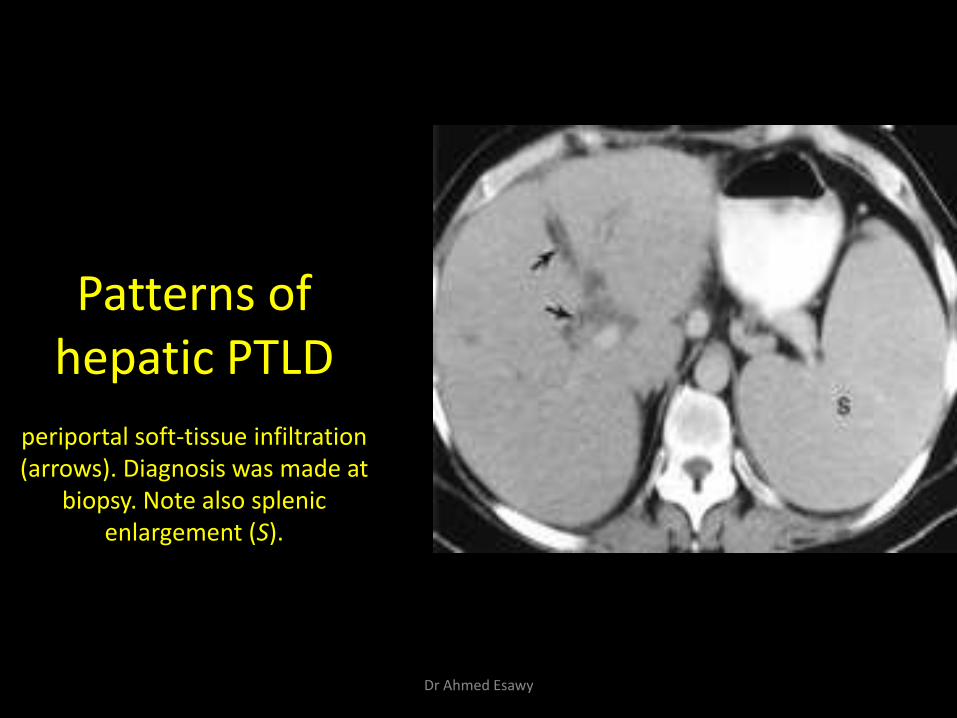
Patterns of hepatic PTLD
periportal soft-tissue infiltration (arrows). Diagnosis was made at
biopsy. Note also splenic enlargement (S).
Dr Ahmed Esawy
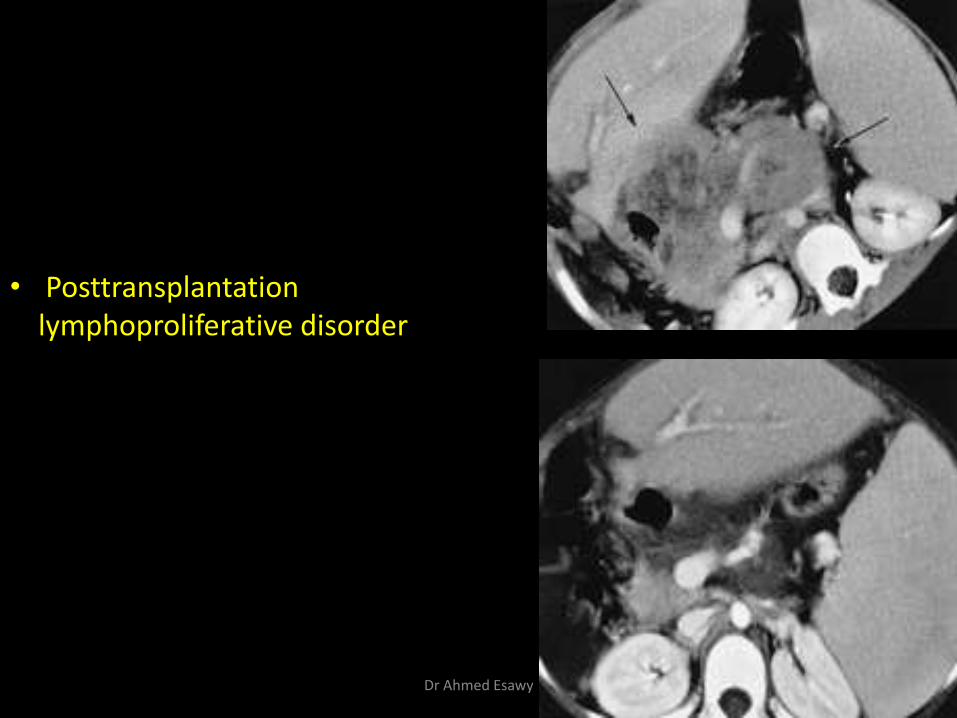
• Posttransplantation lymphoproliferative disorder
Dr Ahmed Esawy
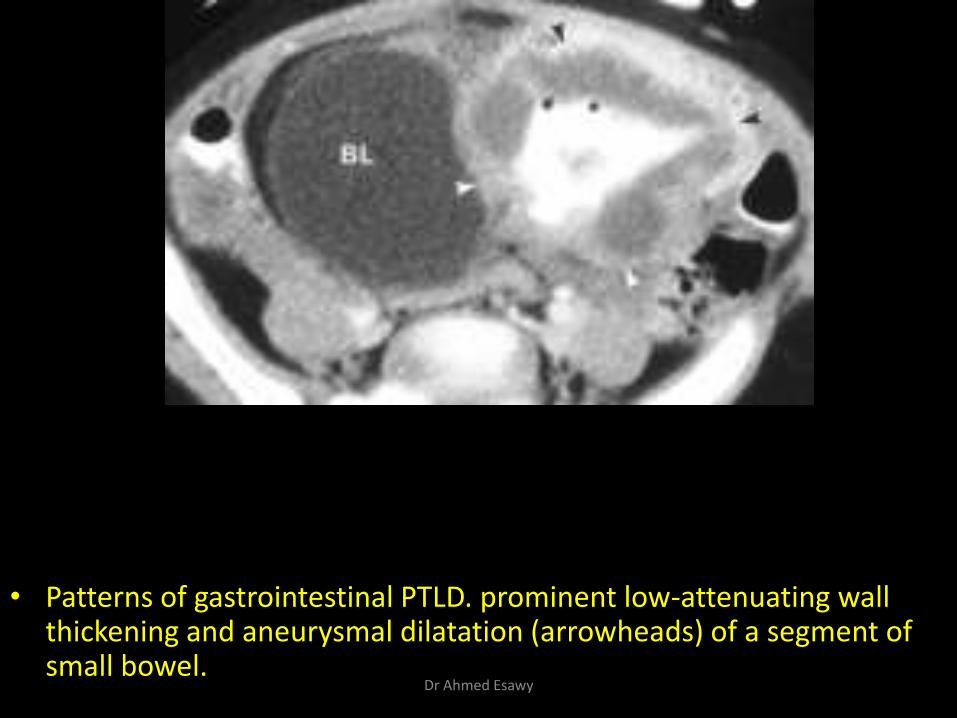
• Patterns of gastrointestinal PTLD. prominent low-attenuating wall thickening and aneurysmal dilatation (arrowheads) of a segment of small bowel.
Dr Ahmed Esawy
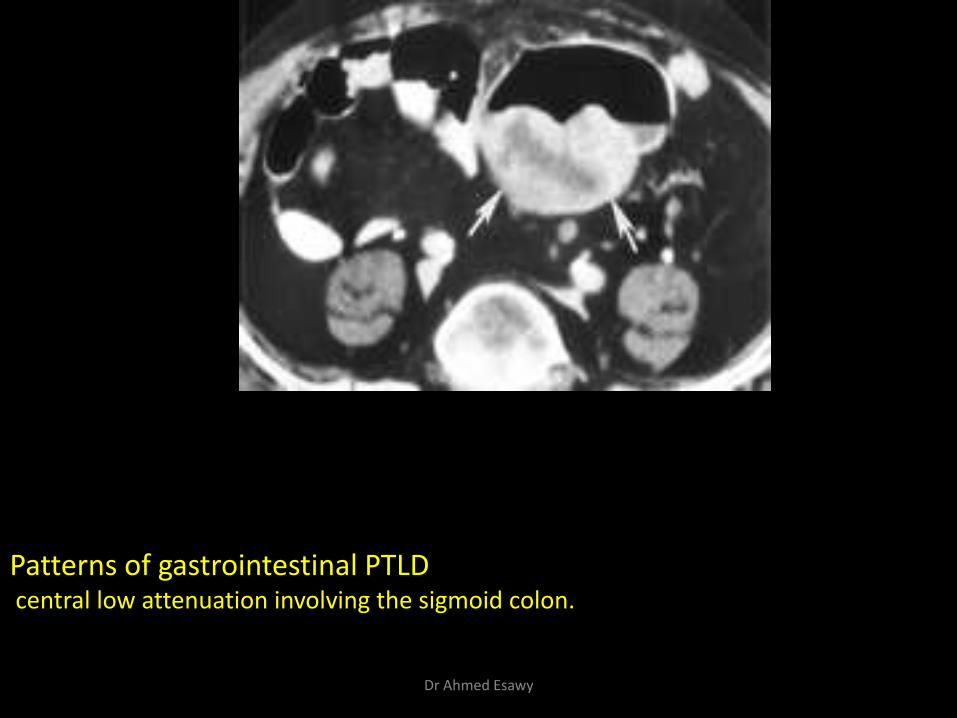
Patterns of gastrointestinal PTLD
central low attenuation involving the sigmoid colon.
