Embed Size (px)
Citation preview

EXTRAORAL RADIOGRAPHY
PRESENTED BY- GAURAV KATHERIYA
JR3

• Introduction
• Types Of Extraoral Radiography And Slight Elaboration
About Techniques
– Indications
– Landmarks
– Interpretations
• Overview

• Extraoral radiographs (outside the mouth) are
taken when large areas of the skull or jaw must be
examined or when patients are unable to open
their mouths for film placement.

• Extraoral radiographs are very useful for evaluating large
areas of the skull and jaws but are not adequate for detection
of subtle changes such as the early stages of dental caries or
periodontal disease.
• There are many type of extraoral radiographs. Some types
are used to view the entire skull, whereas other types focus
on the maxilla and mandible.

Historical aspect

Extra-oral Source
Discovered by
Dr. Hisatugu Numata of Japan, 1933

Father of Panoramic Radiography
•1949, extra-oral films
•X-ray source - stationary
Dr Yrjo Veli Paatero


Indication
• When it is not possible to place the film intraorally as
during trismus.
• To examine the extent of large lesions, especially when
the area of pathology is greater than which can be covered
by an intraoral periapical film.
• When jaws or other facial bones have to be examined for
evidence of disease lesions and other pathological
conditions.

4.To evaluate skeletal growth and development.
5. To evaluate the status of impacted teeth.
6. To evaluate trauma.
7. To evaluate temporomandibular joint area

Drawbacks
• Magnification occurs due to the greater object to
film distance used.
• Details are not well-defined due to the use of cassettes
and intensifying screens.
• For optimum balance between loss of image detail and
reduction of patient exposure medium or high speed
screen,film combinations should be used.
• Contrast is reduced as the secondary radiation
produced by the soft tissues is more.

Definition of Some Extraoral Landmarks
used for Patient Positioning
The Median Plane of the Head
• (Midsagittal Plane)
• line that is coincident with the sagittal suture between the
upper margins of the parietal bones, running from the top
of the skull backwards.
• The Infraorbital Line
This line runs across the face from one infraorbital
margin to the other.

• The Orbitomeatal Line (Canthomeatal Line)
This is an imaginary line from the outer canthus of the
eye to the tragus of the ear.
• This is known as the radiological base line and joins the
upper edge of the auditory meatus with the outer canthus
of the eye.

Fig. 12.1: Diagram showing external guide line used for patient
positioning: 1. Glabellomeatal line,
2. Orbitomeatal line, 3. Inframeatal line, 4. Acanthomeatal line

The Frankfort Horizontal Line
• Is the line which runs from the most inferior portion
of the infraorbital margin of the orbit to the highest
point on the superior surface of the external auditory
meatus.

Most Commonly Used Views For
Maxillofacial Imaging
A. Radiography of Sinuses
• 1. Posteroanterior Projection (also known as occipito frontal
projection of Nasal Sinuses)
There are 2 methods for obtaining this projection.
• a. Posterior Anterior (Granger Projection).
• b. Modified method, Inclined Posterior Anterior (Caldwell
Projection).

• Standard Occipitomental Projection (O° OM)
• Modified Method (30° occipitomental projection)
• Bregma Menton
• PA Water’s

C. Radiography of the Mandible
1. PA Mandible
2. Rotated PA Mandible
3. Lateral Oblique
Anterior body of mandible
Posterior body of mandible
Ramus of mandible

• D. Radiography of Base of the Skull
1. Submento Vertex projection
• E. Radiography of the Zygomatic Arches
1. Jughandle view (A Modification of submentovertex view)
• F. Radiography of the Temporomandibular Joint
1. Transcranial Projection
2. Trans Pharyngeal Projection
3. Trans Orbital Projection
4. Reverse Towne’s Projection
5. Dental panoramic tomograph (including specific TMJ field
limitation techniques)
6. Tomography, both linear and spiral.

