Embed Size (px)
Citation preview
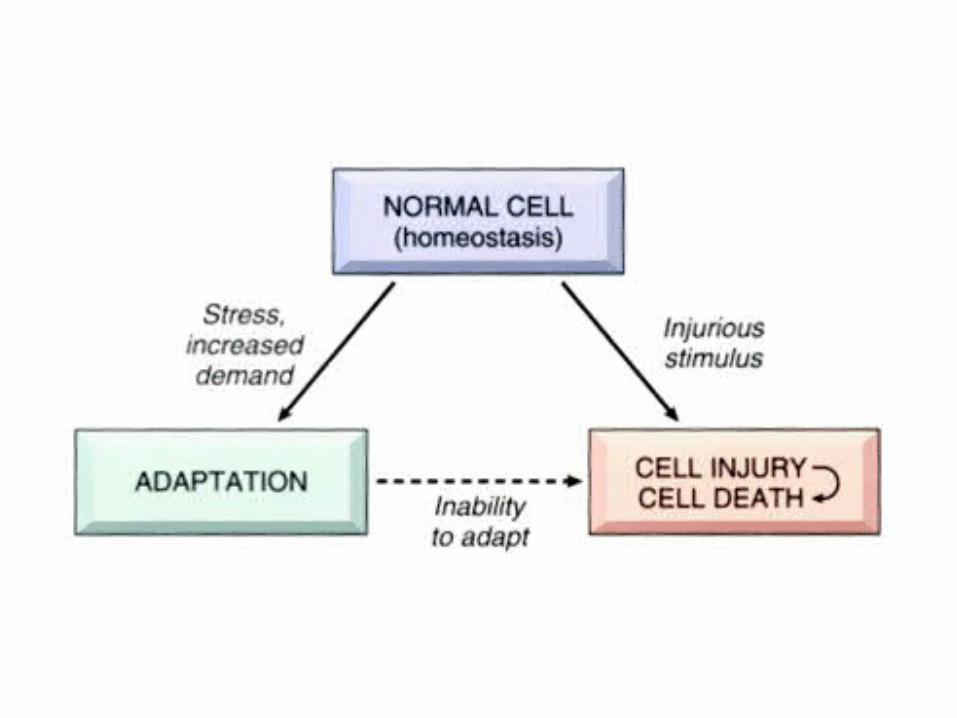
Cellular adaptation
Cell Injury

Cellular adaptation• Cells are the structural and functional units of tissues and
organs. They are capable of adjusting their structure and functions in response to various physiological and pathological conditions. This capability is called cellular adaptation.
• Cellular adaptations include:– Atrophy--shrinkage of cells – Hypertrophy--increase in the size of cells which results in
enlargement of the organs – Hyperplasia--increased number of cells in an organ or
tissue – Metaplasia--transformation or replacement of one adult
cell type with another
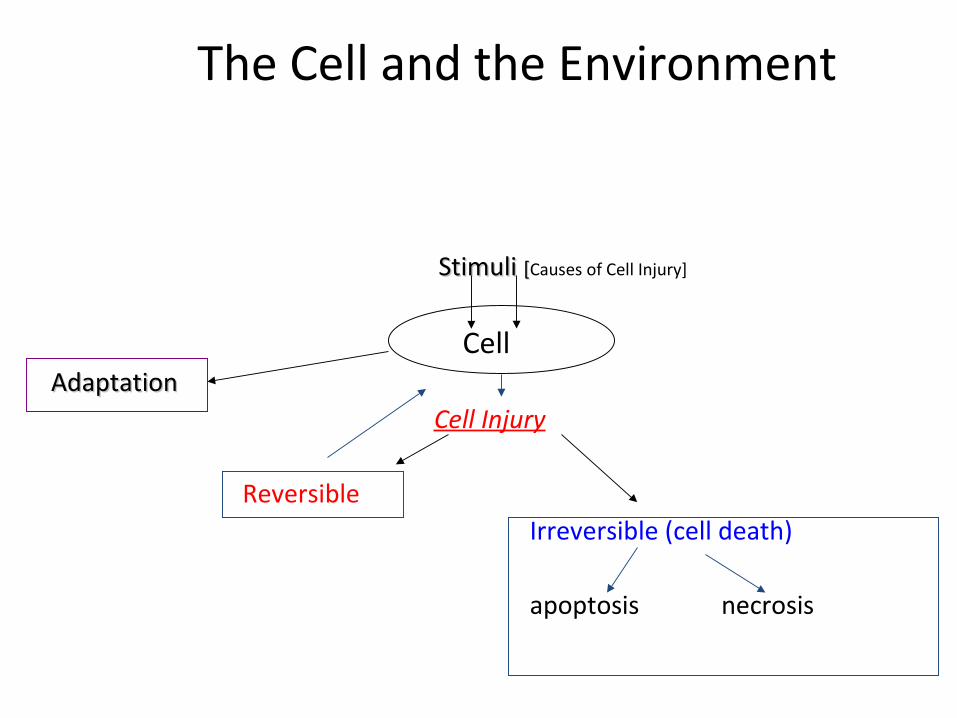
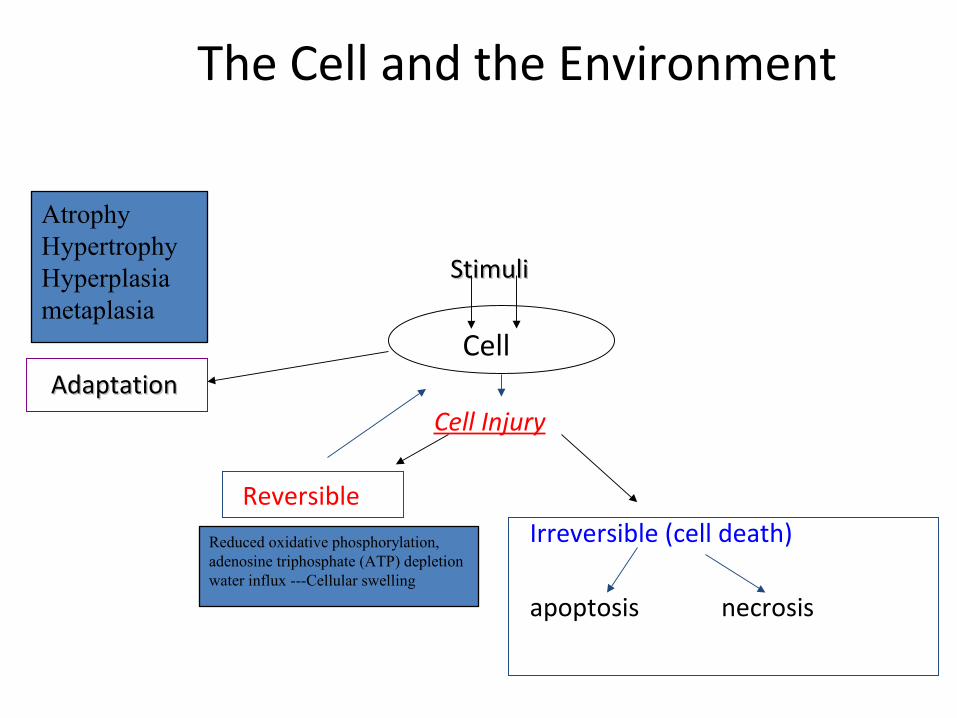
The Cell and the Environment
Stimuli Stimuli [[Causes of Cell Injury]
Cell AdaptationAdaptation
Cell Injury
ReversibleIrreversible (cell death)
apoptosis necrosis
Apoptosis
Necrosis

Cell injury
• If the cells fail to adapt under stress, they undergo certain changes called cell injury. The affected cells may recover from the injury (reversible) or may die (irreversible).
Causes of Cell Injury1.1. Hypoxia: Hypoxia: (Oxygen deficiency) Mainly due to:
ischemia (impaired blood supply) most commonmost common inadequate oxygenation of blood (cardio-respiratory failure) loss of oxygen carrying capacity (anaemia) Carbon monoxide poisoning
1.1. Physical AgentsPhysical Agents Trauma, radiation, extremes of temperatures, electric shock
1.1. Chemicals and DrugsChemicals and Drugs Wide variety
1. Microbiologic Agents Viruses, worms, bacteria …..
1. Immunologic Reactions Allergic reactions, autoimmune diseases
1. Genetic Defects Obvious congenital malformations (Down syndrome) Subtle single amino acid substitution (hemoglobin S of sickle cell anemia)
1. Nutritional Imbalances Deficiency of nutrients/ or excess
1. Aging
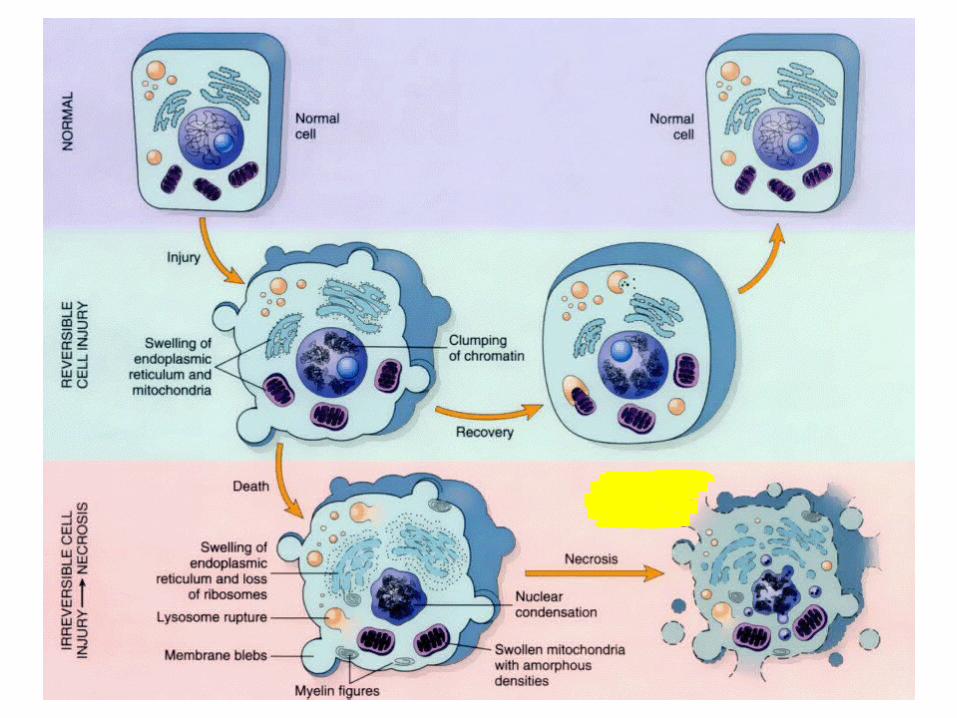
Morphology of cell injury
• Reversible:– Cellular swelling and vacuole formation (Hydropic
changes) – Changes at this stage are better appreciated by
EM that may show blebbing of the plasma membrane, swelling of mitochondria and dilatation of ER
– Fatty changes
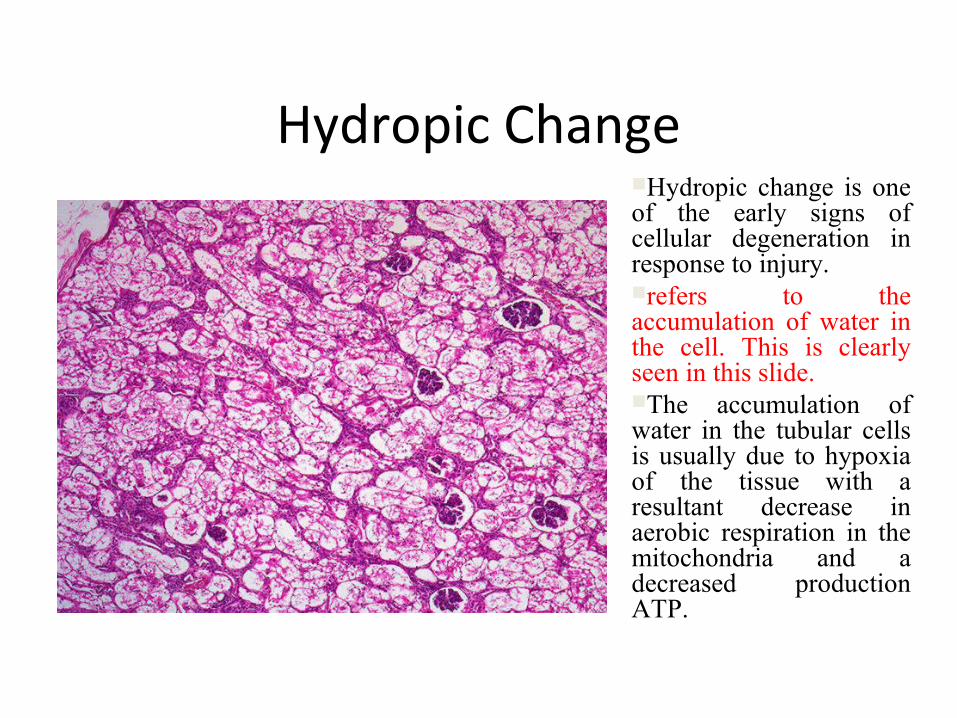
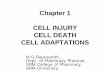
Hydropic change is one of the early signs of cellular degeneration in response to injury.refers to the accumulation of water in the cell. This is clearly seen in this slide. The accumulation of water in the tubular cells is usually due to hypoxia of the tissue with a resultant decrease in aerobic respiration in the mitochondria and a decreased production ATP.
