Embed Size (px)
DESCRIPTION
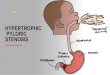
IHPS is the commonest cause for non-bilious vomiting in infants. Treatment is Ramsted's pyloromyotomy either open or laparoscopic.
Citation preview

Infantile Hypertrophic Pyloric
Stenosis (IHPS)
Infantile Hypertrophic Pyloric
Stenosis (IHPS)
AN OVERVIEW AN OVERVIEW

Dr.B.SELVARAJ,MS;Mch;FICS; Dr.B.SELVARAJ,MS;Mch;FICS;
Neonatal & Pediatric Surgeon
Associate Professor
Melaka Manipal Medical College
Melaka- 75150
Malaysia

OBJECTIVES
•To discuss the etiology, clinical features and pathophysiology of IHPS
•To discuss workup to clinch the correct diagnosis
•To discuss the various treatment options
•To make you confident in managing an infant with IHPS

PLAN
• Etiology
• Pathophysiology
• History & Physical
• Differential Diagnosis
• Workup
• Preop preparation
• Management
• Complications

History
• 1646-Sabricus Hildanus-1st described
• 1888-Hirschsprung-Pathology
• 1908-Fredet-Longitudinal incision closed
transversely
• 1912- Ramstedt- omitted transverse closure
• 1986- Tan&Bianchi- Periumbilical incision
• 1992- Lap Pyloromyotomy

Etiology
• Hypertrophy of muscles surrounding pyloric
channel
• Idiopathic
• Various Hypothesis: Milk curd theory& theory of
Aganglionosis
• Male:Female 4:1
• Female parent with the disorder four times more
chances of having affected offspring
• Increased incidence within families

Pathology
• Hypertrophied muscles
• Gastric outlet obstruction
• Nonbilious projectile vomiting
• Gastric fluid loss
• Hypochloremic Hypokalemic Alkalosis
• Paradoxical Aciduria

History&Physical
• Cyclical Nonbilious projectile vomiting at
2wks to 2 months of age
• Usually first born male child
• Failure to thrive
• Loss of weight & Dehydration
• Visible Gastric Peristalsis����VGP
• Olive tumor
• Occasional jaundice

History & Physical
• Nonbilious projectile vomiting at 3 to 6 weeks of age
• Usually first born male child
• Failure to thrive
• Loss of weight & Dehydration
• Visible Gastric Peristalsis����VGP
Olive tumor
– Occasional jaundice


IHPS- Paradoxical Aciduria

Differential Diagnosis
• GE Reflux
• Faulty feeding techniques
• Indirect marker of illness like UTI, ICP and
Congenital adrenal hyperplasia
• Pyloric Atresia
• Pyloric Membrane Neonatal only
• Antral Atresia
• Antral Membrane

Workup
• AXR- Erect :Dilated Stomach
• Barium meal series: String sign and Rail
road track sign
• USG Abdomen: Dilated and elongated
pyloric channel muscles
• Serum electrolytes
• Arterial blood gas analysis

Plain AXR & Barium Meal

USG Abdomen

USG Diagnostic criteria IHPS
• Pyloric channel length����1.5 to 2 cms
(Normal 1.2cms)
• Pyloric channel diameter����1.3 to 1.5cms
(Normal 1 cms)
• Circular muscle thickness���� 4 to 5 mms
(Normal < 2mms)

Preop Preparation
• NPO
• NGT Decompression and gastric lavage
• Correction of dehydration and alkalosis withD5W with 1/2 normal saline
• Serum bicarbonate should be < 28 meq/ ltr and Serum chloride should be > 100 meq/ltr before taking up the child for surgery

Management
• Fredet- Ramstedt’s Pyloromyotomy
����conventional open procedure
• Laparoscopic Pyloromyotomy
• Postop����Progressive increase in feeding
from 8 hrs onwards
• D/C IVF if child tolerates 60ml Q3H

Fredet- Ramstedt’s
Pyloromyotomy

Fredet- Ramstedt’s
Pyloromyotomy

Laparoscopic Pyloromyotomy

Laparoscopic Pyloromyotomy

Complications
• Unrecognised Duodenal perforation
• Occasional intraabdominal bleeding
• Postop persistent vomiting: If > 1Wk Redo
Surgery ���� Torgerson’s muscle incision
• Wound infection/ Wound dehiscence

Etiology
Preop prep
Imaging
• Hypertrophied muscle
• G O Obstruction
• Non bilious vomiting
• Gastric fluid loss
• Hypochloremic alkalosis
• Paradoxical aciduria
• Idiopathic
• Milk curd Theory
• Familial
• AXR- dilated stomach
• Ba Meal- String sign
• USG Abd- dilated &
elongated pyloric muscles
Tt &
Complica
tions
Pathology
IHPS
H & P
• 1st born male child
• Cyclical non bilious
projectile vomiting
• Dehydration& loss of
weight
• Olive tumor
• NPO
• NGT aspiration & gastric
lavage
• Correction of dehydration &
Electrolytes imbalance
• Fredet-Ramstedt’s
Pyloromyotomy
• Unrecognised perforation with
peritonitis
• Occasional bleeding
• Persistent vomiting
• Wound infn & dehiscence
P
M
Stenosis
Infantile Hypertrophic Pyloric
Stenosis


Mindmaps in Surgery