Dr Ahmed Esawy
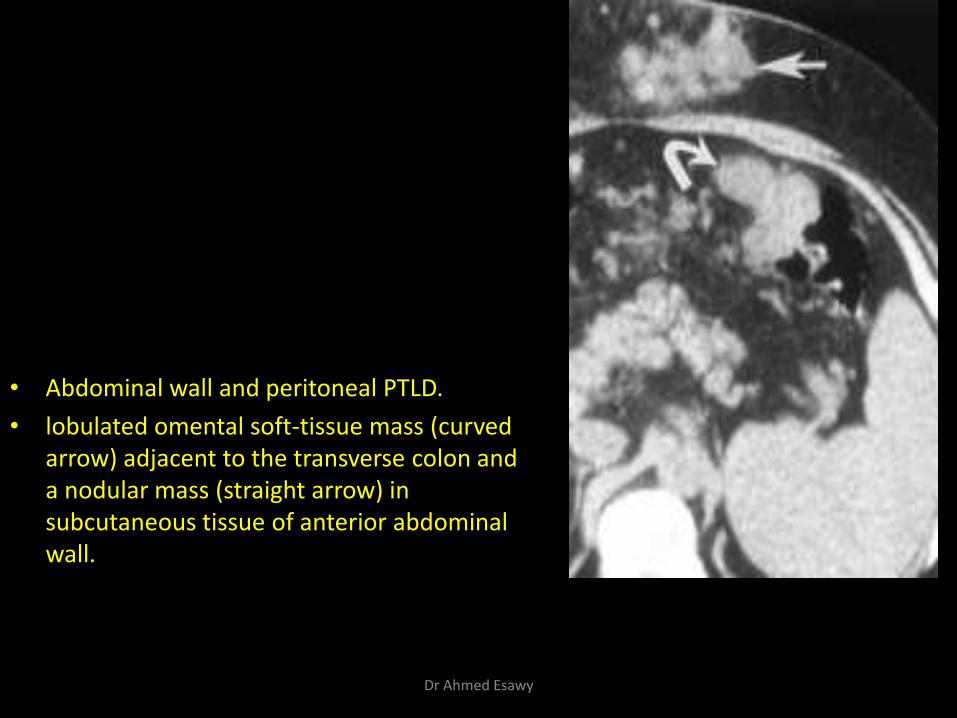
• Abdominal wall and peritoneal PTLD.
• lobulated omental soft-tissue mass (curved arrow) adjacent to the transverse colon and a nodular mass (straight arrow) in subcutaneous tissue of anterior abdominal wall.
Dr Ahmed Esawy
PARENCHYMAL COMPLICATIONS
Hepatic infarction
Hepatic abscess
Biloma
Rejection
Recurrence of malignancy
Fatty liver
Complication of biopsy
Dr Ahmed Esawy
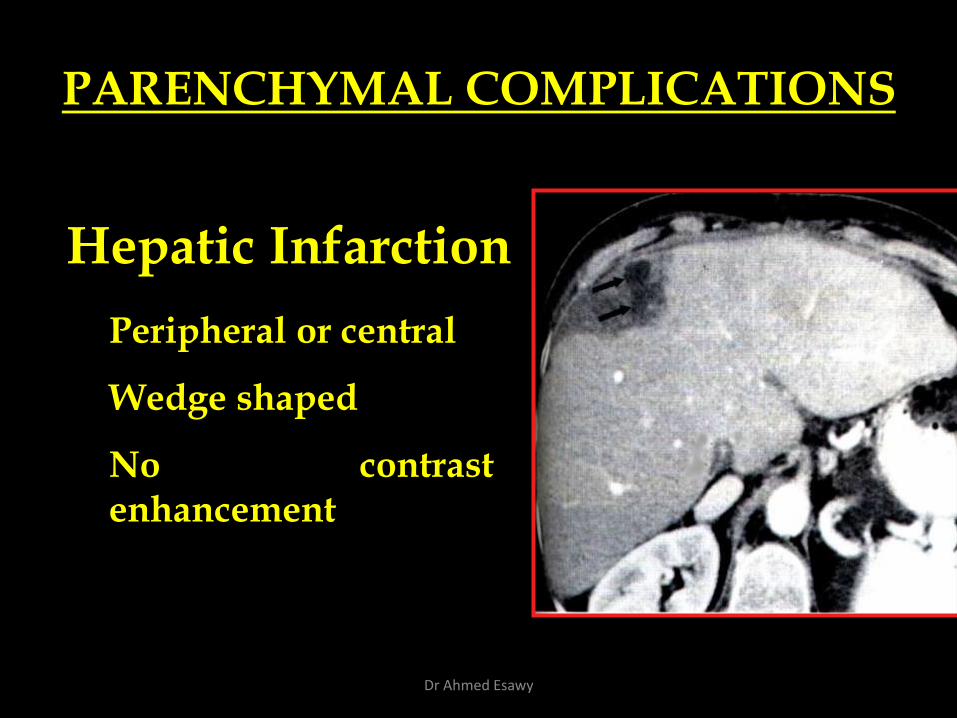
PARENCHYMAL COMPLICATIONS
Hepatic Infarction
Peripheral or central
Wedge shaped
No contrast enhancement
Dr Ahmed Esawy
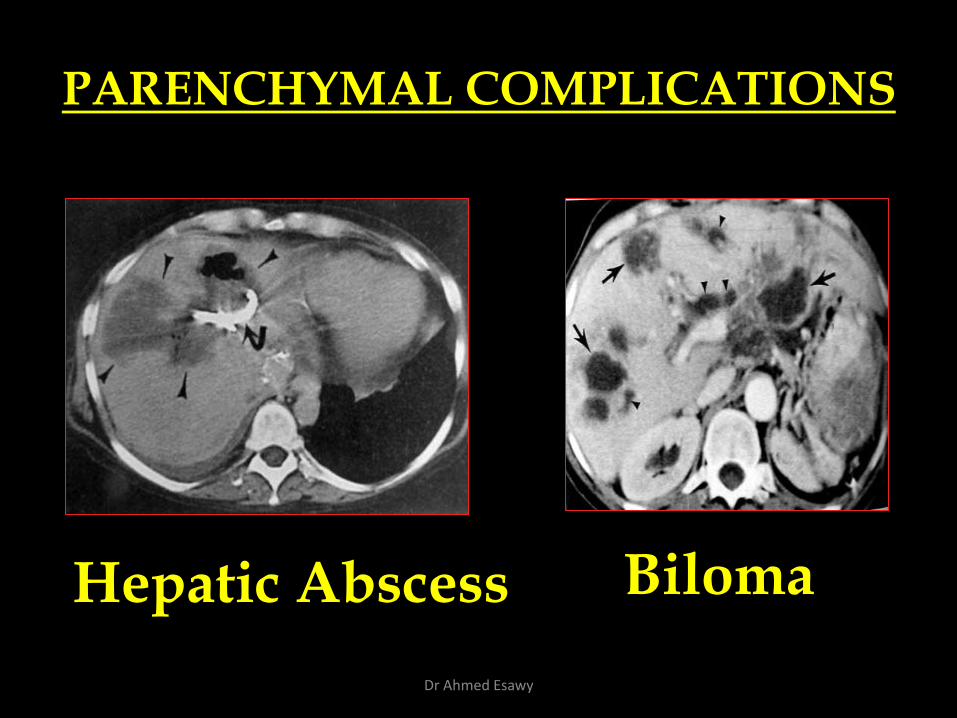
PARENCHYMAL COMPLICATIONS
Hepatic Abscess Biloma
Dr Ahmed Esawy
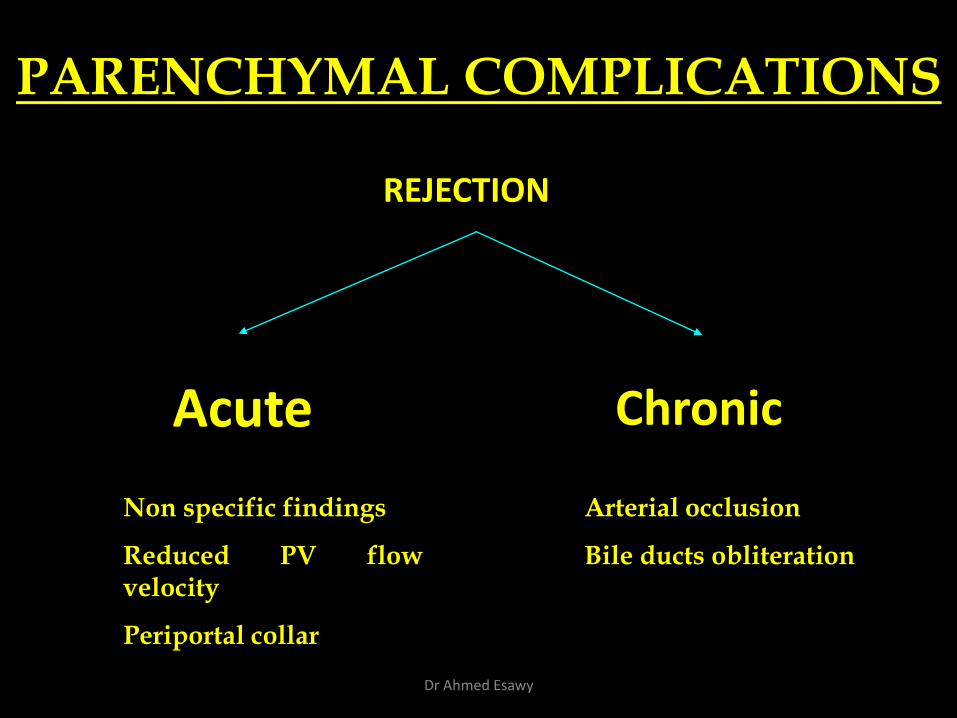
Acute Chronic
PARENCHYMAL COMPLICATIONS
Non specific findings
Reduced PV flow velocity
Periportal collar
Arterial occlusion
Bile ducts obliteration
REJECTION
Dr Ahmed Esawy
Primary Graft Failure:
