Embed Size (px)
Citation preview

Dr. Onur GÖKSEL
Istanbul University, Istanbul Medical FacultyDepartment of Cardiovascular Surgery

Behçet’s disease is an inflammatory disorder characterized with recurrent oral and genital ulcers, uveitis, skin and vascular lesions and extends from Eastern Asia to the Mediterranean Basin along the ancient Silk Road

HULUSİ BEHÇET(1889-1948)

Behcet’s: EpidemiologyDisease prevalence and expression vary
geographically
Mediterranean Basin
Turkiye has the highest prevalence: 80 to 370 cases per 100,000 population.

Behcet’s: EpidemiologyPrevalence in Japan, Korea, China, Iran, and Saudi
Arabia ranges from 13.5 to 20 cases per 100,000The prevalence is much lower in Western countries.Prevalence of 0.33 per 100,000 in the United States.

Behcet’s: PathophysiologyThe underlying cause of Behcet's disease is unknown. As with other autoimmune diseases, the disorder may
represent aberrant immune activity triggered by exposure to an agent, perhaps infectious, in patients with a genetic predisposition to develop the disease.

Behcet’s: PathophysiologyThe prevalence of the HLA-B51 allele is high among
patients with Behçet's disease who are of Middle Eastern or Far Eastern ancestry (up to 81 percent of Asian patients have the allele)
Not among white patients who live in Western countries (13 percent).
Studies suggest a possible pathogenic role of certain bacterial/viral antigens that have cross-reactivity with human peptides.

Behcet’s: Pathophysiology
Endothelial activation in vasculo-Behcet's
Hyperfunction of neutrophils noted within active lesions
Recurrent lesions
Inflammatory obliteration of the vasa vasorum and consequent transmural necrosis may develop a pseudoanurysm or rupture an arterial wall.

Behcet’s: PathophysiologyMatrix metalloproteinase proteins (MMP) which play
an important role in tissue remodeling and destruction of extracellular matrix components are thought to have significant role in aneurysm formation.
MMP-9 & MMP-2 markers of vascular involvement (Pays et al)(Pays et al)
Surgery has been reported to yield poor results and a focal repair procedure often results in early to late complications

Clinical Manifestations: VascularThe involvement of large vessels may be observed in
1.8–39.4 % of patients with BD.
The vascular involvements of BD occur in the veins more frequently than the arteries.
Vascular involvement of BD is characterized by aneurysm and pseudoaneurysm formation in arteries and thrombotic occlusion in arteries and veins.

Hamza classification of vascular involvement in Behçet Dİsease
Type Vascular involvementI Venous thrombosisII Arterial thrombosisIII Arterial aneurysmIV Arterial thrombosis and aneurysmV Venous thrombosis and arterial lesion

ArterialOcclusive or aneurysmal lesionsThe most severe complication is
aneurysm formation and rupture. Abdominal aorta is the commonest site of
aneurysm and approximately 60% of reported arterial lesions associated with BD is an aneurysm.
Ao>PA>FA

AneurysmAortic aneurysms show rapid progression to rupture,
and as a result, huge retroperitoneal hematoma or hemoperitoneum.
Aortic aneurysms are often a pseudoaneurysm
Posterior or lateral walls of normally sized aorta and then extend into the adjacent retroperitoneal space

AneurysmOccurrence of PAA along with deep vein thrombosis
is defined as Hughes-Stovin syndrome (HSS), which may be a variant of BD.
Patients with HSS have a poor prognosis.The occurrence of intracranial aneurysm in BD is very
rare

TreatmentVascular DiseaseThere are no controlled data on, or evidence of
benefit from uncontrolled experience with anticoagulants, antiplatelet or antifibrinolytic agents in the management of deep vein thrombosis or for the use of anticoagulation for the arterial lesions of BD.

Clinical Manifestations: VascularFatal complications organ failureBleedinglimb ischemia
Despite immunosuppression
TreatmentVascular DiseaseThere is no firm evidence to guide the management
of major vessel disease in BD. For the management of acute deep vein thrombosis
in BD, immunosuppressive agents such as corticosteroids, azathioprine, cyclophosphamide or cyclosporine A are recommended.

