Embed Size (px)
Citation preview
Simulation, feedback and intensive coaching to improve BLS skills performance
Alan Batt
• Alan Batt
– Clinical Educator, National Ambulance LLC, UAE
– Associate Researcher, Centre for Prehospital Research, Graduate Entry Medical School, University of Limerick, Ireland
– Research Committee Member, National Association of EMS Educators
– Editor-in-chief, prehospitalresearch.eu
– No financial conflicts
Conflict of interest statement
Realistic?
• Inappropriate or inadequate skill performance at a particular time (Kohn, Corrigan & Donaldson 2000)
• Inappropriate or inadequate team performance and communication (AHRQ 2003)
• Human factor issues: conflict between humans and equipment (Reason 2000)
• Combination of the above
Inadequate performance

Meet “Steve”
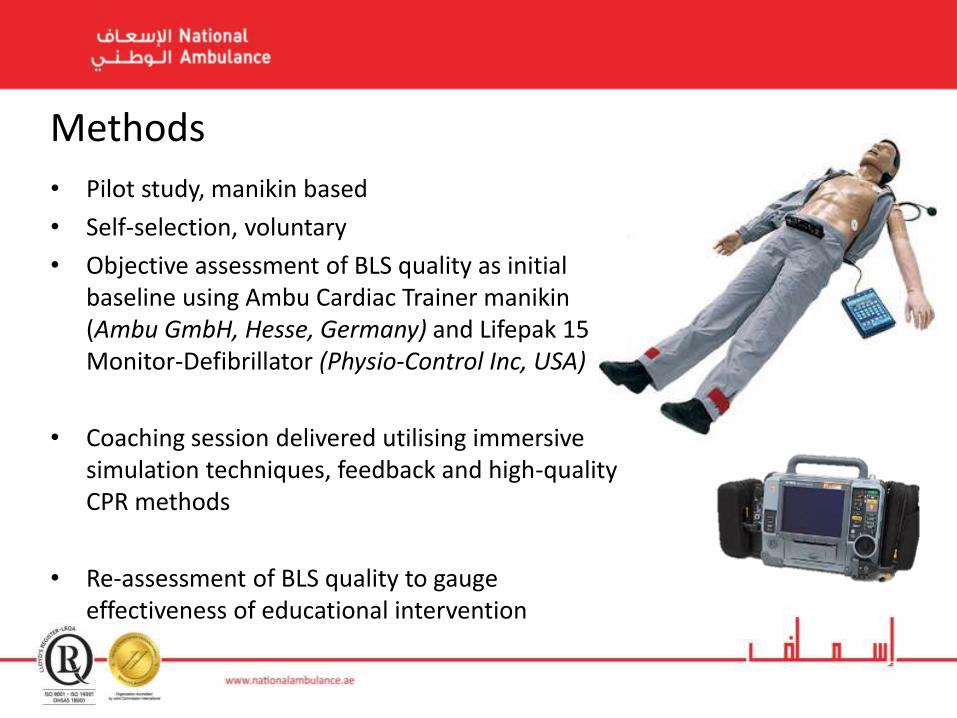
• Pilot study, manikin based
• Self-selection, voluntary
• Objective assessment of BLS quality as initial baseline using Ambu Cardiac Trainer manikin (Ambu GmbH, Hesse, Germany) and Lifepak 15 Monitor-Defibrillator (Physio-Control Inc, USA)
