Embed Size (px)
Citation preview
Pulmonary Aspergillosis: Aspergilloma In Focus
Respiratory Unit Dept of MedicineOAUTHC Ile-Ife

Outline
• Introduction• The organism/Ecology• Epidemiology• Disease Entities• Pathophysiology• Clinical features• Differential Diagnosis• Investigation • Treatment• Prognosis• References
Introduction
• Aspergillosis refers to illness due to allergy, airway or lung invasion, cutaneous infection, or extrapulmonary dissemination caused by pathogenic species of Aspergillus
• Aspergillus species are ubiquitous molds found in organic matter/decaying vegetation
• Tissue invasion is uncommon and occurs most frequently in the setting of immunosuppression
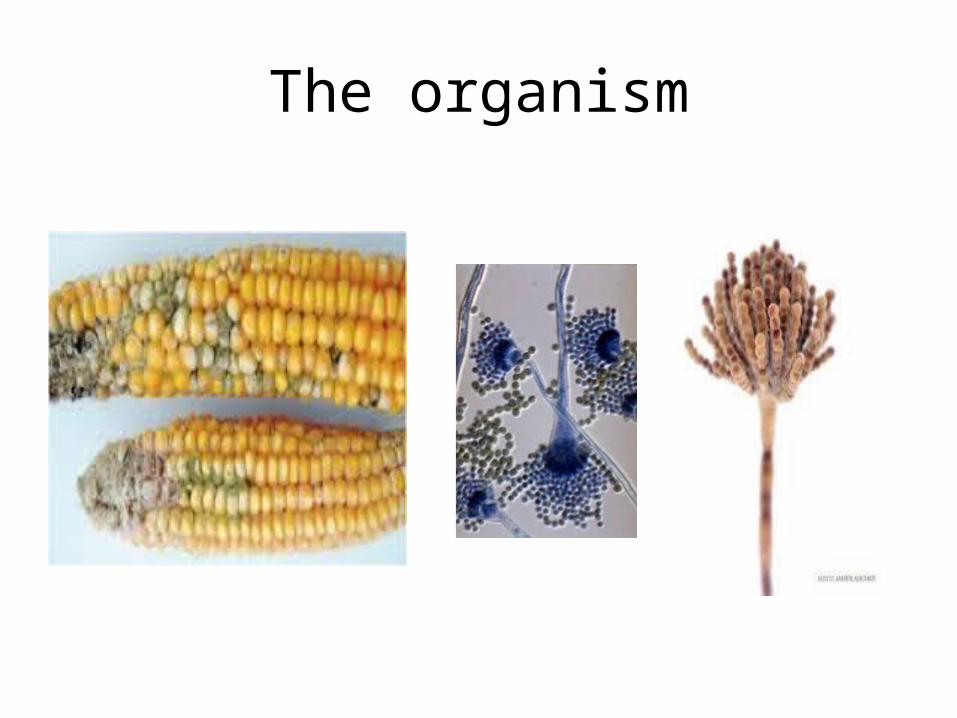
The causative organism
• More than 100 species have been identified, majority of human illness is caused by
- A. fumigatus - A. niger and, less frequently, by - A. flavus -A. clavatus and -A. nidulans. - A. terreus• Transmission is via inhalation of fugal spores
The Organisms and Ecology• Hyaline (non-pigmented),narrow, septate,
branching mold • Produces vast numbers of conidia (spores) on
stalks above the surface of mycelial growth.• Hyphae are histologically distinct from other
fungi in that the hyphae have frequent septae, which branch at 45° angles.
• The hyphae are best visualized in tissue with silver stains.
The organism
Epidemiology• Invasive Aspergillosis now uncommon in US
with the advent HAART - US National base reveals incidence 3.5 cases/1000
persons - incidence 0.02-013% per annum in HIV patients
and 0.43% in transplant recipient in France• Surveys & ABPA registry, - 0.25-0.8% of people with asthma - 7% of patients with Cystic fibrosis
• Higher incidence in steroid-dependent asthma 7-10% and bronchiectasis
Epidemiology
• Study of 77 patients in UMTHa
• 20-30yrs F>M; 30-40yrs M>F
• CNPA is rare found at autopsy
a- Journal of Medicine and Medical Sciences Vol. 4(6) pp. 237-240, June, 2013
Epidemiology
• Frequency of invasive aspergillosis parallells disease states and treatments: neutropenia and immunosuppression.