• Primary graft failure occurs in approximately 7% of patients and is a very serious complication. The patient decompensates quickly, and a desperate search for a new graft must be initiated. Patients show markedly abnormal liver function, coagulopathy, oliguria, and severe CNS changes (including seizures and status epilepticus). Stage IV coma, alkalosis, hyperkalemia, and hypoglycemia characterize the terminal phase of this acute hepatic decompensation. (Jalan R et al 1997)
• Urgent re-transplantation is the solution to this complication if it can be performed before pneumonia or irreversible coma occurs. (Jalan R et al 1997
Dr Ahmed Esawy
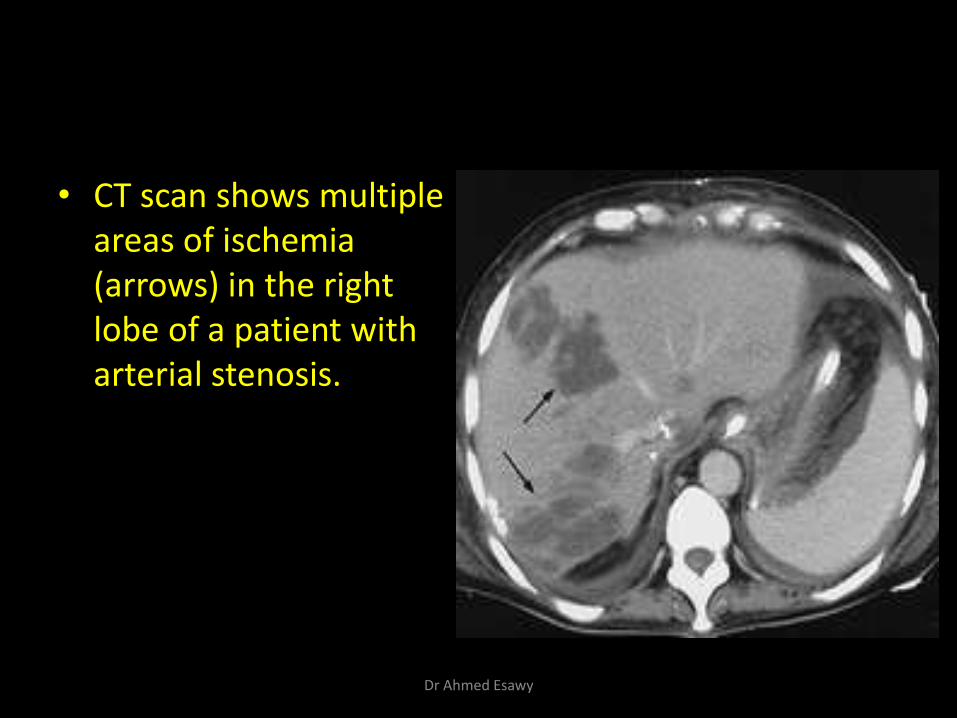
• CT scan shows multiple areas of ischemia (arrows) in the right lobe of a patient with arterial stenosis.
Dr Ahmed Esawy
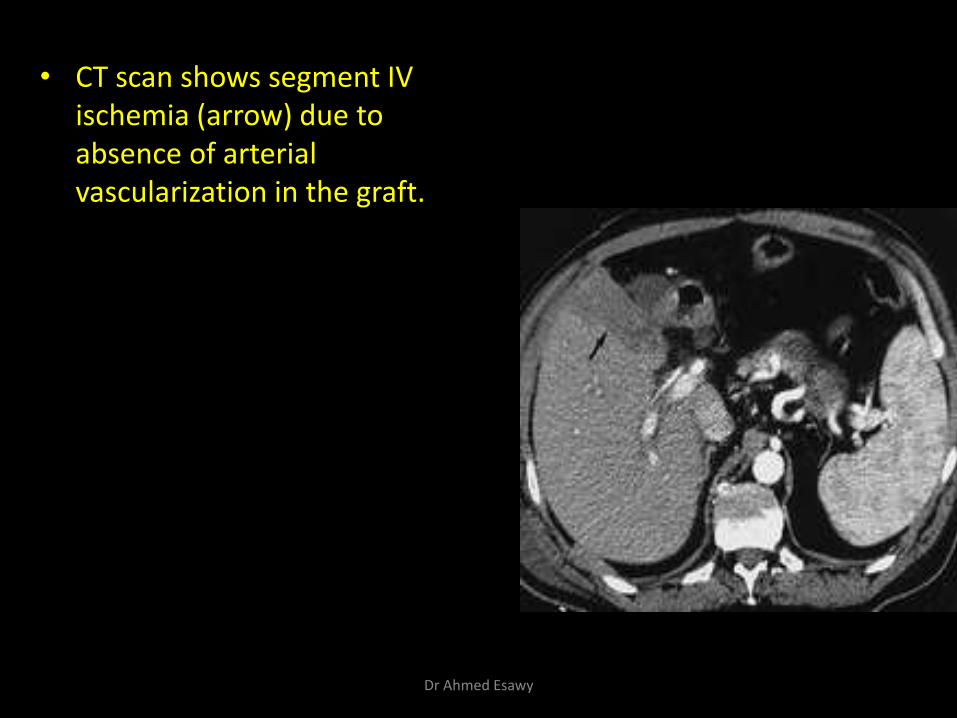
• CT scan shows segment IV ischemia (arrow) due to absence of arterial vascularization in the graft.
