Embed Size (px)
Citation preview
WHO 2016 update of lymphoid
neoplasms
Medical Director,Hematopathology and Molecular Pathology Program Director,International Hematopathology/Molecular Pathology Fellowship,Florida HospitalProfessor of Pathology,University of Central Florida, College of Medicine
E-mail: [email protected]
Phone: 407-303-1879

• Updated diagnostic categories and criteria to
current entities (some with new names) and a
limited number of new provisional entities
• Expanding the genetic/molecular landscape
and the biologic and clinical correlates
• Development of targeted therapeutic
strategies

Monoclonal B-cell lymphocytosis
(MBL)
• Up to 12% healthy individuals (DO NOT
ORDER FLOW CYTOMETRY FOR FUN)
• Must distinguish low count (< 0.5 x109/l),
extremely limited chance of progression, no
follow-up needed, from high count (> 0.5
x109/l) MBL, need yearly follow-up (annual
progression rate: 1 to 2%).
• Non-CLL type MBL: related to splenic MZL
• A lymph node equivalent of MBL exists:
preserved nodal architecture, with cells of
MBL phenotype, <1.5 cm, no proliferation
center (be careful with FNA specimen)

CLL/SLL
• Cytopenias or disease-related symptoms are now
insufficient to make a diagnosis of CLL with < 5
x109/l PB CLL cells.
• Large/confluent (broader than a 20x field) and/or
highly proliferative proliferation centers (PC) (either
>2.4 mitoses or Ki-67 >40%/PC) are adverse
prognostic indicators.
• PC may express weak cyclin D1, increase MYC
protein expression
• Mutations of TP53, NOTCH1, SF3B1, ATM, and
BIRC3: adverse prognostic factors, targeted therapy
(del TP53 for Ibrutinib).

Follicular lymphoma (FL)
• Mutational landscape better understood but
clinical impact remains to be determined
• Mutations in chromatin regulator/modifier
genes [CREBBP, KMT2D (MLL2)] and
EZH2: early event and potential treatment
targets

In situ follicular neoplasia
• New name for in situ follicular lymphoma (FL)
reflecting low risk of progression to lymphoma
• May associated with prior or synchronous overt
lymphoma, requiring clinical assessment
• Strong BCL2 expression, CD10+/BCL6+ cells
predominantly restricted inside follicle (no
spilling out)
• Flow cytometry showing clonal B-cells with FL
phenotype: be careful with FNA specimen
• Must be distinguished from partial involvement
by FL

Pediatric-type FL
• A localized (most stage 1) clonal proliferation with
excellent prognosis; excision alone may be sufficient
• Occurs in children and young adults, rarely in older
individuals
• Blastoid cells more frequent than centroblasts/or
centrocytes
• “Starry sky” follicles, no diffuse areas (foci of DLBCL)
• BCL2 protein -/+, CD10+, BCL6+, MUM1-/+ (+ in
Waldeyer’s ring cases), MIB1 high (> 30%)
• IGH clonal rearrangement
• BCL2, BCL6, MYC rearrangement: absent, IRF4
rearrangement: some Waldeyer’s ring cases (overlapping
with LBL-IRF4)

Am J Surg Pathol. 2013 Mar; 37(3): 333–343.

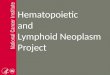
Large B-cell lymphoma with IRF4
rearrangement
• New provisional entity to distinguish from
pediatric-type FL and other DLBCL
• Children and young adult
• Localized disease, often involves cervical lymph
nodes or Waldeyer ring
• Low stage, treatment usually required
• Follicular (Grade 3B, D/D CD10-, MUM1+ FL in
older patients; pediatric-type FL, may need FISH),
follicular and diffuse, or pure diffuse pattern
• Strong MUM1+, BCL6+, high MIB1, BCL2 +/-
(NO BCL-2 rearrangement), CD10+/-

IRF4/MUM1 BCL6

Duodenal-type FL
• Localized process with low risk for
dissemination, excellent outcome
• Overlap with ISFN

Predominantly diffuse FL with 1p36
deletion
• Grade 1 to 2
• Presents as localized mass, often inguinal
• Lacks BCL2 rearrangement
• CD10+, CD23+, BCL2+/-
• 1p36 deletion not specific, seen in other
lymphomas, including classical FL
• Appearing to have good prognosis (13%
recurred and 6% progressed after
chemo/radiotherapy in 29 cases reported)

Blood.
2009;113:1053-1061

Mantle cell lymphoma (MCL)
• Two MCL subtypes: different clinicopathological
manifestations and molecular pathogenetic pathways
• Classical: Largely with unmutated/minimally
mutated IGHV and mostly SOX11+, nodal and
extranodal site
• largely with mutated IGHV and mostly SOX11-
(indolent leukemic non-nodal MCL with PB, BM,
±splenic involvement, may become more aggressive
with additional mutations, such as p53).
• Mutations of potential clinical importance, such as TP53,
NOTCH 1/2, recognized in small proportion of cases.
• CCND2 rearrangements in approximately half of cyclin
D1 negative MCL.