Hydropic Change
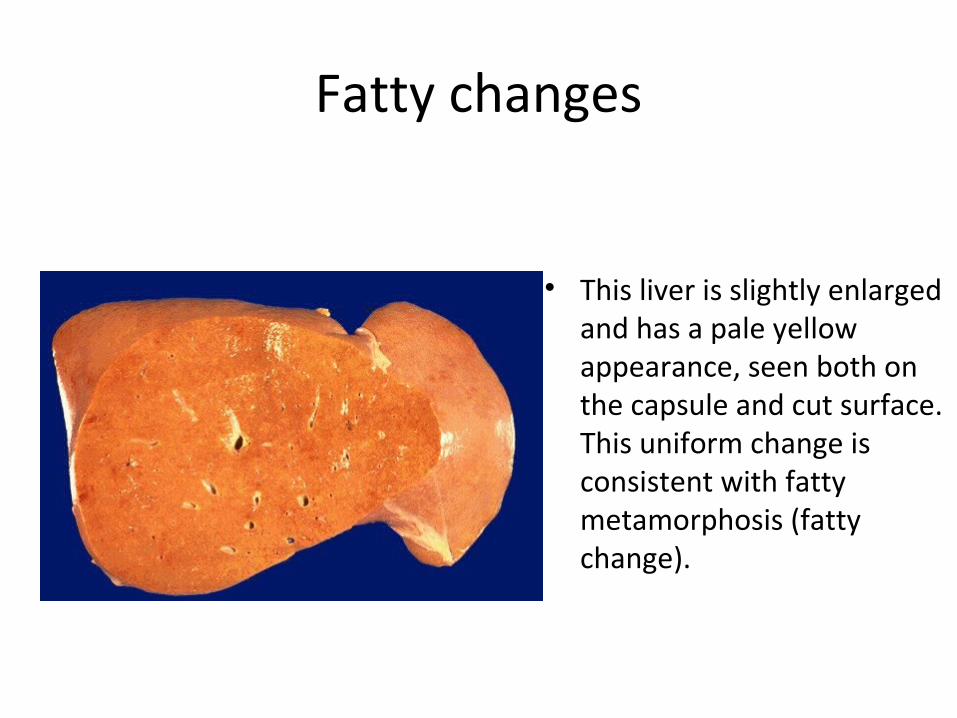
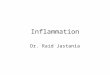
Fatty changes
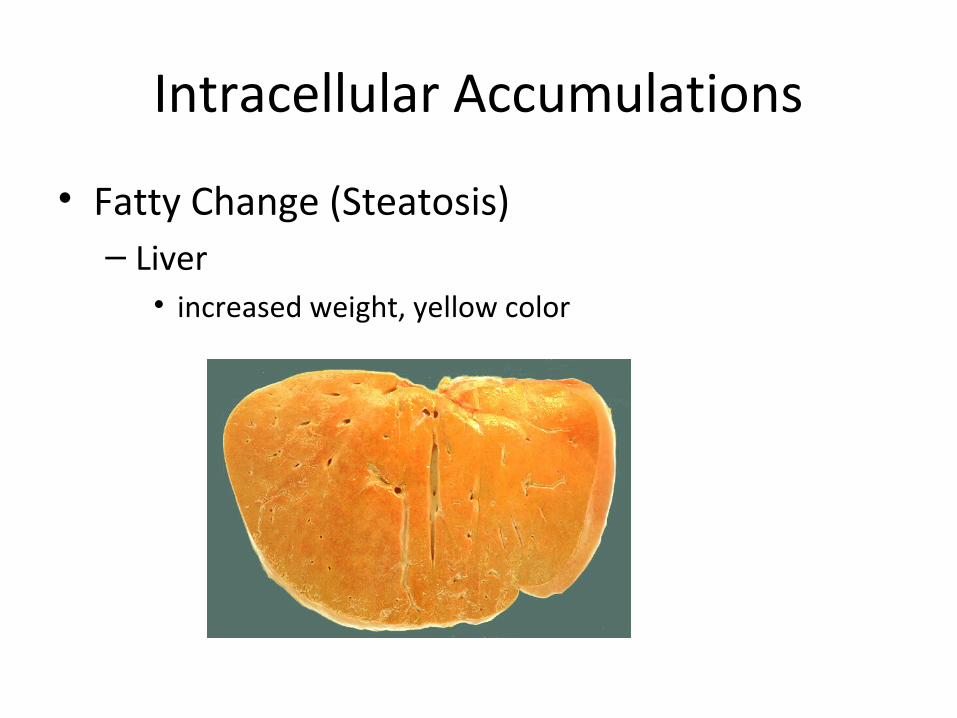
• This liver is slightly enlarged and has a pale yellow appearance, seen both on the capsule and cut surface. This uniform change is consistent with fatty metamorphosis (fatty change).
Morphology of cell injury
• Irreversible/Necrosis– The changes are produced by enzymatic digestion of dead
cellular elements, denatunation of proteins and autolysis (by lysosomal enzymes)
– Cytoplasm - increased eosinophilia – Nucleus - nonspecific breakdown of DNA leading to
• pyknosis (shrinkage), • karyolysis (fading) and • karyorrhexis (fragmentation
The Cell and the Environment
StimuliStimuli [Causes of Cell Injury]
Cell AdaptationAdaptation
Achieving a new steady state and preserving viability
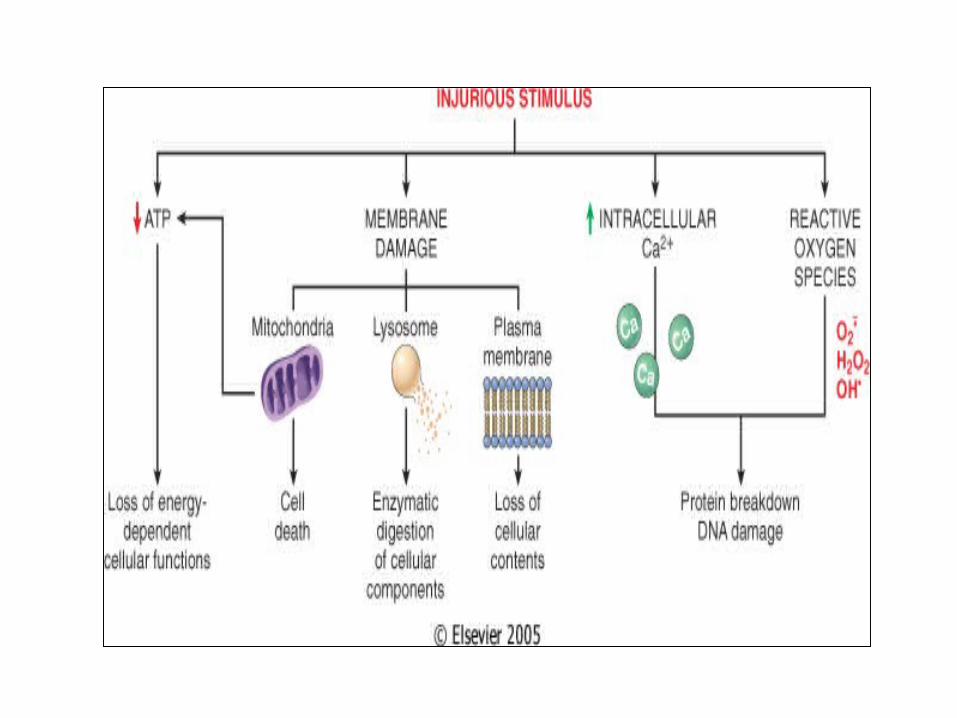
IMPORTANT TARGETS OF CELL INJURY
• Aerobic respiration – – ATP depletion or decreased synthesis.
• Cell membranes - plasma membranes, mitochondrial, lysosomal and other organelle membranes.
• Protein synthesis.• Cytoskeleton.• Genetic apparatus.