Dr Ahmed Esawy
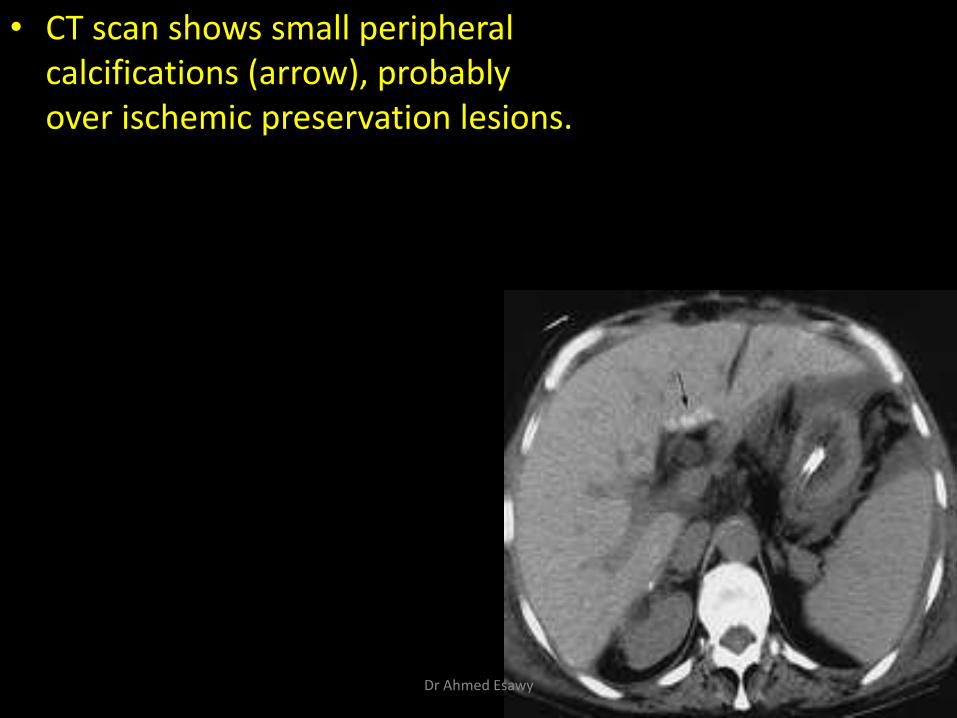
• CT scan shows small peripheral calcifications (arrow), probably over ischemic preservation lesions.
Dr Ahmed Esawy

• shows perihepatic hematoma (arrows).
Dr Ahmed Esawy
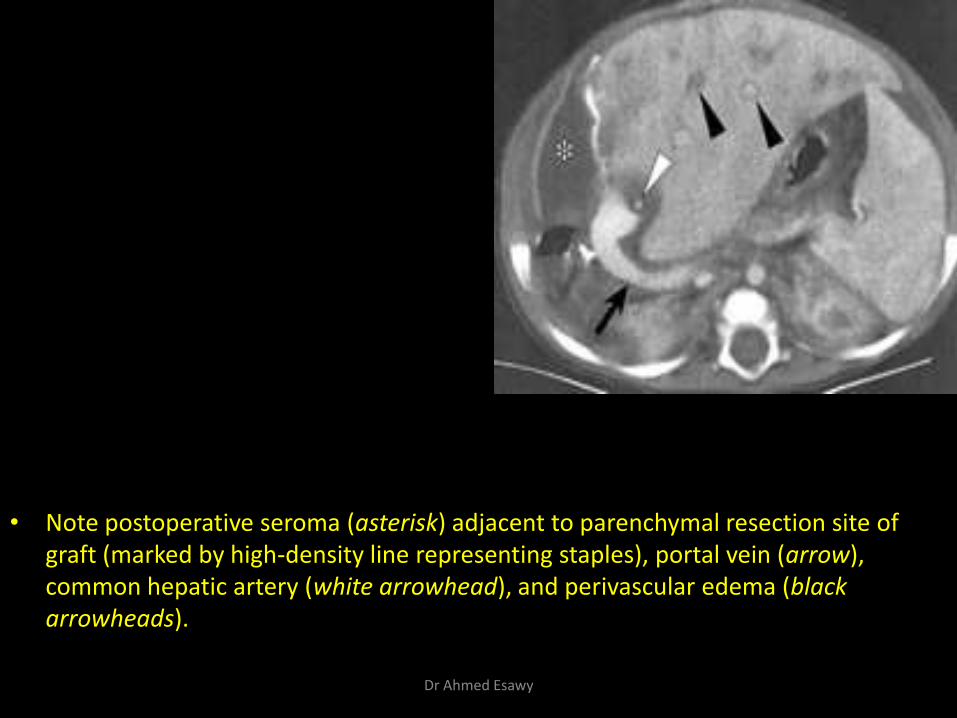
• Note postoperative seroma (asterisk) adjacent to parenchymal resection site of graft (marked by high-density line representing staples), portal vein (arrow), common hepatic artery (white arrowhead), and perivascular edema (black arrowheads).
Dr Ahmed Esawy
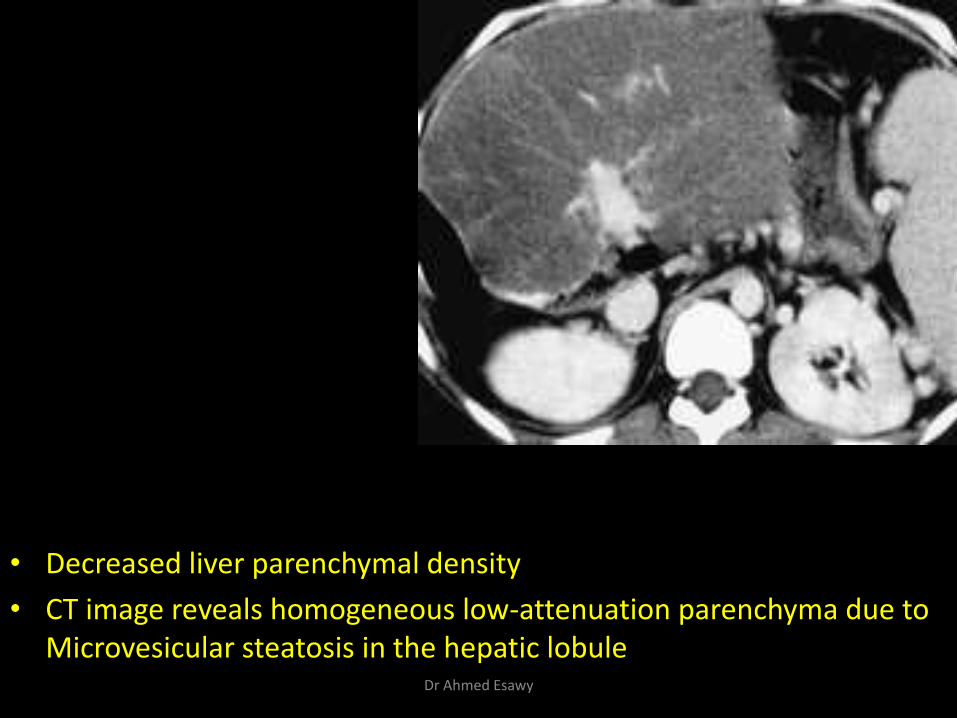
• Decreased liver parenchymal density
• CT image reveals homogeneous low-attenuation parenchyma due to Microvesicular steatosis in the hepatic lobule
Dr Ahmed Esawy
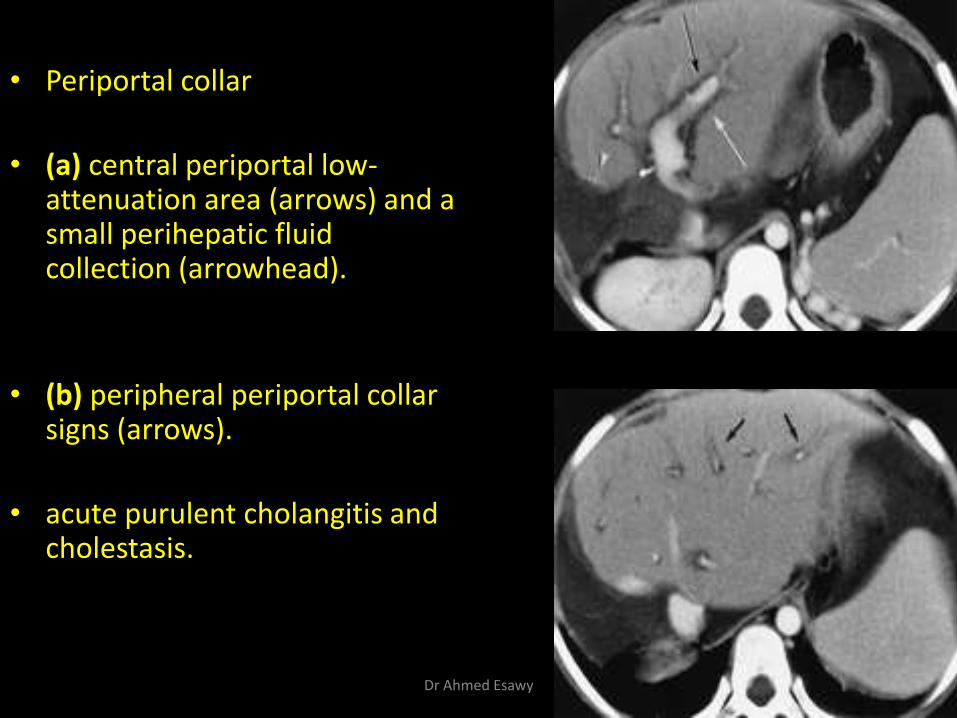
• Periportal collar
• (a) central periportal low-attenuation area (arrows) and a small perihepatic fluid collection (arrowhead).
