Embed Size (px)
Citation preview

A novel approach for treatment of theimpacted maxillary incisorMohammed Almuzian, Jimmy Freel, Nicola Cross and Alastair GardnerOrthodontic Department, Glasgow Dental Hospital and School, Glasgow, Scotland, UK
This case report demonstrates a novel treatment approach to deal with a severely rotated and impacted upper
central incisor in an adolescent patient. A precision custom-made gold attachment was fabricated from a prototype
using cone beam computerized tomograph (CBCT) scan data and then used to align and de-rotate the impacted
central incisor.
Key words: precision attachment, CBCT, impacted incisor
Received 24 September 2014; accepted 3 January 2015
IntroductionThe incidence of unerupted maxillary central incisors
during the mixed and early permanent dentition stage
has been reported to be 0.13–2.6% (MacPhee, 1935;
DiBiase, 1969). Missing and unerupted maxillary
incisors have a negative effect on dentofacial appearance(Shaw et al., 1991). An additional impact of missing
maxillary incisors includes speech difficulties particu-
larly with the ‘s’ sound (Weinberg, 1968). The aetiology
of an impacted upper central incisor is multifactorial.
Hereditary factors include supernumerary teeth, cleft lip
and palate, cleidocranial dysostosis, abnormal tooth/
tissue ratio and gingival fibromatosis. Environmental
factors can include trauma, early extraction or loss ofdeciduous teeth, retained deciduous teeth, cystic forma-
tion and thick bone or tissue (Yaqoob et al., 2010).
The management of impacted maxillary incisors is the
subject of specific clinical guidelines in the UK (Yaqoob
et al., 2010). However, this situation can present
significant challenges to the clinician in terms ofmanagement. Successful treatment depends on the
interaction of many factors. Among these are patient
age, compliance, aetiology of impaction, accurate
localisation of impacted tooth, treatment mechanics,
amount of keratinized gingivae, presence of dilacera-
tions and the method of surgical exposure (DiBiase,
1971; Kolokithas and Karakasis, 1979; Munns, 1981;
Vermette et al., 1995; Noar and Gaukroger, 2000).
Clinical and radiographic methods exist to allow
localisation of the impacted central incisor (Moyers,
1976). Radiological methods frequently involve the right-
angle, magnification (Brook, 1974; Armstrong et al., 2003;
Chaushu et al., 1999) and parallax techniques (Clark,
1910). If conventional radiographs cannot provide
enough information regarding the clinical condition, thencone beam computerized tomography (CBCT) is justified
on an individual basis (Isaacson et al., 2008).
This paper describes a novel method of utilizing a
CBCT scan to localize an impacted central incisor,
assess the space requirement, plan the orthodontic
mechanics and design and construct a precision attach-
ment. The custom-made attachment was prescribed to
perform particular tooth movements, which would bedifficult to achieve by conventional methods.
HistoryA fit and well 15-year-old male was referred to the
Orthodontic department at Glasgow Dental Hospital and
School, complaining of an unerupted upper right perma-
nent central incisor. There was a history of early loss of the
deciduous right central incisor due to previous trauma,which might explain the patient’s clinical presentation.
Extra-oral assessmentThe patient presented with a mild class II skeletal base
with average vertical proportions, mild retrogenia and
no obvious asymmetries. The lips were competent with
normal incisor show at rest and smile (Figure 1).
Intra-oral assessmentThe patient was in the permanent dentition with no
active dental disease. The incisor relationship was class
III with an edge-to-edge occlusion. There was moderate
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:1
3
CLINICAL SECTION Journal of Orthodontics, Vol. 000, 2014, 000–000
Address for correspondence:
Email: [email protected]# 2014 British Orthodontic Society DOI 10.1179/1465313315Y.0000000002

crowding in the upper arch and mild crowding in the
lower arch. The molar relationship was class I bilat-
erally, with the upper centreline shifted by 3 mm to the
right side (Figure 2).
Radiographic assessmentAn orthopantomogram (Figure 3) and lateral cephalo-
metric radiograph (Figure 4a) showed the maxillary
right central incisor to be impacted, severely rotated and
located within the line of the arch. The cephalometric
tracing confirms the clinical diagnosis (Figure 4b).
