Embed Size (px)
Citation preview
POSTERIOR FOSSA MALFORMATIONS
Dr.Archana Koshy
1. Posterior fossa anatomy
2. Chiari malformations
3. Dandy walker malformation
4. Joubert syndrome
5. Rhomencephalosynapsis
6/8/2017 Posterior Fossa Malformations 2
• Congenital posterior fossa anomalies may result from inherited (genetic) or acquired (disruptive) causes.
• A malformation is defined as a congenital morphologic anomaly of a single organ or body part due to an alteration of the primary developmental program caused by a genetic defect .
• Gene mutations causing malformations may be de novo (ie, new in the affected child, rather than present in or transmitted by the parents) or inherited from the parents.
6/8/2017 Posterior Fossa Malformations 3
• The cerebellum is one of the earliest cerebral structures to develop.
• Its development is also unusually protracted as cellular proliferation, migration, and maturation extend into the first few postnatal months.
• Neural structures in the posterior fossa - Embryonic hindbrain (rhombencephalon)
• Mesencephalon - Midbrain structures. (Mesodermal elements give rise to the meninges and bone.
6/8/2017 Posterior Fossa Malformations 4
• The Posterior fossa is the largest and deepest of all the cranial
fossae .
• Bowl shaped, relatively protected space that lies below the tentorium.
• Contains the HINDBRAIN – Brainstem , the vermis anteriorly and the
cerebellar hemispheres posterolaterally .
• Posterior fossa CSF containing spaces include
1. Part of the cerebral aqueduct
2. Fourth ventricle
3. CSF cisterns that surround the brainstem and cerebellum .
6/8/2017 Posterior Fossa Malformations 5
BONE
• Anterior wall –
1. Dorsum sellae of the sphenoid body
2. Clivus of the basioccipital bone
• Lateral wall –
1. Petrous temporal bone
• Floor – Occipital squamae
• Superiorly – with the supratentorial compartment through the
U shaped tentorial incisura
• Inferiorly – Cervical subarachnoid space through the ovoid
foramen magnum .6/8/2017 Posterior Fossa Malformations 6
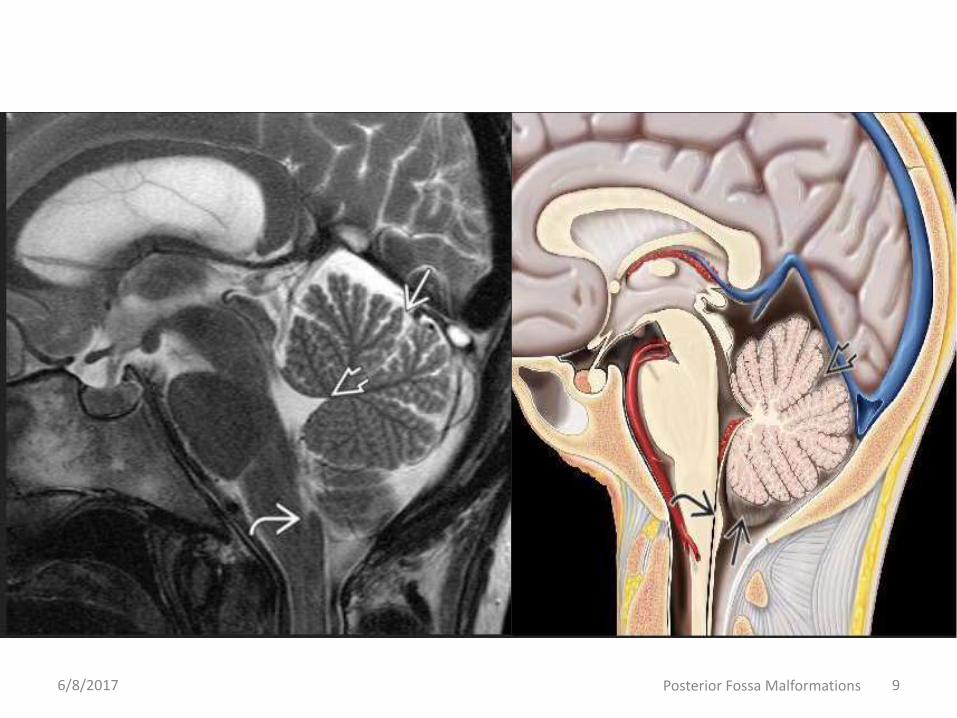
• Conventional magnetic resonance (MR) imaging allows
detailed evaluation of the anatomy of the posterior fossa
and its contents.
• A midline sagittal T1- or T2-weighted sequence is ideal for
showing the size of the posterior fossa, the shape and size
of the vermis, and the size and morphology of the fourth
ventricle and brainstem
6/8/2017 Posterior Fossa Malformations 7
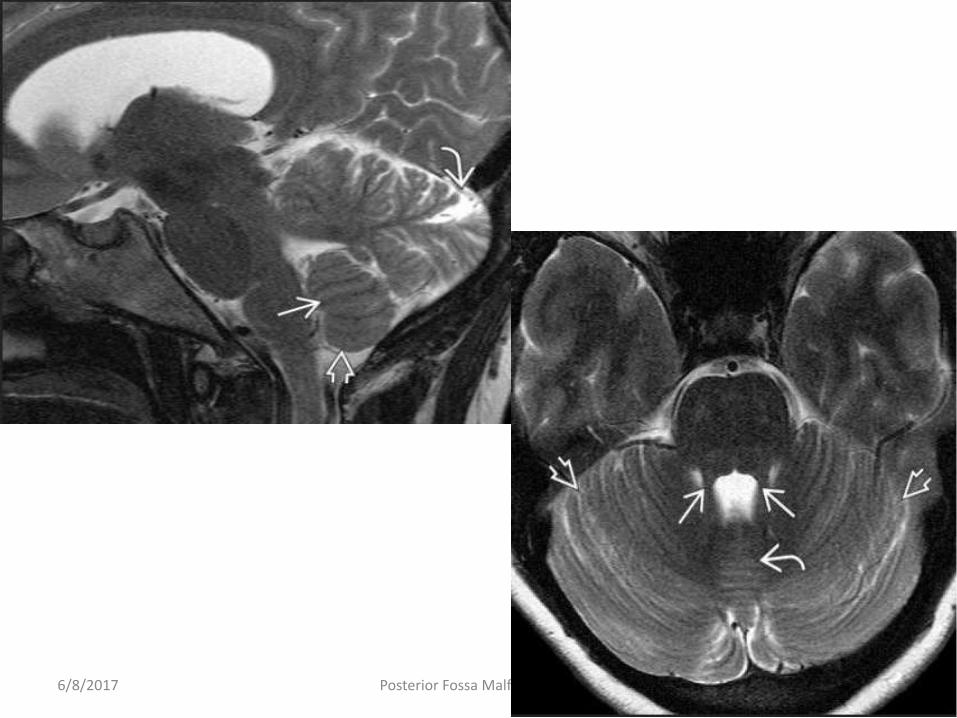
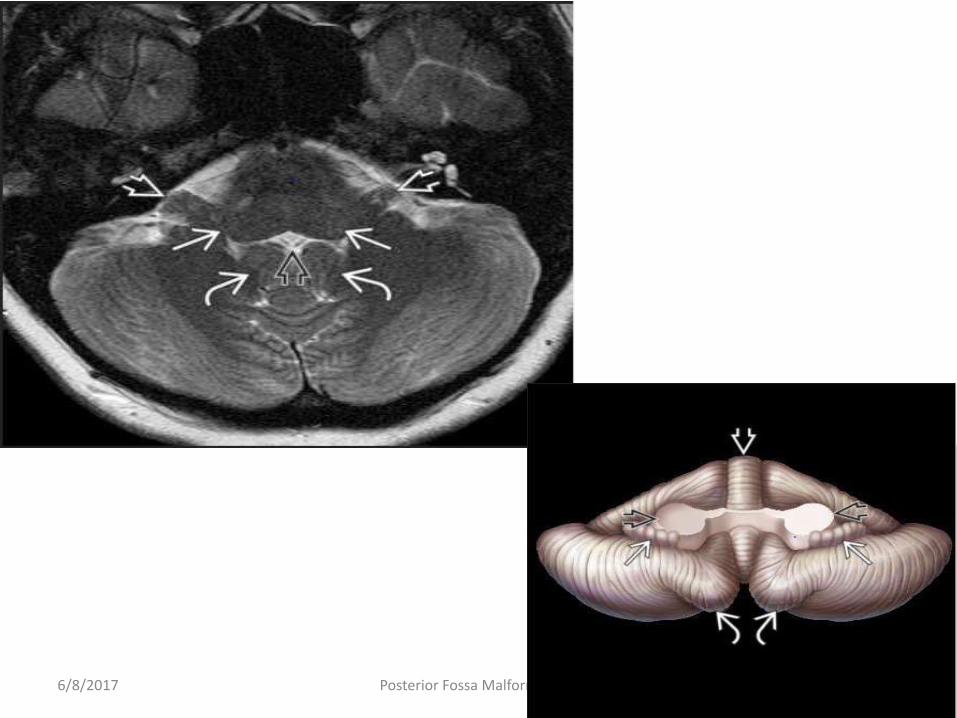
• BRAINSTEM
• The brainstem has three anatomic divisions: The midbrain, pons, and
medulla.
• The midbrain (mesencephalon) lies partly above and partly below the
tentorium.
• The bulb-shaped pons nestles into the gentle curve of the clivus.
• The medulla is the most caudal brainstem segment and represents the
transition from the brain to the spinal cord.
• An important imaging landmark is the prominent “bump” along the
dorsal medulla created by the nucleus gracilis.
• This demarcates the junction between the fourth ventricle (obex) and
central canal of the spinal cord. The nucleus gracilis normally lies above
the foramen magnum.