• Coaching session delivered utilising immersive simulation techniques, feedback and high-quality CPR methods
• Re-assessment of BLS quality to gauge effectiveness of educational intervention
Methods
• EMTs and Paramedics with previous BLS training and certification
• 8 teams of 2 providers (n=16)
• Mixed BLS and ALS providers
Population
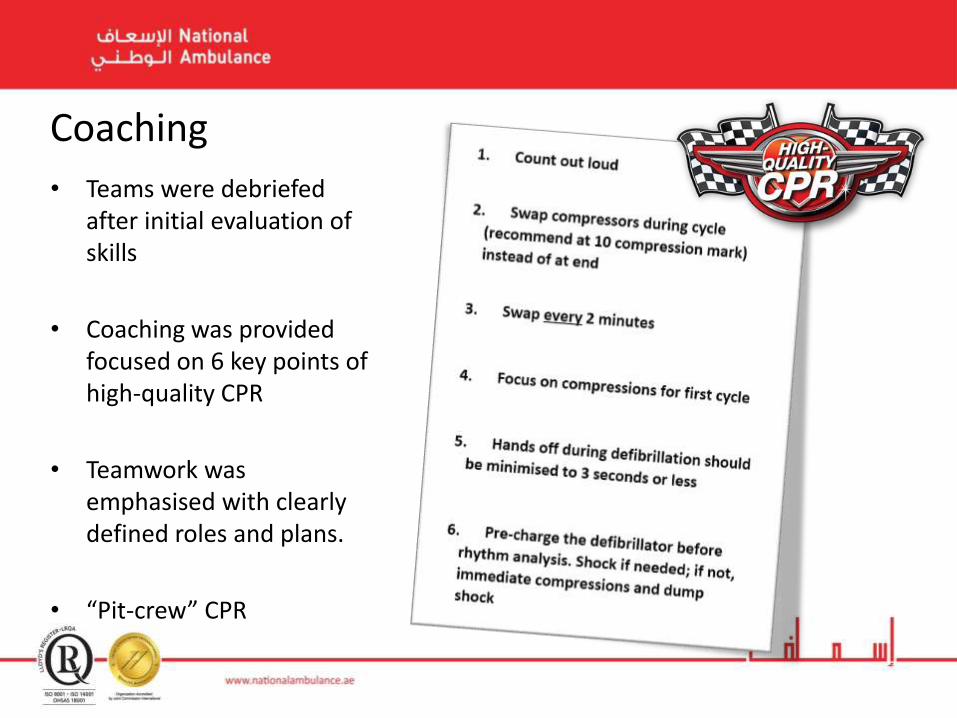
• Teams were debriefed after initial evaluation of skills
• Coaching was provided focused on 6 key points of high-quality CPR
• Teamwork was emphasised with clearly defined roles and plans.
• “Pit-crew” CPR
Coaching
• No skill sheet used, no time limit enforced
• Full body manikin used with ability to generate cardiac rhythms and palpable pulse
• Equipment used as per in-field equipment
• Manikin on ground in collapsed position
• No interaction from assessor
• Immersion in clinical environment has been shown to simulate stressful conditions encountered by personnel. LeBlanc et al. (2005) found a decrease in drug calculation performance during stress.