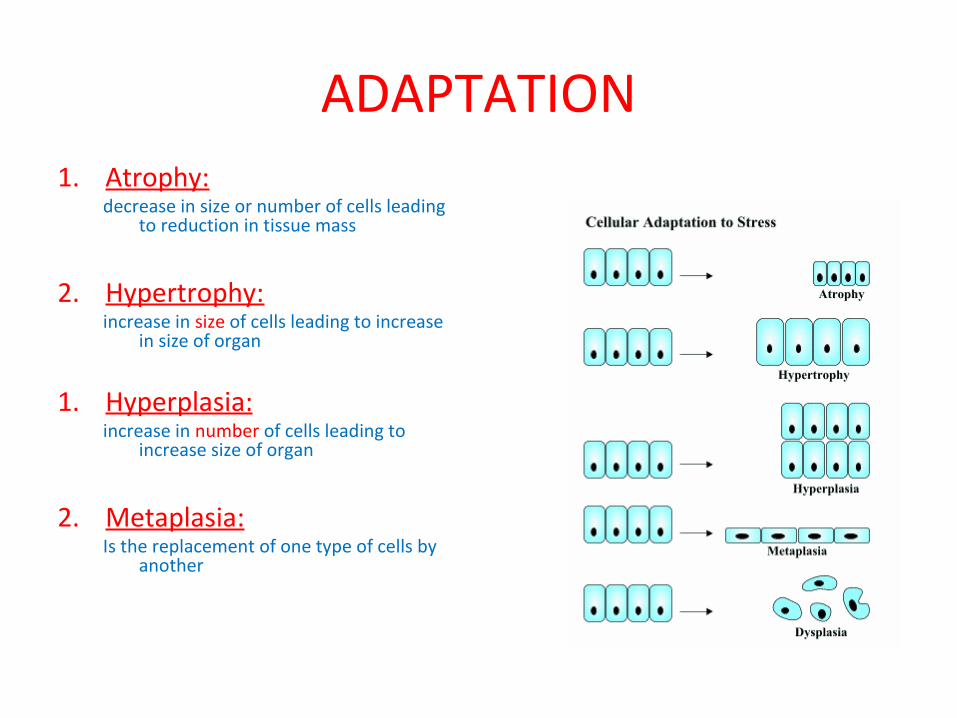
ADAPTATION1. Atrophy:
decrease in size or number of cells leading to reduction in tissue mass
2. Hypertrophy:increase in size of cells leading to increase
in size of organ
1. Hyperplasia:
increase in number of cells leading to increase size of organ
2. Metaplasia:Is the replacement of one type of cells by
another
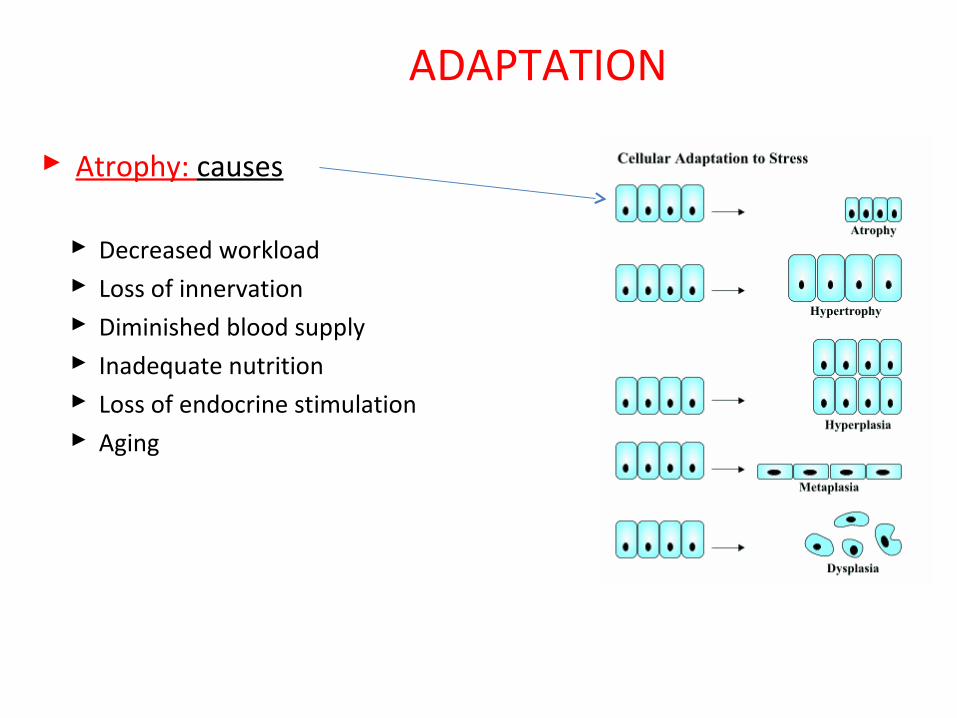
ADAPTATION
Atrophy: causes
Decreased workload Loss of innervation Diminished blood supply Inadequate nutrition Loss of endocrine stimulation Aging
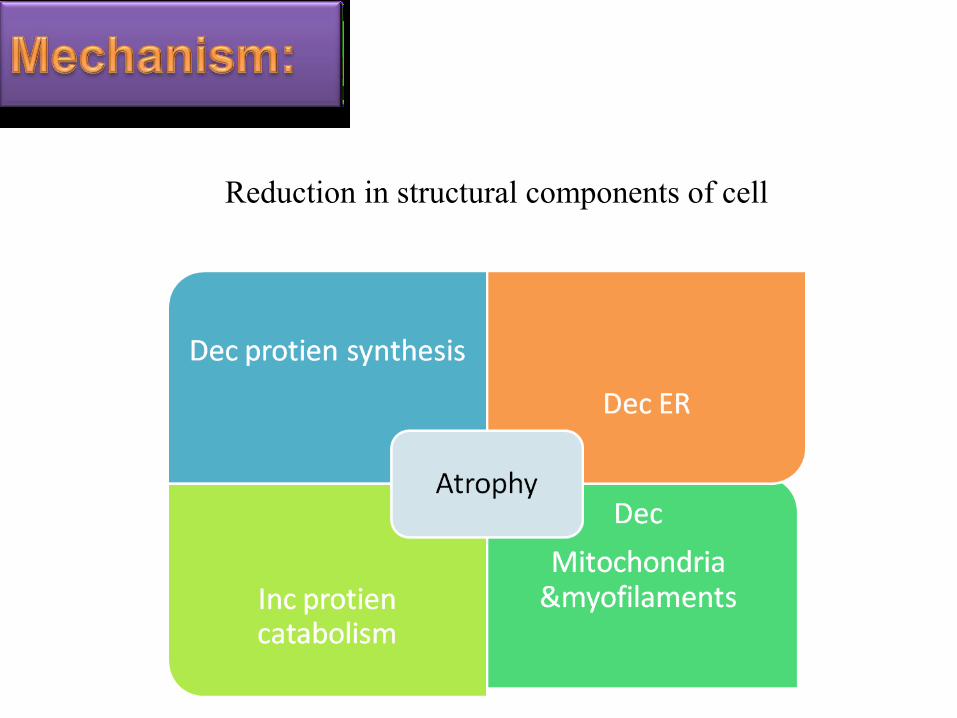
Reduction in structural components of cell

1.Atrophy of thymus gland 2.thyroglossal duct after birth 3.atrophy of ovaries & uterus after menopause 4.Atrophy of uterus following child birth
PHYSIOLOGICAL
TYPES OF ATROPHY
1. Starvation
PATHOLOGICAL
3. Senile atrophy : in old age
2.Neuropathic atrophy: due to loss of innervation
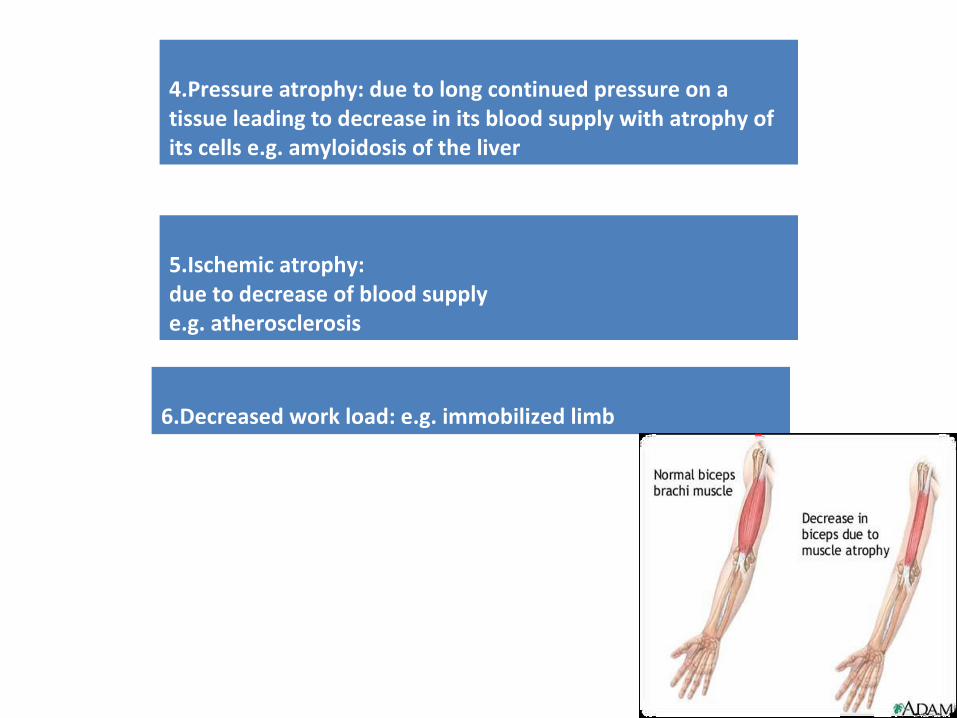
4.Pressure atrophy: due to long continued pressure on a tissue leading to decrease in its blood supply with atrophy of its cells e.g. amyloidosis of the liver
6.Decreased work load: e.g. immobilized limb
5.Ischemic atrophy: due to decrease of blood supply e.g. atherosclerosis
How To Avoid Atrophy?
