Embed Size (px)
Citation preview
Webinar: Turning Around Your Slow Enrolling Trial
Dan McDonald, BS DAC Patient Recruitment Services
1
Scott Treiber, PhD, MBA Theorem Clinical Research
August 11, 2015
Question & Answer
• We will be using the chat feature for question and answer.
• During the presentation, please type in your question in the chat box at that bottom of the control panel on the left side of your screen.
• At the conclusion of the presentation, Scott and Dan will answer your questions.
2
3
Speaker Introductions
4
Speaker Introduction
5
Setting the Stage
The Facts
6
On time enrollment of clinical trials is costing the industry hundreds of millions of dollars
• in direct fixed costs and • opportunity costs
The numbers are startling • Although 9 out of 10 studies achieve enrollment goals, it
can take up to double the original time to get there* • 11% of sites in a given trial typically fail to enroll a single
patient • 37% under-enroll • 39% meet their enrollment targets • 13% exceed their targets
• 95% of all trial delays are due to slow patient recruitment *Tu*s Center for the Study of Drug Development – Jan 15, 2013
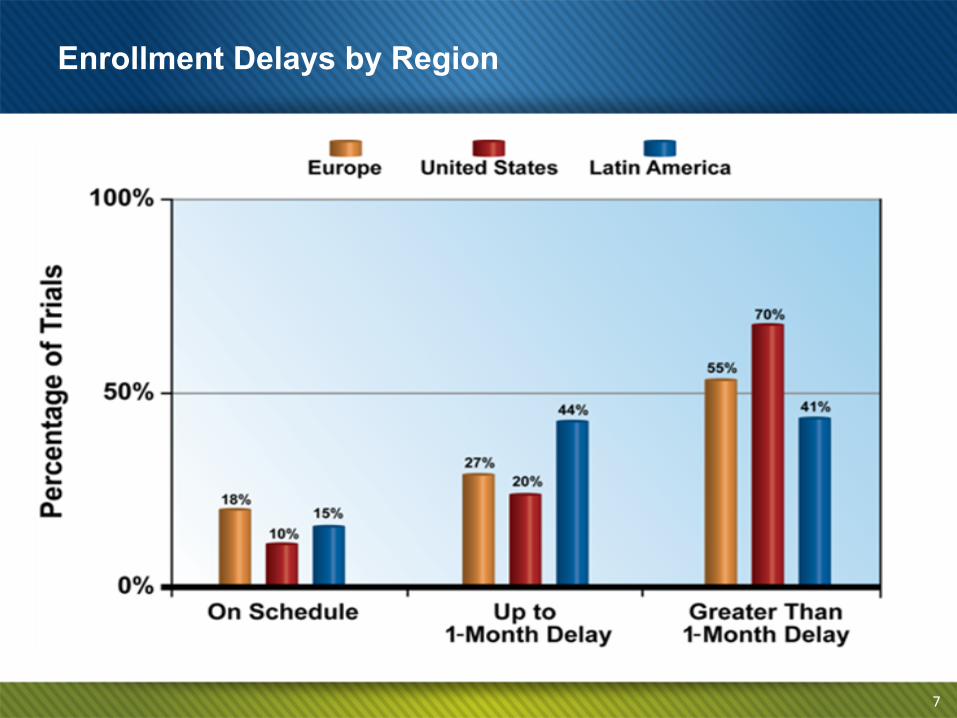
Enrollment Delays by Region
7
The Evolution of Patient Recruitment
8
1990s • Patient recruitment for special populations • Mainly advertising – radio, TV, newspaper
2000s • Data mining techniques • Links to scripts/pharmacy data
2010s • Social media • Targeted training • Patient advocacy groups
Reasons for Enrollment Challenges
Protocol Criteria
Iden/fying Pa/ents
Screen Failures
Consent
Compe/ng Studies
Site Fa/gue
Fairness of Grant
Proactive vs. Reactive
10
Proactive patient recruitment • Becoming the norm • Not just for special populations, rare/orphan diseases • Can save money