• Occurs in – 5-13% of recipients of bone marrow transplants – 5-25% of patients with heart or lung transplants – 10-20% of patients receiving intensive chemotherapy for
leukemia.• chronic cavitary lung disease- not rare• In one survey of patients with chronic CLD due to
tuberculosis, 17% developed aspergilloma
Risk factors
• Immunocompromised states - Coticosteroid use - Advanced HIV infection - Neutropenia - Bone marrow /solid organ transplant• Chronic granulomatous disease: TB,
Sarcoidosis• Cystic Fibrosis
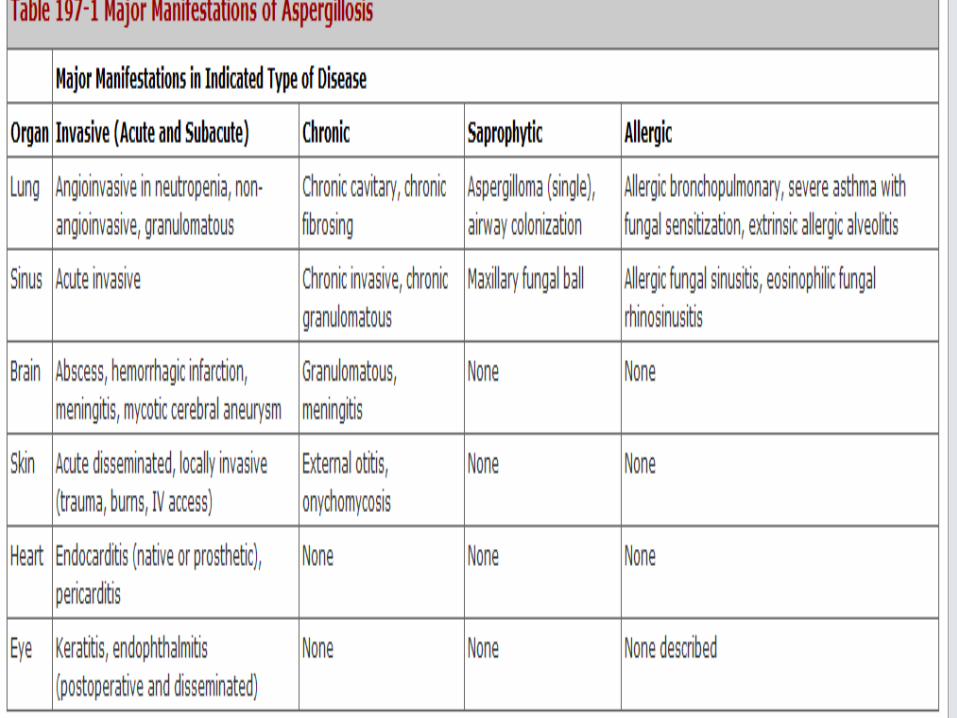
Pulmonary aspergillosis
Primarily affects the lungs, causing the following main syndromes:
• Allergic bronchopulmonary aspergillosis (ABPA)• Invasive aspergillosis• Chronic necrotizing Aspergillus pneumonia (or
chronic necrotizing pulmonary aspergillosis [CNPA])
• Aspergilloma
In patients who are severely immunocompromised,
Aspergillus may hematogenously disseminate beyond
the lung, potentially causing ;
• Endophthalmitis,
• Endocarditis, and
• Abscesses in the myocardium, kidney, liver, spleen,
soft tissue, and bone

Transmission• Via inhalation and daily exposure abound• Daily exposures vary from a few to many millions of
conidia; • High numbers of conidia are encountered in hay
barns and other very dusty environment• Required size of the infecting inoculum is uncertain • Intense exposures (e.g., during construction work)
are required to cause disease in healthy individuals.
Transmission2
• The incubation period of invasive aspergillosis after exposure is highly variable 2 to 90 days.
• Outbreaks usually are directly related to a contaminated air source in the hospital
Pathophysiology
• A. fumigatus is the most common cause of infection in humans.
• Possess ability to grow at normal human body temperature
• Most other sp cannot
Pathophysiology
• Human host defense against the inhaled spores begins with the mucous layer and the ciliary action in the respiratory tract.
• Macrophages and neutrophils encompass, engulf, and eradicate the fungus.
• However, many species of Aspergillus produce toxic metabolites that inhibit macrophage and neutrophil phagocytosis.
• Corticosteroids also impair macrophage and neutrophil function.
Pathophysiology
• Underlying immunosuppression contributes directly to neutrophil dysfunction or decreased numbers of neutrophils.
• Vascular invasion is common in immunosuppressed states
• May result in infarction, hemorrhage, and necrosis of lung tissue.
