Embed Size (px)
Citation preview

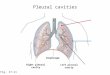
THE PLEURA

PLEURAL EFFUSION
• CAUSES1.Increase microvascular pressure in
lungs,CHF2.Reduce plasma oncotic pressure3.Increase microvascular permeability4.Reduced lymphatic draniage5.Passage of peritoneal fluid across defects in
the diaphragm

•Transudate or exudate

• Hemothorax• Chylothorax

• Radiological appearances of pleural fluid
Free fluidLoculated fluidEmpyema

• Free fluid• it casts a shadow of water
or soft tissue density

• The most dependent part of pleura is posterior costophrenic angle first accumulate here and is seen on lateral CXR

• when more fluid accumulates it fill the lateral costophrenic angle and becomes visible on frontal CXR,with increasing pleural effusion homogenous opacity spreads upward,obscuring the lung base,this opacity has a well defined ,concave upper edge is higher laterally than medially and obscures the diaphragmatic shadow,frequently track into pleural fissures.

Massive pleural effusion will cause opaque hemithorax with contralateral mediastinal shift.If there is complete collapse of underlying lung shift towars side of collapse may occur.

• Illustration of the chest, depicted in an upright position from the lateral aspect, shows a small effusion accumulating in the posterior costophrenic (CP) sulcus. Such small effusion cannot be detected on the frontal view but can be visible on the lateral radiographic view as blunting of the posterior CP angle

• Depiction of upright posteroanterior and lateral views of the chest (using overlay on actual normal radiograph) demonstrates the radiographic appearance of small left effusion as the one in the previous image. The blue arrow points to the effusion.

• Illustration of the chest, depicted in an upright position from the lateral aspect, shows a larger small effusion accumulating in the lower chest, which can be detected on both lateral and frontal radiographic views. This effusion produces blunting of the lateral costophrenic angle on the frontal view.

• Depiction of upright posteroanterior and lateral views of the chest (using overlay on actual normal radiograph) demonstrates the radiographic appearance of a larger small left effusion as the one in the previous image. The blue arrows point to the effusions.

• Illustration of the chest, depicted in an upright position from the lateral aspect. This image shows a moderate effusion accumulating in the lower chest, which can be seen on both the frontal and lateral views as a dependent density with meniscal-shaped margin. Note that the actual fluid upper margin is horizontal. However, there is more fluid posteriorly and laterally due to the shape of the chest and recoil characteristics of the lung.

• Illustration of upright posteroanterior and lateral views of the chest (using overlay on actual normal radiograph) demonstrates the radiographic appearance of a moderate left effusion, as in the previous image. The blue arrows point to the effusions.

• Illustration of the chest, depicted in supine position from the lateral aspect, shows a moderate effusion accumulating in the posterior aspect of the chest. This layering effusion can be visible on the frontal view as an increased haziness. The vascular structures can be seen through this density.

• Posteroanterior supine view of the chest in a 60-year-old man with right-sided effusion. The pleural fluid is layering, given the position of the patient. There is asymmetric density with increased haziness in the lower right hemithorax (blue arrow). Note that the pulmonary vascular structures are not obscured or silhouetted by the vague density but, rather, are still visible through it (open arrow).

• Posteroanterior chest radiograph in a 42-year-old woman with breast cancer shows blunting of the right cardiophrenic angle (arrow) with slight elevation of the right hemidiaphragm.

• Lateral chest radiograph of a 42-year-old woman with breast cancer shows a crescent-shaped opacity is present in the posterior costophrenic sulcus (arrow). Minimal amount of fluid can be seen in the inferior aspect of the right major fissure. The findings are compatible with right pleural effusion. Some of the fluid is infrapulmonary.

• Right lateral decubitus view in a 42-year-old woman with breast cancer confirms a right pleural effusion by demonstrating dependent layering of the fluid (arrows).

• Follow-up posteroanterior chest radiograph in a 42-year-old woman with breast cancer shows an opacity (E) in the lower left hemithorax with obliteration of the left hemidiaphragm and curvilinear upper margin consistent with effusion. Note the extension of the fluid into the left major fissure (arrow) and mediastinal shift to the right.


meniscus

• Diffrentiation between ascites and pleural effusions





bilateral pleural effusion with meniscus sign


• The Serratus anterior muscle can produce an opacity that may resemble pleural tickening. This is sometimes referred to as a "bowling-pin" silhouette.
• "When the muscle is well developed, the medial edge of this silhouette may be superimposed upon the air shadow of the lung in a variety of ways. When it overlies the apex of the lung, it gives rise to the companion shadow; when overlying the midlateral lung edge and costophrenic angle it may mimic pleural and/or extrapleural disease. Recognition of the various possible patterns is important to prevent overdiagnosis of disease, particularly asbestosis."

prominent serratus muscles bilaterally. This apparance can be mistaken for pleural effusion or
pleural thickening (single white arrow).

