Embed Size (px)
Citation preview
KellyAnn Light-McGroary, MD, FACC Cardiomyopathy Program and Palliative Med Program
University of Iowa Hospitals and Clinics ACC 2015
San Diego, Sunday, March 15th
I have no disclosures that are specifically relevant to this presentation.
Disclosures
To review the goals of mechanical circulatory
support
To discuss how patients and providers approach the decision
To outline the essential elements of preparedness planning/palliative consult in ACT and the impact on decision making.
Objectives
LVAD Candidate Pool
250,000-500,000 ESHF pts in terminal phase of disease (ACC Stage D = refractory to MM)
Mean survival 3.4 months
Inotrope dependent = up to 94% 1 yr mortality
80,000-150,000 pts/yr could benefit from HT
HT performed approximately 2,200/yr
LVAD as DT is available alternate
Lietz et al; J Card Surg 2010;25:462-471
Goals of MCS
Improve survival
Reduce hospitalizations
Improve quality of life
Improve likelihood of successful transplantation
What the medical team sees when deciding about MCS:
Medical team considerations:
Age
Co-morbid conditions
Anticipated survival
Risk scores
Bleeding risks
Social support
Right ventricle, right ventricle, right ventricle!
What is the right timing?
“Too Early” vs. “Too Late”
Sick enough to recognize the benefit
Well enough to minimize risks/burdens
What the patient often hears when deciding about MCS:
Patient approach:
Receive MCS and live
Decline MCS and die
Ideally, a patient would understand the exchange of end-stage HF problems for bleeding risks, infections, and/or stroke
Song, ISHLT 2012
Swetz, et al, Cardiology Research & Practice 2012
Preparedness Planning for Advanced Cardiac Therapies
How do we bring these two partners together?
Step 1: Goals of Care and Expectations
What are they hoping for, where are their values?
Can MCS or transplant actually help the achieve those goals?
GOC set the stage for the entire discussion; it is the foundation for many challenging issues.
Understanding goals of care can help manage expectations, ie “realistic hope”
Essential Elements of Preparedness Planning
Step 2: Advanced Care Planning and Identification
of Surrogate Decision Maker
What have they already done?
Consider Honoring Your Wishes, Five Wishes, etc (robust advanced care plans)
Include surrogate in discussions including responsibilities and how to approach this role
Normalize this as part of routine health care
Essential Elements of Preparedness Planning
Step 3: Preparedness Discussion for Patient and
Family
Discuss what to expect during the perioperative period including possible challenges and expectations for patients and providers.
Discuss long term benefits and complications including:
Infection
Bleeding issues
Ongoing HF/RV failure
Renal failure/dialysis
Discussion around device deactivation
Essential Elements of Preparedness Planning
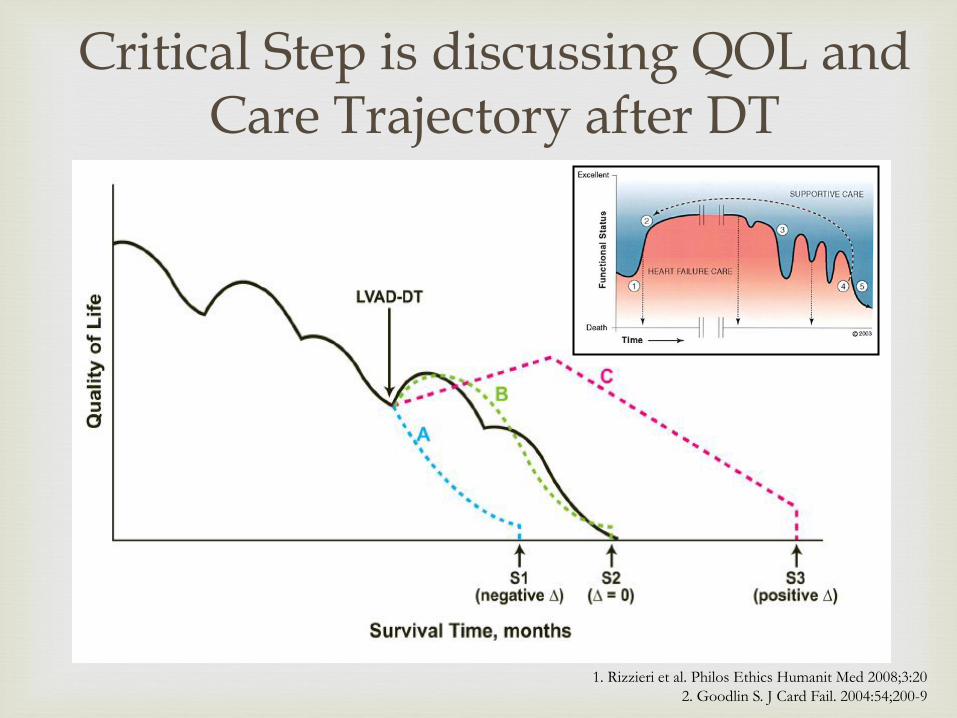
1. Rizzieri et al. Philos Ethics Humanit Med 2008;3:20
2. Goodlin S. J Card Fail. 2004:54;200-9
Critical Step is discussing QOL and Care Trajectory after DT
Long term care and QOL considerations in DT patients
Caregiver misperceptions
Frequent clinic visits
Insurance/financial
Geographical limitations due to power source
Limited local resources
− Local medical community likely unprepared to care for DT patients
Caregiver burnout
EOL issues
− Inevitable
− Ethical aspects of withdrawing DT support
− Palliative care
These considerations emphasize
the need for a “preparedness
plan.”