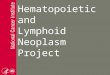
In situ mantle cell neoplasia• New name for in situ MCL, reflecting low
clinical risk
• Cyclin D1+ cells in the inner mantle zone of
follicles with preserved nodal architecture
• D/D: overt MCL with a mantle zone growth
pattern
Scientific Figure on ResearchGate. Available from:
https://www.researchgate.net/figure/257780134_fig7_Fig-8-Session-
32-Mantle-cell-lymphoma-'-in-situ-'-Case-431-P-Browne-a-At-low

Lymphoplasmacytic lymphoma (LPL)
• MYD88 L265P mutation in vast majority (90%) of
LPL and significant portion of IGM MGUS (more
closed to LPL/B-cell lymphoma than PCM)
• CXCR4: 30% of LPL (higher extent of BM
infiltration and lower leucocyte counts, haemoglobin
and platelet counts, resistant to Ibrutinib)
• Not specific for LPL: small proportion of other small
cell lymphoma (MZL, CLL); 30% non-GC DLBCL;
50% primary cutaneous DLBCL, leg type; but not
PCM, even of IGM type
• Morphology: monotony of lymphoplasmacytic
proliferation (lack of monocytoid cells, large
transformed cells), sometimes follicular colonization

Hairy cell leukemia
• BRAF V600E mutations in vast majority of
cases
• MAP2K1 mutations in most cases that that
use IGHV4-34 and lack BRAF mutation

Diffuse large B-cell lymphoma, NOS
• Distinction of GCB versus ABC/non-GC type
required with use of immunohistochemical
algorithm acceptable, may affect therapy.
• Co-expression of MYC (> 40% cells) and BCL2
(> 50% of cells) considered new prognostic
marker (20 to 35% of DLBCL, double expressor
lymphoma, most do not have MYC/BCL2
rearrangement)
• Double expressor worse outcome than other
DLBCL, NOS but better than the DHLs
• CD30 expression may be tested for new
antibody-based (anti-CD30) treatment

• GCB-DLBCL: mutations in histone methyl
transferase EZH2, cell motility regulator
GNA13, BCL2 translocation
• ABC-DLBCL: BCR/TLR and NFkB pathway
(MYD88, CD79A, CARD11, TNFSIP3)
Diffuse large B-cell lymphoma, NOS

EBV+ DLBCL, NOS
• Replaceing EBV-positive DLBCL of the
elderly (worse prognosis) since it may occur
in younger patients (with better outcome)
• Not including EBV+ B-cell lymphomas that
can be given a more specific diagnosis (e.g.
LYG)

EBV+ mucocutaneous ulcer
• New provisional entity associated with iatrogenic
immunosuppression or age-related
immunosenescence.
• Self-limited growth potential
• Conservative management
• Isolated sharply circumscribed ulcers involving
oropharyngeal mucosa, skin, and gastrointestinal
tract
• Polymorphous infiltrate and atypical large B-cell
blasts often with Hodgkin/Reed-Sternberg (HRS)
cell-like morphology
• B cells showed strong CD30 and EBER positivity
• CD15 -/+, CD20+/-

Modern Pathology (2013) 26, S42–S56
Blood 2011;117(18):4726-4735

Burkitt lymphoma
• TCF3 or ID3 (negative regulator of TCF3)
mutations in up to approximately 70% of
sporadic and immunodeficiienty related cases
and 40% of endemic cases
• TCF3 activating BCR/PI3K pathway
promoting survival and proliferation of
lymphoid cells

Burkitt-like lymphoma with 11q
aberration
• New provisional entity that closely resembles
Burkitt lymphoma but lacks MYC
rearrangement
• Clinical course and gene expression profile
similar to BL
• Interstitial gains including 11q23.2-q23.3 and
telomeric losses of 11q24.1-qter
• More complex karyotypes, lower level of MYC
expression, certain degree of cytological
pleomorphism, sometimes a follicular patten,
frequently nodal presentation

CD20
BCL6MIB1

High grade B-cell lymphoma, with MYC
and BCL2 and/or BCL6 translocations
• New category for all ‘double/triple hit’
lymphomas other than FL or lymphoblastic
lymphomas.

