Embed Size (px)
Citation preview

Antonio Pio MasciotraCampobasso – Molise – Italy
Website
www.masciotra.net
YouTube Channel
https://www.youtube.com/channel/UCgCj21nKGAhR997Ia3-QegQ
Shear Wave Elastography and more in a clinical case of Multiple Myeloma

Clinical case
• Male 62 years old• Asymptomatic IgG/K chains gammopathy since 3 years• Then evolution to multiple myeloma stage DS IIIA with multiple bone lesions• The images of initial studies are showed in the following slides










Clinical case
• Male 62 years old• Asymptomatic IgG/K gammopathy since 3 years• Then evolution to multiple myeloma stage DS IIIA with multiple bone lesions• The patient has been treated with only the first part of the planned therapy which consists in :
4 cycles of induction with Bortezomib-CFA-DexamethasoneMobilization of hemopoietic stem cells with CFA at intermediate doses then increasedAutologous transplant of hemopoietic stem cells or 4 more cycles of CT with Bortezomib-Melphalan-PrednisoneAt the end of the induction phase manteinance phase with Lenalidomide (eventually starting after 2 cycles of
Bortezomib-Lenalidomide-Dexamethasone)

Before therapy
After 4 cycles of induction therapy

Before therapy
After 4 cycles of induction therapy

Before therapy
After 4 cycles of induction therapy

Before therapy
After 4 cycles of induction therapy
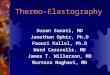
Multiple Myeloma Mean Stiff.kPa
Min. Stiff.kPa
Max. Stiff.kPa
Stand. Dev.kPa
Ratio Rib vs Muscle
Rib before therapy 22-113 10-90 30-126 4-21 0,9-1,6
Rib after 4 cycles 2-47 20-34 5-108 1-10 0,2-1,1
Muscle before therapy 107-119 73-98 30-168 7-20 0,9-1,6
Muscle after 4 cycles 32-108 3-120 5-69 1-10 0,2-1,1

Clinical case
• Male 62 years old• Asymptomatic IgG/K gammopathy since 3 years• Then evolution to multiple myeloma stage DS IIIA with multiple bone lesions• The patient has completed the planned therapy which consisted in :
4 cycles of induction with Bortezomib-CFA-DexamethasoneMobilization of hemopoietic stem cells with CFA at intermediate doses then increasedAutologous transplant of hemopoietic stem cells or 4 more cycles of CT with Bortezomib-Melphalan-PrednisoneAt the end of the induction phase manteinance phase with Lenalidomide (eventually starting after 2 cycles of
Bortezomib-Lenalidomide-Dexamethasone)
The induction treatment was successfull and the final PET showed complete remission
While in the mainteinance phase of the planned treatment the patient showed a painful enlargment of the right testis which was considered inflammatory and then antibiotic therapy was started.
Images are shown of the initial and 2 following exams At this point another PET showed no active disease in the skeleton, while high metabolic activity was seen in the
right testis

8/11/2014
20/11/2014
Ceftriaxone 1 g. i.m.
daily

8/11/2014
20/11/2014
Ceftriaxone 1 g. i.m.
daily

8/11/2014
20/11/2014
Ceftriaxone 1 g. i.m.
daily

8/11/2014 20/11/2014 10/12/2014

8/11/2014 20/11/2014 10/12/2014

8/11/2014 20/11/2014 10/12/2014

10/12/2014

10/12/2014

10/12/2014

10/12/2014

10/12/2014

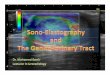
Feature (kPa) 08/11/2014 10/12/2014
Mean stiffness 18.9 – 56.7 25.5 – 86.8
Maximum stiffness 47.7 - 68.8 32.4 – 104.5
Minimum stiffness 3.2 – 41.2 18.4 - 55.5
Standard Deviation 5.2 – 14.0 2.5 - 11.6



Plasmacytoma of the Testis in a Patient With Previous Multiple Myeloma: Is the Testis a Sanctuary Site?
Radical orchiectomy was performed.
Macroscopic examination of the specimen showed that the testis was almost in full occupied by tanned white areas often with intact
tunica albuginea.
Histopathology demonstrated diffuse infiltration of the interstitial tissue by abnormal plasma cells (immunoblasts) with a proliferation
index >50% (as expressed by MiB1/Ki67) .
The seminiferous tubules were very scant, but retained their architecture with nil spermatogenesis (effect of chemiotherapy).
Immunohistochemistry stained positive for plasma cell markers (IgG, CD56, CD 138, Kappa chains and MuM1).

In this slide and in following slides are shown the correlations of US (B dimensional, color/powerdoppler
and SWE) images and histopathology images (so called ‘Rad/Path correlation)


HematoxylinEosin
KAPPAChains

Is the Testis a Sanctuary Site?
In this case testicular relapse was the first and only sign of disease recurrence.
Multiple myeloma involvement of the testicle is a rare occurrence.
The overall incidence of extramedullary lesions in myeloma found at necropsy ranges from 10% to 70%,
but the incidence of clinical testicular plasmacytoma is less than 0.1% of all primary and secondary tumors
of the testis.
The prognosis of patients with extramedullary manifestations of myeloma in earlier reports was poor.
Postoperative survival ranged from a few weeks to 4 years.
It is well known that, as a result of the testicular blood barrier (see the following slide for its description) ,
the testes can serve as a sanctuary site for hematologic malignancies.
In acute lymphoblastic leukemia, testicular relapse is reported in up to 17% of patients after complete
remission, being male sex a negative prognostic factor for treatment outcome.
Multiple myeloma can infiltrate any organ or tissue by mimicking different pathologic entities (like in this
case with clinical presentation very similar to orchiepididymitis).
In conclusion the testicles may serve as a sanctuary site in multiple myeloma and
the knowledge of this possible evenience needs to be taken in proper account in
the initial workup and in the follow up of such patients, both performing the
thorough physical examination and adding US of the scrotum.