6/8/2017 Posterior Fossa Malformations 8
6/8/2017 Posterior Fossa Malformations 9
6/8/2017 Posterior Fossa Malformations 10
6/8/2017 Posterior Fossa Malformations 11
6/8/2017 Posterior Fossa Malformations 12
•ARNOLD CHIARI MALFORMATIONS
6/8/2017 Posterior Fossa Malformations 13
• Chiari malformations were first described in the late nineteenth
century by the Austrian pathologist Hans Chiari.
• He described what seemed to be a related group of hindbrain
malformations associated with hydrocephalus and divided them into
three types: Chiari 1-3.
• Chiari 1 and 2 are pathogenetically distinct disorders.
6/8/2017 Posterior Fossa Malformations 14
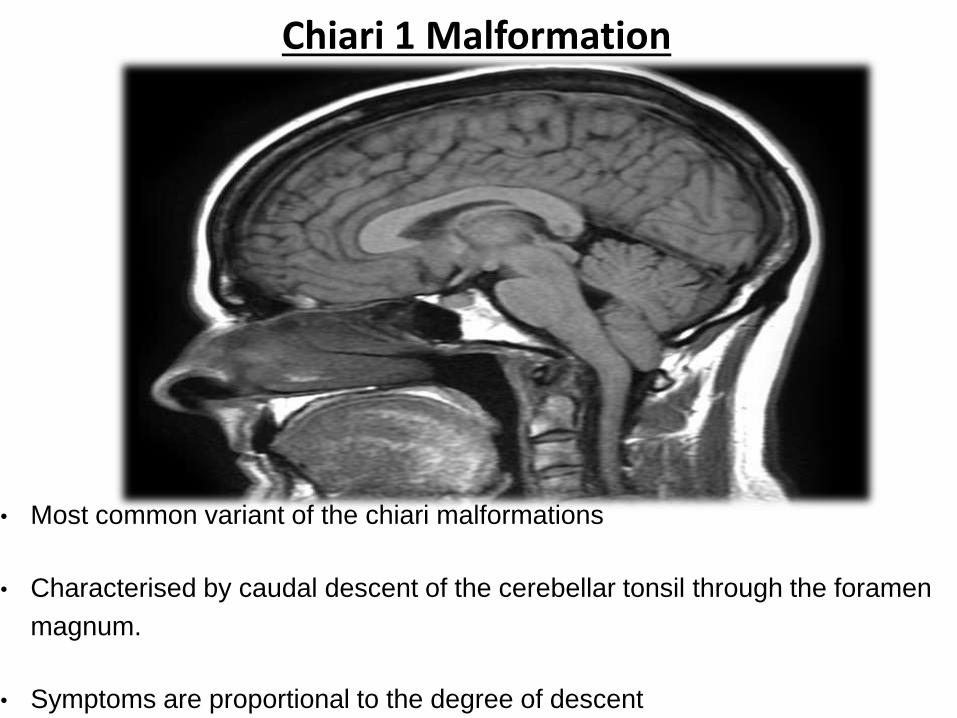
Chiari 1 Malformation
• Most common variant of the chiari malformations
• Characterised by caudal descent of the cerebellar tonsil through the foramen
magnum.
• Symptoms are proportional to the degree of descent
ETIOLOGY
• The pathogenesis of CM1 is incompletely understood and remains
controversial.
• Primary paraxial mesodermal insufficiency with underdeveloped occipital
somites has also been invoked to explain the development of CM1.
• Other theories suggest that disorders of neural crest-derived elements
could lead to hyper- or hypoossification of the basi-chondro-cranium,
resulting in morphometric changes in the posterior fossa.
• A combination of altered bony anatomy and abnormal CSF
hydrodynamics is the most widely accepted concept
PRESENTATION
• Between one-third and one-half of all patients with imaging findings
consistent with CM1 are asymptomatic at the time of diagnosis.
• Presentation of symptomatic CM1 differs with age.
• Children who are two years and younger most commonly present with
oropharyngeal dysfunction (nearly 80%).
• Those between three and five years present with headache (57%) or
symptoms related to syringomyelia (86%) and scoliosis (38%).
• Uncommon presentations include hypersomnolence and sleep apnea.
• Valsalva-induced suboccipital headache (i.e., with coughing or
sneezing), neck pain, and syncope are common in adults.
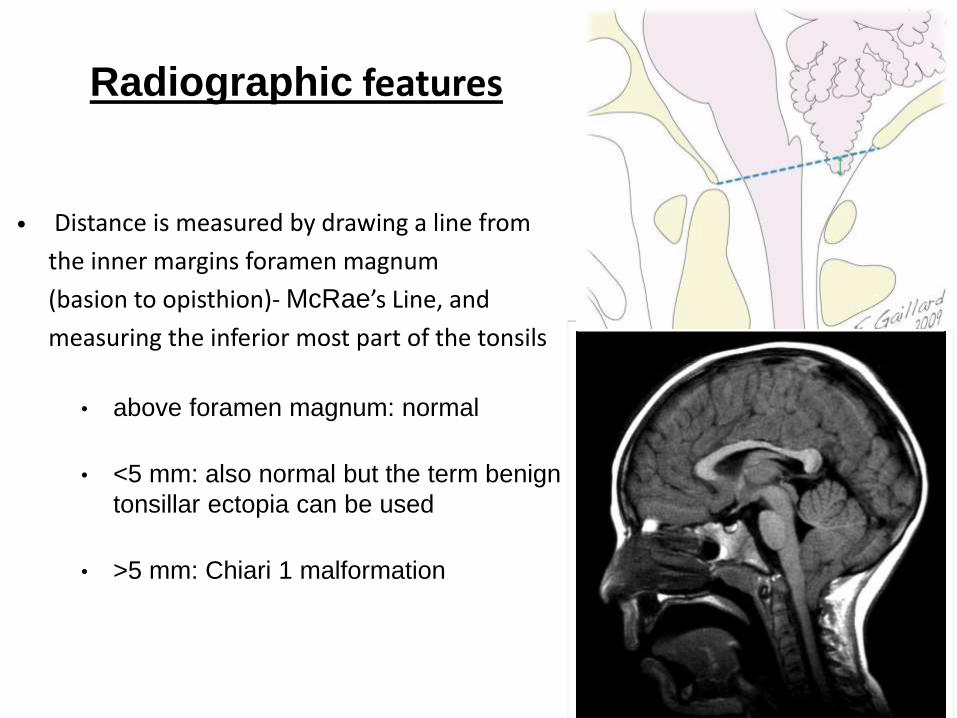
Radiographic features
• Distance is measured by drawing a line from
the inner margins foramen magnum
(basion to opisthion)- McRae’s Line, and
measuring the inferior most part of the tonsils
• above foramen magnum: normal
• <5 mm: also normal but the term benign
tonsillar ectopia can be used
• >5 mm: Chiari 1 malformation
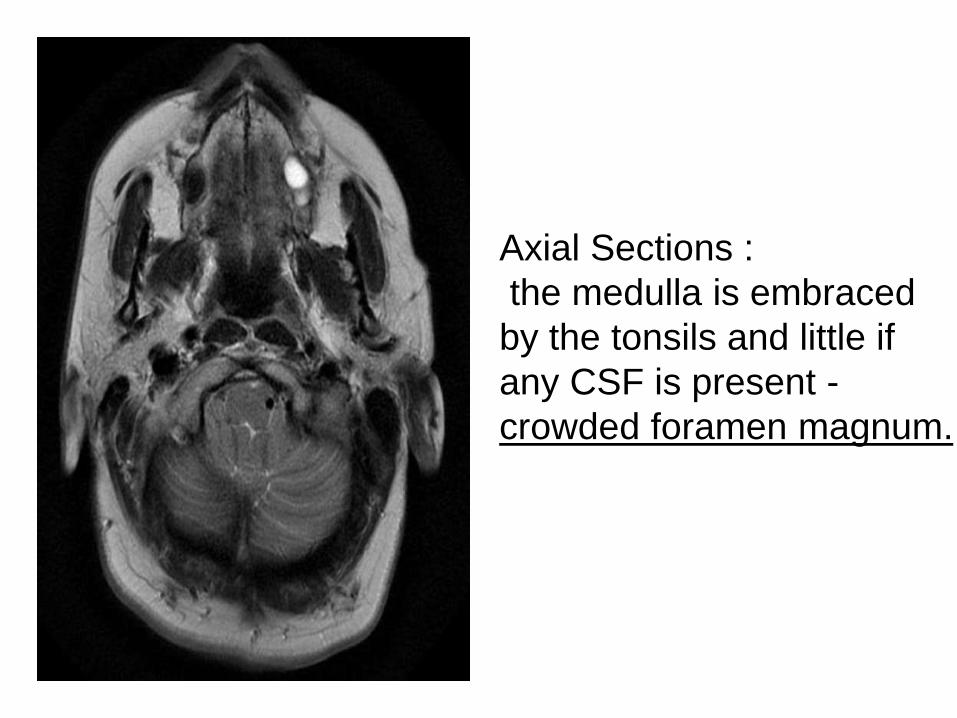
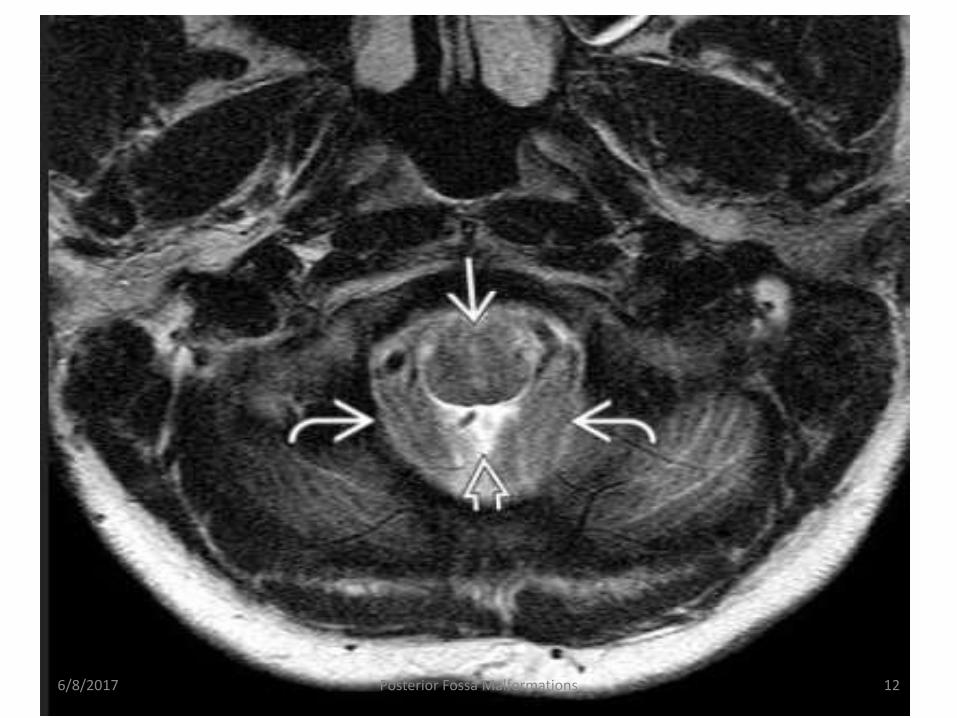
Axial Sections :
the medulla is embraced
by the tonsils and little if
any CSF is present -
crowded foramen magnum.