High grade B-cell lymphoma, NOS
• Together with the new category for the
‘double/triple hit’ lymphomas, replacing the
2008 category of B-cell lymphoma,
unclassifiable, with features intermediate
between DLBCL and Burkitt lymphoma
(BCLU)
• Includes blastoid-appearing large B-cell
lymphomas and cases lacking MYC and
BCL2 or BCL6 translocations that would
formerly have been called BCLU

MYC R


Peripheral T-cell lymphoma (PTCL),
NOS• Subsets based on phenotype and molecular
abnormalities being recognized that may have clinical
implications but are mostly not a part of routine
practice at this time.
• GATA3 overexpression subtype: inferior prognosis,
high levels of Th2 cytokines
• Mutations of epigenetic mediators: KMT2D, TET2,
KDM6A, ARID1B, DNMT3A, CREBBP, MLL AND
ARID2.
• Mutations in signaling pathway: TNFAIP3, APC,
CHD8, ZAP70, NF1, TNFRSF14, TRAF3
• Mutations in tumor suppressors: TP53, FOXO1, ATM

Node-based EBV+ PTCL
• Considered a variant of PTCL, NOS
• EBV in the majority of neoplastic cells
• Monomorphic, lack of angioinvation and
necrosis
• Older pateints, post-transplant setting, other
immunodeficiency states

Nodal T-cell lymphomas with T
follicular helper (TFH) phenotype• A new umbrella category created to highlight the
spectrum of nodal lymphomas with a TFH
phenotype : angioimmunoblastic T-cell lymphoma,
follicular T-cell lymphoma and other nodal PTCL
with TFH phenotype (specific diagnoses to be used
due to clinicopathologic differences)
• TFH phenotype: at least 2 or 3 of TFH-related
antigens: CD279/PD1, CD10, BCL6, CXCL13,
ICOS, SAP, CCR5
• Overlapping recurrent molecular/cytogenetic
abnormalities: TET2, IDH2, DNMT3A, RHOA,
CD28 mutations; ITK-SYK OR CTLA4-CD28 fusion

• AITL and FTCL: EBV+ B-cell blasts,
progression to EBV+ (rarely EBV-) BCL
• FTCL: localized disease, fewer systemic
symptoms
Nodal T-cell lymphomas with T
follicular helper (TFH) phenotype

ALK-negative anaplastic large cell
lymphoma
• Now a definite entity
• Convergent mutations and kinase fusions
leading to activation of JAK/STAT3 pathway
• Including cytogenetic subsets with
prognostic implications:
• 6p25 rearrangements at IRF4/DUSP22
locus: relatively monomorphic, lack
cytotoxic granules, superior prognosis,
also occurring in LYP, primary
cutaneous ALCL
• TP63 rearrangement: very aggressive


Breast implant-associated anaplastic
large cell lymphoma
• New provisional entity distinguished from
other ALK-negative ALCL
• Seroma fluid between the implant and
surrounding fibrous capsule.
• Both saline and silicone implants
• Median time interval: 10 years
• If no invasion of the capsule, removal of
implant and capsule
• If invasion through the capsule, systemic
chemotherapy due to risk of LN involvement
and systemic spray


CD3CD45
CD30TIA1
GRAZYME BALK1


Primary cutaneous acral CD8+ T-cell
lymphoma
• New provisional entity
• Indolent, originally described as originating in the ear,
almost always localized to a single site
• Clonal CD8+ cytotoxic T-cells
• Dense, diffuse proliferation of monomorphous
medium-sized T cells throughout the dermis and
subcutis; no epidermotropism
• CD3+, CD8+, CD4−, TIA1+, granzyme B−
• Conservative management only
• D/D: primary cutaneous CD8+ aggressive
epidermotrophic cytotoxic T-cell lymphoma

CD8
haematologica | 2014; 99:1421

T-cell large granular lymphocyte
leukemia
• New subtypes recognized with clinicopathologic
associations.
• STAT3 mutations common (also in NK-LGL)
• STAT5B mutations in a subset, associated with
more clinically aggressive disease.