• (b) peripheral periportal collar signs (arrows).
• acute purulent cholangitis and cholestasis.
Dr Ahmed Esawy
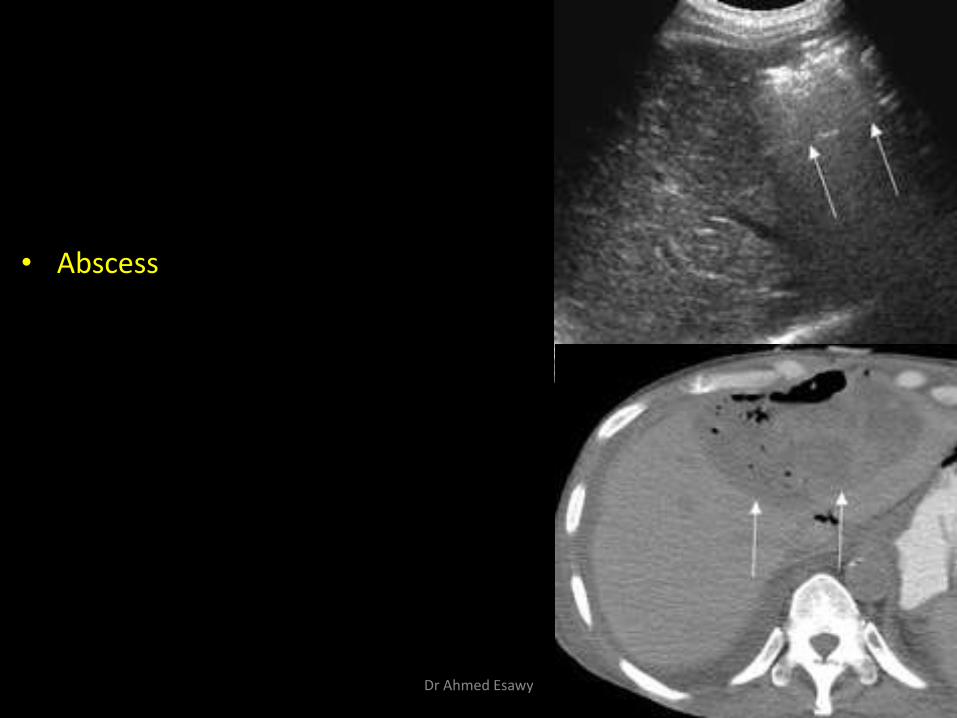
• Abscess
Dr Ahmed Esawy
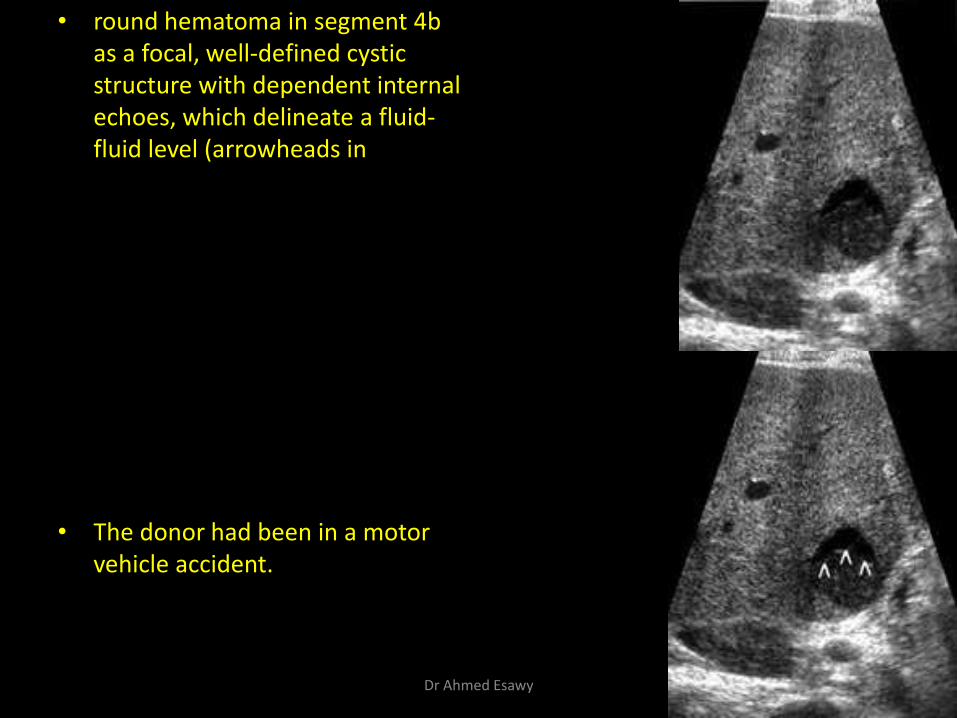
• round hematoma in segment 4b as a focal, well-defined cystic structure with dependent internal echoes, which delineate a fluid-fluid level (arrowheads in
• The donor had been in a motor vehicle accident.
Dr Ahmed Esawy
the differential diagnosis for diffuse parenchymal abnormality in the transplanted liver is also wide and includes
• rejection
• ischemia
• hepatitis
• cholangitis
Dr Ahmed Esawy
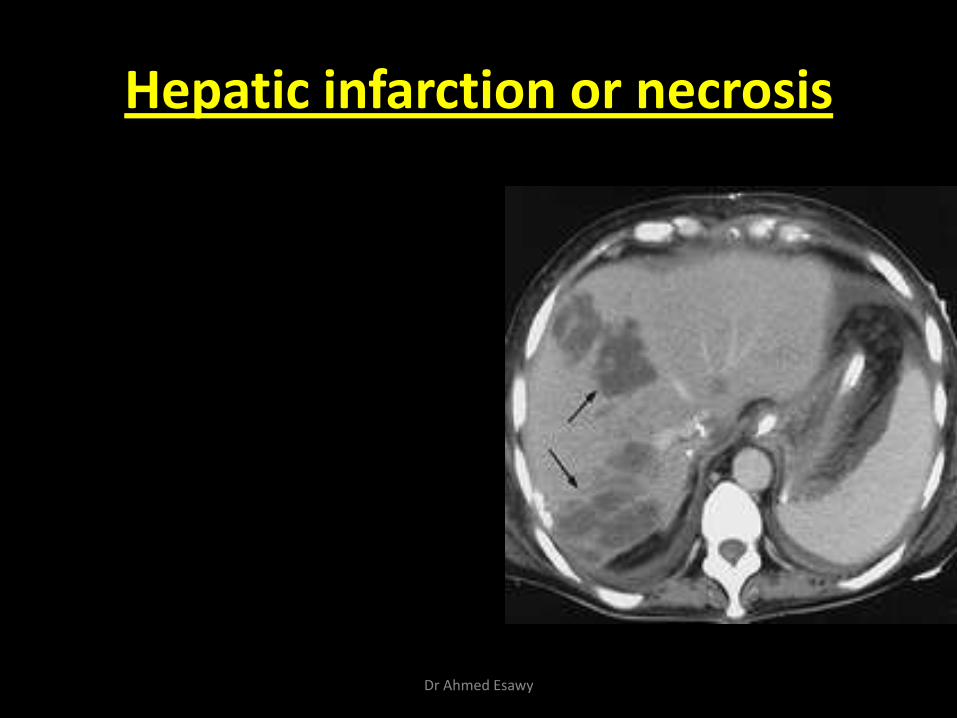
Hepatic infarction or necrosis
Dr Ahmed Esawy
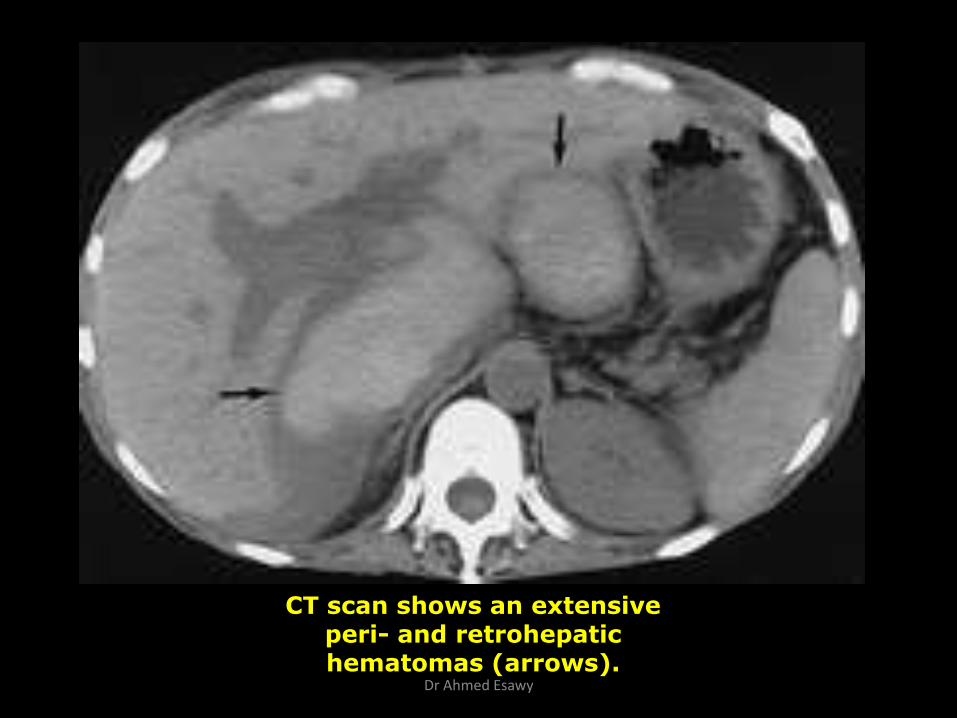
CT scan shows an extensive peri- and retrohepatic hematomas (arrows).
