Embed Size (px)
DESCRIPTION
Designed for UG pathology teaching.
Citation preview

Inflammation
and Repair - 2
Dr.CSBR.Prasad, M.D.
V2-May,2011

Revision of lecture-I

The nomenclature used to describe
inflammation in different tissues employs
the tissue name and the suffix “-itis”
e.g
Pancreatitis
Meningitis
Pericarditis
Arthritis

…itis
• Pneumonitis
• Nephritis
• Cystitis
• Balanitis
• Posthitis
• Panniculitis
• Proctitis
• Dactylitis
• Typhlitis
• Pleurisy
• Paronychia
• Bacterial vaginosis
• Cellulitis












What are the cardinal signs of
inflammation?
• Rubor = redness
• Tumor = swelling
• Calor = heat
• Dolor = pain • (described by Celsus 1st. Century AD)
• Functio laesa = loss of function – (added by R. Virchow)

Which sign was introduced by
Virchow?
• Functio laesa = loss of function

Which is the fifth sign of
inflammation?
• Functio laesa = loss of function

Factors that control the fluid
balance between the intravascular
and extravascular compartments
• OP and HP

What happens to total white count
in acute inflammation?
• Usually elevated

Name THREE elements which
make the inflammation possible?
1. Vessels
2. Plasma components
a) Immunoglobulins
b) Complement components
3. Leucocytes

Name THREE differences between
Necrosis and Apoptosis?
In Apoptosis:
• Structures are membrane bound
• Changes occur before death [Until the last moment the cell is alive]
• Absence of inflammation
• ATP dependent process

What makes inflammation a
reality?
Blood vessels

Why we need inflammation?
• To remove infectious / injurious agents
• To remove dead tissue form the body
• It’s protective.

Name some instances where
inflammation is damaging?
• Laryngitis
• Inflammation of the 4th ventricular area
• Encephalitis / Meningitis

Name the acute inflammatory
cells?
• Pyogenic infections – Neutrophil
• Allergic inflammation – Eosinophil
• Viral infections – Lymphocyte

Name the chronic inflammatory
cells?
• Lymphocytes
• Macrophages
• Plasma cells

How do you differentiate acute from
chronic inflammation?
• Onset / duration
• Type of inflammatory cells

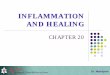
FIGURE 2-1 The major
local manifestations of
acute inflammation,
compared to normal.
(1)Vascular dilation and
increased blood flow
(causing erythema and
warmth)
(2)Extravasation and
extravascular deposition
of plasma fluid and
proteins (edema);
(3)Leukocyte emigration
and accumulation in the
site of injury.


Exudation
The escape of fluid, proteins, and blood cells
from the vascular system into the
interstitial tissue or body cavities is known
as exudation

Terms
• Exudate
• Transudate
• Edema
• Pus


Differences between
Transudate and Exudate
Transudate • Usually seen in
congestive states
• Increased HP
• Sp. Gr: <1.020
• Proteins: <2 gm/dl
• Few leucocytes
Exudate • Seen in inflammatory
states
• Increased vascular
permeability
• Sp. Gr: >1.020
• Proteins: >2 gm/dl
• Many leucocytes


Vascular Events

Vascular events
1. Changes in Vascular Flow and Caliber
2. Increased Vascular Permeability
(Vascular Leakage)
3. Responses of Lymphatic Vessels

Vascular events
1. Changes in Vascular Flow and Caliber
Begins early in inflammation
Consists of the following:
Vasoconstriction (transient – a few seconds)
Vasodilation (first – arterioles, then vascular bed)
Histamine, NO
Vasodilation with increased vascular permeability

Vascular events
1. Changes in Vascular Flow and Caliber
2. Increased Vascular Permeability o Contraction of endothelial cells resulting in increased
interendothelial spaces o [histamine, bradykinin, leukotrienes, substance P]
o Immediate transient response occurs rapidly / short-lived (15–30 minutes)
o Delayed prolonged leakage [begins after a delay of 2 to 12 hours] may be caused by contraction of endothelial cells or mild endothelial damage. Eg: sunburn
o Endothelial injury, resulting in endothelial cell necrosis and detachment
o Direct damage to the endothelium - in burns, or by the actions of microbes, Neutrophils that adhere to the endothelium
o Transcytosis, VEGF
o Newly formed capillaries are leaky

Vascular events

Normal
tight
Gap
junction
Contraction
Causing
vascular
leakage

Vascular events

Vascular events

Vascular events

Vascular events

Vascular events
Although various mechanisms can cause
vascular leak, combination of mechanisms
discussed earlier may play a role in a
given setting

Vascular events
1. Changes in Vascular Flow and Caliber
2. Increased Vascular Permeability
3. Responses of Lymphatic Vessels
• Normally interstitial fluid is drained by lymphatics
• Lymphatics proliferate to handle the increased load
• May carry injurious substances away from the site
• In this process they may get inflammed - Lymphangiitis