Aims of the treatmentThe aims of treatment were as follows:
N secure and maintain dental health throughout treatment;
N relieve the crowding and align teeth with early de-
rotation of the impacted tooth;
N surgical exposure of the upper right central incisor
(UR1) (closed surgical exposure) and bonding of a
precision attachment;
N achieve a class I incisor, molar and canine relationshipwith normal overjet and overbite;
N long-term retention.
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:1
3
Figure 2 Intra-oral views
Figure 1 Extra-oral views
COLOURFIGURE
COLOURFIGURE
2 Almuzian et al. Clinical Section JO Month 2014

Treatment plan and rationaleAll treatment options were explained to the patient and
his parent, including:
1. accepting the position and monitoring the impacted
tooth;
2. orthodontic camouflage on a non-extraction basis
using upper and lower fixed appliances to open
space for the impacted UR1, followed by surgical
exposure of the impacted tooth and bonding of a
precision attachment to align the tooth. If the tooth
failed to respond to active traction then the
treatment would be modified to options 3 or 4);
3. orthodontic camouflage using upper and lower
fixed appliances to regain space for the UR1,
followed by restorative replacement. The impacted
incisor would be monitored or extracted;
4. orthodontic camouflage based on extraction of the
impacted tooth, using upper and lower fixed
appliance to close the space and disguise the UR2
as a UR1.
The patient and his parent chose option number (II).
Treatment progressAfter acquiring informed consent form the patient and
parent, an upper pre-adjusted fixed appliance 0.02260.028-inch slot with MBT prescription was bonded, with
the exception of the UR1 and UR2, which were bonded
with Roth prescription brackets at a later stage. The
lower arch was bonded at a subsequent visit. In theupper arch, during the first three visits, the UR2 was by-
passed (Figure 5) and then at the fourth visit, it was
bonded with an axially offset-positioned bracket This
particular bracket position with the Roth prescription
aided in increasing the tip expression of the upper right
lateral incisor, which kept its root away from the
impacted incisor to reduce the risk of root resorption.
In the upper arch, a light nickel–titanium push coil
was used on 0.016 and 0.018-inch stainless steel
archwires to create sufficient space for the unerupted
UR1 (Figure 6). The required space was achieved by
6 months and maintained with an acrylic tooth attached
to an orthodontic bracket to camouflage the space
(Figure 7). This was followed by radiographic consulta-tion to exclude any potential resorption and/or anky-
losis. Accordingly, a sectional CBCT scan for the
maxillary region was recommended for detailed assess-
ment of the anterior teeth. The CBCT provided a more
refined depiction of the UR1 ectopia, illustrating its
rotation and close proximity to the thin cortical plate,
with its apex located within the anterior portion of the
nasal septum with a mild degree of vestibular rootangulation. There was no resorption of the adjacent
teeth, follicular expansion, periapical pathology internal
root resorption or ankyloses (Figure 8).
The DICOM file of the CBCT scan was converted to
an STL file, which was used to print a three-dimensional
model of the maxillary region. This model assisted intailoring the future mechanics that were required to
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:1
5
Figure 3 Pre-treatment orthopantograph
Figure 4 Pre-treatment cephalometric radiograph: (a) cephalometric radiograph; (b) tracing
COLOURFIGURE
JO Month 2014 Clinical Section A novel approach for impacted incisors 3

align the impacted tooth. Additionally, it helped the oral
surgeon with surgical planning. It was used by the dental
technician to construct the precision attachment and
aided with informed consent of the second phase of
treatment. The laboratory procedure to construct this
attachment involved using the plastic tubes cut into
three equal sized pieces, waxed together in a horizontal
parallel arrangement and attached to the wax pattern of
the attachment. The wax pattern was then sprued, invested
using a carbon-free phosphate bonding investment and
cast using yellow gold alloy (type 4, gold content of 72%,
melting range of 1090–1140uC). The pattern was then
divested, sandblasted using 50-mm aluminium oxide,
trimmed, highly polished and autoclaved for sterilisation
(Figure 9). The laboratory cost for constructing this
precision attachment was around £70.