Dr Ahmed Esawy
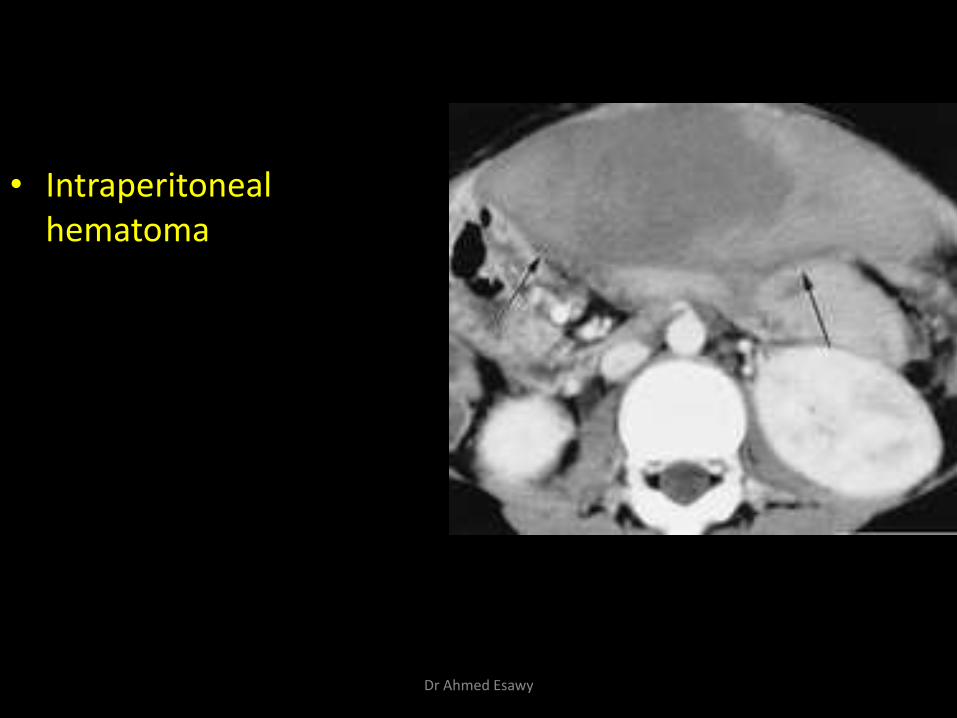
• Intraperitoneal hematoma
Dr Ahmed Esawy
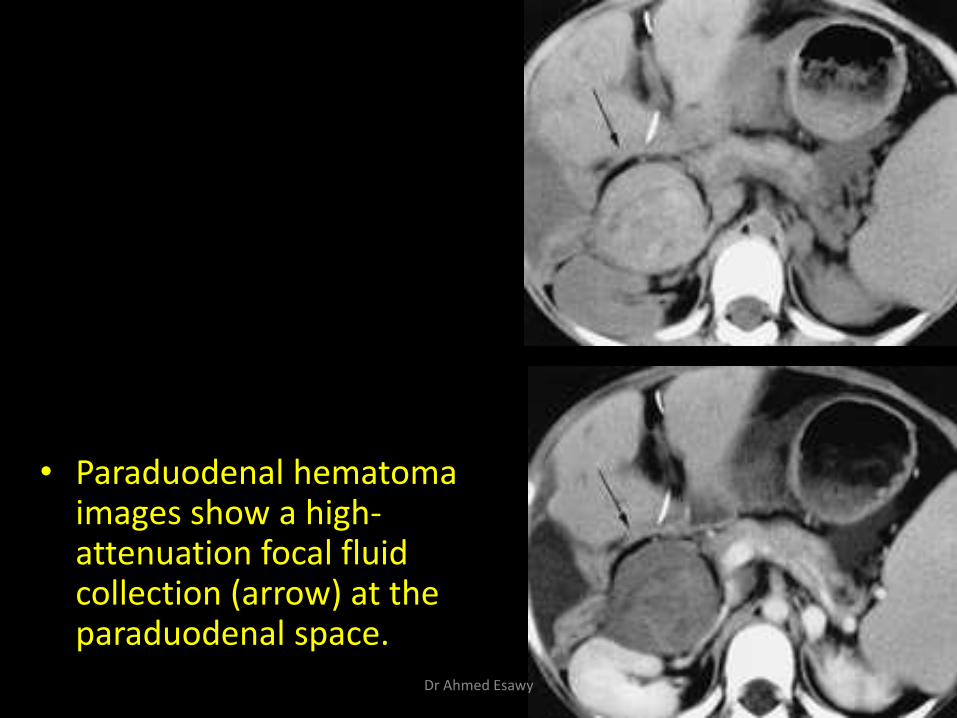
• Paraduodenal hematoma images show a high-attenuation focal fluid collection (arrow) at the paraduodenal space.
Dr Ahmed Esawy
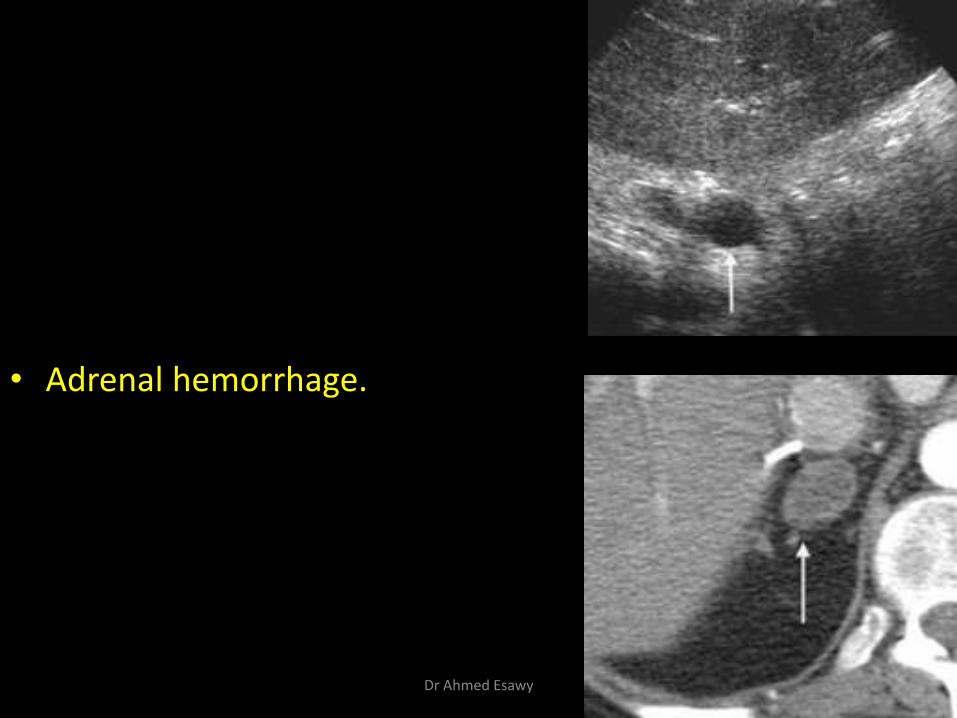
• Adrenal hemorrhage.