Reactive – what is the best way to rescue a slow enrolling trial
• Use a vendor that has an established track record • Understand their strengths and ensure fit • Don’t wait too long to ask for help
11
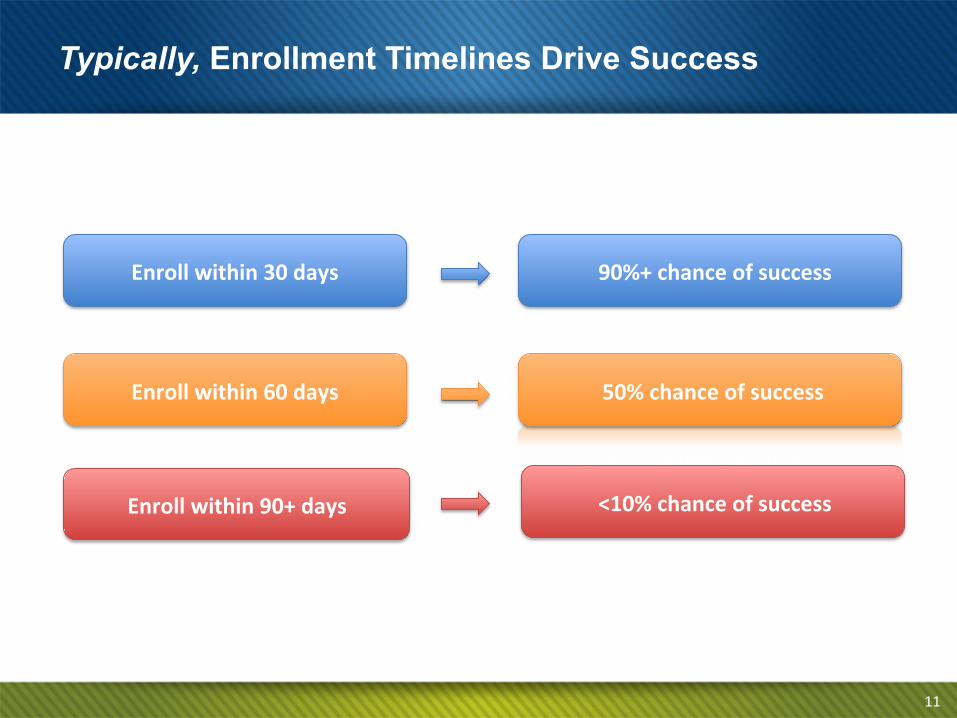
Enroll within 90+ days <10% chance of success
Enroll within 60 days 50% chance of success
Enroll within 30 days 90%+ chance of success
Typically, Enrollment Timelines Drive Success

Problem Acceptance and
Solution Planning
12
Don’t Panic! Take a Deep Breath and Plan
13
Understanding Your Situation: § How many patients left to enroll?
§ How much time left to enroll if not at deadline?
§ What is your average enrollment rate PSPM?
§ What is your recent enrollment rate (e.g. last 3 months)
§ When will enrollment complete at your current rate?
§ Who are your top enrolling sites?
§ Create your pie: (25% poor; 25% fair; 25% better; 25% best)
§ What is the enrollment rate at your top sites?
§ Consider support of only your top 50% enrollers in your turn-around plan!
Diagnose and Design Your Plan
Diagnosing Your Challenges: § Ask your Sites
§ Ask your Monitors
§ Ask your Project Managers
§ Chart and Compare Responses
§ Consider the Common Causes for Delay
Diagnose and Design Your Plan
Protocol Criteria
Iden/fying Pa/ents
Screen Failures
Consent
Compe/ng Studies
Site Fa/gue
Fairness of Grant
Choosing Solutions for
Optimal Results
16
Solutions: Add More Sites
Initiative: Identification, selection and contacting of new study sites to supplement enrollment for low enrolling sites.
Pros:
§ Fresh pool of patients
§ New sites are typically more enthusiastic
§ Benchmark enrollment data to compare sites against
§ Appropriate for most study types
Cons:
§ Time consuming – Site contracts are #1 trial delay factor
§ Costly (Site Grants; Monitoring; CRO Mgmt. Fees; etc.)