Systemic EBV+ T-cell Lymphoma of
childhood
• Name changed from lymphoproliferative
disorder to lymphoma due to its fulminant
clinical course and desire to clearly
distinguish it from chronic active EBV
infection (CAEBV).
• CAEBV: from indolent/localized forms
(hydroa vacciniforme-like LPD, severe
mosquito bite allrgy ) to a more systemic
form with fever, hepatosplenomegaly,
lymphadenopathy, w/wo skin manifestations.
• D/D: EBV associated HLH, may response to
HLH 94 protocol, not neoplastic

Hydroa vacciniforme-like
lymphoproliferative
disorder
• Name changed from lymphoma to
lymphoproliferative disorder.
• Relationship with CAEBV and a spectrum in
terms of its clinical course.

Enteropathy associated T-cell
lymphoma (EATL)
• Diagnosis only to be used for cases formerly
known as type I EATL
• Typically associated with celiac disease
• Predominantly occurring in patients of
northern European origin

Monomorphic epitheliotropic
intestinal T-cell lymphoma (MEITL)
• Formerly type II EATL
• Lack of association with celiac disease
• Asians and Hispanic population
• Monomorphic, expression of CD8, CD56
and MAPK, most are GD-T cells,
• STAT5B mutation
• Gains in 8q24 involving MYC

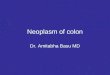
Indolent T-cell lymphoproliferative
disorder of the GI tract
• New provisional entity
• diffuse, band-like monoclonal intestinal T-
cell infiltration of the lamina propria, and,
focally, the submucosa by lymphoid infiltrate
• Clonal cytotoxic T-cells: CD8+ >> CD4
• Indolent clinical course, some cases show
progression

Blood 2013, 122:3599

TIA1
CD8CD4
Blood 2013, 122:3599

CD8CD4
Blood 2013, 122:3599

Phenotype/genotype: T-LPD
• CD3+, CD2+, CD5±, CD7±, CD56-, TCRβ+,
TCRγ-, EBER-, CD30-.
• Ki-67 up to 5-10%.
• CD8+ cases (majority): TIA1+, granz B-
• CD4+ cases: cytotoxic marker negative
• Clonal TCRγ rearrangements (1 oligoclonal)

D/D: Histologically/
immunophenotypically
Indolent T-LPD: nondestructive, involving the
lamina propria and muscularis mucosae, small
mature cells.
EATL : large and destructive infiltrate.
medium- to large-sized pleomorphic cells with
prominent nucleoli; the intestinal mucosa
adjacent to the main tumor mass frequently
shows evidence of enteropathy (Not indolent T-
LPD)

MEITL: destructive infiltrate, monotonous and
small to medium-sized cells, florid infiltration
of the intestinal crypt epithelium and adjacent
intestinal mucosa by lymphoma cells (Not
indolent T-LPD).
MEITL: CD3+, CD8+, CD56+, often TCR-
G+, CD4-.
CD56- in indolent T-LPD also aids in the
distinction from NK cell enteropathy.

Primary cutaneous CD4+ small
medium T-cell lymphoproliferative
disorder
• Remains a provisional entity.
• No longer to be diagnosed as an overt
lymphoma due to limited clinical risk,
localized disease, and similarity to clonal
drug reactions.

Nodular lymphocyte predominant
Hodgkin lymphoma
• Variant growth patterns, if present, should be noted in
diagnostic report: “classic” (B-cell-rich) nodular
(patter A), serpiginous/interconnected nodular (B),
nodular with prominent extranodular L&H cells (C),
T-cell-rich nodular (D), diffuse with a T-cell-rich
background (T-cell-rich B-cell lymphoma [TCRBCL]-
like) (E), and a (diffuse) B-cell-rich pattern (F)
• Presence of many extranodular L&H cells (pattern C)
predicts for progression to a diffuse pattern


• Histopathologic NLPHL variants (pattern C,
D, E, F) are associated with advanced disease
and a higher relapse/progress rate.
• Cases associated with synchronous or
subsequent sites indistinguishable from
THRLBCL without a nodular component
should be designated THRLBCL-like
transformation.

Erdheim-Chester disease
• Should be distinguished from other members
of the juvenile xanthogranuloma family
• Often associated with BRAF mutations

Other histiocytic/dendritic neoplasms
• Clonal relationship to lymphoid neoplasms
(FL, CLL, T/B lymphoblastic lymphoma,
PTCL) recognized in some cases.
• Indicating transdifferentiaiton.
• V600E in LCH, histiocytic sarcoma,
disseminatied JXG, ECD, FDCS