• Granuloma formation and alveolar consolidation may occur in CNPA
Pathophysiology
• Colonization of previously formed cavities in the lung
• Inhaled Aspergillus spores may also colonize the mucus within the bronchi,
• As obtained in moderately severe asthma with thick and tenacious mucus
• Aspergillus spores may invade adjacent lung tissues and produce a gradually progressive and destructive process in lung containing centrilobular emphysema
invasive Semi-invasive
ABPA TRACHOEBRONCHITIS
RISK FACTORS
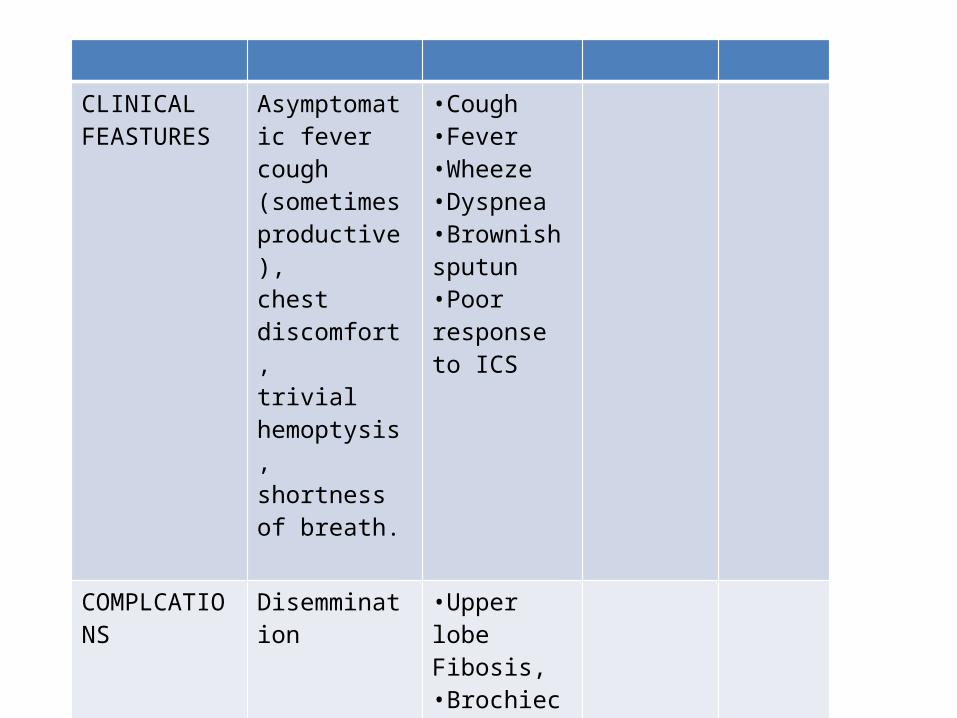
CLINICAL FEASTURES
Asymptomatic fevercough (sometimes productive),chest discomfort, trivial hemoptysis, shortness of breath.
•Cough•Fever•Wheeze•Dyspnea•Brownish sputun•Poor response to ICS
COMPLCATIONS Disemmination •Upper lobe Fibosis, •Brochiectasis
Disseminated Infections• The most lethal form of aspergillosis is disseminated or pyemic
aspergillosis. • the fungi will grow within the alveoli and invade adjacent vascular
structures, leading to occlusion of these vessels. • Necrosis follows occlusion of the vessels, leading to wedge-
shaped areas of infarction. • Metastatic abscesses in brain, lung, liver, heart, and other organs
are common. • Skin involvement gives rise to a characteristic lesion: an area of
central necrosis and a black eschar (ecthyma gangrenosum)• Occasionally, Aspergillus endocarditis may follow pyemic spread
or surgery
Aspergilloma
• Aspergilloma (fungal ball) occurs in up to 20% of residual chest cavities 2cm in diameter.
• Some fungal balls remain stable in a single cavity for many years, and 10% resolve spontaneously.
• They are often a feature of chronic pulmonary aspergillosis with its associated features
Aspergilloma2
• Vast majority of fungal balls are caused by A. fumigatus
• A. niger implicated in diabetic patients; aspergillomas due to
• A. niger can lead to oxalosis with renal dysfunction

Classification
• Pulmonary aspergilloma is classified as - simple - complex pulmonary aspergilloma (CPA), • based on the radiological aspect, which reveals the nature
and extent of the pulmonary impairment caused by the pre-existing disease.
• SPA : Well-localized lesion, thin-walled cavities, and little or no change in the adjacent lung tissue.