Next, surgical exposure and bonding of the precision
attachment under intravenous sedation was performed
with the precision gold pad attachment bonded using
dual cure resin bonding material (Figure 10).
On review, the patient reported an uneventful recovery
and orthodontic treatment was started. Orthodontic
mechanics involved a combination of two couple forces
generated by power chain elastic that extended from the eyelet
of a horizontal auxiliary arm welded to the working archwire
and passed through the horizontal tube of the precision
attachment. The auxiliary arm was made from 0.01960.025-
inch stainless steel wire, welded using a CO2 laser. It
extended palatally at a tangent to the incisive papillae.
Night-time anterior box elastics (3/8-inch, 3.5 ounce) were
prescribed to control the overbite (Figure 11). As a result
of these mechanics, the impacted tooth was completely
derotated, while partially erupted, moved palatally and
erupted within the attached palatal tissue in three visits.
Subsequently, an UR1 bracket with reduced torque
(Roth prescription) was bonded and a piggy-back
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:1
6
Figure 5 Upper fixed appliance, 0.016-inch stainless steel archwire and light NiTi compression spring in place(note: the UR2 is not bonded)
Figure 6 Upper and lower fixed appliance (fully bonded), 0.018-inch stainless steel archwires and light NiTicompression spring in place
Figure 7 (a) At the end of space-opening with 0.01960.025-inch stainless steel customized and coordinated
COLOURFIGURE
COLOURFIGURE
COLOURFIGURE
4 Almuzian et al. Clinical Section JO Month 2014

technique used, consisting of a base arch wire of
0.01960.025-inch stainless steel, with a vertical step to
avoid interference with tooth alignment and an auxiliary
archwire of 0.012-inch nickel–titanium. Night-time
anterior box elastics (3/8-inch, 3.5 ounce) were used
simultaneously (Figure 12). These mechanics were
carried out for 3 months with regular monitoring of
the tooth and gingival condition.
The final bracket position was reassessed, repositioned
and 0.01960.025-inch nickel–titanium archwire placed
in conjunction with night-time use of two lateral box
elastic (3/8-inch, 3.5 ounce) whilst the closure of resi-
dual spacing was carried out on a 0.01960.025-inch
stainless steel using power chain elastic (Figure 13).
After complete space closure, a 0.01960.025-inch TMA
archwire, for detailing and finishing, was placed in
addition to settling elastics at night time (Figure 14).
The patient was then debonded and fitted with an
upper bonded retainer on the four incisors. Upper
and lower vacuum-formed retainers were provided for
nocturnal use. A localized gingivectomy of the excess
gingivae of the UR1 was performed at debond using
electro-surgical cautery (Figure 15). Fixed appliance