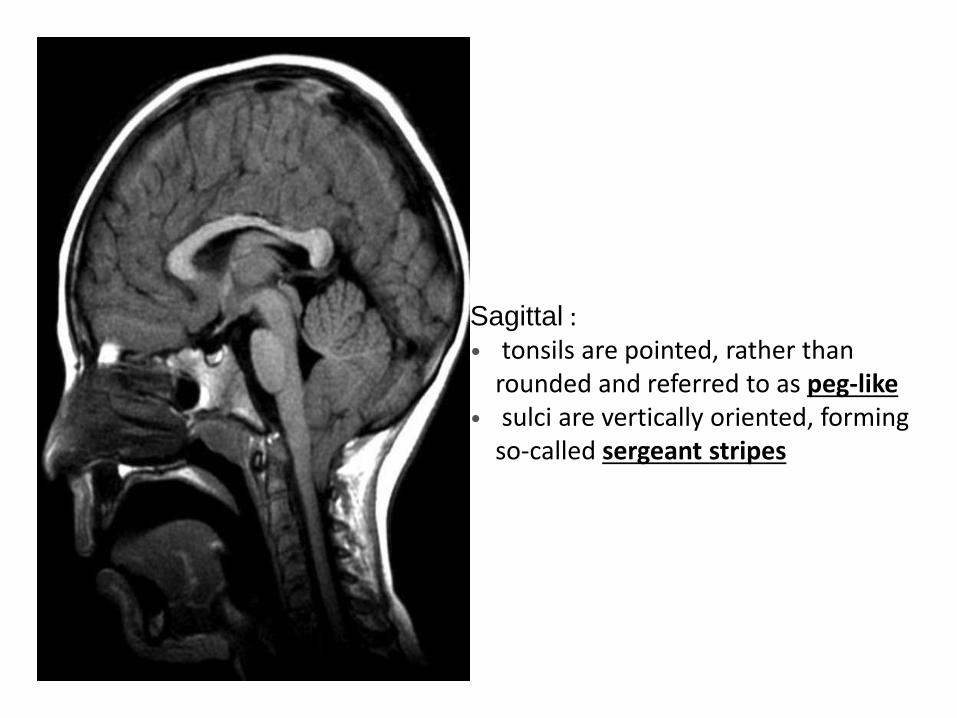
Sagittal :• tonsils are pointed, rather than
rounded and referred to as peg-like• sulci are vertically oriented, forming
so-called sergeant stripes
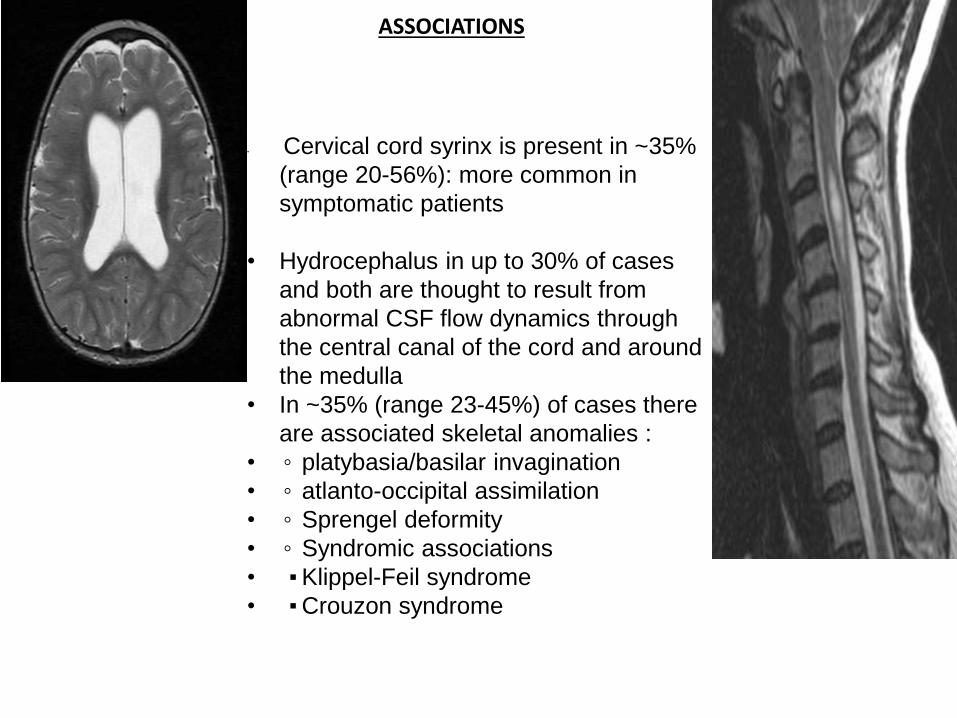
ASSOCIATIONS
• Cervical cord syrinx is present in ~35%
(range 20-56%): more common in
symptomatic patients
• Hydrocephalus in up to 30% of cases
and both are thought to result from
abnormal CSF flow dynamics through
the central canal of the cord and around
the medulla
• In ~35% (range 23-45%) of cases there
are associated skeletal anomalies :
• ◦ platybasia/basilar invagination
• ◦ atlanto-occipital assimilation
• ◦ Sprengel deformity
• ◦ Syndromic associations
• ▪Klippel-Feil syndrome
• ▪Crouzon syndrome
TREATMENT OPTIONS.
• Asymptomatic tonsillar ectopia in the absence of an associated syrinx or
scoliosis is usually not treated.
• Periodic surveillance of patients with documented hydrosyringomyelia is
generally recommended, as 12% of syringes show increase in size and
may require craniocervical decompression if symptoms worsen.
• Treatment of symptomatic CM1 attempts to restore normal CSF fluid
dynamics at the foramen magnum .
• A suboccipital/posterior C1 decompression with or without partial tonsillar
resection is the most common procedure.
DIFFERENTIAL DIAGNOSIS• Congenital tonsillar descent (CM1) must be distinguished from normal variants
(mild uncomplicated tonsillar ectopia).
• The most important pathological differential diagnosis is acquired tonsillar
herniation caused by INCREASED INTRACRANIAL PRESSURE OR
INTRACRANIAL HYPOTENSION.
• Approximately 20% of patients with idiopathic intracranial hypertension
(“pseudotumor cerebri”) exhibit cerebellar tonsillar ectopia ≥ 5 mm.
• Half of these patients exhibit a peg-like tonsil configuration, and many have a
low-lying obex.
• Other conditions that reduce posterior cranial fossa volume can also displace
the tonsils below the foramen.
• Such causes of cranial constriction include CRANIOSYNOSTOSIS,
ACHONDROPLASIA, ACROMEGALY, AND PAGET DISEASE.