Unenhanced CT scan of thorax in 79-year-old man shows relatively low density (8.8 HU; SD, 13.3) 2,549-mm2 right-sided pleural effusion (circle). Patient had pleural exudate
secondary to colon carcinoma with pleural metastasis (white arrows).
Read More: http://www.ajronline.org/doi/full/10.2214/AJR.08.1286

Contrast-enhanced axial CT scan of thorax in 80-year-old woman with congestive heart failure showing bilateral loculated pleural effusion. CT density measurement of right effusion (circle) 691
mm2 in size was 14.5 HU with SD of 19.8. Fluid was proven to be transudate at thoracentesis.
Read More: http://www.ajronline.org/doi/full/10.2214/AJR.08.1286

Large right effusion (red arrow) displacesthe heart to the left
(yellow arrow

• Calcinosis in a patient with CREST syndrome. Also note the encapsulated pleural empyema on the right side.
• Related Articles:

cp

hydropneumo

• A large left sided pleural effusion is present with no fluid seen on the right. No evidence of cardiomegaly or pulmonary venous congestion. No evidence of trauma.
• Multiple surgical clips are seen in the right supraclavicular fossa.


• Atypical distribution
• Lamellar effusions are the shallow collections between the lung surface and the visceral pleura sometimes sparing the costophrenic angle.


• Subpulmonic effusions Large effusions accumulate between the diaphragm and undersurface of the lung mimicking elevation of hemidiaphragm.

subpulmonic effusion




• The contour of diaphragm is altered ,its apex being more lateral,there may be some blunting of costophrenic angle or tracking of fluid into the fissures.On the left side increase distance between the gastric bubble and lung base seen.

• A large right pleural effusion may collect in azygoesophageal recess and mimic retrocardiac mass.The reasons for atypical distribution is not clear but it may be associated with abnormality of underlying lung.

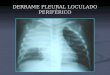
• LOCULATED FLUID• Pleural space may be partially obliterated
by pleural disease.causing fusion of parietal and visceral layers.
• An encysted effusion is often associated with free pleural fluid or other pleural shadowing and may extend into the fissure.

loculated effusion


• Loculated effusion in the minor fissure (arrow). The opacity is smoothly marginated and biconvex.

• Frontal and lateral views of an 89 year-old female with an oval soft tissue density superimposed on the minor fissure on both the frontal and lateral views. The lesion has slight "points" where it abuts the minor fissure, a sign of a "pseudotumor" or "vanishing tumor" in the minor fissure. There are usually more signs associated with congestive heart failure than are seen in this patient.

• Axial computed tomography images of the lower chest in 51-year-old patient with acute lymphoblastic leukemia. A small, dependent, crescent-shaped area with attenuation similar to that of water in the right hemithorax is consistent with a tiny right pleural effusion (arrow). This effusion is most obvious on the mediastinal window.

• Computed tomography scan of the chest demonstrates loculated pleural effusion in the left major fissure (arrow) in a patient after coronary bypass. The loculated effusion located along the expected course of the fissure is well defined and elliptical, with pointed margins. The fluid is similar to water in its attenuation.

• Computed tomography scan of the chest demonstrates a loculated pleural effusion (E) in the left hemithorax. The loculated effusion is well defined and elliptical and similar to water in its attenuation.

• These have little depth but considerable width like biconvex lens.
• Differentiate it from extrapleural opacities which have much sharper outline with tapered smooth concave edges where they meet the chest wall. For Differentiation CT and USG are particularly helpful.

• Fluid may become loculated in one or more of the interlobar fissures,This is uncommon seen in CHF.Appearance depends on which fissure is involved.Fluid collecting in horizontal fissure produces a lenticular,oval or round shadow with well demarcated margins.

• Loculated fluid in oblique fissure is better seen on lateral CXR and the typical lenticular configuration is seem.
• Following treatment they may disappear rapidly and hence known as pseudo or vanishing tumors,They may recur in subsequent episode of heart failure

•Empyema• May be suspected on plain film by
spontaneous appearance of fluid level in pleural effusion but best seen on CT or USG.
• On CT empyema has a lenticular shape and may compress underlying lung.Fluid with or without gas may be present in pleura,both layers of pleura may be thickened.









• Pleural thickening progress to pleural rind so rapid Dx and treatment required,surgical decortication may be necessary bcz it cause respiratory function impairment.

• Multiple septations may be broken down by fibrinolytic agent like urokinase ,100,000 units instilled in 50ml normal saline,drain clamped for 1 hour after which free drainage or low pressure suction done.treatment may be repeated daily for 5 days.

• USG appearance of pleural fluid
• USG is an excellent method for locating loculated pleural fluid prior to aspiration.
• Transudate is anechoic• Exudate may or may not contain reflective
material• Septations can be seen• pleural mass can be seen

fetal pleural effusion


• Ultrasonogram of the right lower chest in a 60-year-old man with a right pleural effusion. This sagittal study was performed with the patient seated and confirms the presence of the effusion as slightly complex but mostly anechoic (E) in the right hemithorax. Note the echogenic curvilinear diaphragm (arrow).


m