Immersion

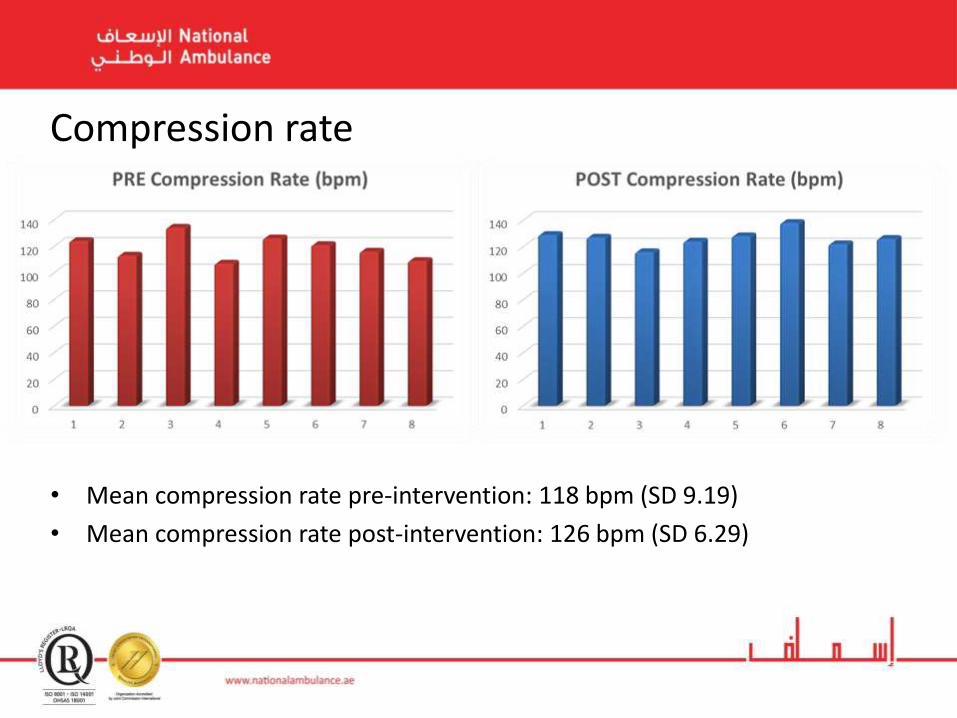
Compression rate
• Mean compression rate pre-intervention: 118 bpm (SD 9.19)
• Mean compression rate post-intervention: 126 bpm (SD 6.29)
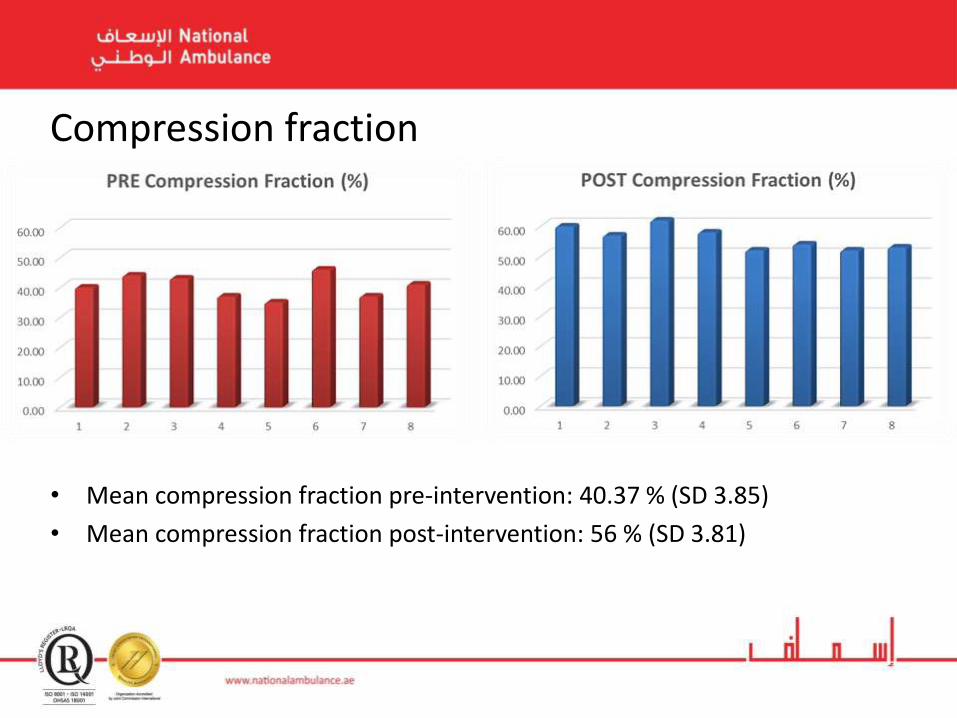
• Mean compression fraction pre-intervention: 40.37 % (SD 3.85)
• Mean compression fraction post-intervention: 56 % (SD 3.81)
Compression fraction
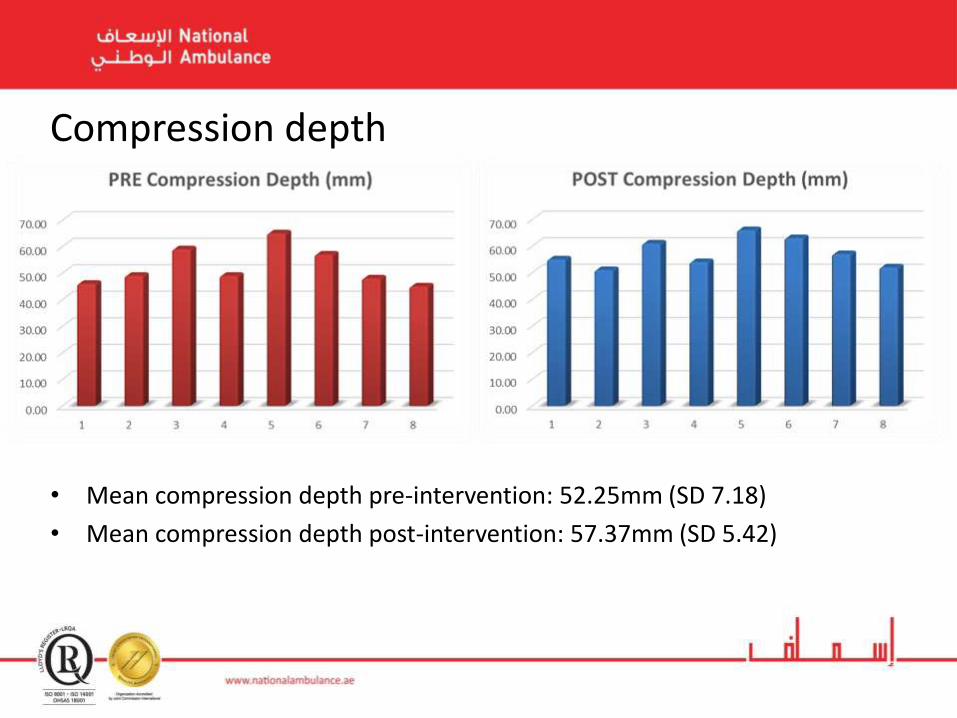
• Mean compression depth pre-intervention: 52.25mm (SD 7.18)
• Mean compression depth post-intervention: 57.37mm (SD 5.42)
Compression depth
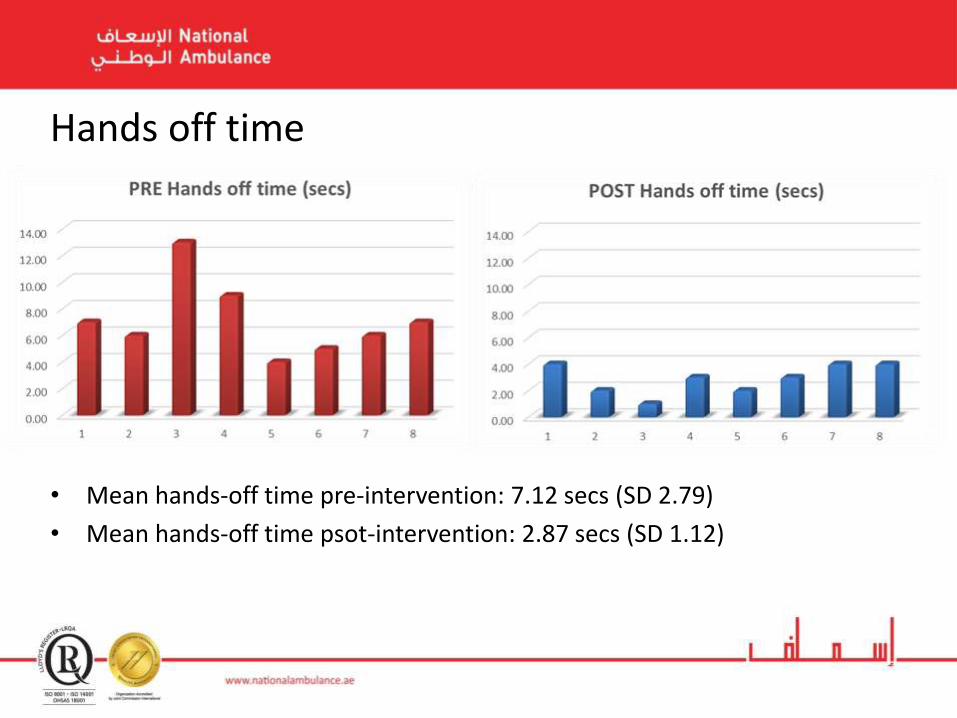
• Mean hands-off time pre-intervention: 7.12 secs (SD 2.79)
• Mean hands-off time psot-intervention: 2.87 secs (SD 1.12)
Hands off time
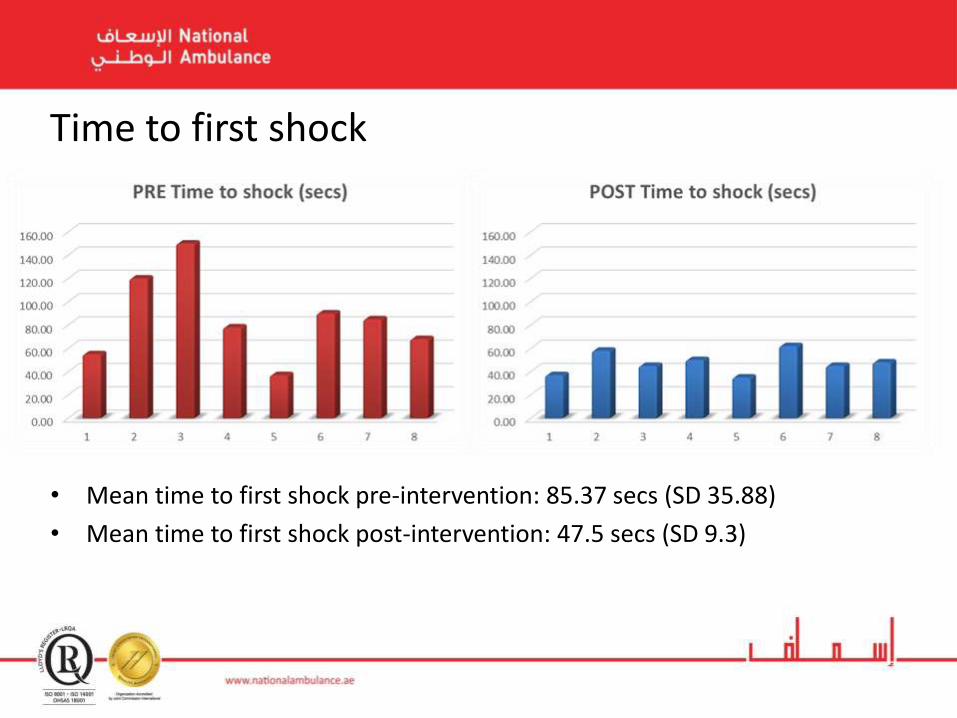
• Mean time to first shock pre-intervention: 85.37 secs (SD 35.88)
• Mean time to first shock post-intervention: 47.5 secs (SD 9.3)
Time to first shock
• A combination of immersive simulation, intensive coaching and feedback resulted in:
• Higher compression rate