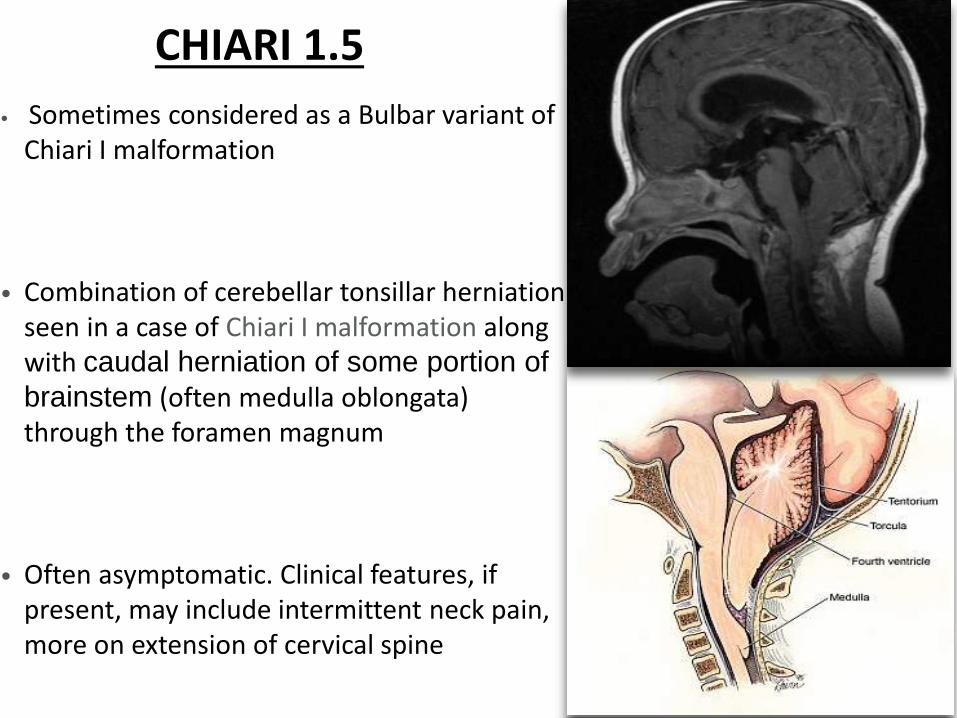
CHIARI 1.5
• Sometimes considered as a Bulbar variant of Chiari I malformation
• Combination of cerebellar tonsillar herniation seen in a case of Chiari I malformation along with caudal herniation of some portion of
brainstem (often medulla oblongata) through the foramen magnum
• Often asymptomatic. Clinical features, if present, may include intermittent neck pain, more on extension of cervical spine
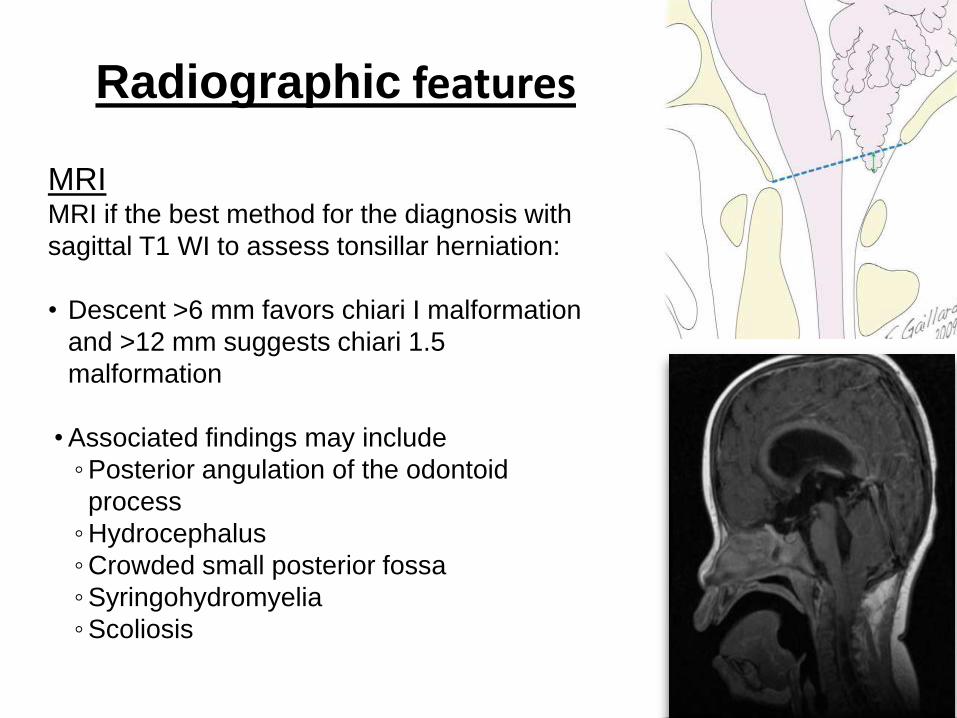
Radiographic features
MRIMRI if the best method for the diagnosis with
sagittal T1 WI to assess tonsillar herniation:
• Descent >6 mm favors chiari I malformation
and >12 mm suggests chiari 1.5
malformation
•Associated findings may include
◦Posterior angulation of the odontoid
process
◦Hydrocephalus
◦Crowded small posterior fossa
◦Syringohydromyelia
◦Scoliosis
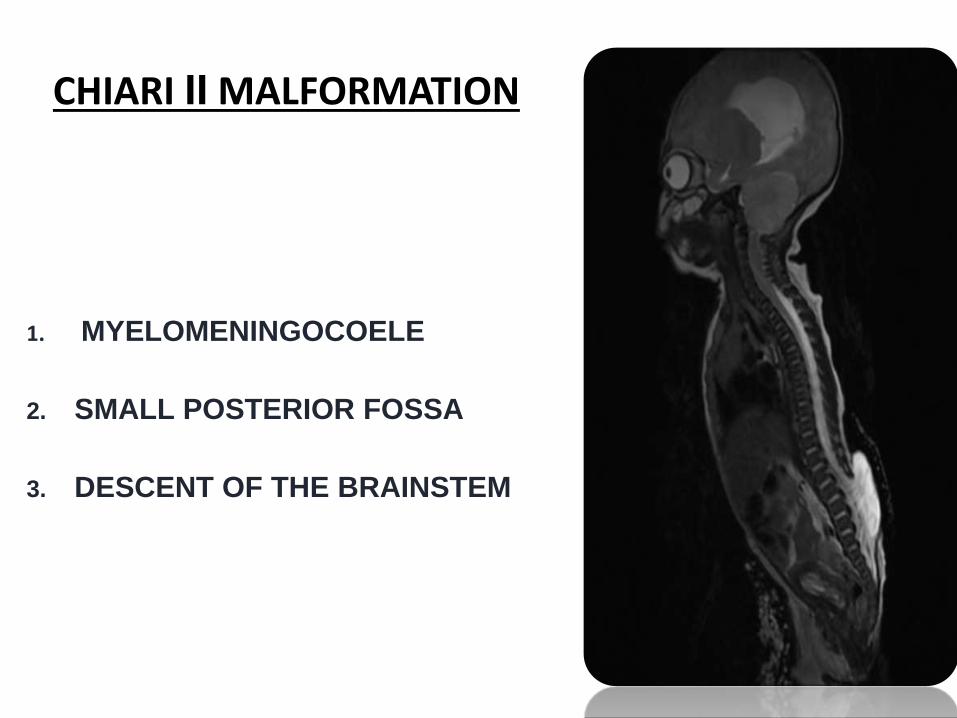
CHIARI II MALFORMATION
1. MYELOMENINGOCOELE
2. SMALL POSTERIOR FOSSA
3. DESCENT OF THE BRAINSTEM
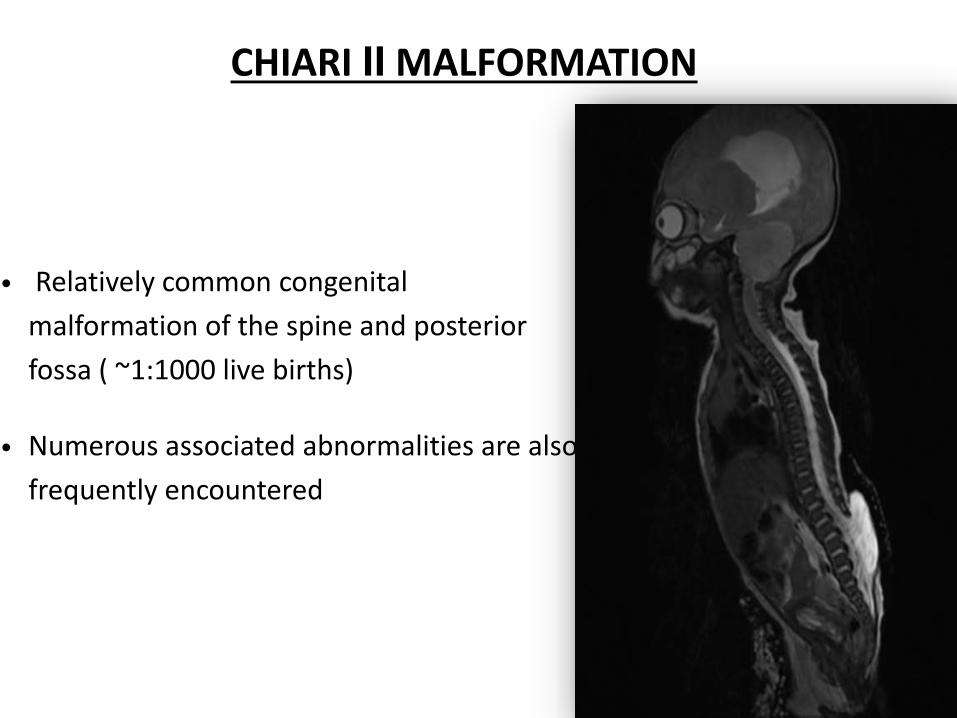
CHIARI II MALFORMATION
• Relatively common congenital
malformation of the spine and posterior
fossa ( ~1:1000 live births)
• Numerous associated abnormalities are also
frequently encountered
• CM2 is a disorder of neural tube closure but also involves paraxial
mesodermal abnormalities of the skull and spine.
• A number of steps are required for proper neural tube closure and formation of
the focal expansions that subsequently form the cerebral vesicles and
ventricles.
• Skeletal elements of both the skull and vertebral column become “modeled”
around the neural tube.
• Only if the posterior neuropore closes will the developing ventricles expand
sufficiently for a normal-sized posterior fossa to form around the hindbrain.
• If this does not happen, the cerebellum develops in a small posterior fossa
with abnormally low tentorial attachments.
• The growing cerebellum is squeezed cephalad through the tentorial incisura
and stretched inferiorly through the foramen magnum (FM).