Dr Ahmed Esawy
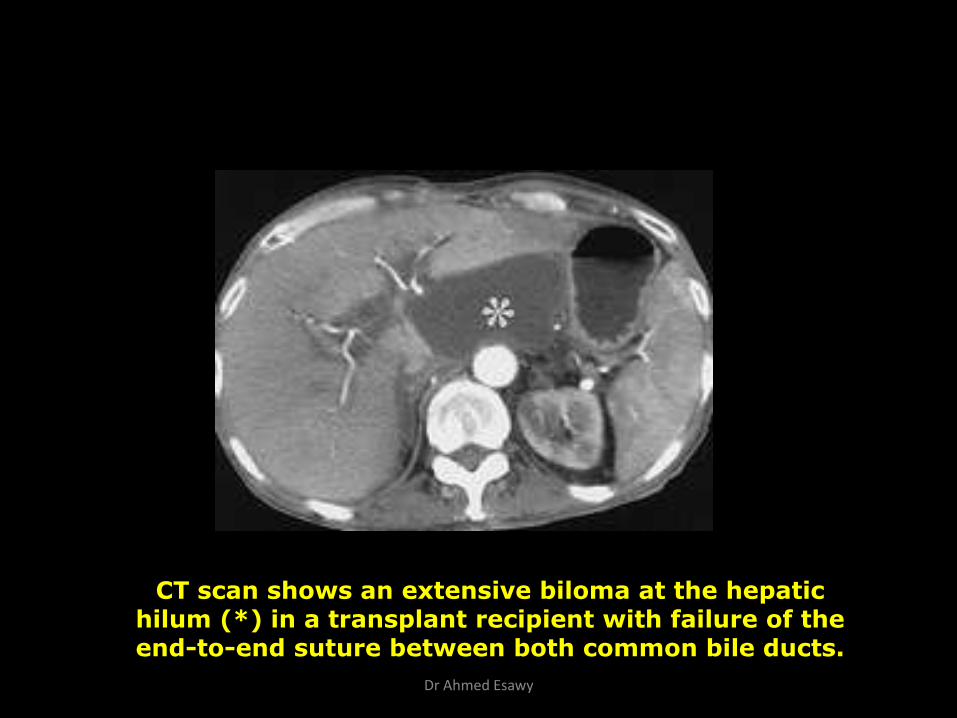
CT scan shows an extensive biloma at the hepatic hilum (*) in a transplant recipient with failure of the end-to-end suture between both common bile ducts.
Dr Ahmed Esawy
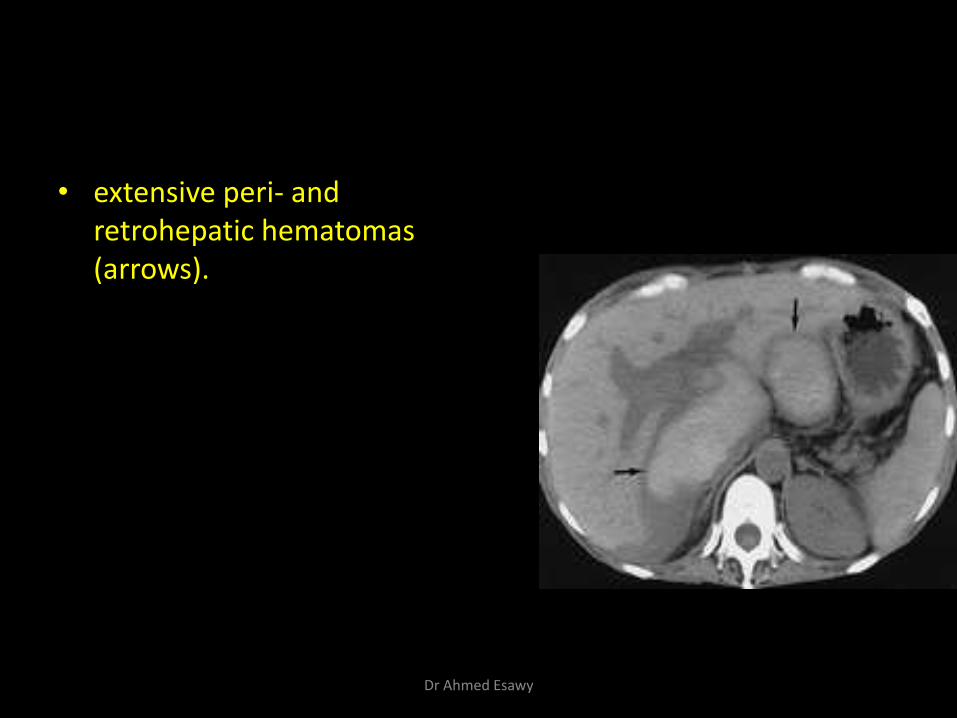
• extensive peri- and retrohepatic hematomas (arrows).
Dr Ahmed Esawy
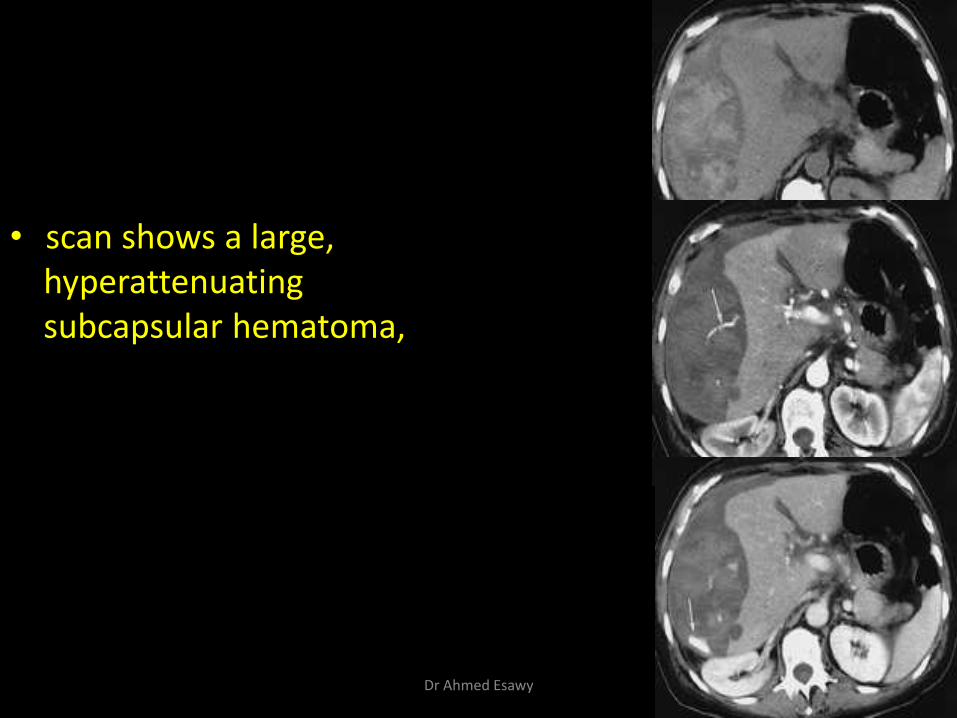
• scan shows a large, hyperattenuating subcapsular hematoma,
Dr Ahmed Esawy
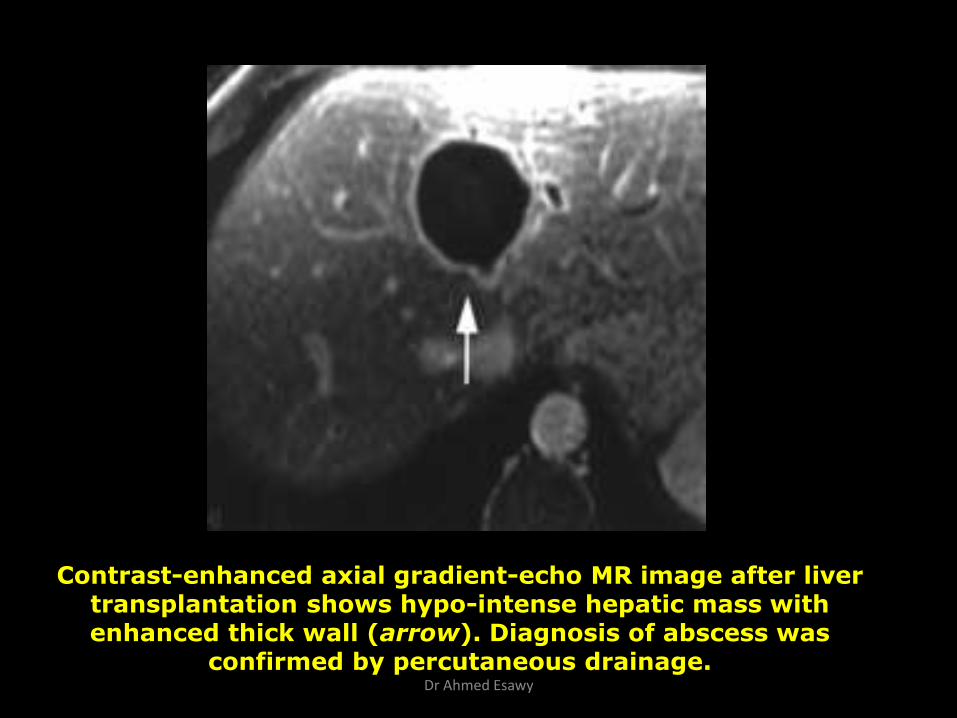
Contrast-enhanced axial gradient-echo MR image after liver transplantation shows hypo-intense hepatic mass with enhanced thick wall (arrow). Diagnosis of abscess was
confirmed by percutaneous drainage. Dr Ahmed Esawy
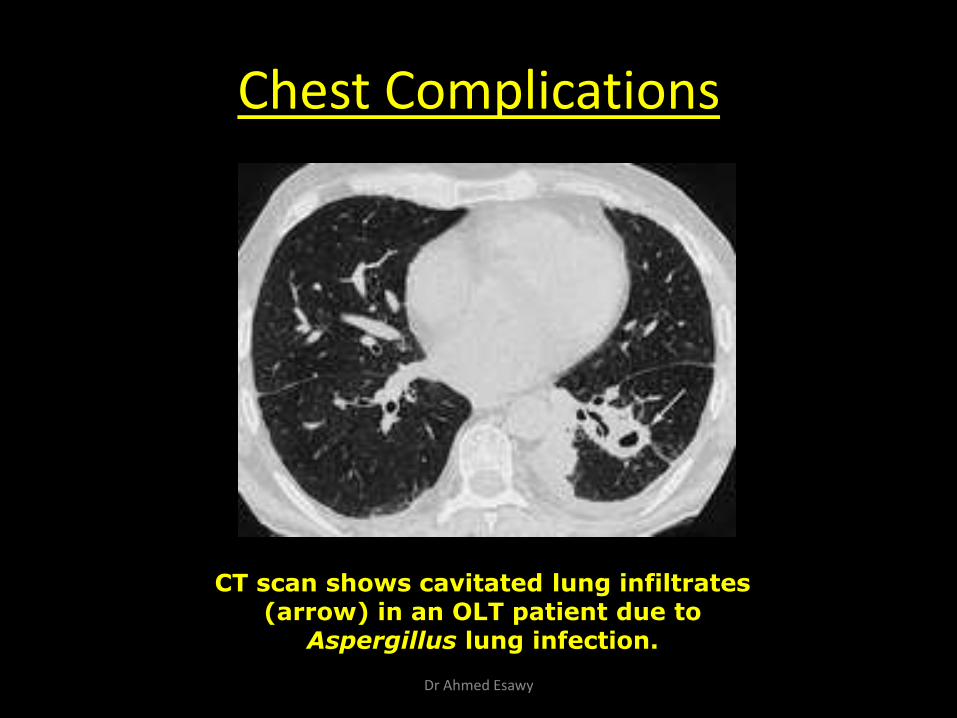
Chest Complications
CT scan shows cavitated lung infiltrates (arrow) in an OLT patient due to Aspergillus lung infection.
Dr Ahmed Esawy
Neurological Complications:
-Hemorrhage
-Ischemia
-Abscess
-PTLD
-alterations of consciousness
-seizures, stroke, tremor
-polyneuropathy.
CT or MRI can be used to detect and differentiate many of the causes for these symptoms. (Emre S et al 1994)
Dr Ahmed Esawy
Infection & Fevers:
• Immunosuppressive therapy leads to a significant increase in the likelihood of infections in transplant recipients and this complication remains the commonest overall cause of mortality. The risk of infection by viral, fungal and bacterial agents is well documented, the responsible organisms including CMV, invasive candidiasis, aspergillus, legionella and the more opportunistic pneumocystis carinii. (O'Grady J & Sutherland S 1995)