1.eating a healthy diet 2.getting regular, moderate exercise 3.avoiding smoking or quitting 4.Do not stay in one position for too long
ADAPTATION
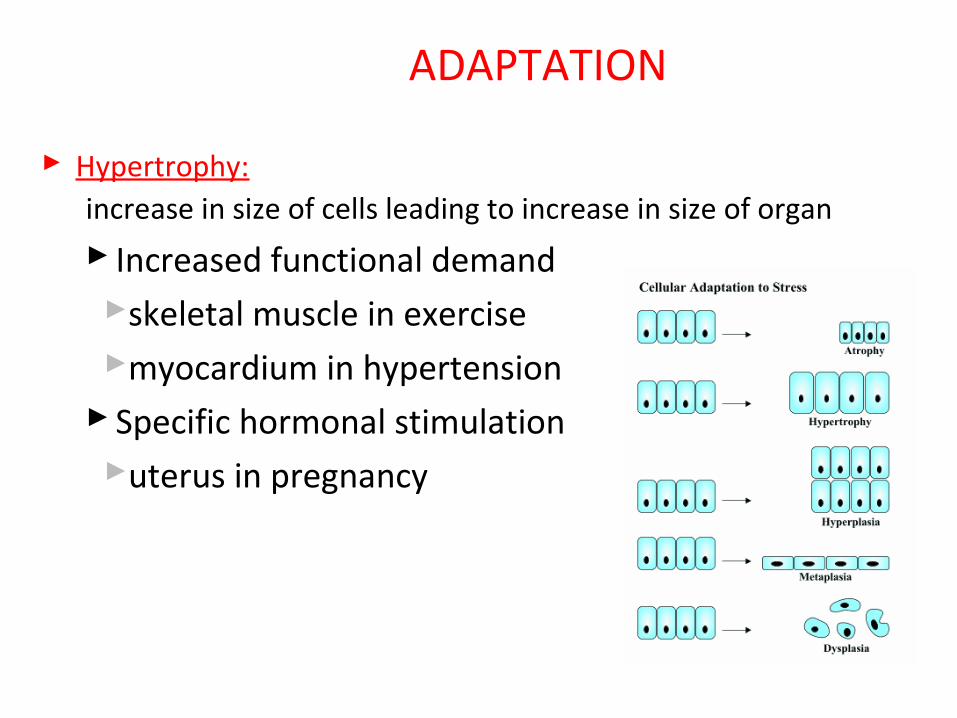
Hypertrophy:increase in size of cells leading to increase in size of organ
Increased functional demandskeletal muscle in exercisemyocardium in hypertension
Specific hormonal stimulationuterus in pregnancy
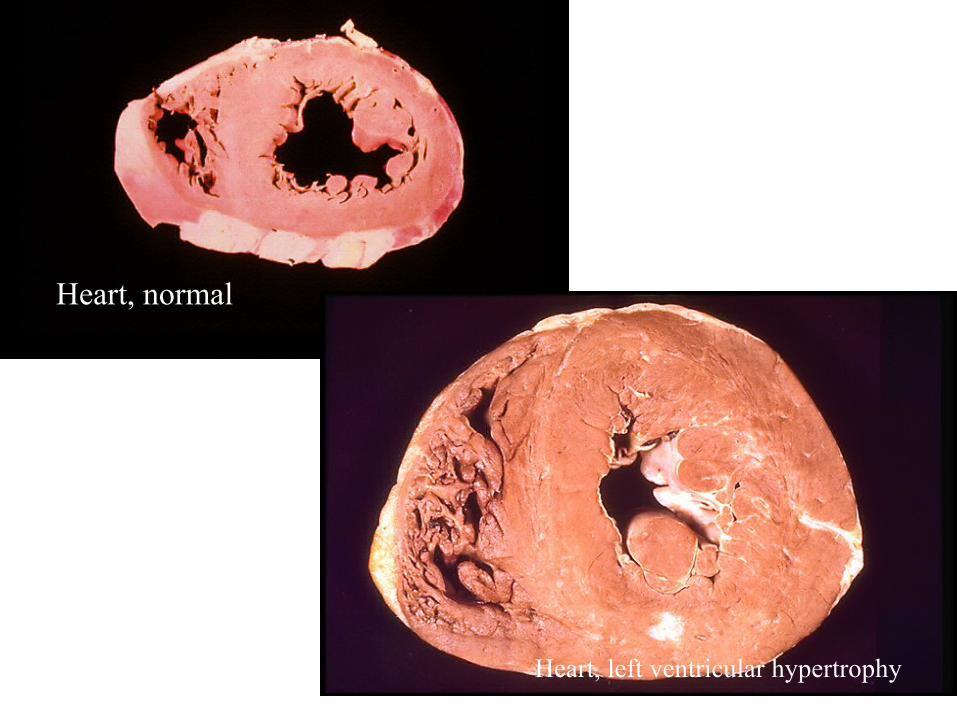
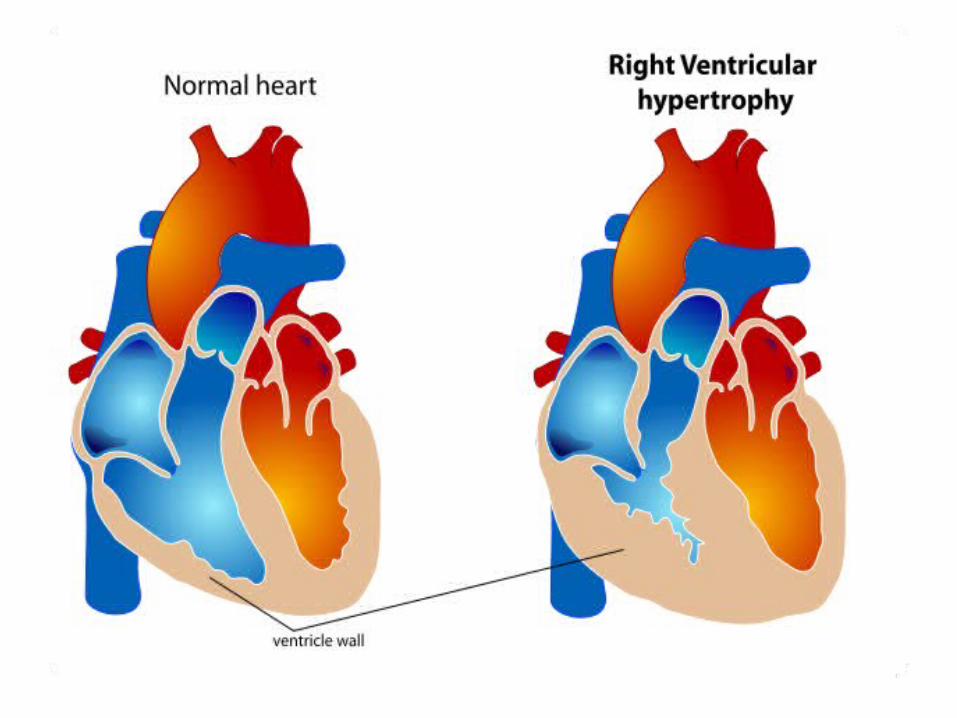
Heart, left ventricular hypertrophy
Heart, normal
TYPES• Physiological Hypertrophy
Increase in size due to increased work load or exercise. The common examples includes:
I- Muscular hypertrophy: increase in bulk of skeletal muscles that occurs in response to strength training exercise
II- Ventricular hypertrophy: Increase in size of ventricular muscles of the heart-good if it occurs in response to exercise

Continued….• Pathological Hypertrophy
Increase in cell size in response to pathological changes
Example: Ventricular hypertrophy that occurs due to pathological conditions such as high blood pressure where the work load of ventricles increases

Continued…• Compensatory Hypertrophy
Increase in size of cell of an organ that occurs in order to compensate the loss or dysfunction of another organ of same type
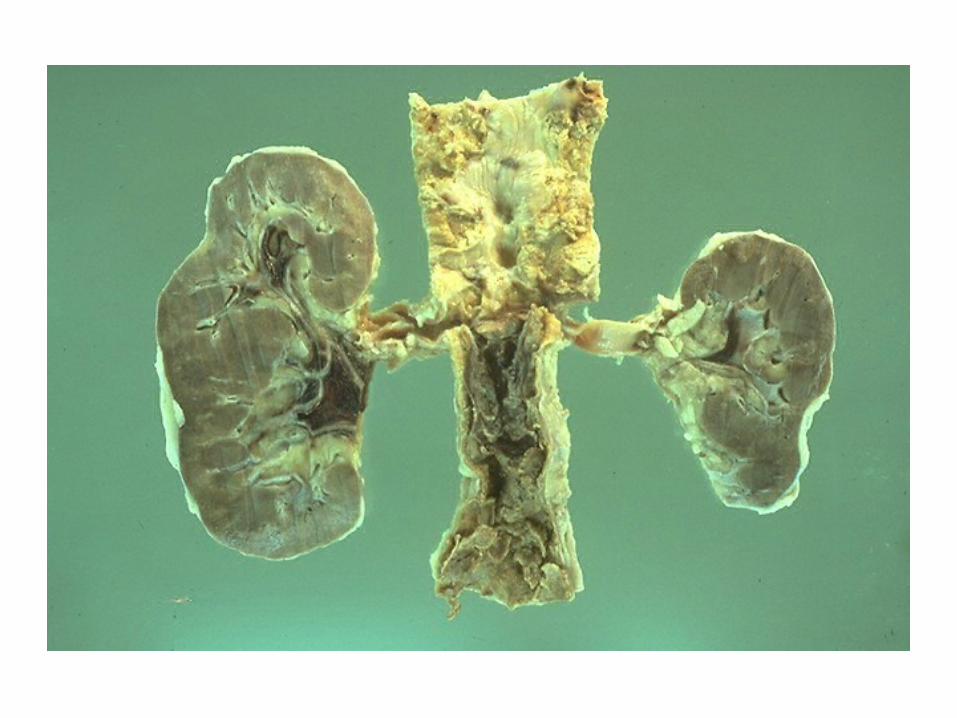
Examples: Hypertrophy of one kidney when the other kidney stops functioning
Increase in muscular strength of an arm when other arm is lost or dysfunction
ADAPTATION
Hyperplasia:increase in number of cells leading to increase size of
organ Physiologic
Hormonal (breast during pregnancy) Compensatory (partial hepatectomy)
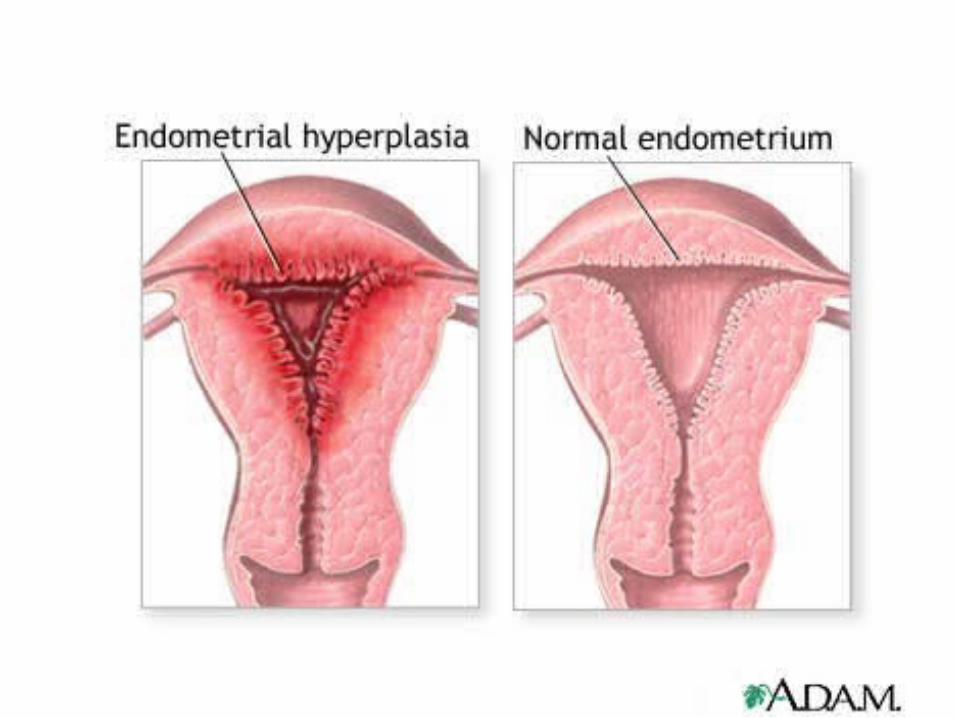
Pathologic Excessive hormonal / growth factor absolute or relative increase in estrogen over
progesterone--endometrial hyperplasiaBenign Prosthetic hyperplasia (androgens)