treatment was completed in nineteen months. At review
visit, 2 months later, the patient presented with the
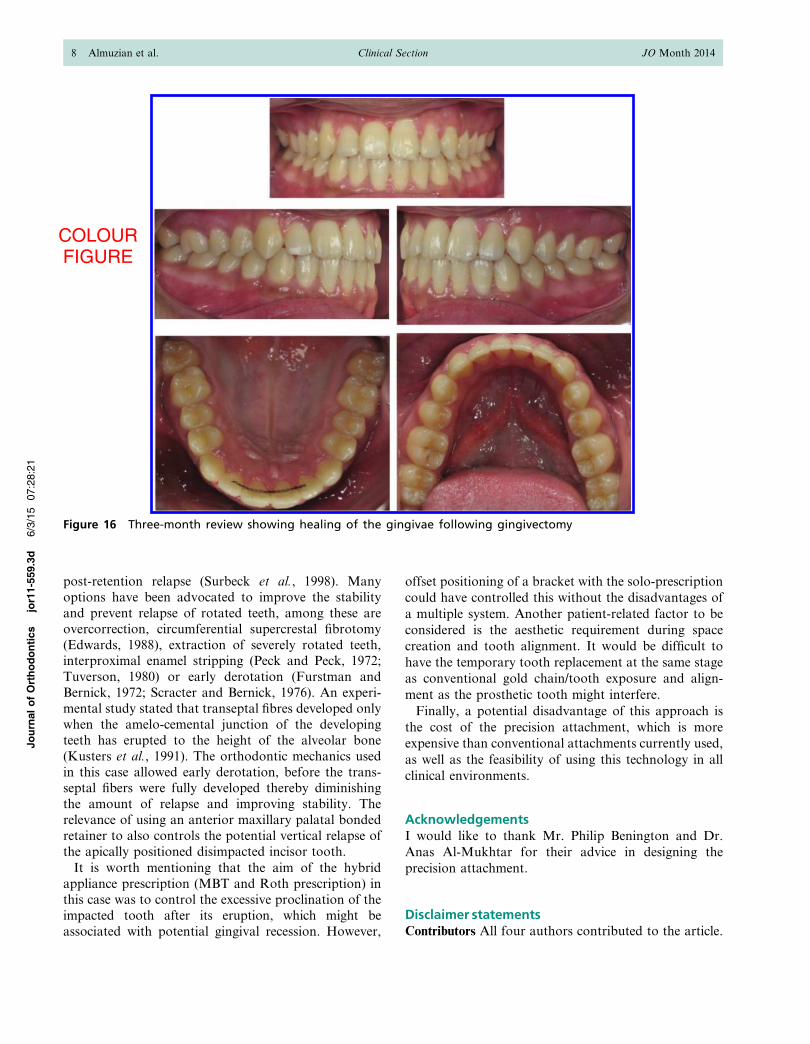
wound healed and gingivitis resolved (Figure 16).
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:1
7
Figure 8 CBCT of the maxillary region using i-Cat vision #. Top row of serial CBCT slices shows a crown-rootdilaceration and an apical third vestibular root angulation in relation to the root deflecting off the cortical boneof the floor of the nose during final root development
Figure 9 Completed precision attachment on a three-dimensional model of the maxillary region
COLOURFIGURE
COLOURFIGURE
JO Month 2014 Clinical Section A novel approach for impacted incisors 5

DiscussionEarly identification of ectopic central incisors, their
position and the degree of displacement are essential for
successful outcome (Macleod and Heath, 2008; Becker
et al., 2010). An impacted incisor with a thin cortical
bone or bone dehiscence has a high potential for
gingival recession (Vandenberghe et al., 2007) and
subsequent aesthetic and hypersensitivity problems(Noar and Gaukroger, 2000).
In this case, the precision attachment and the
information derived from the CBCT scan helped in
identifying the clinical condition of the impacted tooth
and adjacent teeth (Hodges et al., 2013) alongside
designing the precision bonded incisor tip attachment
and planning the orthodontic movement. The mechanics
used in this case allowed the tooth to move and erupt
within the attached palatal gingivae and prevented labial
eruption of the tooth that showed some degree of
vestibular root angulations. These had been reported to
be associated with bone fenestration, gingival recession
(Topouzelis et al., 2010) and even loss of vitality due
to apex perforation of the labial plate of bone (Uematsu
et al., 2004). This would have been difficult or
impossible to achieve using conventional attachments,
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:1
9
Figure 10 Surgical procedure to expose the impacted UR1 and bond the precision attachment
Figure 11 Mechanics used to derotate the impacted UR1
Figure 12 Mechanics used to align and erupt the impacted UR1
COLOURFIGURE
COLOURFIGURE
COLOURFIGURE
6 Almuzian et al. Clinical Section JO Month 2014

which lack rigidity, particularly in the axial and antero-
posterior planes.
Additionally, this technique preserved the labial
cortical bone as a minimal amount of clinical crown
was sufficient to provide retention for the precision
attachment which was replaced, when the severity and
depth of impaction had reduced, with a labial bracket
without the need for another surgical exposure. The
second surgical exposure was avoided which might be
required if a single exposure to place an initial labial
bracket from the outset otherwise be undertaken (Lin,
1999; Pavlidis et al., 2011).