§ May not solve root problems of slow enrollment
§ You may end up in the same situation in a few months
§ Regulatory approval required sites in some countries
Consider leveraging
insurance claims data and EMRs for validation of
patient volume at the site.
18
Solutions: Determining Site Challenges and Needs
Offer $5 Starbucks gift
cards to CRCs that participate
in survey and ongoing
committees
Initiative: Web-based survey of sites to determine challenges and support needs. Conduct of other ongoing forums to maintain momentum: Face-to-face meetings or Web conferences; Advisory committee
Pros: § Quick and easy to implement § Low Cost § Recognizes sites as a critical stakeholder § Reveals obstacles that only sites may see § Captures best practices § Drives adoption rates for recruitment initiatives § Engaging CRCs has a proven impact on enrollment
Cons: § Adds more “work” for sites § May establish false expectations § Can turn into a complaint session if not managed
Initiative: One-hour training session providing study-relevant, hard-hitting tips, tools and resources that sites can immediately take and use in their recruitment efforts Pros: § Demonstrates sponsors interest in sites success
§ Introduces new skills and best practices
§ Relatively low cost
§ Quick and easy to implement, especially via Web
§ Provides simple yet effective approaches to improve enrollment
Cons:
§ Requires time most CRCs don’t have
§ Content development time
§ Not a stand-alone solution
19
Solutions: Training – Simple Logic, Big Results
Use an accredited
training service provider and
offer CCRCs CEU credits to drive
interest and participation
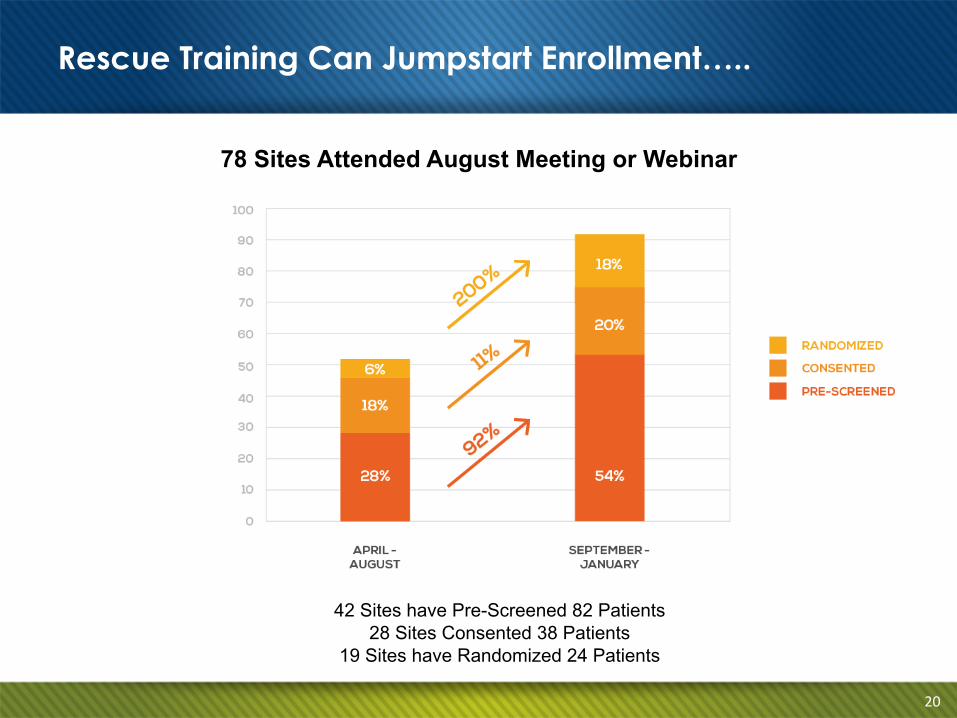
Rescue Training Can Jumpstart Enrollment…..