• CPA : disseminated lesions, thick walls, parenchymal sequelae resulting from the previous lung disease-in most cases TB
Clinical Features
• May manifest as an asymptomatic• Radiographic abnormality in a patient with
pre-existing cavitary lung disease due to sarcoidosis, TB, necrotizing pulmonary processes, CF, emphsematous bullae
• May occur in cystic areas resulting from prior Pneumocystis jiroveci pneumonia in patients with HIV disease
Clinical Features
• Hemoptysis is the major feature 40-60% (rarely, occasional exsanguinating hemorrhage)
• Less commonly, cough and fever. • wheezing, and mild fatigue
Clinical Features
• Aspergillomata can form in other body cavities.
• abscesses in the brain, usually in people who are immunocompromised.
• They can also form within the different sinuses in the face, within the kidneys and urinary system, the ear canal, and on the heart valves
Diseases Featutes
Bronchogenic ca Short durationWt loss, hoarseness of voiceHx of risk factorsct
bronchiectasis
Mitral stenosis
Acute lvf
Paragonomiasia
Allergic Bronchopulmonary Aspergillosis (ABPA)
• characterised by an exaggerated response of the immune system (a hypersensitivity response) to the fungus Aspergillus (most commonly A. fumigatus).
• Occurs most often in patients with asthma or cystic fibrosis 1 about 1% and 15% resp
• Occasional cases are reported in patients without either of these diseases
ABPA
• Patients develop a hypersensitivity response, both a type I response (atopic, with formation of IgE) and a type III hypersensitivity response (with formation of IgG).
• The reaction of IgE with Aspergillus antigens results in mast cell degranulation with bronchoconstriction and increased capillary permeability.
• Immune complexes (a type III reaction) and inflammatory cells deposited within the mucous membranes leading to necrosis and an eosinophilic infiltrate.
• Type 2 T helper cells secreting interleukin 4 and interleukin 5, and attraction of neutrophils by interleukin 8 are also involved
ABPA
• In spite of this pronounced immune reaction, the fungus is not cleared from the airways.
• Proteolytic enzymes are released by the immune cells, and toxins are released by the fungi.
• Together these result in bronchiectasis, most pronounced in the central parts of the airways.
• Repeated acute episodes left untreated can result in progressive pulmonary fibrosis that is often seen in the upper zones and can give rise to a similar radiological appearance to that produced by TB.
ABPA
• The otherwise-severe course of underlying asthma is punctuated by episodes of worsening, when thick mucus plugs become inspissated in bronchi, causing an inflammatory process distal to the obstruction.
• This propensity to cause bronchial obstruction gives rise to the characteristic radiographic pattern of the disease, the so-called finger-in-glove appearance, in which multiple adjacent bronchi are distended with the mucus plug

Clinical Features
• Episodes of bronchial obstruction with mucous plugs leading to – coughing fits, – breathlessness and – production of thick sputum casts, usually brown or
clear• Fever, unresponsive to antibacterial therapy
Clinical Features
• Hemoptysis. • Wheezing • People with asthma who have ABPA may have
poorly controlled disease and difficulty tapering off oral corticosteroids.
• ABPA may occur in conjunction with allergic fungal sinusitis
• Development of chronic fibrous changes, the restrictive lung function pattern is overlaid on top of the reactive airways disease

ABPA Sequallae
ABPA may be progressive, and the following 5 stages have been described• Acute disease• Remission• Exacerbation or recurrence• Corticosteroid-dependent asthma• End-stage fibrosis

Invasive Aspergillosis
• Invasive aspergillosis is divided into – Acute (<1mnth) – Subacute forms (1-3mnths)
• >80% of cases of invasive aspergillosis involve the lungs.
• The keys to early diagnosis in at-risk patients are– high index of suspicion, – screening for circulating antigen, and – urgent CT of the thorax.