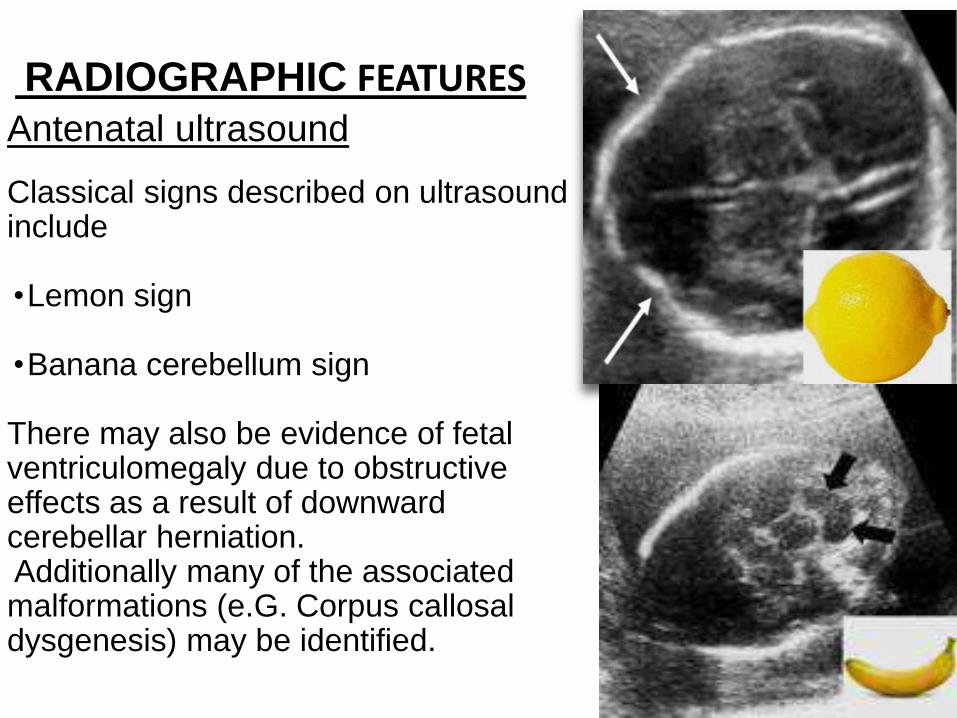
RADIOGRAPHIC FEATURESAntenatal ultrasound
Classical signs described on ultrasound include
•Lemon sign
•Banana cerebellum sign
There may also be evidence of fetal ventriculomegaly due to obstructive effects as a result of downward cerebellar herniation.Additionally many of the associated malformations (e.G. Corpus callosaldysgenesis) may be identified.
SKULL AND DURA
• The calvarial vault forms from membranous bone.
• With failure of neural tube closure and absence of fetal
brain distension, normal induction of the calvarial
membranous plates does not occur.
• Disorganized collections of collagen fibers and
deficient radial growth of the developing calvaria
ensue.
• The results a striking anomaly called lacunar skull
(i.e., Lückenschädel)
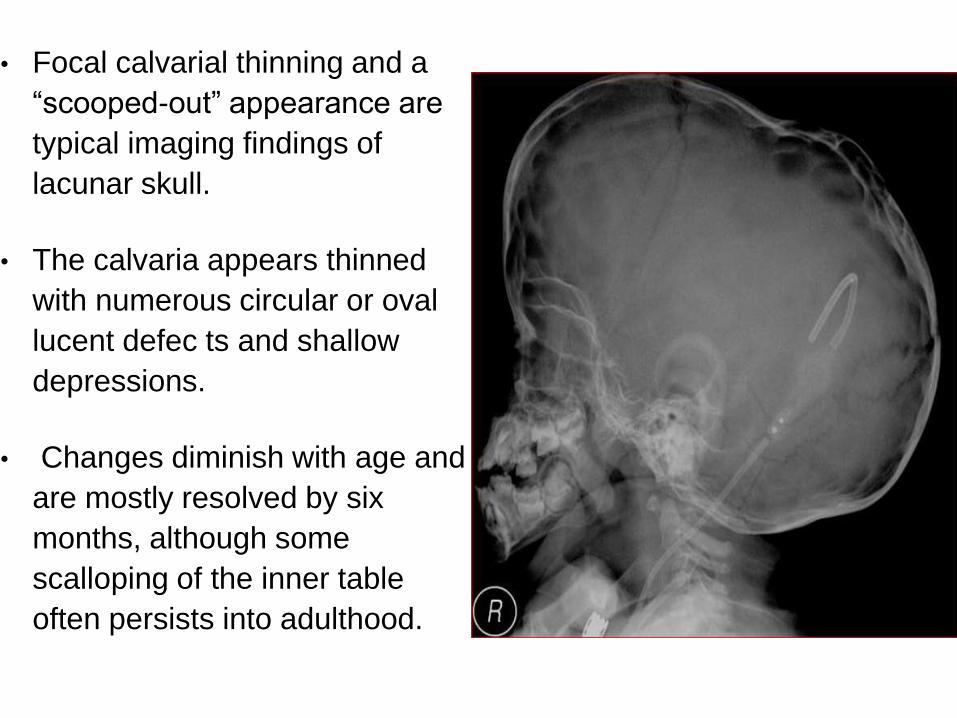
• Focal calvarial thinning and a
“scooped-out” appearance are
typical imaging findings of
lacunar skull.
• The calvaria appears thinned
with numerous circular or oval
lucent defec ts and shallow
depressions.
• Changes diminish with age and
are mostly resolved by six
months, although some
scalloping of the inner table
often persists into adulthood.
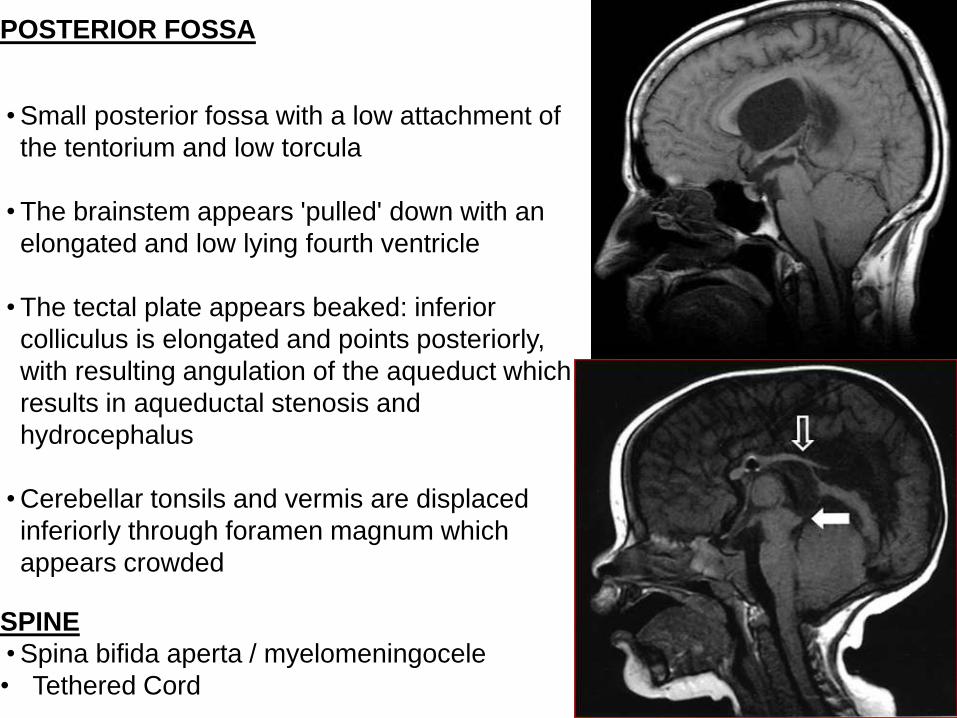
POSTERIOR FOSSA
•Small posterior fossa with a low attachment of
the tentorium and low torcula
•The brainstem appears 'pulled' down with an
elongated and low lying fourth ventricle
•The tectal plate appears beaked: inferior
colliculus is elongated and points posteriorly,
with resulting angulation of the aqueduct which
results in aqueductal stenosis and
hydrocephalus
•Cerebellar tonsils and vermis are displaced
inferiorly through foramen magnum which
appears crowded
SPINE
•Spina bifida aperta / myelomeningocele
• Tethered Cord
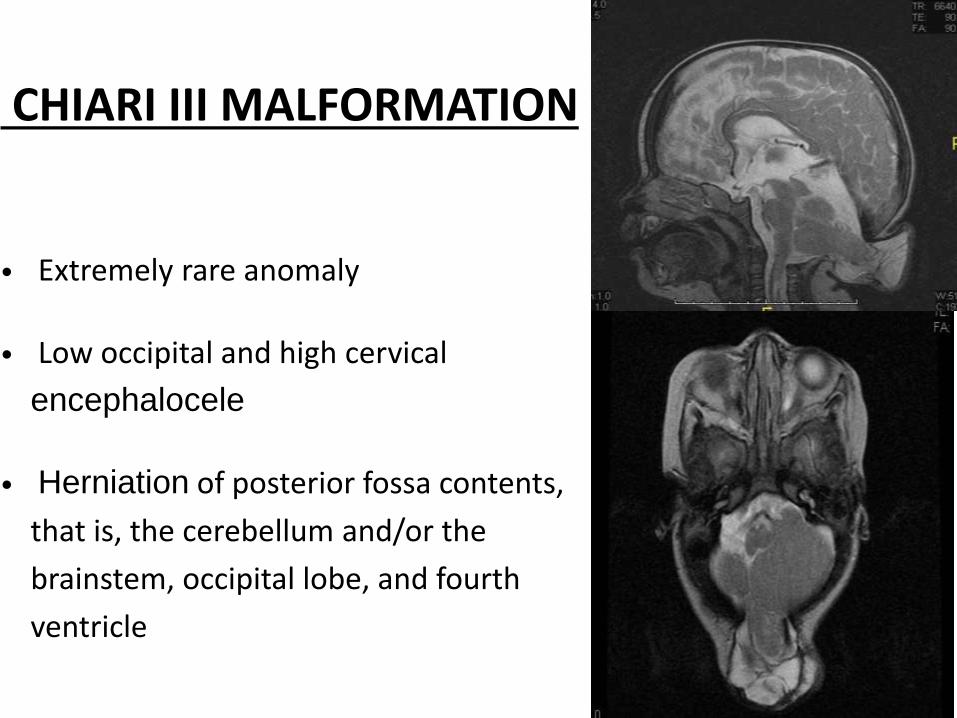
CHIARI III MALFORMATION
• Extremely rare anomaly
• Low occipital and high cervical
encephalocele
• Herniation of posterior fossa contents,
that is, the cerebellum and/or the
brainstem, occipital lobe, and fourth
ventricle
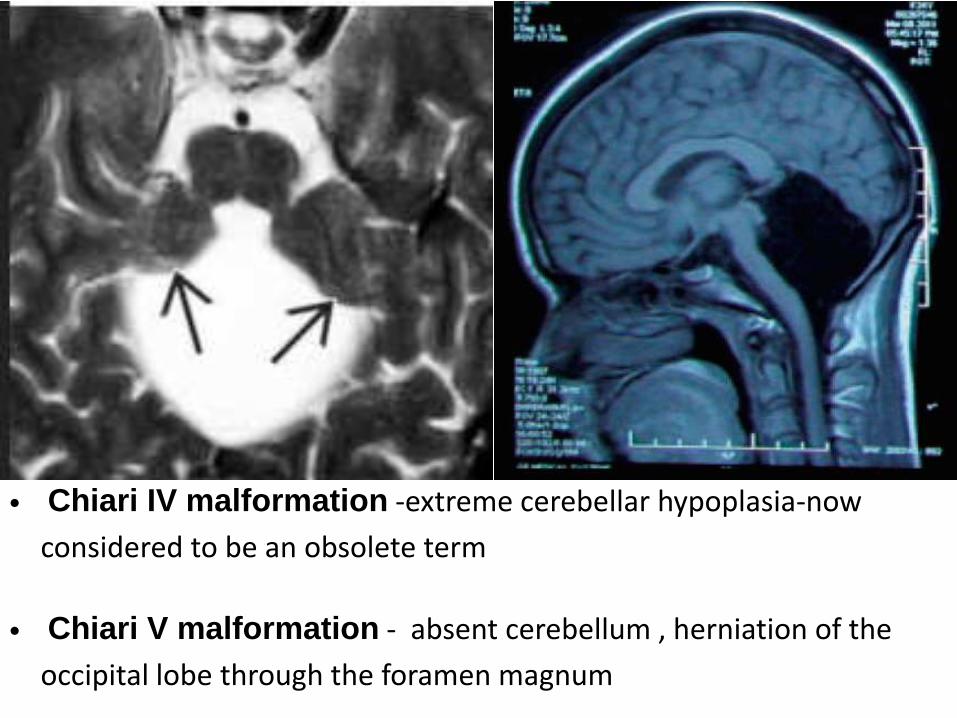
Variants
• Chiari IV malformation -extreme cerebellar hypoplasia-now
considered to be an obsolete term
• Chiari V malformation - absent cerebellum , herniation of the
occipital lobe through the foramen magnum
DANDY WALKER COMPLEX
• Malformation of posterior fossa
– Pathogenesis unknown but thought to be due to arrest of
development of hindbrain around 7-10 week gestation.