G. Radiography of the Skull
• Lateral cephalogram
• True lateral
• PA cephalogram
• PA Skull
• Towne’s Projection

RADIOGRAPHY OF THE
PARANASAL SINUSES
• study the relationship of the sinuses to each other and to the
surrounding structures.
1. Posteroanterior Projection (also known as the Occipitofrontal
Projection of the Nasal Sinuses):-
• two methods for obtaining this projection:-
• A. Posteroanterior (Granger) Projection.
• B.Modified Method, Inclined Posteroanterior(Caldwell) Projection

A. Posteroanterior (Granger) Projection.

OF / PA VIEW1. Nasal Septum
2. Frontal Sinus
3. Maxillary Sinus
4. Ethmoid Sinus
5. Inferior Turbinate
6. Superior orbital fissure
7. Sagittal suture
8. Coronal suture
9. Sphenoid ridge
10. Mastoid process
11. Hard palate
12. Innominate line
13. Petrous ridge
2
1
4
3
5
6
7
8
9
10
12
11
13

Structures Shown
• excellent for evaluating the inner and middle ear
because the petrous pyramid can be viewed through
the orbits.

B.Modified Method, Inclined Posteroanterior
(Caldwell) Projection
• Also known as Occipitofrontal View Or Nose Forehead
Structure Seen:-
1. Frontal Sinuses (Seen Best)
2. Ethmoid Sinuses
3. Maxillary Sinuses
4. Frontal Process Of Zygoma And Zygomatic Process Of
Frontal Bone
5. Superior Margin Of Orbit And Lamina Papyracea
6. Superior Orbital Fissure



RADIOGRAPHY OF THE MAXILLARY
SINUSES
A.Standard Occipitomental Projection (0° OM)
This projection shows the facial skeleton and
maxillary antra., and avoids superimposition of the dense
bones of the base of the skull.
Indications:-
• Investigation of the maxillary antra
• Detecting the following middle third facial fractures
(using Campbell lines) :
• — LeFortI
• — Le Fort II

• Le Fort III
• Zygomatic complex
• Naso-ethmoidal complex
• Orbital blow-out
• Coronoid process fractures
• Investigation of the frontal and ethmoidal sinuses
• Investigation of the sphenoidal sinus (projection
needs to be taken with the patient's mouth open).

• Examine the 0° OM using an approach based
• broadly on that suggested originally by
• McGrigor & Campbell (1950), often referred
• to as Campbell's lines.




B.Modified Method (30° Occipitomental
Projection)
• also shows the facial skeleton, but from a different angle from
the 0° OM, enabling certain bony displacements to be
detected.
• Main indications
• The main clinical indications include:
• • Detecting the following middle third facial
• fractures:
• — LeFortI
• — Le Fort II
• — Le Fort III
• Coronoid process fractures



3. Bregma Menton
Structures Shown
• walls of the maxillary sinus (especially in the posterior areas),
the orbits, the zygomatic arches and the nasal septum.
• It also demonstrates medial or lateral deviations of any part of
the mandible.


4. PA Water’s
• Structures seen
• maxillary sinus, frontal and ethmoidal sinuses.
• The sphenoidal sinuses can be seen if the patient is
asked to open his mouth, whereby the sphenoidal
sinuses are projected on the palate.
• The orbit, frontozygomatic suture, nasal cavity,
coronoid process of the mandible and the zygomatic
arch are also seen.



C. Radiography of the Mandible
I. PA Mandible
•A posteroanterior projection
of the mandibular body and
the ramus.
•The symphysis region is not
well seen because of the
superimposition of the spine.

Indications
• used to study fractures of the posterior third of the
body of the mandible, angles, rami and lower
condylar neck
• mediolateral expansion of the posterior third of the
body or the rami in case of tumors or cystic
lesions,maxillofacial deformities and mandibular
hypoplasia or hyperplasia.



2. Rotated PA Mandible
• used to show the tissues
of one side
• of the face and used to
investigate the parotid
gland
• and the ramus of the
mandible.

Indications
• Stones/calculi in the parotid glands
• Lesions such as cysts or tumours in the ramus to note
any medio-lateral expansion.
• Submasseteric infection — to note new bone
formation.


A. Anterior Body of the Mandible
• Anterior body of the
mandible, position of
the teeth in the same
area.

indications
• evaluate impacted teeth
• fractures
• lesions located in the anterior portion of the
mandible


B. Posterior Body of the Mandible
• Structures seen
• Body of the mandible, position of the teeth in the
• same area, ramus of the mandible, angle of the
• mandible

Indications
• evaluate impacted teeth
• fractures
• lesions located in the posterior border of the
mandible.