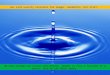
"Germinal epithelium testicle" by User:Uwe Gille - Own work. Licensed under CC BY 2.5 via Wikimedia Commons -http://commons.wikimedia.org/wiki/File:Germinal_epithelium_testicle.svg#/media/File:Germinal_epithelium_testicle.svg
1 basal lamina
2 spermatogonia
3 spermatocyte 1st order
4 spermatocyte 2nd order
5 spermatid
6 mature spermatid
7 Sertoli cell8 occlusive junctions
The blood–testes barrier can be damaged by trauma to the testes (including torsion or impact), by surgery or as a result
of vasectomy.
When the blood–testes barrier is breached, and sperm enters the bloodstream, the immune system mounts an autoimmune response
against the sperm.
The anti-sperm antibodies generated by the immune system can bind to various antigenic sites on the surface of the sperm. If they
bind to the head, the sperm may be less able to fertilize an egg, and, if they bind to the tail, the motility of the sperm can be reduced
The presence of the SCB allows Sertoli cells to control the adluminal environment in which germ cells (spermatocytes, spermatids
and sperm) develop by influencing the chemical composition of the luminal fluid.
The barrier also prevents passage of cytotoxic agents (bodies or substances that are toxic to cells) into the seminiferous tubules.
The blood–testis barrier is a physical barrier between the blood
vessels and the seminiferous tubules of the animal testes.
The name "blood-testis barrier" is misleading in that it is not a blood-
organ barrier in a strict sense, but is formed between Sertoli cells of
the seminiferous tubule and as such isolates the further developed
stages of germ cells from the blood.
A more correct term is the "Sertoli cell barrier" (SCB).
The barrier is formed by tight junctions, adherens junctions and gap
junctions between the Sertoli cells, which are sustentacular
cells(supporting cells) of the seminiferous tubules, and divides the
seminiferous tubule in a basal compartment (outer side of the tubule,
in contact with blood and lymph) and an adluminal compartment (inner
side of the tubule, isolated from blood and lymph).

CONCLUSIONS
In imaging it's like in every day's life.If you need to know the details of an object you can rely on the information given by different tools :
1) your eyes tell you its morphology and the colors2) your hand tells you its consistence, the characteristics of its surface and very approximately the temperature,
weight and lenght3) your tongue tells you its taste, but also its consistence, the characteristics of its
surface and its temperature4) your nose tells you its smell.
Likewise it is in imaging. Each modality and technique give us different kind of information.
Shear Wave Elastography is capable to show the mechanical properties of the normal parenchyma compared to the different kind of tumors of the testis (plasmacytoma. seminoma and yolk sac tumor) as showed in the former slides.

• Bidimensional • 3D
On the SWE image are displayed different information on elasticity
(or stiffness) quantification for each ROI selected in the colored box:
• Mean value in kPa or m/s (mean elasticity or stiffness)
• Minimum value in kPa or m/s (softest)
• Maximum value in kPa or m/s (stiffest)
• Standard deviation in kPa or m/s (its an index of more or less homogeneity)
• Elasticity ratio (if are selected 2 ROIs) < or > than 1
• Diameter of the ROI selected in mm

Shear Wave Elastography is capable to show the mechanical properties of the normal parenchyma ofthe testis (2 to 6 kPa) compared to different kind of tumors (Seminoma 61 kPa - Yolk sac tumor 41 kPa– Plasmacytoma 86 kPa) giving very useful information not only in the initial diagnostic approach,but also in the serial exams targeting the temporal evolution of the condition examined, like in this casein which the first exam did seem to suggest epidydimitis (20-56 kPa).The failure of the antibiotic treatment expressed also by the increasing stiffness (26-87 kPa) thensuggests that underlying condition was not an acute inflammation, but the relapse of the plasmacytoma(confirmed at the operation).

Likewise Shear Wave Elastography in this clinical case gives importantinformation about the response of the diseases to the therapy, here evenin the ribs of multiple myeloma after 4 cycles pf induction chemiotherapy.Then it can be considered like the thermometer we normally use to checkif the antibiotic we are giving for an infection is effective or not.

Furthermore Shear Wave Elastography gives very valuable information on the differencesin stiffness both between primitive cancers and its metastases in the same patient and in the sameanatomical sites (like bone malignant conditions primary and metastatic) in different kind of tumors .
Primitive colon cancer 15 kPa





CONCLUSIONS
Shear Wave Elastography adds valuable information to the study of tissues and organs, potentially
resulting in
“a virtual biopsy” .
This final aim will be achieved when further improvement of Shear Wave Elastography technology
(the only actually capable to quantify elasticity or stiffness) will give us the right consistency of the
quantitative measurements of tissue elasticity that up todate is still lacking.
Hence the RSNA initiative of ‘Quantitative Imaging Biomarkers Alliance’ applied to
Sono-Elastography too.
This means that if the intrinsic elasticity of the testis is 2 kPa all the measurements have to give this
value, not depending on the probe’s frequency or on other variables.
When this requirement will be accomplished we’ll can really establish the cutoff value between
normal and abnormal tissues both in focal and in diffuse diseases.
Therefore we’ll can rely on it at same extent we actually rely on the use a thermometer to check
the behavior of the fever during an infection (if it’s responding to the treatment).
Then let’s go on!
Lessons need to be drawn from great men of the past who had
the vision to preparing for the future through imagination.


Shear Wave Elastography and more in a clinical case of Multiple Myeloma