TreatmentVascular DiseasePeripheral artery aneurysms carry a high rupture risk
and require repair accompanied by systemic immunosuppressives.







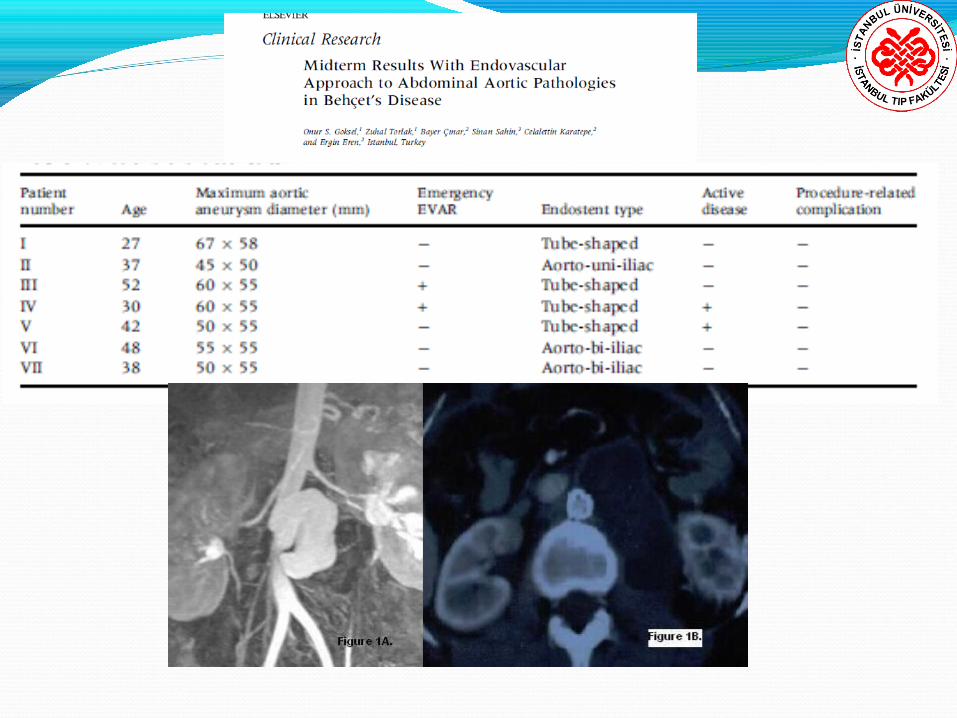

27-year old lady 90x67x58 mm abdominal aortic pseudoaneurysm
from distal suture line of an earlier patch 24x70 mm, tube-shaped Talent Endoluminal
Stent-Graft Initial experience with EVAR in Behçet’s diseaseInitial experience with EVAR in Behçet’s diseaseRupture of right CIA (Ligation and cross-over
bypass with 6 mm ePTFE graft) She is well and complication-free at her 4th year
followup.