Hyperplasia: Mechanism
• Cell proliferation
• via increased production of TRANSCRIPTION FACTORS due to
* Increased production of GF
* Increased levels of GF receptors
* Activation of intracellular signaling
• Results in larger organ
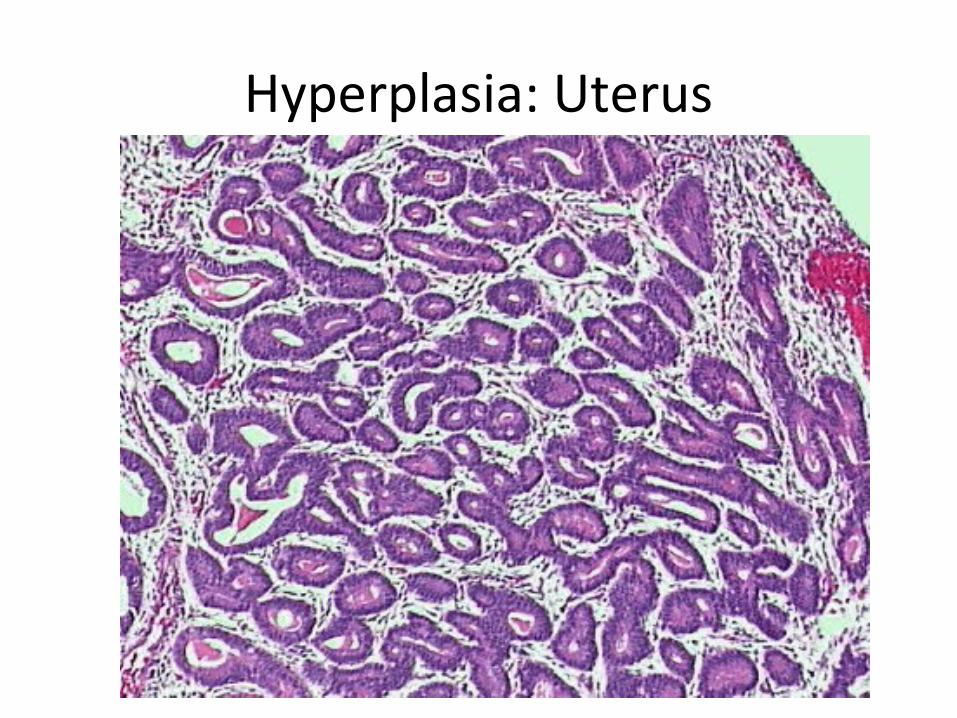
Hyperplasia: Uterus

Thyroid Hyperplasia
ADAPTATION
Metaplasia:• Is the replacement of one type of cells by anotherTYPES:Physiological metaplasia: Replacement of cells in normal conditions Examples: transformation of cartilage into bones and transformation of
monocytes into macrophagesPathological Metaplasia: Irrevesible replacement of cells due to constant
exposure to harmful stimuluiExample: Chronic smoking results in transformation of normal mucus
secreting ciliated columnar epithilial cells into non mucus secreting non ciliated squamous epithilial cells which become cancerous cells if stimulus (smoking) is prolonged Squamous Metaplasia
Intestinal Metaplasia Lower esophageal epithelium
chronic gastric reflux
Metaplasia: Mechanism
• Reprogramming
1. of stem cells present in normal tissues
2. of undifferentiated mesenchymal cells in connective tissue
• Mediated by signals from
cytokines, Growth Factor Leading to induction of specific transcription factors
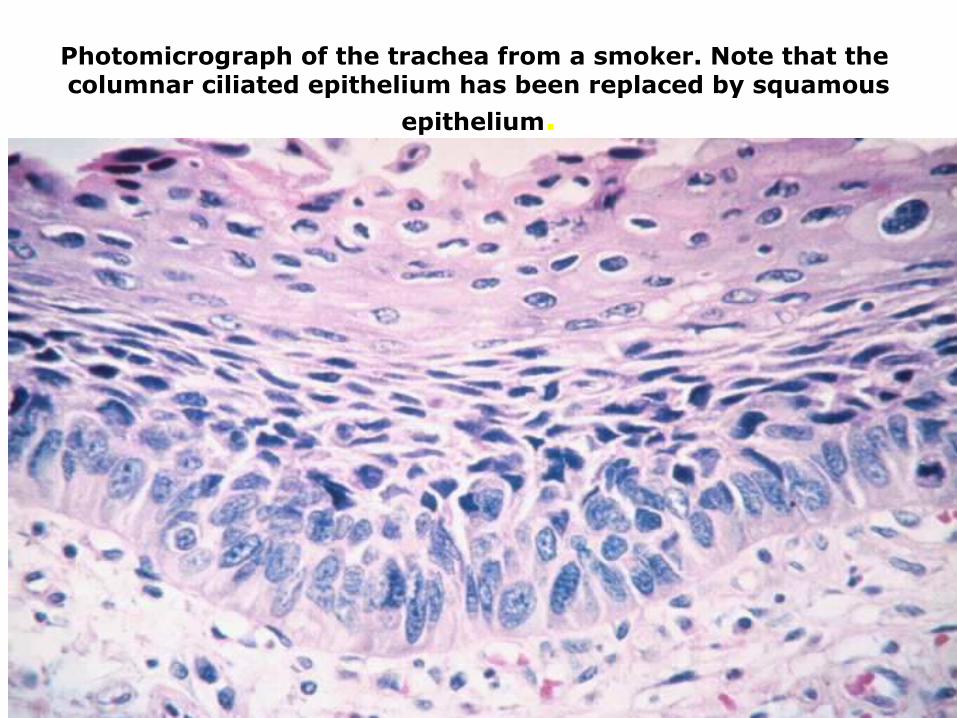
Photomicrograph of the trachea from a smoker. Note that the columnar ciliated epithelium has been replaced by squamous
epithelium.
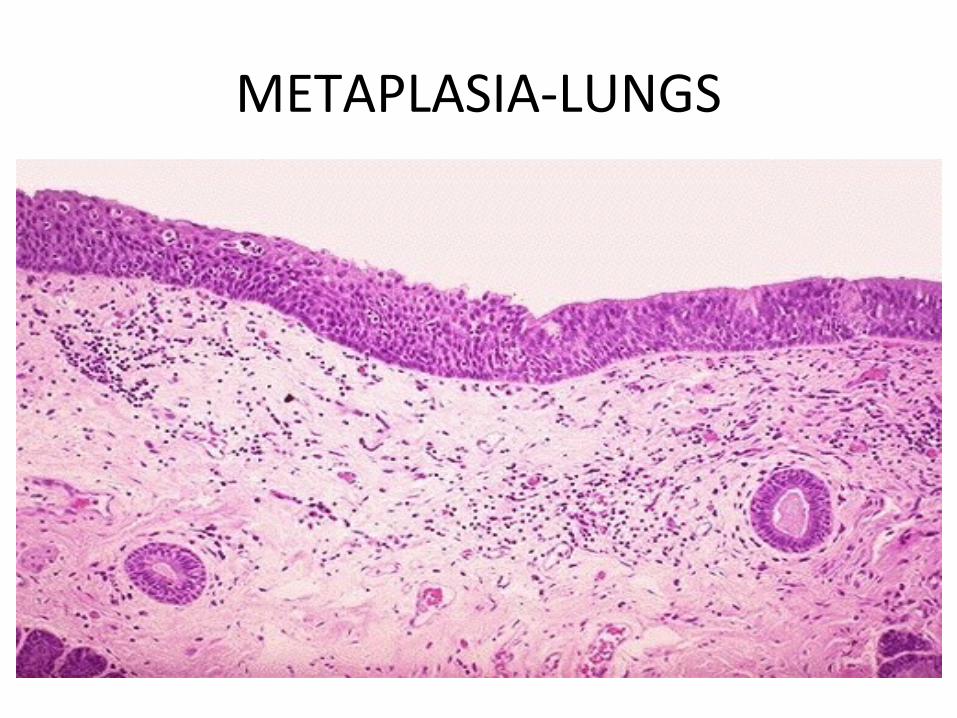
METAPLASIA-LUNGS
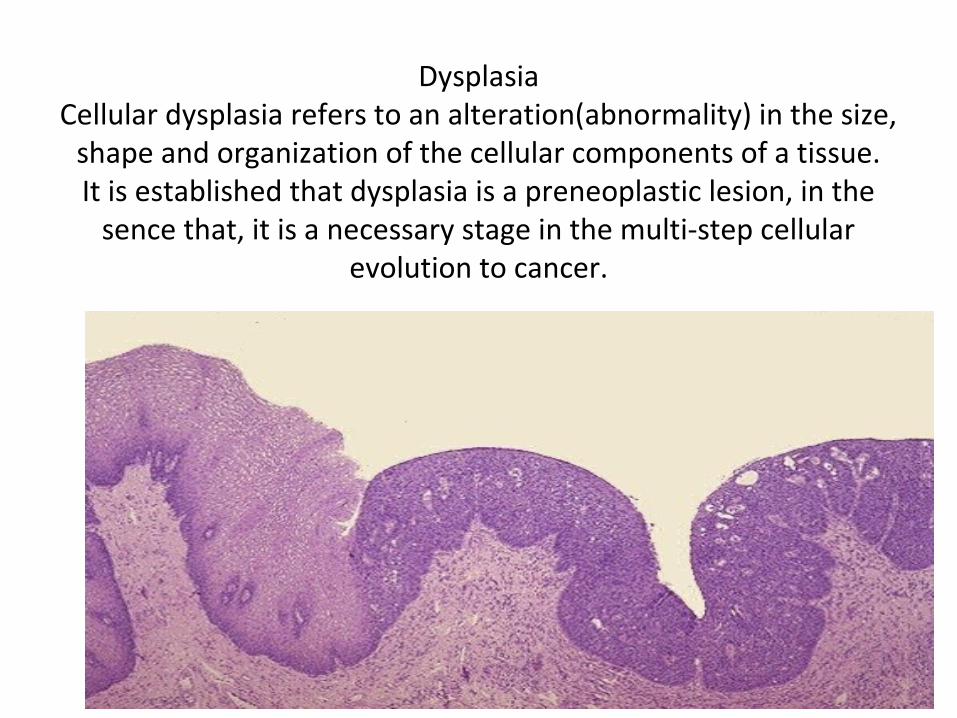
DysplasiaCellular dysplasia refers to an alteration(abnormality) in the size,
shape and organization of the cellular components of a tissue.It is established that dysplasia is a preneoplastic lesion, in the
sence that, it is a necessary stage in the multi-step cellular evolution to cancer.