At the same time, the tooth was fully derotated while
partially erupted. A gold cast attachment was used for
its biocompatibility and the potential increased success
of bonding due to the increased retentive surface area.
Additionally, the information extracted from CBCT
data helped in assessing the amount of space available
for the unerupted tooth. An additional factor, which
plays a crucial part in the management of impacted
incisors, is the position of the tooth axially, as this has a
significant effect on the stability of the result (Swanson
et al., 1975). A histological observational study by
Reitan found that the teeth with sever rotation show a
significant risk of relapse due to the influence of
free gingival fibre (Reitan, 1967). Another study has
suggested that pre-treatment irregularity and/or rota-
tion of maxillary incisors is a significant risk factor for
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:2
0
Figure 13 Pre-finishing stage of the treatment
Figure 14 Finishing stage with settling elastic in use
Figure 15 Immediately post-debond and retainer in use
COLOURFIGURE
COLOURFIGURE
COLOURFIGURE
JO Month 2014 Clinical Section A novel approach for impacted incisors 7
post-retention relapse (Surbeck et al., 1998). Many
options have been advocated to improve the stability
and prevent relapse of rotated teeth, among these are
overcorrection, circumferential supercrestal fibrotomy
(Edwards, 1988), extraction of severely rotated teeth,interproximal enamel stripping (Peck and Peck, 1972;
Tuverson, 1980) or early derotation (Furstman and
Bernick, 1972; Scracter and Bernick, 1976). An experi-
mental study stated that transeptal fibres developed only
when the amelo-cemental junction of the developing
teeth has erupted to the height of the alveolar bone
(Kusters et al., 1991). The orthodontic mechanics used
in this case allowed early derotation, before the trans-septal fibers were fully developed thereby diminishing
the amount of relapse and improving stability. The
relevance of using an anterior maxillary palatal bonded
retainer to also controls the potential vertical relapse of
the apically positioned disimpacted incisor tooth.
It is worth mentioning that the aim of the hybrid
appliance prescription (MBT and Roth prescription) in
this case was to control the excessive proclination of the
impacted tooth after its eruption, which might be
associated with potential gingival recession. However,
offset positioning of a bracket with the solo-prescription
could have controlled this without the disadvantages of
a multiple system. Another patient-related factor to be
considered is the aesthetic requirement during space
creation and tooth alignment. It would be difficult to
have the temporary tooth replacement at the same stage
as conventional gold chain/tooth exposure and align-
ment as the prosthetic tooth might interfere.
Finally, a potential disadvantage of this approach is
the cost of the precision attachment, which is more
expensive than conventional attachments currently used,
as well as the feasibility of using this technology in all
clinical environments.
AcknowledgementsI would like to thank Mr. Philip Benington and Dr.
Anas Al-Mukhtar for their advice in designing the
precision attachment.
Disclaimer statementsContributors All four authors contributed to the article.
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:2
1
Figure 16 Three-month review showing healing of the gingivae following gingivectomy
COLOURFIGURE
8 Almuzian et al. Clinical Section JO Month 2014

Funding None.
Conflicts of interest None.
Ethics approval None.;
ReferencesArmstrong C, Johnston C, Burden D, Stevenson M. Localizing ectopic maxillary
canines: horizontal or vertical parallax. Eur J Orthod 2003; 25: 585–589.
Becker A, Chaushu S, Casap N. Cone-beam computed tomography and the
orthosurgical management of impacted teeth. JADA 2010; 141: 14S–18S.
Brook AH. Dental anomalies of number, form and size: their prevalence in
British schoolchildren. J Int Assoc Dent Child 1974; 5: 37–53.
Chaushu S, Chaushu G, Becker A. The use of panoramic radiographs to localize
displaced maxillary canines. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 1999; 88: 511–516.
Clark CA. A method of ascertaining the relative position of unerupted teeth by
means of film radiographs. Proc R Soc Med 1910; 3: 87.
DiBiase DD. Midline supernumeraries and eruption of the maxillary central
incisor. Dent Pract 1969; 20: 35–40.
DiBiase DD. The effects of variations in tooth morphology and position on
eruption. Dent Pract 1971; 22: 95–108.