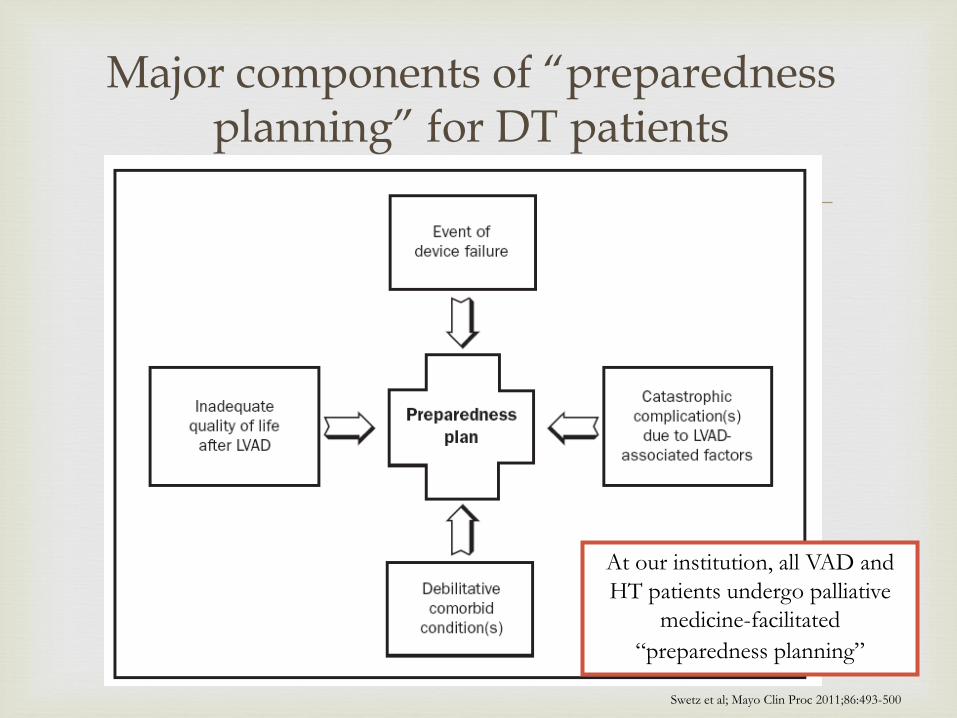
At our institution, all VAD and
HT patients undergo palliative
medicine-facilitated
“preparedness planning”
Major components of “preparedness planning” for DT patients
Swetz et al; Mayo Clin Proc 2011;86:493-500
What does palliative medicine specifically offer to VAD patients?
Medical decision-making
Establish goals of care
Coordinate care
Manage symptoms
Psychosocial and spiritual support
Assure comfort, QOL and dignity
Prognosis
Ethics
Technical assistance
Active care of dying patients and loved ones
Bereavement support
Swetz et al; Mayo Clin Proc 2011;86:493-500
CP is a 64 y/o man with a history of an ischemic
cardiomyopathy/prior CABG, Stage D, NYHA Class IV.
In September presented in progressive biventricular failure.
Inotrope dependent by October but not thriving
Implanted in early November as DT HM2 VAD after palliative/preparedness planning consult.
Goals: live longer but most importantly be able to fish, go to grandson’s sporting events and stay out of hospital.
Case Presentation
After implant developed mesenteric ischemia felt to be
due to embolic event from VAD .
By December developed recurrent GI bleeds that were aggressive and difficult to control.
Multiple unsuccessful GI/IR procedures.
Multiple transfusions and hemodynamic instability.
Off anticoagulation he had stroke and VAD thrombosis. Full resolution of stroke with heparin.
Ongoing low level hemolysis.
Has been an inpatient 80% of the last 3-4 months.
Reactivated on the list as a 1A 2 weeks ago and transplanted 4 days ago
Case Presentation
What have his thoughts been about VAD?
Has it met expectations?
Did he feel prepared?
How have his symptoms been managed?
What is the impact on his family?
How is he suffering?
Case Presentation
Goals of Care are critical as the foundation of
deciding appropriateness of VAD and timing.
Ensuring that patients and surrogates understand ahead of time the possible decision points helps to create a road map for even the unexpected.
Managing expectations for the team and the patient/family can be successful through structured preparedness planning.
Summary