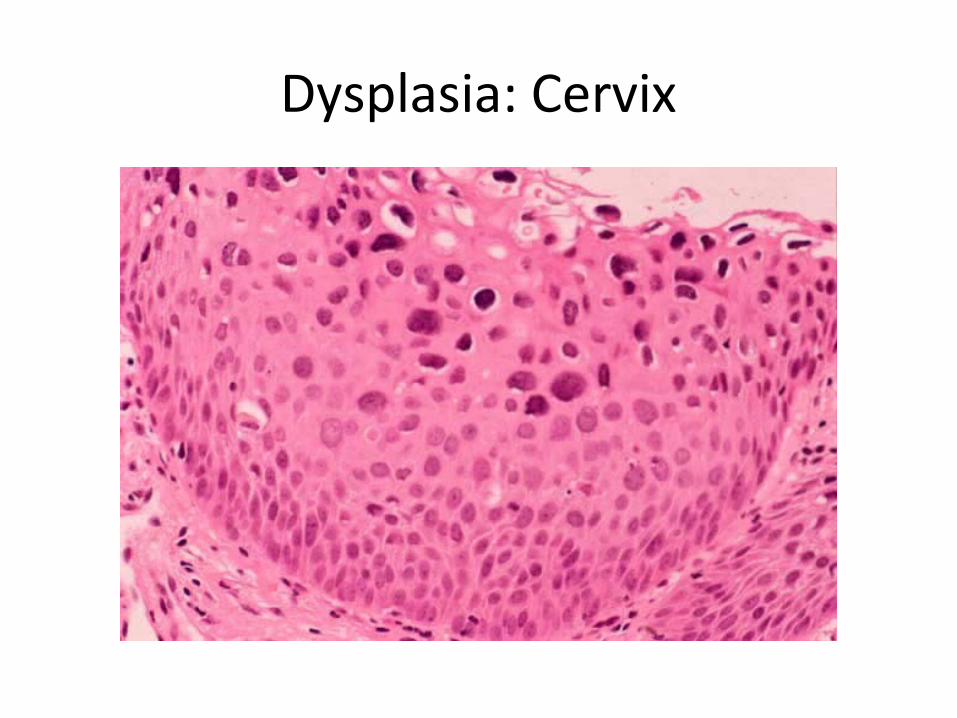
Dysplasia: Cervix

Aplasia
• Defective development resulting in the absence of all or part of an organ or tissue
Aplasia Cutis Congenita
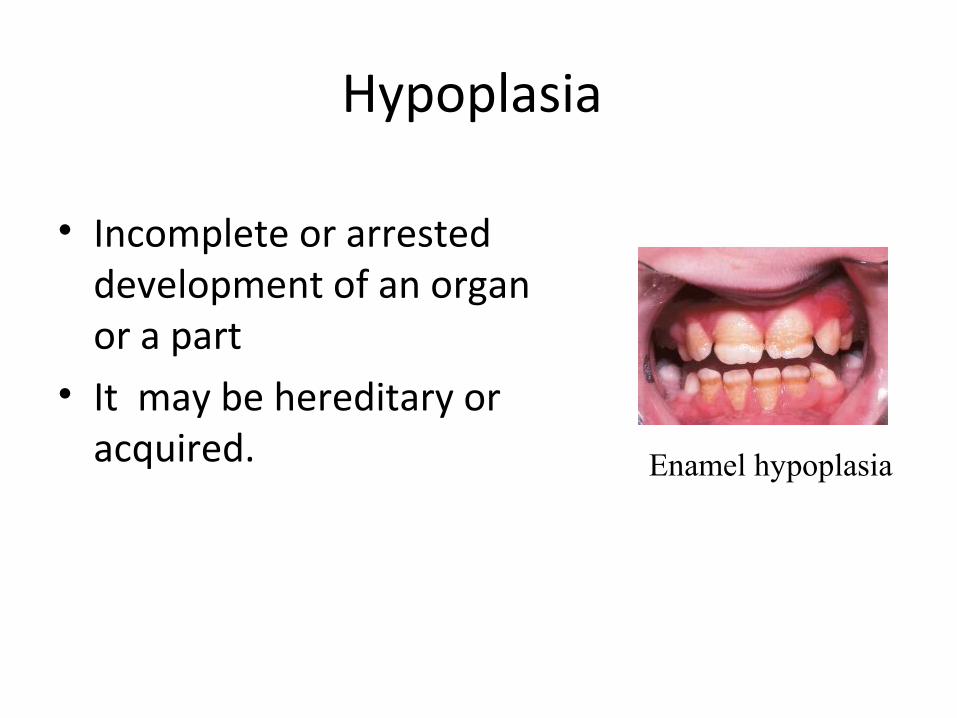
Hypoplasia
• Incomplete or arrested development of an organ or a part
• It may be hereditary or acquired. Enamel hypoplasia
The Cell and the Environment
StimuliStimuli
Cell AdaptationAdaptation
Cell Injury
ReversibleIrreversible (cell death)
apoptosis necrosis
Atrophy HypertrophyHyperplasiametaplasia
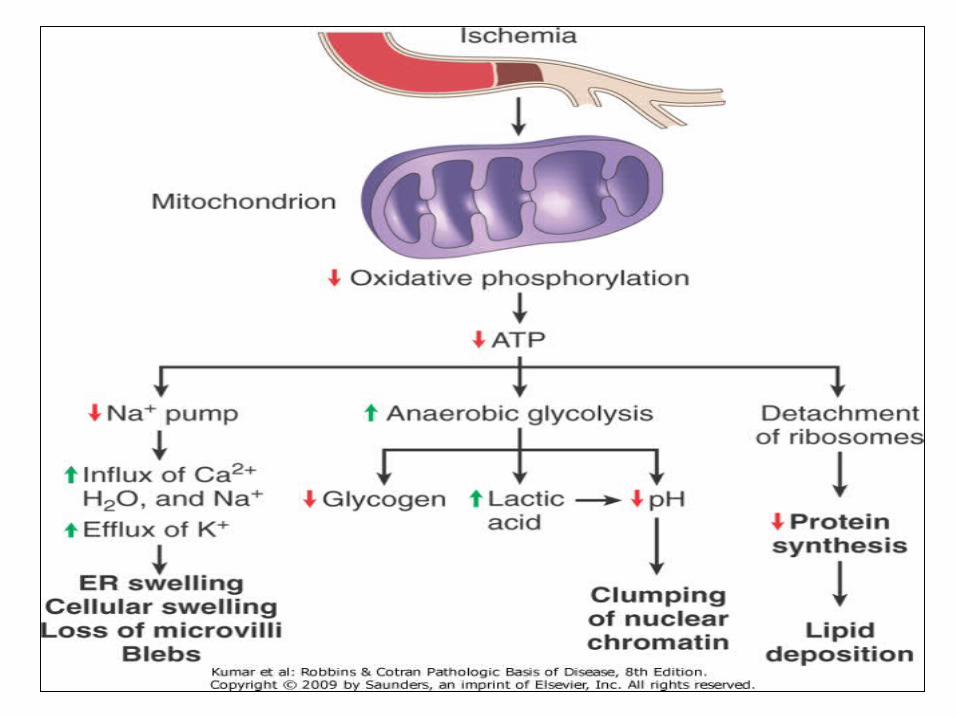
Reduced oxidative phosphorylation, adenosine triphosphate (ATP) depletionwater influx ---Cellular swelling
Mechanisms of cell injury
Depletion of ATP
• Usually in hypoxic and chemical injuries.• Sources : oxidative phosphorylation of ADP in
the mitochondria and Glycolytic pathway using Glucose.
• The major causes of ATP depletion are reduced supply of oxygen and nutrients, mitochondrial damage and the actions of some toxins (Cyanide).
ATP depletion continued….
• Tissues with a greater glycolytic capacity (liver) are more able to survive loss of oxygen and decreased oxidative phosphorylation better than are tissues with limited capacity for glycolysis (brain).
• Low oxygen situation results in misfolding of proteins which trigger a cellular response called the unfolded protein response that may lead to cell death (Activation of apoptosis).
Mitochondrial damage• Supplies ATP (energy) to the cell.• Damaged by Calcium influx, reactive oxygen species,
radiation, oxygen deprivation, toxins and mutations in mitochondrial genes.
• Consequences of mitochondrial damage: Formation of mitochondrial permeability transition pore which leads to loss of membrane potential, failure of phosphorylation and ATP depletion and then necrosis.
• Release of cytochrome c into the cytosol that activate apoptosis (death).
Failure of oxidative phosphorylation leads to
ATP depletion and formation of reactive
oxygen species(ROS).


• Depleting extracellular Ca protects the cell from injury and delays it.
• Cytosolic Ca concentration is very low and is present intracellularly in mitochondria and ER.
• Injury will lead to increase cytosolic Ca.
• Consequences of Ca increase: opening of mitochondrial permeability transition pore, and activation of a number of enzymes (phospholipases, proteases, endonucleases & ATPases)
• Induction of apoptosis by direct activation of caspases and increasing mitochondrial permeability
Influx of calcium and loss of calcium homeostasis


• It is important in chemical and radiation injuries, ischemia-reperfusion injury, cellular aging and microbial killing by phagocytosis.
• Free radicals: chemical species that have a single unpaired electron in the outer orbital.
• Unstable atoms, react with inorganic and organic chemicals (proteins, lipids, carbohyd.)
• Initiate autocatalytic reactions..... Creation of more radicals (propagation).
Accumulation of oxygen derived free radicals
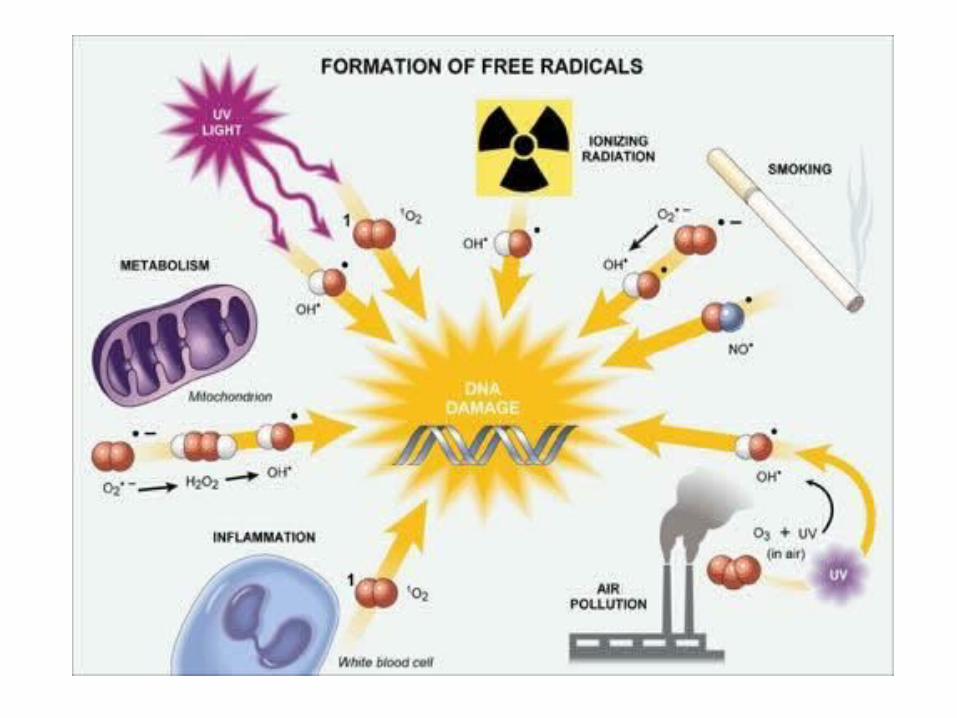
• One of the oxygen derived free radicals.
• Produced normally in small amounts and removed by defence mechanisms.
• Once the ROS amount increases this will lead to what so called oxidative stress.
• Oxidative stress : cell injury, cancer, aging and some degenerative diseases like Alzheimer. Also ROS are produced by leukocytes and macrophages in inflammation.
Reactive oxygen species (ROS)
• Decay spontaneously.• Antioxidants: Vitamin E and A, ascorbic acid
and glutathione in the cytosol.• Binding proteins.• Enzymes: Catalase-----H2O2 ----- O2 and H2O,
Superoxide dismutase-(SOD)----- superoxide anion ----H2O2, Glutathione peroxidase---- H2O2 ---H2O or OH------ H2O. Reduced Glutathione level is important in cell safety.
Removal of free radicals
Pathological applications of free radicals
• Lipid peroxidation in membranes. Oxidative damage of the double bonds in the polyunsaturated fatty acids resulting in formation of peroxides which are unstable and lead to membrane damage.
