Embed Size (px)
Citation preview

Malrotation
Abhilash
11/09/2013

Introduction
• Malrotation –
• Group of congenital anomalies resulting from aberrant intestinal rotation and fixation.
• Takes place during the first three months of gestation.
• First reported by William Ladd in 1932.

Epidemiology
• Incidence : 1/6000 live births
• Most present < 1 month
• Incidence in general population – 0.2 to 0.5 %
• No sex/race predilection

Embryology
• 1. Herniation
• 2. Return to the abdomen.
• 3. Fixation.
• mutations in the forkhead box transcription factor FOX - familial malrotation

Key points in embryology
• Intestinal rotation starts at 5th week.
• Midgut – SMA
• Rotation takes place around SMA axis
• 270 degree counterclock wise rotation of prearterial and post arterial limb.
• Ladds bands attach to the cecum irrespective of its postion at the end of rotation from right paracolic region.








Nonrotation
• Neither colon or duodenum undergo rotation
• Most common form of malrotation.
• M:F=2:1

• Duodenum not posterior to SMA
• Ligament of Treitz fails to reach its normal position is right upper quadrant.
• Midgut mesentry is narrow and highly mobile.
• May cause
• Duodenal obstruction abnormal peritoneal bands.
• Acute midgut volvulus.


Incomplete rotation
• Counter clock wise rotation of only 180 degrees.
• Caecum in the epigastrium overlying 3rd part of duodenum.
• Most common form of surgically treated malrolation.

REVERSE ROTATION
• Rotates clockwise.
• DJ loop anterior to SMA and transverse colon posterior to SMA.
• Causes
• Compression of colon by SMA -> obstruction.
• Ileocecal volvulus- due to inadequate fixation of right colon.

Stringers classification
• I – Non rotation of colon and duodenum
• IIA – Pure duodenal nonrotation
• IIB- Reversed rotation of duodenum and colon
• IIC – Reversed rotation of duodenum only
• IIIA – Nonrotation of colon
• IIIB- Incomplete fixation of hepatic flexure
• IIIC- Incomplete attachment of cecum and mesocecum


Associated anomalies(seen in 30%-60%)
• Duodenal atresia / stenosis / web
• Congenital diaphragmatic hernia
• Gastroschisis
• Omphalocele
• Choanal atresia
• Polysplenia / asplenia
• Congenital megacolon

How does it present.
• Asymptomatic
• Midgut volvulus
• Mesocolic hernias.
• Duodenal and jejunal obstruction.
• Colonic obstruction.

Clinical features in adults
• Intermittent cramping or persistent aching pain.
• Severe abdominal cramping followed by diarrhea - chronic volvulus.
• Vomiting - bilious /non bilious , variable in duration and frequency.
• Malabsorption - diarrhea, nutritional deficiencies
• Rare - obstructive jaundice, chylous ascites and superior mesenteric vein thrombosis

Plain radiograph
• No pathognomonic signs.
• Right-sided jejunal markings
• Absence colonic shadow in RIF
• Features of complications
- Dilated bowel loops
- Air fluids levels
- Pneumoperitoneum

Ultrasound
• Reversal of the normal anatomic relationship between the SMA and
• “whirlpool sign” - midgut volvulus.
• “bird beak” appearance – duodenal obstruction.
• false-positive rates of up to 21%


Upper GI contrast study
>incomplete duodenal obstruction, usually in the third portion;
>ligament of Treitz not to the left of the midline or at the level of the gastric antrum;
>abnormal position of the proximal jejunal loops to the right of the midline; and
>deformity of the duodenum with a bird's beak, corkscrew,• or coiled• configuration


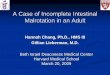
CT Abdomen
• Anatomic location of small bowel on right and colon on left
• Relationship of the superior mesenteric vessels – “vertically placed or inverted sides”
• Aplasia of the uncinate process
• Features of volvulus / obstruction / gangrene
• Other associated anomalies

Reversal of SMA and SMV Whirlpool sign

Management
• Supportive management.
• Surgical management – Ladds procedure.

Ladd's procedure

Post operative care
• nasogastric decompression
• total parenteral nutrition until return of bowel function.

• Mortality from midgut
• volvulus with severe bowel compromise may exceed 30%.
• Long-term complications
1. adhesive small bowel obstruction (10%),
2. recurrent volvulus,
3. short gut syndrome.

References
• Ladd WE. Congenital obstruction of the duodenum in children. N Engl J Med. 1932;206:277–83.
• Principles and Practice of Pediatric Surgery, 4th Edition. Keith T Oldam.
• Shackelford’s Surgery of the Alimentary tract 7th edition.
• Stringer Pediatric Gastrointestinal Imaging and Intervention, 2nd edition


























![Disorders of intestinal rotation and fixation (‘‘malrotation’’)deepblue.lib.umich.edu/bitstream/handle/2027.42/46708/... · 2020. 2. 13. · consequences [4]. ‘‘Malrotation’’](https://img.pdfslide.net/doc/110x75/60afb5330f88520c4e13c968/disorders-of-intestinal-rotation-and-ixation-aamalrotationaa-2020-2.jpg)