78 Sites Attended August Meeting or Webinar
42 Sites have Pre-Screened 82 Patients
28 Sites Consented 38 Patients 19 Sites have Randomized 24 Patients
20
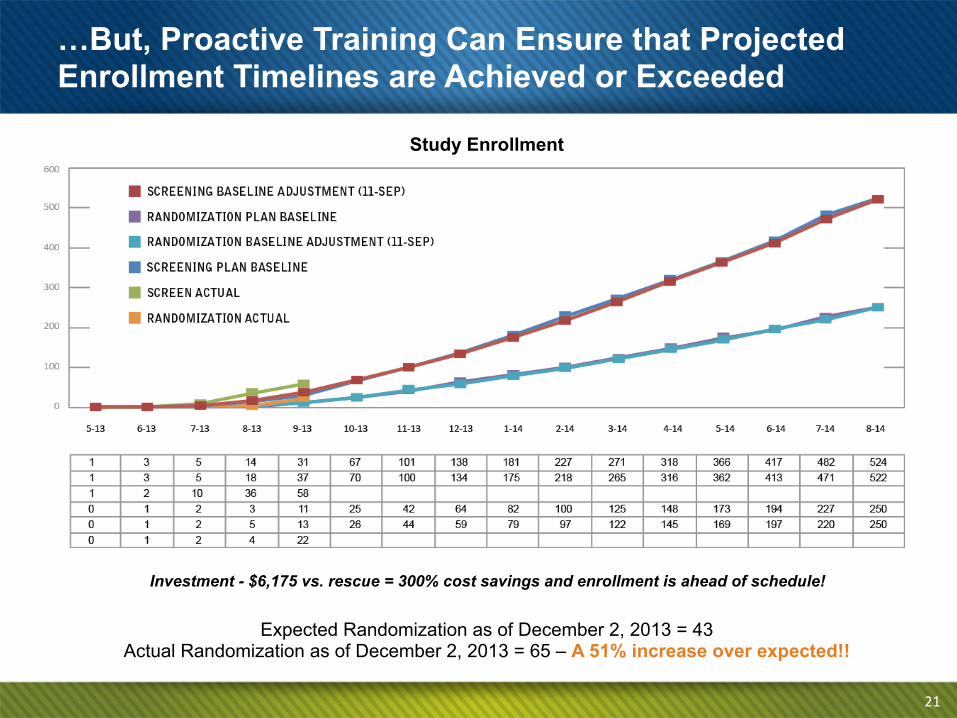
Expected Randomization as of December 2, 2013 = 43 Actual Randomization as of December 2, 2013 = 65 – A 51% increase over expected!!
Investment - $6,175 vs. rescue = 300% cost savings and enrollment is ahead of schedule!
21
Study Enrollment
…But, Proactive Training Can Ensure that Projected Enrollment Timelines are Achieved or Exceeded
Initiative: Leveraging television/radio/print to raise awareness about a study and generate referrals
Pros: § Once initiated, reaches large audience quickly
§ Geo-targeted around study sites
§ Leverages demographics and market data
§ Most-appropriate for broader-based conditions
§ Fairly easy to track performance
Cons:
§ Long ramp up time / Requires IRB approvals
§ High cost initiative
§ Response could be overwhelming to sites
§ May require hiring of a call center / additional cost
§ May not be appropriate for lower prevalence conditions / Studies requiring confirmed diagnosis
22
Solutions: Direct-to-Patient Broadcast/Print Advertising
Initiative: Using one or many digital channels to reach patients directly, for the purpose of raising awareness and encouraging self-referral to a study site
Pros: § Highly-targeted (Geo-targeting, Interest-targeting, etc.)
§ Multi-directional / User-driven
§ Localized campaigns are relatively easy to implement
§ Pay-for-performance pricing
§ Allows for pre-qualification of potential study subjects
§ Once initiated, can generate results quickly § Terrific metrics for performance tracking
Cons:
§ Long ramp up time / Requires IRB approvals
§ Costly when broad-based approach is required
§ Response could be overwhelming to sites
§ Less-appropriate for certain demographics
23
Solutions: Direct-to-Patient Digital Marketing
Share site-specific metrics with each site. Follow-up with
sites on any pre-qualified referrals
to improve response rates
Initiative: Includes outbound communication, education and awareness building about the study in the medical community around each study site.