C. Ramus of Mandible
• Structures seen
• a view of the ramus
from the angle of the
mandible to the
condyles.

indications
• to evaluate impacted third Molars
• large lesions
• fractures that extend into the ramus of the mandible.


RADIOGRAPHY OF THE BASE OF THE
SKULL1. Submento vertex Projection
Structures seen
• the base of the skull
sphenoidal sinuses
facial skeleton from
below.

Indications
• Destructive/expansive lesions affecting the
palate,pterygoid region or base of skull
• Investigation of the sphenoidal sinus
• Assessment of the thickness (medio-lateral) of the
posterior part of the mandible before osteotomy
• Fracture of the zygomatic arches — to show these thin
bones the SMV is taken with reduced exposure factors.


RADIOGRAPHY OF THE ZYGOMATIC ARCHES1. Jug Handle View (A Modification of the
Submentovertex View)
Structure seen
• A symmetrical axial view of the zygomaticarches.

RADIOGRAPHY OF THE TEMPORO
MANDIBULAR JOINTS
1. Transcranial
Structure seen
• Lateral aspect of:
• Glenoid fossa
• Articular eminence
• Joint space
• Condylar head


Indications
• TMJ pain dysfunction syndrome
• Internal derangements of the joint producing
pain,clicking and limitation in opening
• To investigate the size and position of the disc
• this can only be inferred indirectly from the
• relative positions of the bony elements of the joints
• To investigate the range of movement in the joints.

Diagnostic information
• Open mouth
• The range and type of movement
of the condyle
• A comparison of the degree of
movement on both sides.
• Closed mouth
• The size of the joint space.
• The position of the head of the condyle
within the fossa
• The shape and condition of the glenoid fossa
and articular eminence (on the lateral aspect
only)
• The shape of the head of the condyle and the
condition of the articular surface (on the
lateral aspect only)
• A comparison of both sides.


2. Transpharyngeal (Infracranial or McQueen
Dell Technique)
Structure seen
• Lateral view of:
• Condylar head and neck
• Articular surface


Indications
• TMJ pain dysfunction syndrome
• To investigate the presence of joint disease,particularly
osteoarthritis and rheumatoid arthritis
• To investigate pathological conditions affecting the
condylar head, including cysts or tumours
• Fractures of the neck and head of the condyle


3. Transorbital (Zimmer Projection)
• conventional frontal TM
joint projection.
Structures seen
• The anterior view of the
temporomandibular joint
• Medial displacement of
fractured condyle
• Fracture of neck of condyle
are clearly seen in this view.


4. Reverse Towne’s
Structures seen
• Posterior view of both
condylar heads and
necks

Indications
• To investigate the articular surface of the condyles
and disease within the joint
• Fractures of the condylar heads and necks
• Condylar hypo/hyperplasia


SKULL PROJECTION
1. Lateral Cephalogram
• Indications:-
• orthodontics
• Initial diagnosis — confirmation
of the underlying skeletal and/or
soft tissue abnormalities
• Treatment planning
• Monitoring treatment progress,
e.g. to assess,anchorage
requirements and incisor
inclination

• Appraisal of treatment results, e.g. 1 or 2 months before the
completion of active
• treatment to ensure that treatment targets have been met and to
allow planning of retention.
Orthognathic surgery
• Preoperative evaluation of skeletal and soft tissue patterns
• To assist in treatment planning
• Postoperative appraisal of the results of surgery and long-term
follow-up studies.


2. True Lateral
Structure seen
• shows the skull vault
and facial
• skeleton from the lateral
aspect.

Indications
• Fractures of the cranium and the cranial base
• Middle third facial fractures, to show possible
downward and backward displacement of the
maxillae
• Investigation of the frontal, sphenoidal and maxillary
sinuses

• Conditions affecting the skull vault,particularly:
• — Paget's disease
• — multiple myeloma
• — hyperparathyroidism.
• Conditions affecting the sella turcica, such as:
• — tumour of the pituitary gland in acromegaly.