• Oxidative modification of proteins. Damage the active sites on enzymes, change the structures of proteins and enhance proteosomal degradation of unfolded proteins.
• Lesions in DNA. Single and double strand breaks in DNA. Oxidative DNA damage has been implicated in cell aging and in malignant transformation of cells.
• Radicals are involved in both necrosis and apoptosis.
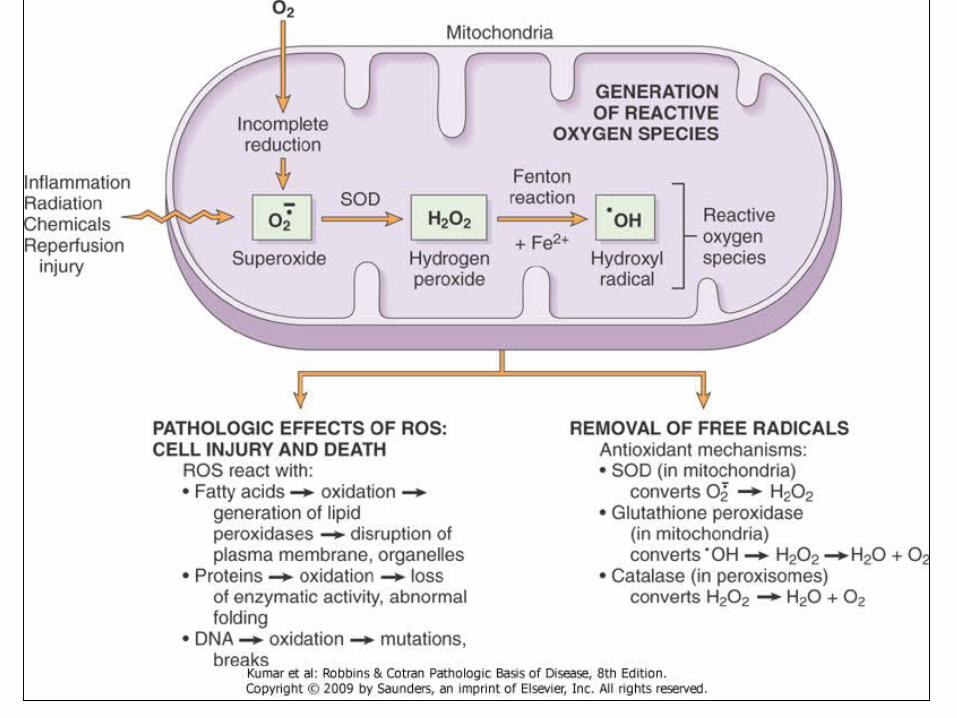
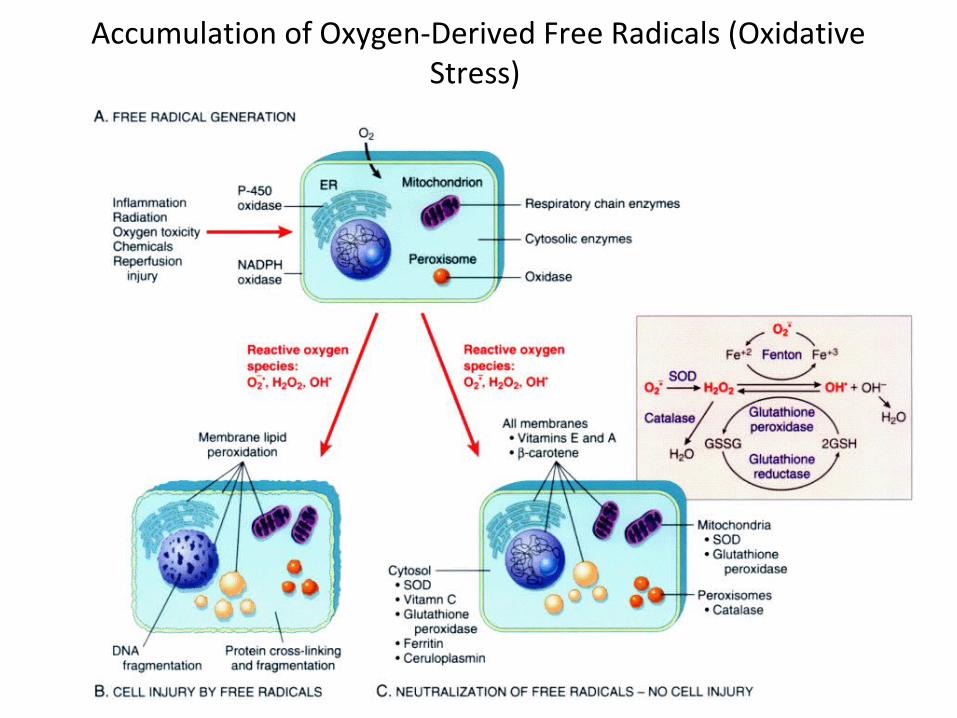
Accumulation of Oxygen-Derived Free Radicals (Oxidative Stress)
Patterns of Acute Cell Injury
• Apoptosis (a falling away from)Apoptosis is programmed cell death.
It is a pathway of cell death that is induced by a tightly regulated intracellular program in which cells destined to die activate their own enzymes to degrade their own nuclear DNA, nuclear proteins and cytoplasmic proteins.
The cell's plasma membrane remains intact, but its structure is altered in such a way that the apoptotic cell sends signal to macrophages to phagocytose it.
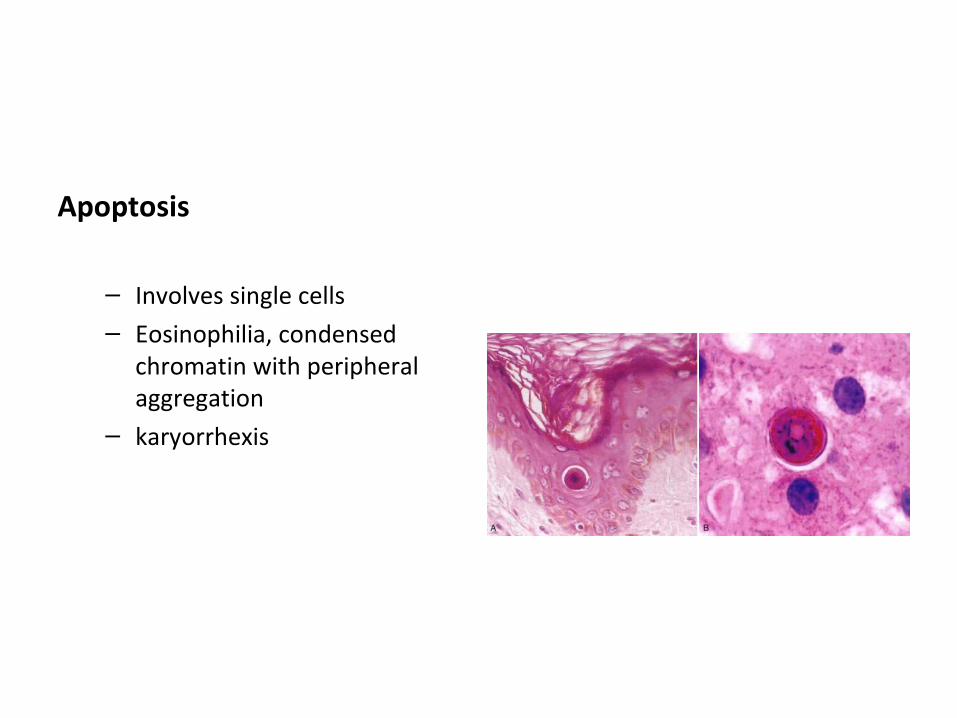
Apoptosis
– Involves single cells– Eosinophilia, condensed
chromatin with peripheral aggregation
– karyorrhexis
Regulation of apoptosis
• It is mediated by a number of genes and their products :
• - bcl-2 gene inhibits apoptosis• - bax genes facilitates apoptosis• - p53 facilitates apoptosis by inhibiting bcl2
and promoting bax genes.
Two types of cell death
Necrosis• Large No. of cells
• Invariably (always ) pathologic
• Disrupted Plasma membrane
• Inflammation
Apoptosis• Single cells or small clusters
• Often physiologic; may be pathologic
• Intact Plasma membrane
• No inflammation , • phagocytes to eleminate it

The Cell and the Environment
StimuliStimuli
Cell AdaptationAdaptation
Cell Injury
ReversibleIrreversible (cell death)
apoptosis necrosis
Atrophy HypertrophyHyperplasiametaplasia
Cellular Accumulations
Intracellular Accumulations
– Endogenous• normal substance produced at normal or increased
rate/rate of metabolism inadequate for removal (fatty liver)• normal or abnormal substance cannot be metabolized
(storage diseases)
– Exogenous– cell cannot degrade substance (carbon)
Intracellular Accumulations
• Fatty Change (Steatosis)
• Any abnormal accumulation of triglycerides within parenchymal cells.
• It is most often seen in the liver, since this is the major organ involved in fat metabolism, but it may also occur in heart, skeletal muscle, kidney, and other organs.
• Alcohol abuse and diabetes associated with obesity are the most common causes of fatty change in the liver (fatty liver) in industrialized nations.