Pros: § Short implementation timeline § Does not require IRB approval
§ Physician referred patients more likely to qualify
§ Ideal for conditions requiring confirmed diagnosis
§ Raises profile of sponsor in broader medical community
§ Geo-targeted
Cons:
§ Some physicians unwilling to refer / Fear losing patient
§ Requires follow-up effort to optimize effectiveness
§ Some lead time required for generation of materials
§ CRC/PI time required for list development
24
Solutions: Medical Community Outreach
Use insurance claims data to
determine which physicians in the
surrounding community are truly seeing the target patient
25
Understanding Cost Factors
§ Establish budget parameters for enrollment completion § Recruitment cost per patient: $1,500–$10,000+ (depending on
factors) § Consider allocating 5% of site per patient grants for retention.
§ 90% of sites have no formal plan/funds to address retention. § Increase allocation based on TA or long-term safety study.
§ Common Contingencies for Slow Enrollment § Hire new CRO § Addition of sites – avg. $20–$30K/site in the U.S. § Protocol amendments – avg. $1M/protocol § Extend timeline – avg.
§ Out of Pocket Costs: $100-150K (day) § Opportunity Costs: $1M (day)
§ Effective contingency planning requires proper support.
Understanding Cost Factors
26
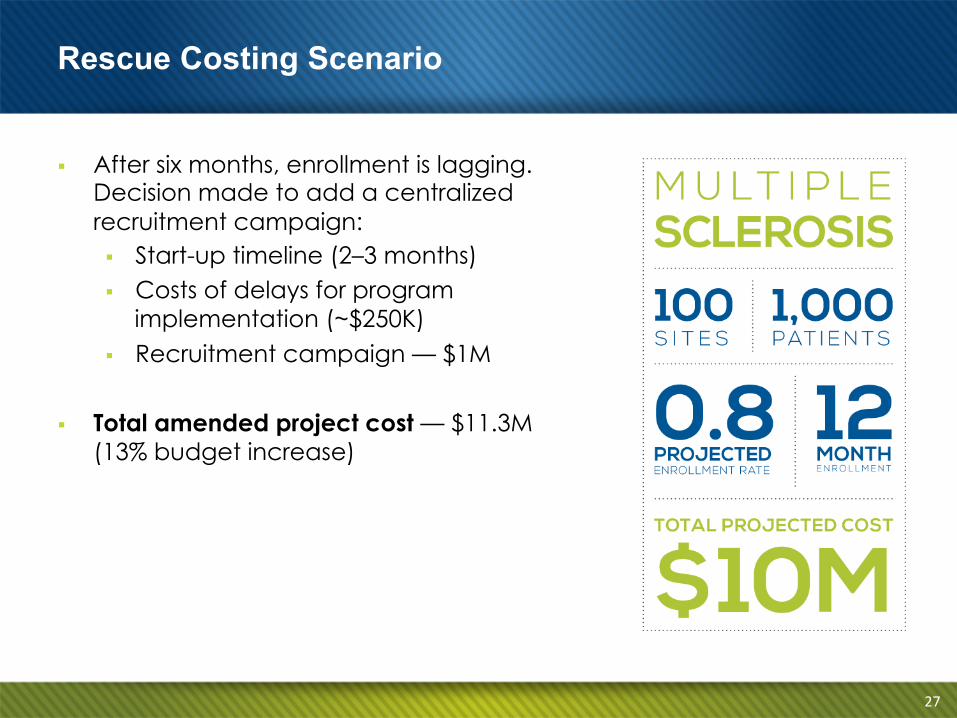
§ After six months, enrollment is lagging. Decision made to add a centralized recruitment campaign: § Start-up timeline (2–3 months) § Costs of delays for program
implementation (~$250K) § Recruitment campaign — $1M
§ Total amended project cost — $11.3M
(13% budget increase)
Rescue Costing Scenario
27
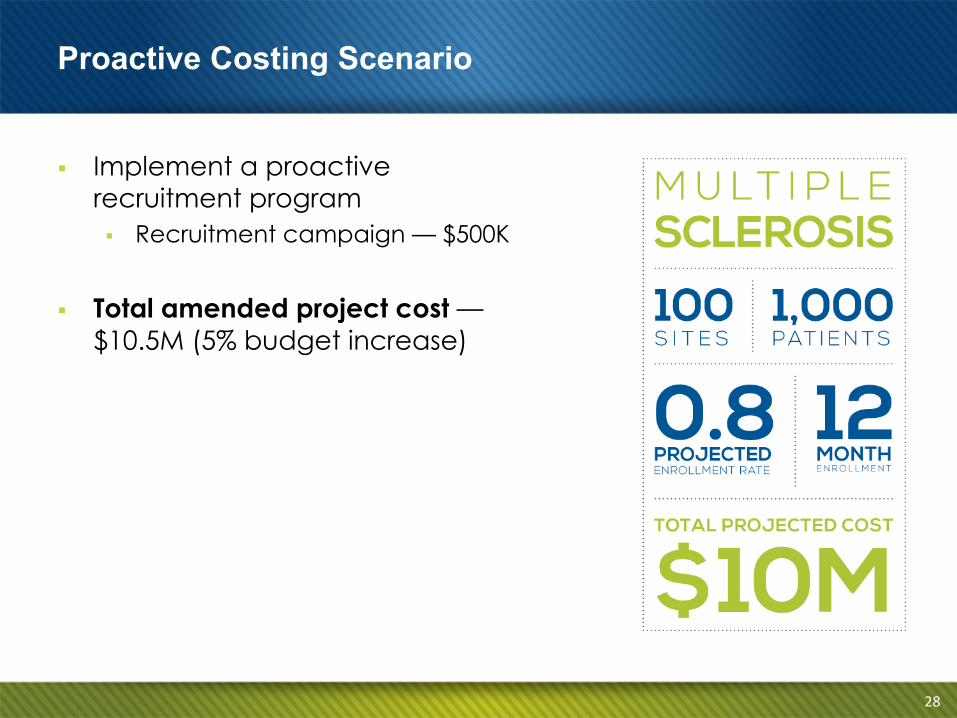
§ Implement a proactive recruitment program § Recruitment campaign — $500K