Cellular Events

REACTIONS OF LEUKOCYTES IN
INFLAMMATION
• A critical function of inflammation is to deliver leukocytes to the site of injury and to activate the leukocytes to eliminate the offending agents.
• Most important leukocytes in inflammatory reactions are the ones capable of phagocytosis, namely neutrophils and macrophages.
• These leukocytes ingest and kill bacteria and other microbes, and eliminate necrotic tissue and foreign substances.
• Leukocytes also produce growth factors that aid in repair.
• Collateral damage: When strongly activated, leucocytes may induce tissue damage

The processes involving leukocytes
in inflammation consist of:
Recruitment
Recognition
Removal

The inflammatory response consists of
TWO main components:
1. Vascular reaction and
2. Cellular reaction

A critical function of the vascular
inflammatory response is to
deliver leukocytes to the site of
injury in order to clear injurious
agents


Recruitment of Leukocytes to Sites
of Infection and Injury
Extravasation of leukocytes is a coordinated
event of:
• Margination
• Rolling
• Adhesion to endothelium
• Diapedesis (Transmigration)
• Chemotaxis

In order for leukocytes to leave the
vessel lumen, endothelial cells need to
be activated and upregulate adhesion
molecules that can interact with
complementary adhesion molecules on
leukocytes

Up-regulation of adhesion molecules on
endothelial cells is induced by an array
of inflammatory mediators such as
TNF, IL-1, histamine and others
produced by tissue resident
inflammatory cells

Four families of adhesion molecules are involved in leukocyte migration
Selectins
E-selectin (on endothelium)
P-selectin (on endothelium &
platelets; is preformed and stored in
Weible Palade bodies)
L-selectin (leukocytes)
Ligands for E-and P-Selectins are
sialylated glycoproteins (e.g
Sialylated Lewis X)
Ligands for L-Selectin are Glycan-
bearing molecules such as
GlyCam-1, CD34, MadCam-1 Immunoglobulin family
ICAM-1 (intercellular
adhesion molecule 1)
VCAM-1 (vascular adhesion
molecule 1)
Are expressed on
activated endothelium
Ligands are integrins on
leukocytes
Integrins (a + b chain)
Heterodimeric molecules
VLA-4 (b1 integrin) binds to
VCAM-1
LFA1 and MAC1
(CD11/CD18) = b2 integrin
bind to ICAM
Expressed on leukocytes
Mucin-like glycoproteins
Heparan sulfate (endothelium)
Ligands for CD44 on
leukocytes
Bind chemokines


Recruitment of Leukocytes to Sites
of Infection and Injury
Steps in extravasation:
• Margination
Redistribution of leucocytes from the central
column to the periphery – more closer to
endothelium
Movement of neutrophils from the center o the blood vessel to their
perimeter is called as margination.


Margination

Rolling



The two pools
of circulation
in peripheral
blood


Adhesion - Pavementing
Flattening and adhesion of PMNs to
endothelium is called as ADHESION -
Pavementing which precedes
transmigration across endothelium into
extravascular space

Chemotaxis
• Once outside the blood vessel, a
neutrophil is guided towards an infection
by various diffusing chemotactic factors.
Examples include the chemokines and
the complement peptide C5a, which is
released when the complement system is
activated either via specific immunity or
innate immunity.

This is a diagram showing the effect of chemokine concentration
gradient on chemotaxis direction. The attracted cell moves through
the gradient toward the higher concentration of chemokine.

Details of Leukocyte Chemotaxis:
Neutrophil adheres via integrin binding
Integrin binds to FN in ECM
Actually recognizes RGD sequence (arg-gly-asp) in FN (not shown in figure)
RGD is also found in other ECM proteins
Integrin is recycled

Adhesion molecules • They are complimentary molecules present on
leucocytes and endothelium
• Adhesion molecule
• Ligand (binding site)
• Helps in attachment of leucocytes to endothelium
• Their expression is enhanced by cytokines secreted by the altered cells
• IL-1
• TNF
• Chemokines

Adhesion molecules
Weak Adhesion: Selectins - The initial rolling
interactions
Types: L, E and P
Firm Adhesion: Integrins – permanent margination
of leucocytes. Present on leucocytes
Lignads for integrins: ICAM, VCAM

Endothelial - Leukocyte Adhesion Molecules
Complimetary molecules
Endothelial Leukocyte Major Role
P-selectin Sialyl-Lewis X–modified
proteins
Rolling (neutrophils, monocytes,
T-lymphocytes)
E-selectin Sialyl-Lewis X–modified
proteins
Rolling and adhesion (neutrophils,
monocytes, T lymphocytes)
GlyCam-1, CD34 L-selectin Rolling (neutrophils, monocytes)
ICAM-1 CD11/CD18 (β2) integrins
(LFA-1, Mac-1)
Adhesion, arrest, transmigration
(neutrophils, monocytes,
lymphocytes)
VCAM-1 VLA-4 (β1) integrin Adhesion (eosinophils, monocytes,
lymphocytes)