Intracellular Accumulations
• Fatty Change (Steatosis)– Liver• increased weight, yellow color
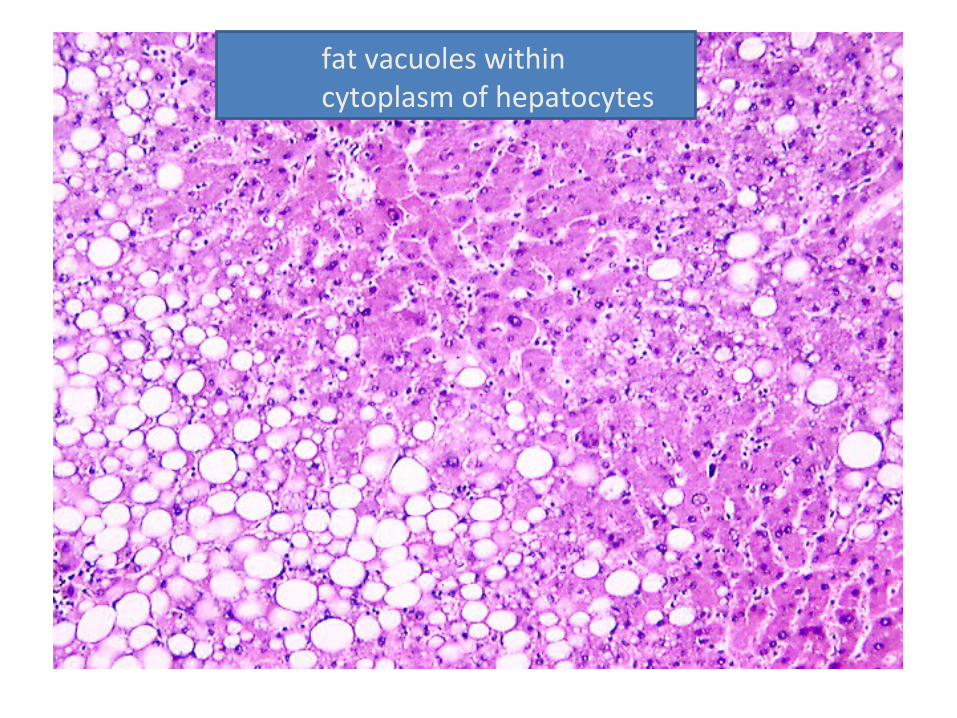
fat vacuoles within cytoplasm of hepatocytes
Intracellular Accumulations
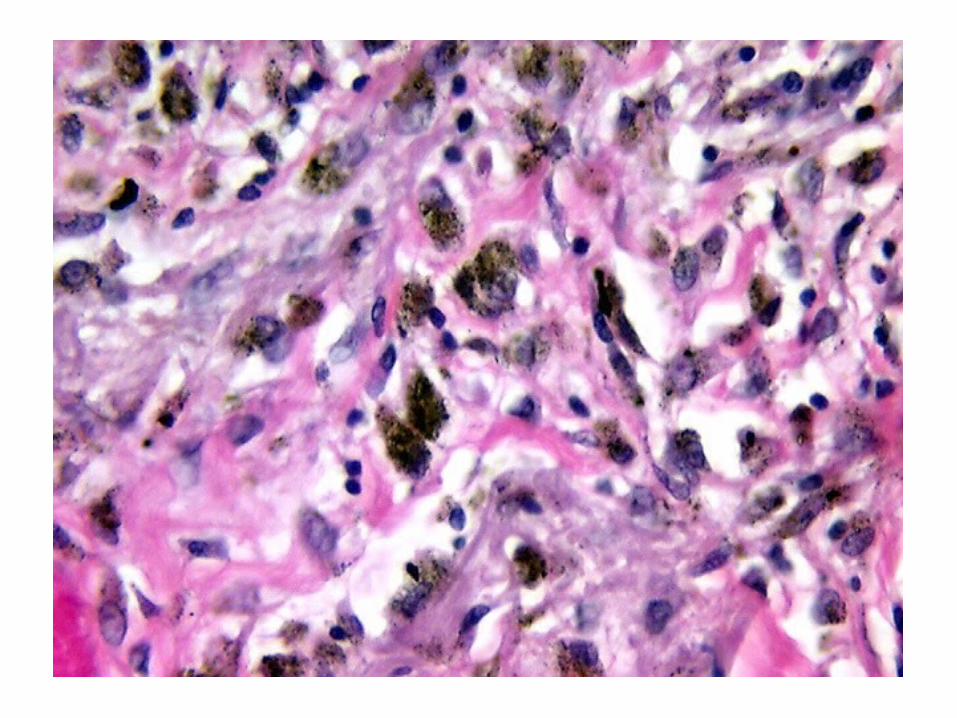
• Exogenous Pigments
– Carbon (anthracosis)• When inhaled, it is phagocytosed by alveolar
macrophages and transported by lymphatics to lymph nodes• mild accumulations usually are of no consequence--
heavy accumulations may induce a fibroblastic response
Intracellular Accumulations
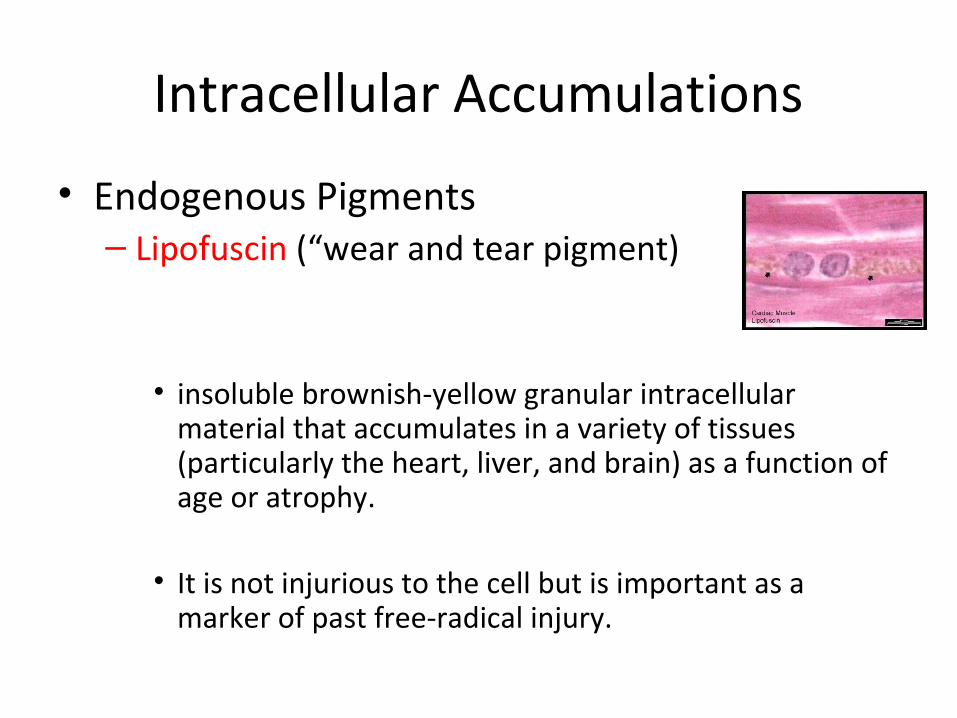
• Endogenous Pigments– Lipofuscin (“wear and tear pigment)
• insoluble brownish-yellow granular intracellular material that accumulates in a variety of tissues (particularly the heart, liver, and brain) as a function of age or atrophy.
• It is not injurious to the cell but is important as a marker of past free-radical injury.
Intracellular Accumulations
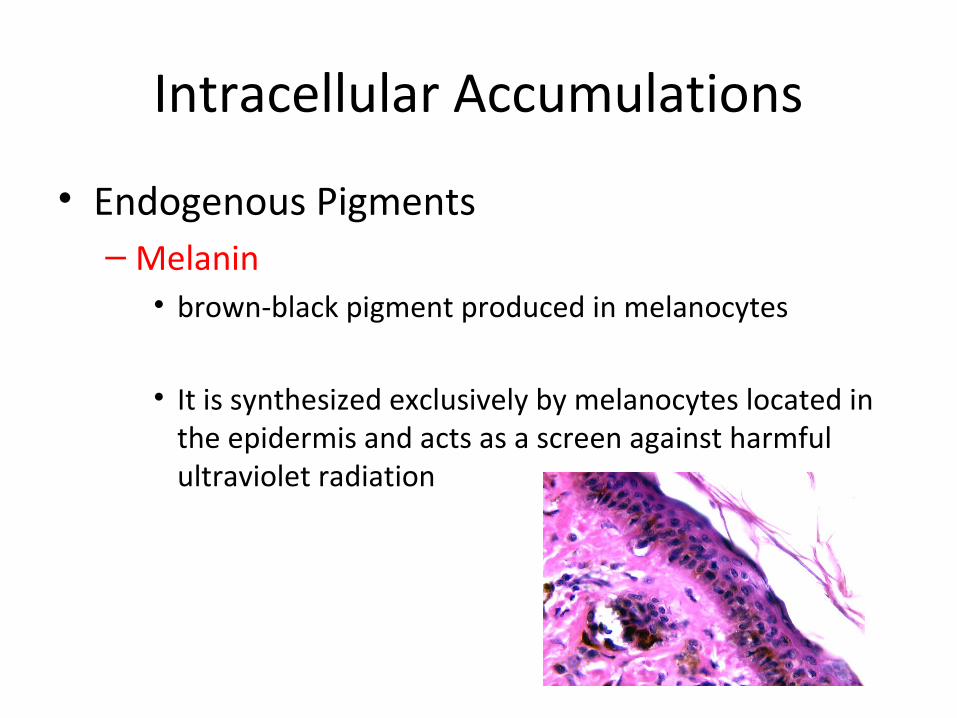
• Endogenous Pigments– Melanin• brown-black pigment produced in melanocytes
• It is synthesized exclusively by melanocytes located in the epidermis and acts as a screen against harmful ultraviolet radiation
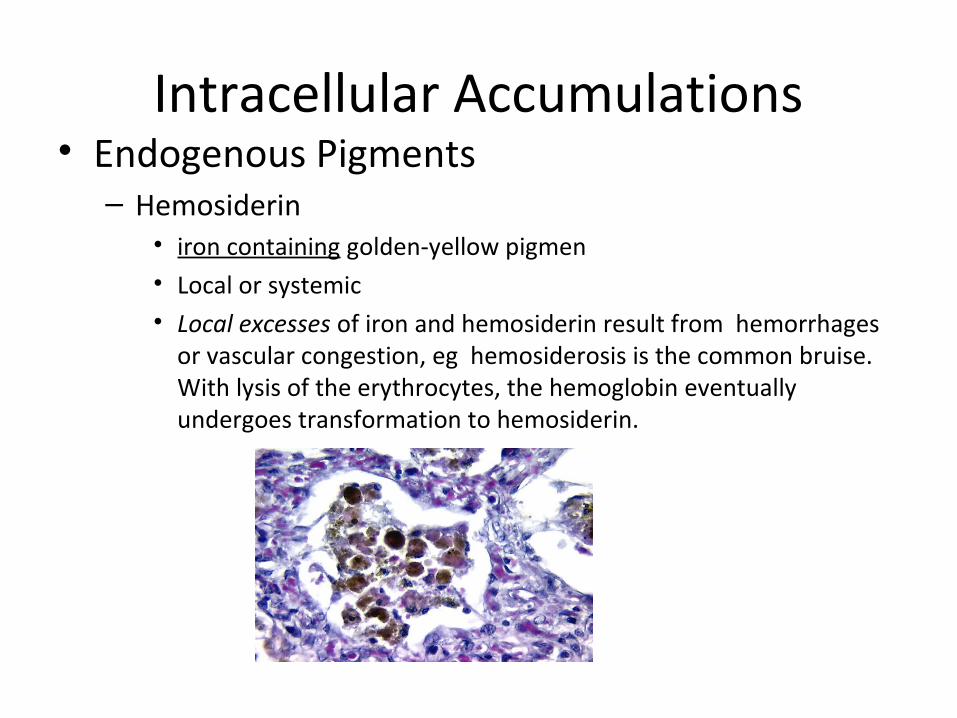
Intracellular Accumulations• Endogenous Pigments– Hemosiderin
• iron containing golden-yellow pigmen• Local or systemic• Local excesses of iron and hemosiderin result from hemorrhages
or vascular congestion, eg hemosiderosis is the common bruise. With lysis of the erythrocytes, the hemoglobin eventually undergoes transformation to hemosiderin.
hemosiderin• hemosiderosis • systemic overload of iron, hemosiderin is deposited in many organs and tissues [ liver, bone
marrow, spleen, and lymph nodes • occurs in
1. increased absorption of dietary iron,
2. impaired utilization of iron,
3. hemolytic anemias,
4. transfusions
• hemochromatosis • hereditary more extensive accumulations of iron with tissue injury including liver fibrosis,
heart failure, and diabetes mellitus.
PATHOLOGIC CALCIFICATION
• dystrophic calcification • deposition occurs in dead or dying tissues, • normal serum levels of calcium.
• metastatic calcification • deposition in normal tissues• almost always reflects some derangement in calcium
metabolism (hypercalcemia).