3. PA Cephalogram
• This projection is identical
to the PA view of the
• jaws, except that it is
• standardized and
reproducible. This makes it
suitable
• for the assessment of facial
asymmetries and
• for preoperative and
postoperative comparisons
in
• orthognathic surgery
involving the mandible.

indications
• used for the assessment of facial asymmetries
• preoperative and postoperative comparisons in
• orthognathic surgeries involving the mandible


4. PA Skull
• Structures seen
• the skull vault, primarily
• the frontal bones and the jaws

indications
• Fractures of the skull vault
• Investigation of the frontal sinuses
• Conditions affecting the cranium, particularly:
• — Paget's disease
• — multiple myeloma
• — hyperparathyroidism
• Intracranial calcification


Towne’s Projection
• Structures seen
• the occipital area of
• the skull. The necks of the condyloid process can
• also be viewed.


‘Panorama’ ‘Tomography’
An
unobstructed
view of a
region in
every
direction
An X-ray technique
for making
radiographs of
layers of tissue in
depth without the
interference of
tissues above and
below the level
PANTOMOGRAPHY

Advantages
• All the teeth and their supporting structures
are shown on one film.
• The technique is reasonably simple
• The radiation dose is relatively low, particularly
with modern DC units with rare-earth intensifying
screens — the dose is equivalent to about three to four
perapical radiographs.

Demerits
• Only structures within the section will be evident and
in focus on the final film.
• image quality is inferior to that of intraoral (periapical
and bitewing) radiographs and interpretation is more
complicated

Indications
• Orthodontic assessment where there is a clinical need
to know the state of the dentition and the
presence/absence of teeth
• To assess bony lesions or an unerupted tooth that are
too large to be demonstrated on intraoral films
• Prior to dental surgery under general anaesthesia

• As part of an assessment of periodontal bone support
where there is pocketing greater than 5 mm
• Assessment of third molars, at a time when
consideration needs to be given to whether they
should be removed or not.
• Fractures of all parts of the mandible except the
anterior region
• Antral disease — particularly to the floor,posterior
and medial walls of the antra

• Destructive diseases of the articular surfaces of
theTMJ
• Vertical alveolar bone height as part of preimplant
planning.

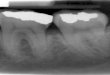
BONY LANDMARKS IN MANDIBLE
97
1
1. Condylar head 2. Sigmoid notch 3. Coronoid process 4. External oblique ridge
5. Mandibular canal
2
3
4
5
6. Post. Border of Ramus 8. Lower border7. Gonial Angle
6
7
9. Mental ridge 11. Mental foramen 10. Genial tubercle
13. Lingula
12. External Oblique Ridge
14. Hyoid bone
8
9
1011
1213

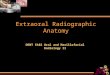
BONY LANDMARKS IN MAXILLA
98
15
15. Glenoid fossa
19. Floor of Max.Sinus
17. Zygomatic Arch16. Articular eminence 18.Post. wall max. sinus
20. Zygomatic process of max. forming innominate line
21. Hard palate 22. Floor of the orbit 23. Nasal septum 24. Incisive foramen
25. Inferior choncha 26. Meatus 27. Frontal process of Z.bone
16
1718
19
2021
22 2329
25
24
26
28.Pterygo max. fissure
30. Maxillary tuberosity29.Spine of the sphenoid bone 31. Lateral pterygoid plate
31
30
28
27

OTHER STRUCTURES
99
32
32. External acoustic meatus 34. Shadow of ear lobe33. Styloid process
35. nose 36. Shadow of Cervical spine
33
34
35
36 37
37. Cervical vertebrae
38
38. Nasopharyngeal space 39. Shadow of uvula
40
39
40 Submandibular fossa




Overview
• Overview





• White SC, Pharoah MJ.Oral Radiology
Principles And Interpretations.6thelsevier::
Missouri; 2009
• Mac Donald,Avery.Dentistry For The Child
And Adolscent.9th.elsevier: Missouri; 2011
• Langland and Langlais.. Principles Of Dental
Imaging.7thed.elsevier: Muir; 2005
• Freny R,Karjodkar.Textbook Of Dental And
Maxillofacial Radiology.6thed.elsevier: Reed;
2000
• Dental radiography, Principles and
Techniques; Haring, Howerton;Third edition.