Features
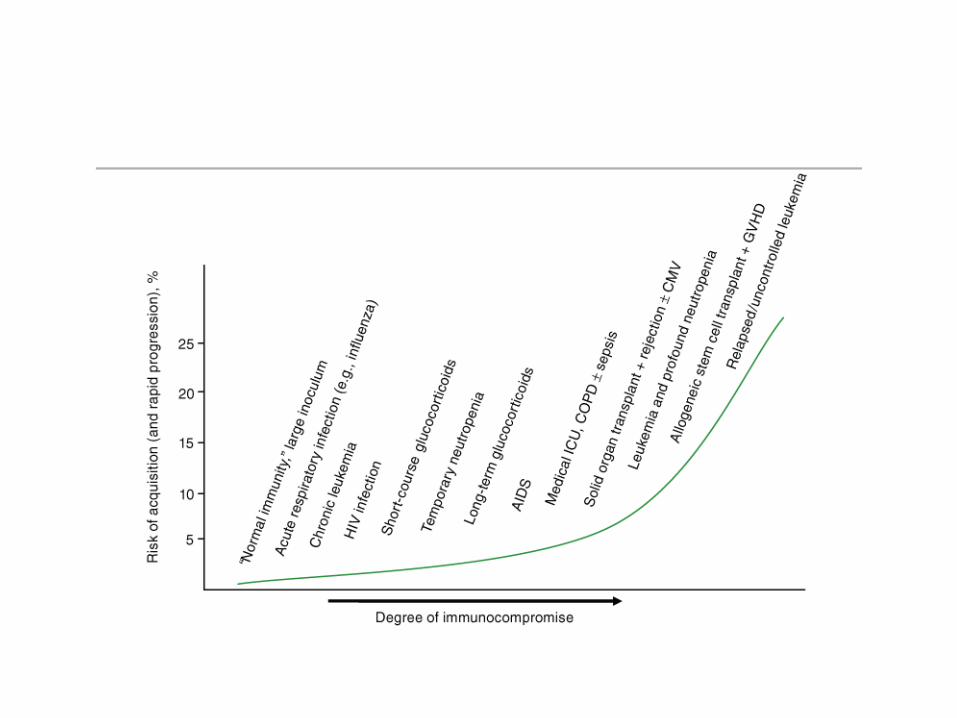
• Frequency and progression increase with greater degrees of immunocompromise
• Neutropenia and corticosteroid therapy are major risk factors
• increasingly observed in patients with COPD on long-term corticosteroid therapy
• Dissemination to other organs, particularly the central nervous system, may occur.
Clinical Features
• Asymptomatic commonly• fever• cough (sometimes productive),• nondescript chest discomfort, • trivial hemoptysis, • shortness of breath.• Although the fever often responds to
glucocorticoids, the disease invariably progresses
Chronic Pulmonary Aspergillosis (CPA)
• A.k.a semi-invasive aspergillosis,
• Can be divided into– chronic cavitary pulmonary aspergillosis – chronic necrotizing aspergillosis,
Features
• subacute pneumonia unresponsive to antibiotic therapy
• progresses and cavitates over weeks, months or years with expanding cavities
• have underlying disease, such as steroid-dependent COPD or alcoholism– And others - TB, atypical mycobacterial infection,
sarcoidosis and other granulomatous lung disease, ankylosing spondylitis, rheumatoid lung disease, pneumothorax, bullae, ILD or prior lung surgery
Clinical features
• Usually >3mnths• Fever, cough, night sweats, and weight loss• Hemoptysis • If untreated, typically progresses (sometimes
relatively rapidly) to unilateral or upper-lobe fibrosis.
• This end-stage entity is termed chronic fibrosing pulmonary aspergillosis.
References• Harrison’s Principles Of Int Med 18th ed• 1.Joshi JM. Hydatidothorax. Lung India 2011;28:315-6. Back to cited text no. 1 [PUBMED
] • 2.Biswas D, Dey A, Biswas S, Chakraborty M. It's easy to miss complicated hydatid cyst of
lung. Lung India 2010;27:164-6. Back to cited text no. 2 [PUBMED] • 3.Sarkar SK, Kumar V, Sharma SD, Bhatnagar M, Khandelwal PP. Crescent sign in
pulmonary hydatid cyst. Lung India 1988;6:155-6. Back to cited text no. 3 • 4.Flisser A. Larval cestodes. In: Collier L, Balows A, Sussman M, editors. Topley and
Wilson's microbiology and microbial infections. Parasitology. 9 th ed. Vol. 5. New York, NY: Oxford University Press; 1998. p. 539-60. Back to cited text no. 4
• 5.Ulkü R, Yilmaz HG, Onat S, Ozçelik C. Surgical treatment of pulmonary hydatid cysts: Report of 139 cases. Int Surg 2006;91:77-81. Back to cited text no. 5
• 6.Sharif A, Ansarin K, Rashidi F, Taghizadieh A. Bronchoscopic diagnosis and removal of a ruptured hydatid cyst. J Bronchology Interv Pulmonol 2011;18:362-4.
• Holding KJ et al Aspergillosis Among People Infected with Human Immunodeficiency Virus; Incidence And Survival, Adult and Adolescents Spectrum of HIV Disease Project Clin Infect Dis 2000;31:1253
![Aspergillosis - Youngstown State Universitypeople.ysu.edu/~crcooper01/Aspergillosis[1]- Katie Jacquie Qazi.pdf•People with Aspergillosis are in three distinct groups •Healthy immune](https://img.pdfslide.net/doc/110x75/5e3883b0e2f2970b7b1c24ad/aspergillosis-youngstown-state-crcooper01aspergillosis1-katie-jacquie-qazipdf.jpg)