Endothelial - Leukocyte Adhesion Molecules
Relocation / Synthesis

Leukocyte Migration through
Endothelium
Diapedesis:
• Commonly occurs in post capillary venules
• Facilitated by PECAM-1 / CD31
Containment to the site of injury
• CD44
• PECAM-1

Importance of studying leucocyte
adhesion molecules
Genetic deficiencies occur involving these
molecules:
• Leucocyte adhesion deficiency type-1 • Deficient synthesis of LFA-1 and Mac-1 integrins
• Leucocyte adhesion deficiency type-2 • Absence of ligand for E- and P-selectins
Features: Recurrent bacterial infections as a
consequence of impaired leukocyte adhesion
and defective inflammation

Integrins & Disease
• Humans: Leukocyte adhesion deficiency
• Genetic defect
• Can't make Beta2 Subunit
• WBCs can't stick to endothelium; an
essential initial step in fighting infections
and inflammation
• Leads to persistent bacterial infections



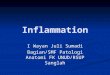
This 10-month-old patient with severe leukocyte adhesion
deficiency type I (LAD I) developed a cervical adenitis
caused by Klebsiella pneumoniae. Following incision and
drainage, wound healing took 4 months.

Labial ulceration from
which Escherichia coli was
cultured in an 8-month-old
girl with leukocyte
adhesion deficiency type 1
(LAD I). Note the thin
bluish scar at the superior
aspect of the labia from an
earlier cellulitis.

This 3-year-old girl had
leukocyte adhesion
deficiency type I (LAD I)
with complete absence of
CD18 expression. Note the
typical gingivostomatitis,
which was culture-negative
for any pathogen.

Omphalitis

E N D


Inflammation

Recruitment of Leukocytes to Sites
of Infection and Injury
The journey of leukocytes from the vessel
lumen to the interstitial tissue, called
EXTRAVASATION

Inflammatory Paracrines
• What causes the characteristic sequence of events in acute inflammation? Various cells at the site of tissue damage or of a specific immune response release regulatory molecules that act locally as paracrines.
• Macrophages and lymphocytes are important sources of inflammatory paracrines. As we have discussed, macrophages release IL-1 and TNF-alpha, which have powerful, widespread effects.
• Also important are mast cells, which are found throughout the body, especially under epithelia. Mast cells are filled with large vesicles containing histamine and other inflammatory paracrines (They also release PG D2, several LTs and TNF-alpha, described below). Factors associated with tissue damage can trigger the exocytosis. But sometimes it is a specific immune response that triggers the release of the inflammatory paracrines.
• Also, various arachidonic acid derivatives are important. Both prostaglandins (notably PG D2) and leukotrienes (LT) can be important, depending on the tissue. Note the effectiveness of aspirin and various NSAIDs in quieting inflammation.
• Complement peptides, C3a and C5a
• Various other molecules including nitric oxide, certain platelet products, kinins, and certain other substances we will not discuss (serotonin, etc)

What types of molecules trigger
inflammation?
• Inflammatory paracrines

Name some cells that release the
paracrine molecules.
• Mast cells
• Macrophages
• Almost every cell can release AA
derivatives

What is complement C5a?
When the complement system is activated,
a small peptide C5a is cleaved from the
protein C5. C5a readily diffuses, causing
chemotaxis and inflammation in general

What change caused by inflammatory
paracrines results in edema in the affected
area?
Increased capillary permeability

Suppose tissue damage triggers the release of a
prostaglandin that causes inflammation in the
area. What specific molecule does the tissue
damage activate that starts the synthesis of the
prostaglandin?
Phospholipase A2
Other enzymes, including COX, then convert
the arachidonic acid to the prostaglandin


The Role of Chemokines in Homing to Inflammation

Tissue Distribution of Chemokines

Introduction to
Chemokine
Families and the
Cells They Affect



Ligands
• In biochemistry and pharmacology, a ligand (Latin ligare = to bind) is a substance that is able to bind to and form a complex with a biomolecule to serve a biological purpose.
• In a narrower sense, it is a signal triggering molecule, binding to a site on a target protein.
• The binding occurs by intermolecular forces, such as ionic bonds, hydrogen bonds and Van der Waals forces. The docking (association) is usually reversible (dissociation). Actual irreversible covalent binding between a ligand and its target molecule is rare in biological systems. In contrast to the meaning in metalorganic and inorganic chemistry, it is irrelevant whether the ligand actually binds at a metal site, as it is the case in hemoglobin.
• Ligand binding to a receptor alters the chemical conformation, that is the three dimensional shape of the receptor protein. The conformational state of a receptor protein determines the functional state of a receptor. Ligands include substrates, inhibitors, activators, and neurotransmitters. The tendency or strength of binding is called affinity.
• Radioligands are radioisotope labeled compounds and used in vivo as tracers in PET studies and for in vitro .