Patient No. 3 open aortoenteric fistula52-year-old lady with hypotension abdominal pain,
pulsatile mid-abdominal mass, fever, anemia (hematocrit of 26%), leukocytosis and abdominal tenderness
Initial diagnosis: 50x 60x 55 mm infrarenal aortic pseudoaneurysm
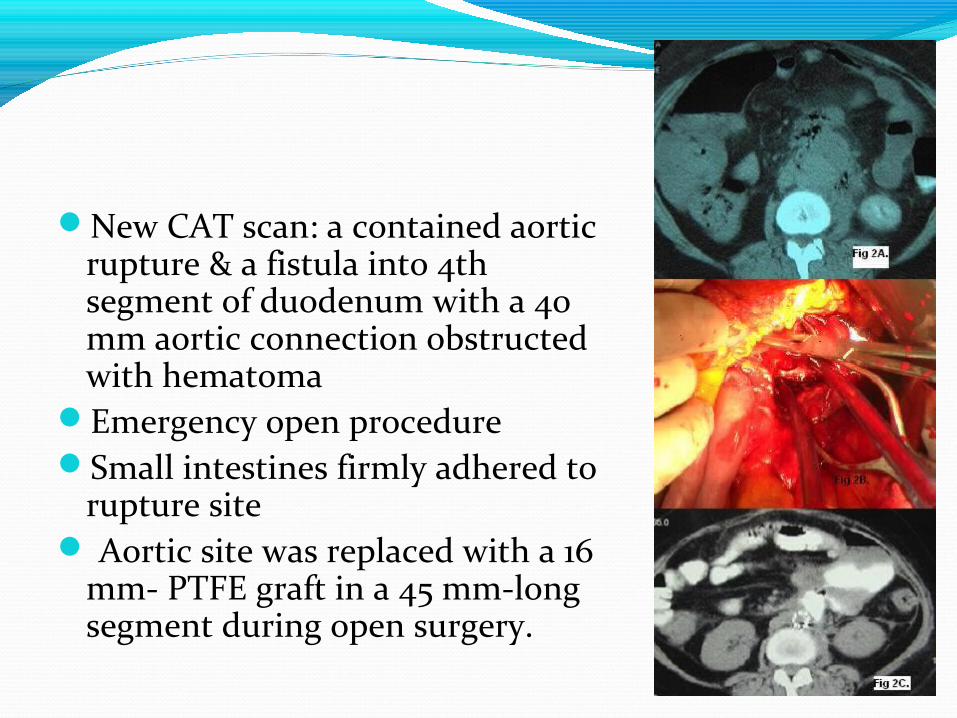
New CAT scan: a contained aortic rupture & a fistula into 4th segment of duodenum with a 40 mm aortic connection obstructed with hematoma
Emergency open procedureSmall intestines firmly adhered to
rupture site Aortic site was replaced with a 16
mm- PTFE graft in a 45 mm-long segment during open surgery.

Intestines viable and intestinal defect primarily repairedOral feeding on day 3Frank hematemesis after 9 days of uneventful course in
the hospital. An abdominal CAT scan with oral contrast showed a
residual aortoenteric fistulaTube shaped self-expandible 18 x 70 mm Talent
Endoluminal Stent-Graft (World Medical Manufacturing, Sunrise, Fla) via right femoral artery

She is symptom-free at 3 years


30-year-old diabetic male w/ ruptured ruptured 60x55 mm-infrarenal aortic aneurysm
Emergency laparatomy with aneurysm repair with 18 mm- polytetrafluoroethylene tube graft
On day 7, persistant abdominal pain and gradual hematocrit drop
CAT scan: a hematoma around the proximal suture line.
A tube shaped self-expandible 18 x 70 mm Talent Endoluminal Stent-Graft
At the time of the intervention, hematocrit was as low as 18% and did not further drop after EVAR and control CAT scan eliminated a possible leak.
Unfavorable general status He expired on day 28 with multiorgan failure. Active Behçet’s disease with other classic
systemic manifestations.

A focal surgical repair often results in late complications requiring a re-intervention as in our first patient
Endovascular repair may be a better option for aortic pseudoaneurysms being less invasive with avoidance from aortic anastomoses
Emergency or contaminated settings (aorto-enteric fistulae) open surgery may be required.
In our experience, treatment of such lesions with patch-repair results in recurrence


Kwon et al. EJVES 2008Kwon et al. EJVES 2008

Small Aneurysm <40 mm


Importance of close scrutiny for vascular lesions in Behcet’s disease can not be overstated
Follow-up with a CAT scan as frequent as every six months in spite of adequate suppression of the active Behçet’s disease has been suggested

Experience on a limited number of patients and presentation of complicated cases at most of the time may hinder the true outcome of EVAR in these situations.
More specific conclusions on issues particularly as aortoenteric fistulae are to be reached with growing experience.

Strategy?

Timing?!?

No ordinary lesion?

Cooperation-coordination!

Investigational Tx
No doubt is about the future role of biologic agents and targeted agents against proinflammatory cytokines such as IL-15, 17, 21, and adhesion molecules in controlling BD.
Using biological agents targeting TNF-alpha may improve endothelial dysfunction responsible for more features of BD.

97 published papers 1990
573 papers 2010



![Review Article Behcet s Disease: Is There Geographical ...downloads.hindawi.com/journals/ijr/2015/945262.pdf · Behcet s Disease [ ]. e ISG dened a set of international classic ation](https://img.pdfslide.net/doc/110x75/5f1a9235717bf0787a15e21c/review-article-behcet-s-disease-is-there-geographical-behcet-s-disease-.jpg)