• Spectrum of disease that includes:
1. Dandy-Walker malformation
2. Dandy-Walker variant
3. Mega Cistern Magna
4. Posterior Fossa Arachnoid Cyst
• Occurs in1:30,000births
• Seen in 4-12% of all babies with hydrocephalus
DANDY WALKER MALFORMATION
TRIAD OF MALFORMATIONS
1. Cystic dilation of fourth ventricle
2. Complete or partial agenesis of the cerebellar vermis
3. Enlarged posterior fossa with displacement of the tentorium and
torcular and lateral sinus.
• Diagnosed after 18 weeks – closure of cerebellar vermis should happen
by that time
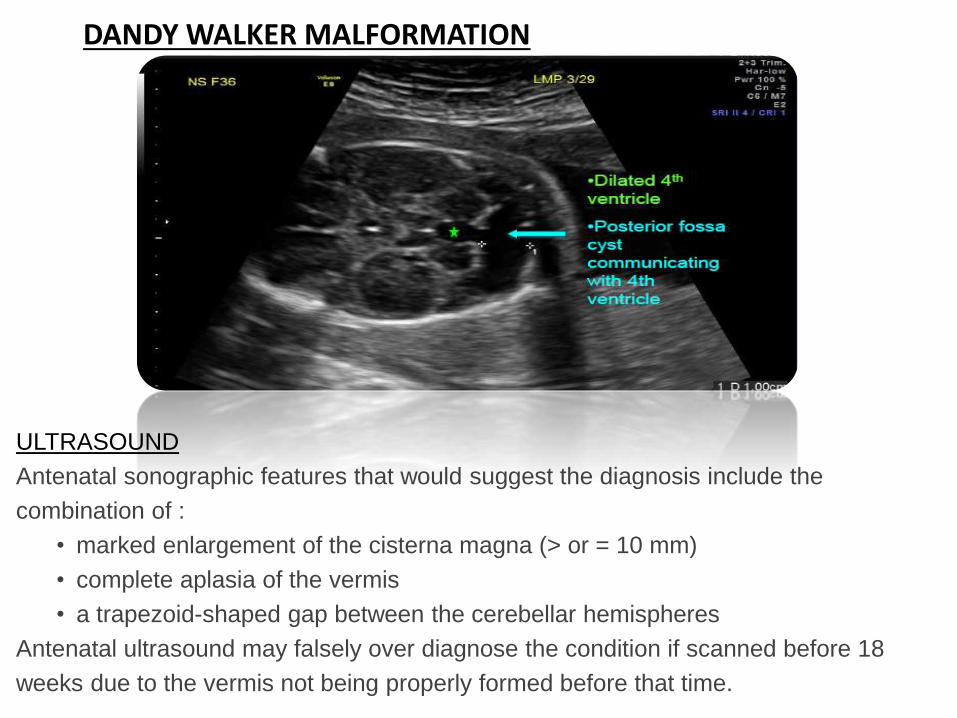
DANDY WALKER MALFORMATION
ULTRASOUND
Antenatal sonographic features that would suggest the diagnosis include the
combination of :
• marked enlargement of the cisterna magna (> or = 10 mm)
• complete aplasia of the vermis
• a trapezoid-shaped gap between the cerebellar hemispheres
Antenatal ultrasound may falsely over diagnose the condition if scanned before 18
weeks due to the vermis not being properly formed before that time.
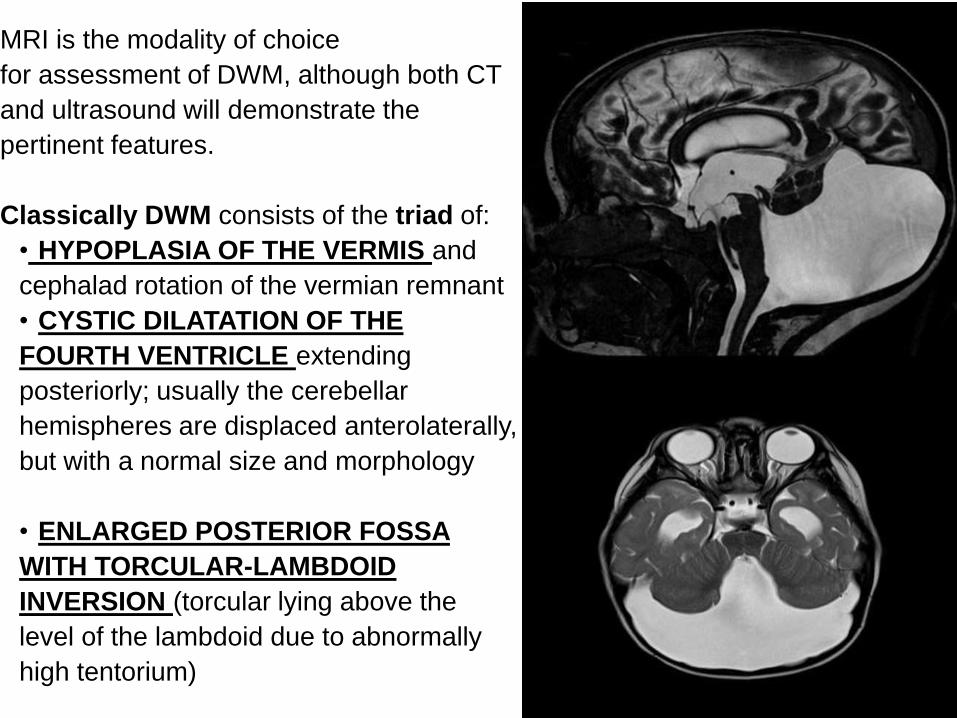
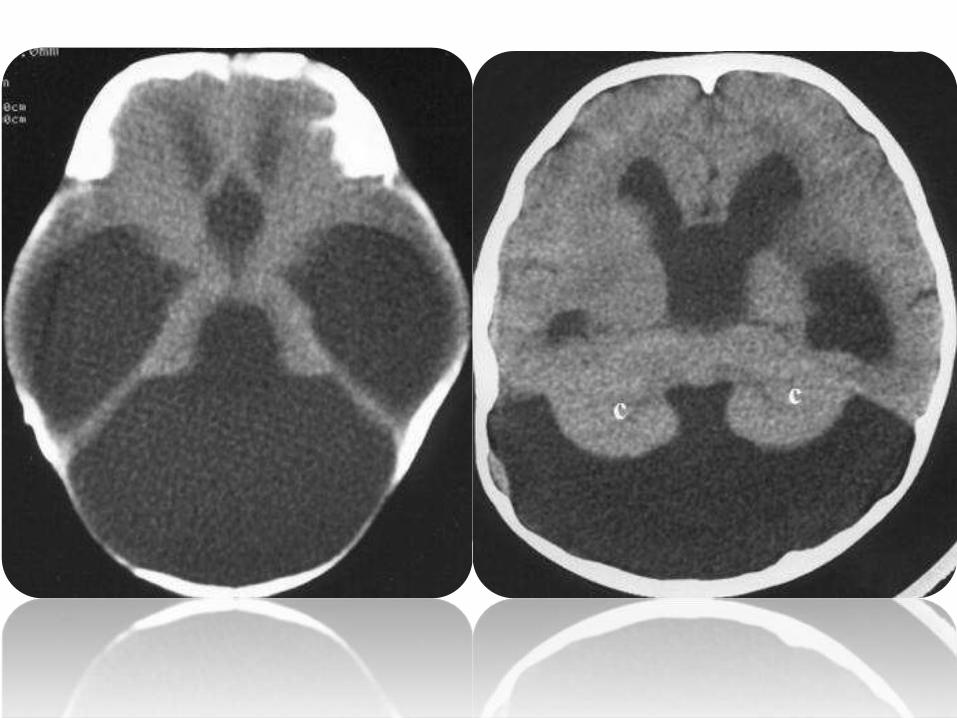
MRI is the modality of choice
for assessment of DWM, although both CT
and ultrasound will demonstrate the
pertinent features.