§ Total amended project cost — $10.5M (5% budget increase)
Proactive Costing Scenario
28
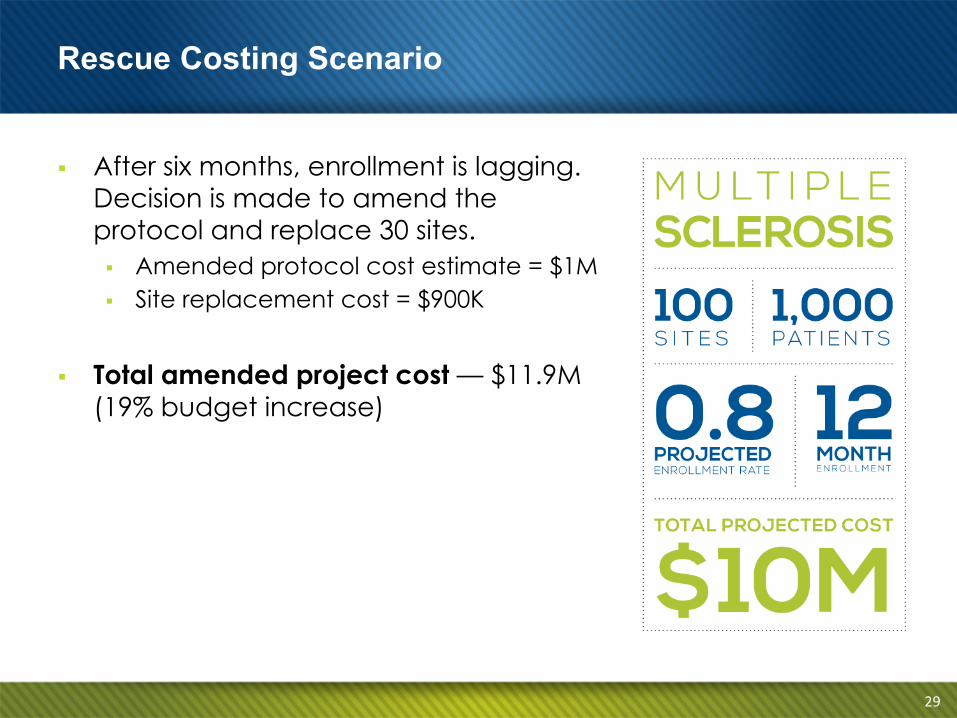
§ After six months, enrollment is lagging. Decision is made to amend the protocol and replace 30 sites. § Amended protocol cost estimate = $1M § Site replacement cost = $900K
§ Total amended project cost — $11.9M (19% budget increase)
Rescue Costing Scenario
29
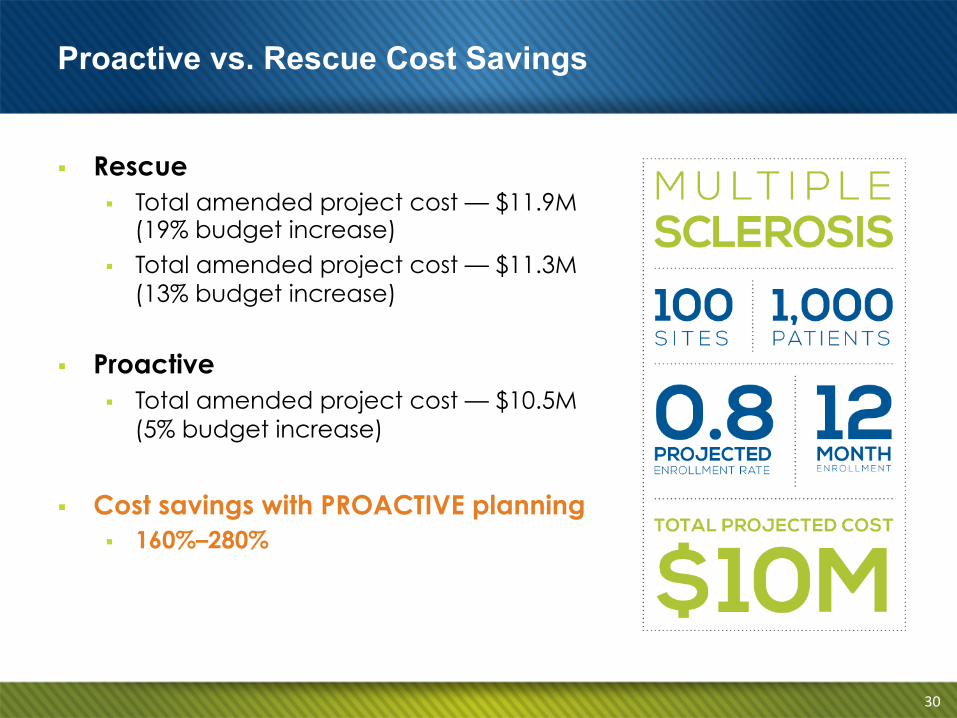
§ Rescue § Total amended project cost — $11.9M
(19% budget increase) § Total amended project cost — $11.3M
(13% budget increase)
§ Proactive § Total amended project cost — $10.5M
(5% budget increase)
§ Cost savings with PROACTIVE planning § 160%–280%
Proactive vs. Rescue Cost Savings
30
Dan McDonald Business Development
DAC Patient Recruitment Services 617-840-5405
31
Scott Treiber, PhD, MBA EVP & GM, Biopharma Development
Theorem Clinical Research 847-964-9611





