Dr Ahmed Esawy
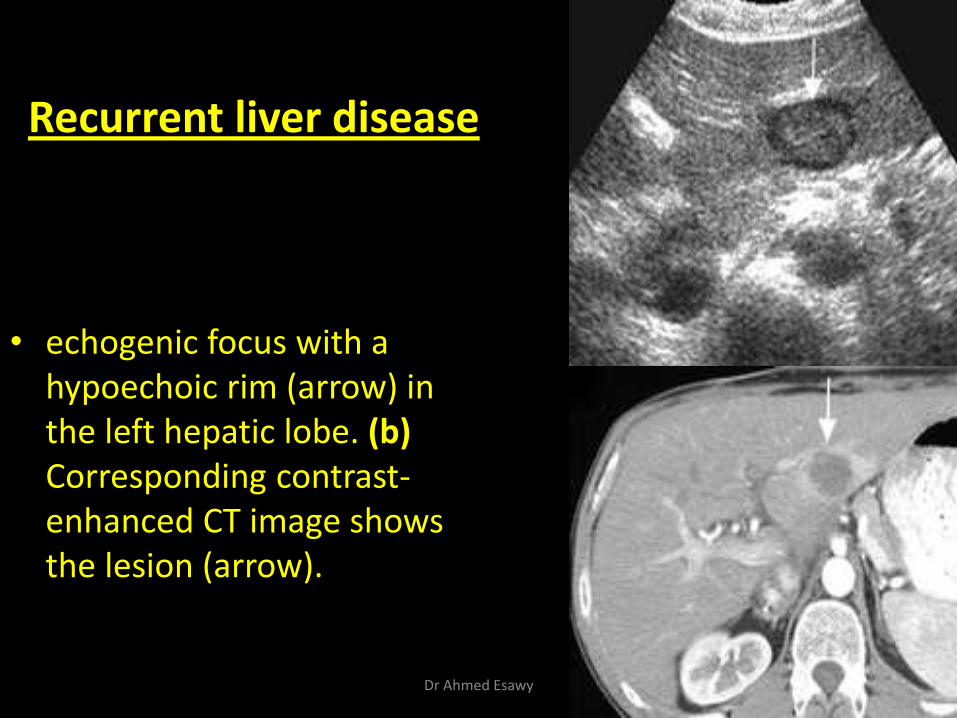
• echogenic focus with a hypoechoic rim (arrow) in the left hepatic lobe. (b) Corresponding contrast-enhanced CT image shows the lesion (arrow).
Recurrent liver disease
Dr Ahmed Esawy
Other long-term complications:
• (i) Arterial hypertension:
• (ii) Diabetes mellitus
Dr Ahmed Esawy
Rejection
(i) Acute rejection: Occur in about 40% of patients during the first 3 months post-transplant, but commonly 7-14 days after operation. The immune system attack the transplanted liver and destroy it.
(ii) Chronic rejection: Ducts suffer from direct immunological injury and ischemia from the obliterative arteriopathy results in progressive jaundice and allograft dysfunction.
The characteristics of chronic rejection in recipients of LT are progressive bile duct disappearance and obliterative arteriopathy (known as ductopenia), which results in progressive jaundice and allograft dysfunction
- Graft biopsy with histologic examination should be performed, if safe, to
document rejection. Adult liver biopsies are routinely performed at the bedside with or without ultrasound guidance.
- The role of imaging methods consists of excluding the other complications have clinical signs and symptoms similar to those of rejection.
Dr Ahmed Esawy












![Kidney Transplantation (Renal Transplantation) Auto Saved]](https://img.pdfslide.net/doc/110x75/577d22b31a28ab4e1e9807d7/kidney-transplantation-renal-transplantation-auto-saved.jpg)