Classically DWM consists of the triad of:
• HYPOPLASIA OF THE VERMIS and
cephalad rotation of the vermian remnant
• CYSTIC DILATATION OF THE
FOURTH VENTRICLE extending
posteriorly; usually the cerebellar
hemispheres are displaced anterolaterally,
but with a normal size and morphology
• ENLARGED POSTERIOR FOSSA
WITH TORCULAR-LAMBDOID
INVERSION (torcular lying above the
level of the lambdoid due to abnormally
high tentorium)
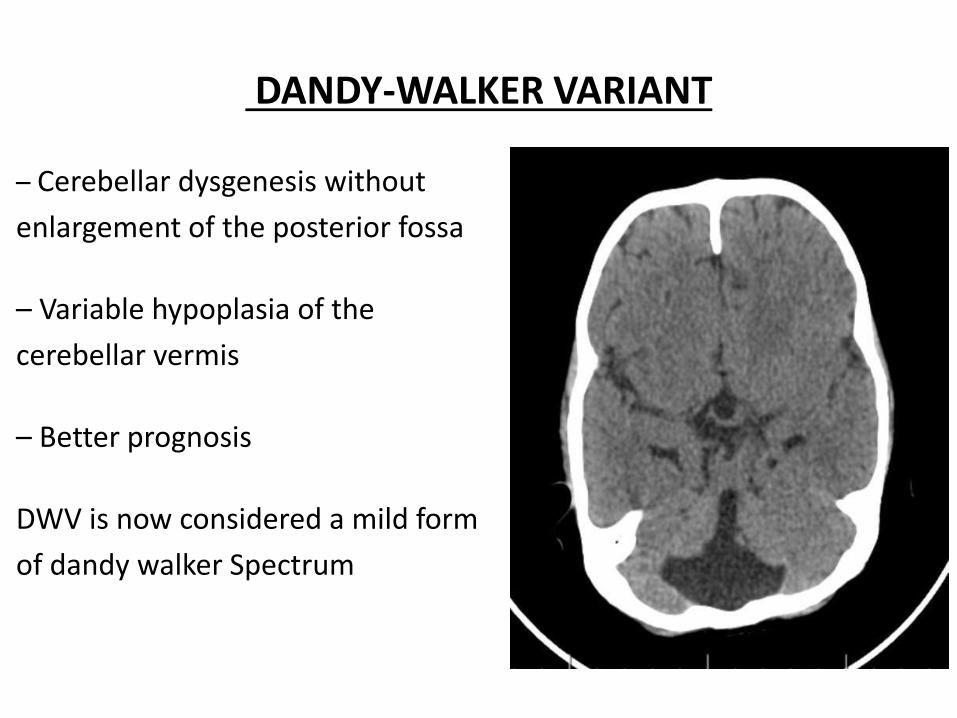
DANDY-WALKER VARIANT
– Cerebellar dysgenesis without
enlargement of the posterior fossa
– Variable hypoplasia of the
cerebellar vermis
– Better prognosis
DWV is now considered a mild form
of dandy walker Spectrum
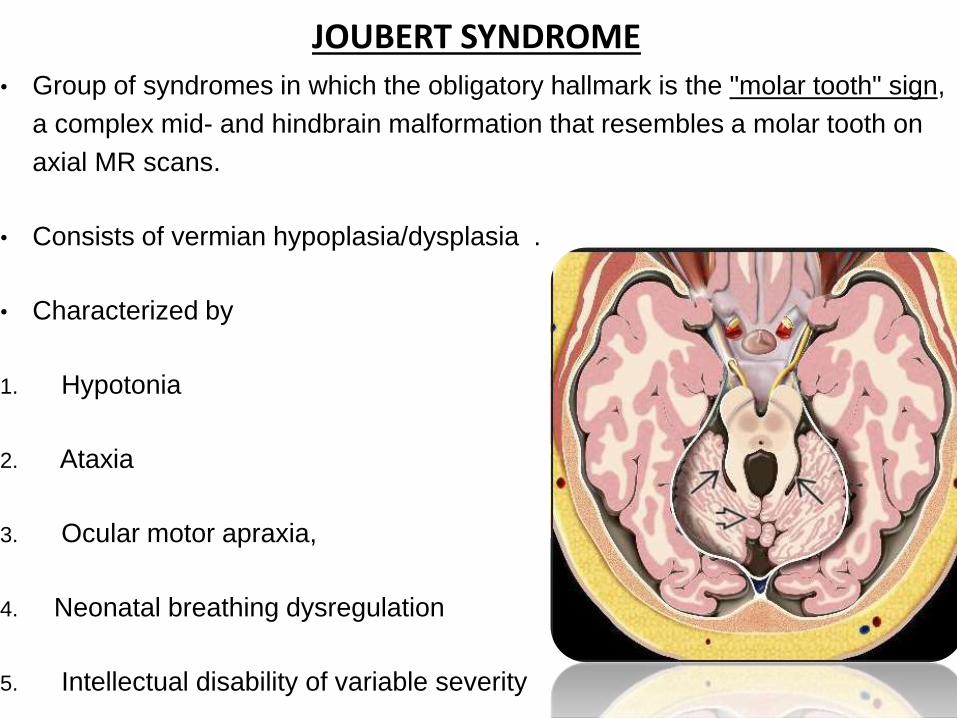
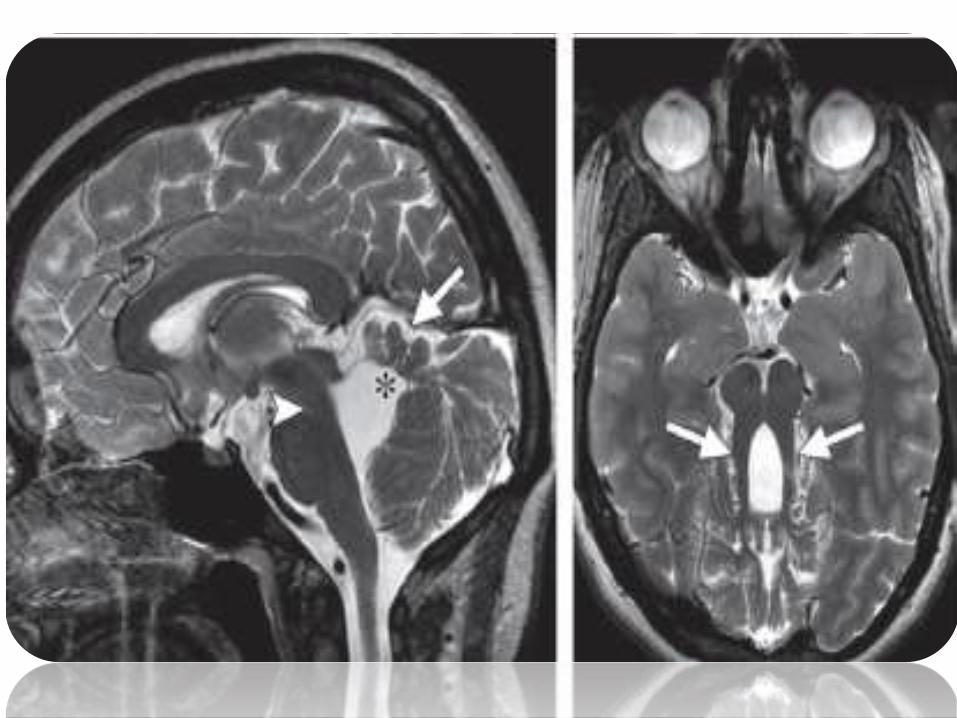
JOUBERT SYNDROME• Group of syndromes in which the obligatory hallmark is the "molar tooth" sign,
a complex mid- and hindbrain malformation that resembles a molar tooth on
axial MR scans.
• Consists of vermian hypoplasia/dysplasia .
• Characterized by
1. Hypotonia
2. Ataxia
3. Ocular motor apraxia,
4. Neonatal breathing dysregulation
5. Intellectual disability of variable severity
• Systemic involvement may be present and includes renal
(nephronophthisis), ocular (colobomas, retinal dystrophy),
hepatic (congenital hepatic fibrosis), and skeletal (various
forms of polydactyly) involvement
• Anomalies of the kidneys, eyes, extremities, liver, and bile
ducts are common in the JSRD spectrum.
POSTERIOR FOSSA ARACHNOID CYSTS
• Duplications of the arachnoid membrane produce fluid-filled cysts
known as arachnoid cysts.