• Deeper compressions
• Less hands-off time
• Higher compression fraction
• Decreased time to first shock
• These are all components of high quality CPR described by ILCOR and the American Heart Association.
Results
• Non-randomised
• Non-blinded due to nature of intervention
• Significant potential for Hawthorne effect
• All providers had previous experience of BLS
Limitations
Bottom Line
• Training matters!
• Simulation makes it better!
• Immediate feedback and focused intensive coaching improves performance.
• Our pilot study indicates that high-quality CPR training can be implemented through immersive team-based simulation, coaching and feedback.
• Agency for Healthcare Research and Quality. (2003). AHRQ’s patient safety initiative: Building foundations, reducing risk. Interim Report to the Senate Committee on Appropriations. AHRQ Publication No. 04-RG005, December 2003. Retrieved January 5, 2015, from http://www.ahrq.gov/qual/pscongrpt/
• Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (2000). To err is human: Building a safer health system. Free Executive Summary. Washington, DC: National Academies Press.
• LeBlanc, V. R., MacDonald, R. D., McArthur, B., King, K., & Lepine, T. (2005) Paramedic performance in calculating drug dosages following stressful scenarios in a human patient simulator. Prehospital Emergency Care : Official Journal of the National Association of EMS Physicians and the National Association of State EMS Directors, 9(4), 439–44.
• Reason, J. (2000). Human error: Models and management. BMJ, 320, 768-770.
• Yu, T. (2002). Adverse Outcomes of Interrupted Precordial Compression During Automated Defibrillation. Circulation, 106(3), 368–372. doi:10.1161/01.CIR.0000021429.22005.2E
References





![BLS Magnet Innovative magnetic materials & solutions · BLS Magnet [8] Attractive technology BLS Magnet [9] Attractive technology BLS Magnet’s magnetic accessories are used in many](https://img.pdfslide.net/doc/110x75/5fe1e8025c38ec6ec573533b/bls-magnet-innovative-magnetic-materials-bls-magnet-8-attractive-technology.jpg)