• About 10% of arachnoid cysts in children occur in the posterior fossa
1. Macrocephaly
2. Signs of increased intracranial pressure
3. Developmental delay.
• However, these cysts may be asymptomatic and discovered incidentally
.Arachnoid cysts do not communicate with the fourth ventricle or the
subarachnoid space
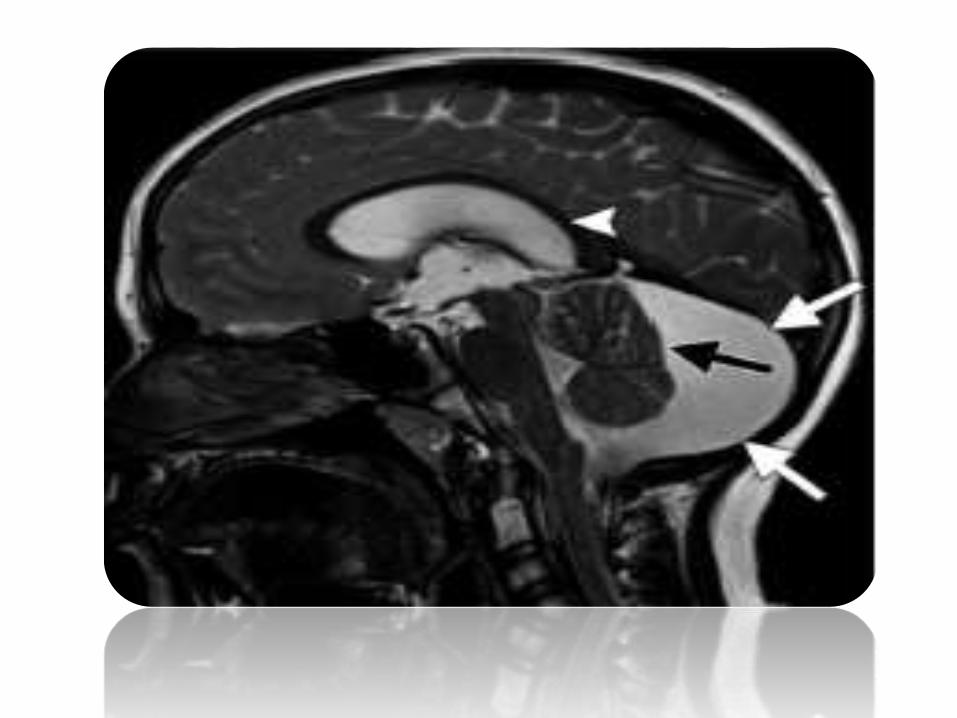
BLAKE POUCH CYST
• Caused by the lack of fenestration of the blake pouch
• Absence of communication between the fourth ventricle and the
subarachnoid space .
• The cerebellum has a normal size and shape.
• Blake pouch cyst occurs sporadically, and no recurrence risk has
been reported.
• Hydrocephalus and macrocephaly are the most common
presenting features in the neonatal period.
• In the absence of shunt-related complications, the prognosis is
generally favorable.

MEGA CISTERNA MAGNA
• Enlarged cisterna magna (-10 mm on midsagittal images) with
an intact vermis, a normal fourth ventricle, and, in some
patients, an enlarged posterior fossa
• Represents a truly focal enlargement of the subarachnoid
space in the inferior and posterior portions of the posterior
fossa.
• Mega cisterna magna freely communicates with the fourth
ventricle and the cervical subarachnoid space
• Results in consistent absence of hydrocephalus.
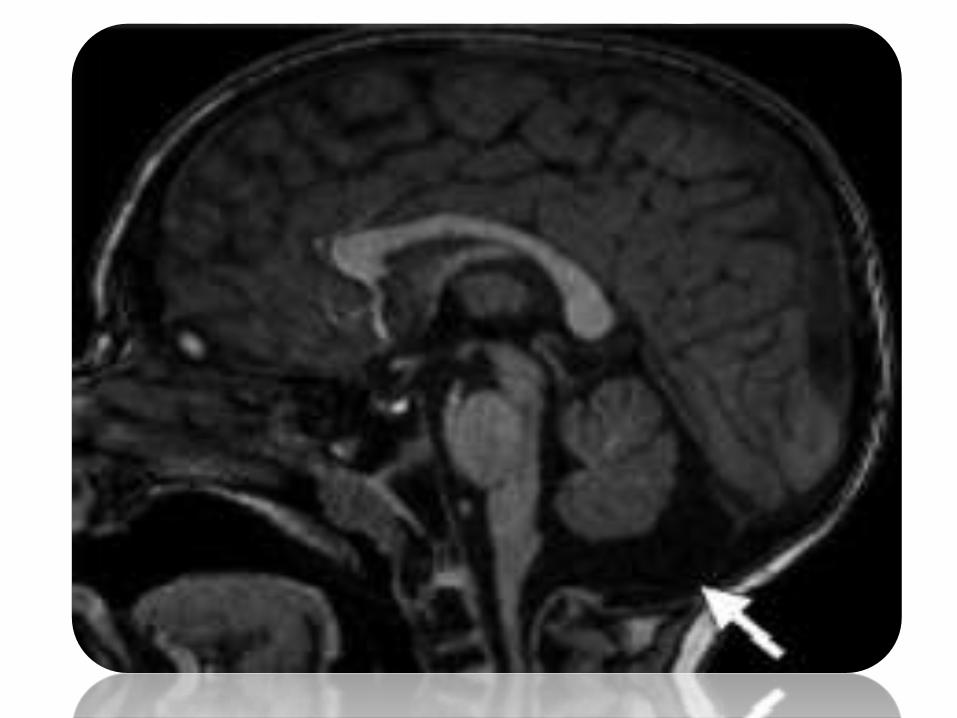
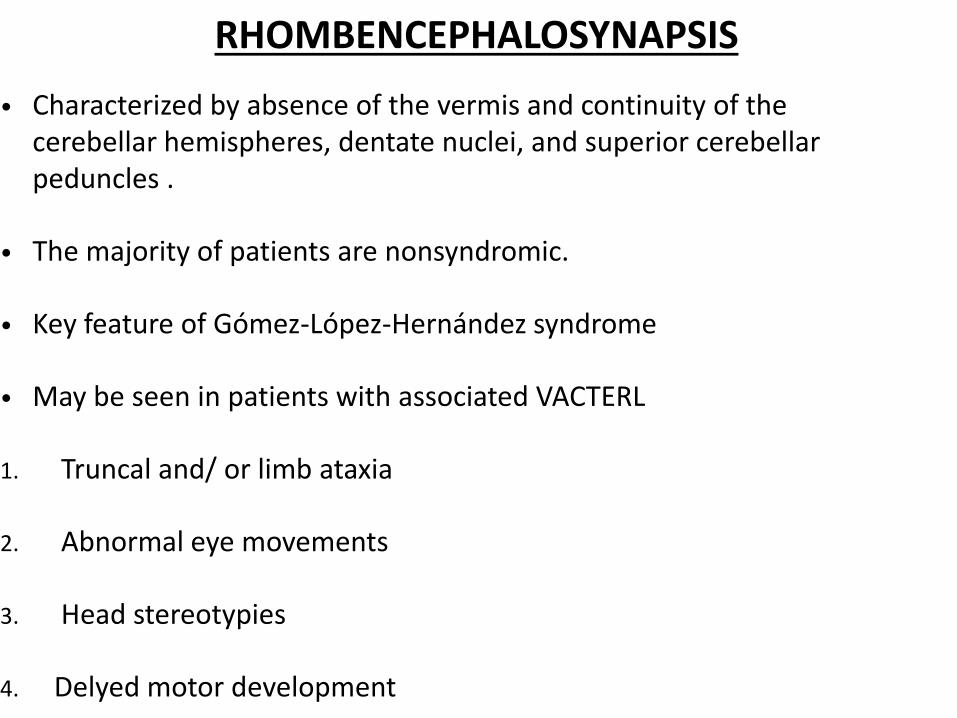
RHOMBENCEPHALOSYNAPSIS
• Characterized by absence of the vermis and continuity of the cerebellar hemispheres, dentate nuclei, and superior cerebellar peduncles .
• The majority of patients are nonsyndromic.
• Key feature of Gómez-López-Hernández syndrome
• May be seen in patients with associated VACTERL
1. Truncal and/ or limb ataxia
2. Abnormal eye movements
3. Head stereotypies
4. Delyed motor development
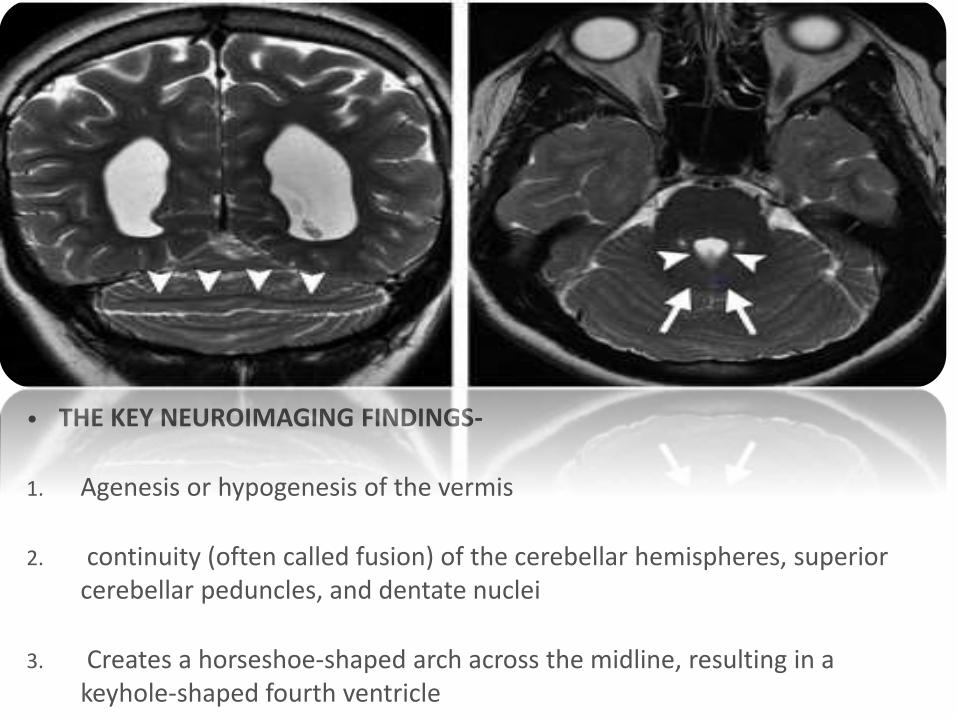
• THE KEY NEUROIMAGING FINDINGS-
1. Agenesis or hypogenesis of the vermis
2. continuity (often called fusion) of the cerebellar hemispheres, superior cerebellar peduncles, and dentate nuclei
3. Creates a horseshoe-shaped arch across the midline, resulting in a keyhole-shaped fourth ventricle