Edwards JG. A long-term prospective evaluation of the circumferential
supracrestal fiberotomy in alleviating orthodontic relapse. Am J Orthod
Dentofac Orthop 1988; 93: 380–387.
Furstman L, Bernick S. Clinical considerations of the periodontium. Am J
Orthod 1972; 61: 138–155.
Hodges RJ, Atchison KA, White SC. Impact of cone-beam computed
tomography on orthodontic diagnosis and treatment planning. Am J
Orthod Dentofac Orthop 2013; 143: 665–674.
Isaacson K, Thom A, Horner K, Whaites E. Orthodontic Radiographs
Guidelines. 3rd edn. London: British Orthodontic Society. 2008.
Kolokithas G, Karakasis D. Orthodontic movement of dilacerated maxillary
central incisor: report of a case. Am J Orthod 1979; 76: 310–315.
Kusters S, Kuijpers-Jagtman A, Maltha J. An experimental study in dogs of
transseptal fiber arrangement between teeth which have emerged in
rotated or non-rotated positions. J Dent Res 1991; 70: 192–197.
Lin YTJ. Treatment of an impacted dilacerated maxillary central incisor. Am J
Orthod Dentofac Orthop 1999; 115: 406–409.
Macleod I, Heath N. Cone-beam computed tomography (CBCT) in dental
practice. Dent Update 2008; 35: 594–598.
Macphee C. The incidence of erupted supernumerary teeth in consecutive series
of 4000 school children. Br Dent J 1935; 58: 59–60.
Moyers RE. Standards of Human Occlusal Development. Ann Arbor, MI:
University of Michigan Center. 1976.
Munns D. Unerupted incisors. J Orthod 1981; 8: 39–42.
Noar JH, Gaukroger MJ. Customized metal coping for elastic traction of an
ectopic maxillary central incisor. J Clin Orthod 2000; 34: 585.
Pavlidis D, Daratsianos N, Jager A. Treatment of an impacted dilacerated
maxillary central incisor. Am J Orthod Dentofac Orthop 2011; 139: 378–
387.
Peck H, Peck S. An index for assessing tooth shape deviations as applied to the
mandibular incisors. Am J Orthod 1972; 61: 384–401.
Reitan K. Clinical and histologic observations on tooth movement during and
after orthodontic treatment. Am J Orthod 1967; 53: 721–745.
Scracter RI, Bernick S. The development and maturation of the supracrestal
fibers in nonhuman primates. Angle Orthod 1976; 46: 351–360.
Shaw W, O’Brien K, Richmond S, Brook P. Quality control in orthodontics:
risk/benefit considerations. Br Dent J 1991; 170: 33–37.
Surbeck BT, Artun J, Hawkins NR, Leroux B. Associations between initial,
posttreatment, and postretention alignment of maxillary anterior teeth.
Am J Orthod Dentofac Orthop 1998; 113: 186–195.
Swanson WD, Riedel RA, D’anna JA. Postretention study: incidence and
stability of rotated teeth in humans. Angle Orthod 1975; 45: 198–203.
Topouzelis N, Tsaousoglou P, Pisoka V, Zouloumis L. Dilaceration of maxillary
central incisor: a literature review. Dent Traum 2010; 26: 427–433.
Tuverson DL. Anterior interocclusal relations Part II. Am J Orthod 1980; 78:
371–393.
Uematsu S, Uematsu T, Furusawa K, Deguchi T, Kurihara S. Orthodontic
treatment of an impacted dilacerated maxillary central incisor combined
with surgical exposure and apicoectomy. Angle Orthod 2004; 74: 132–136.
Vandenberghe B, Jacobs R, Yang J. Diagnostic validity (or acuity) of 2D CCD
versus 3D CBCT-images for assessing periodontal breakdown. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 2007; 104: 395–401.
Vermette ME, Kokich VG, Kennedy DB. Uncovering labially impacted teeth:
apically positioned flap and closed-eruption techniques. Angle Orthod
1995; 65: 23–32.
Weinberg B. A cephalometric study of normal and defective/s/articulation
and variations in incisor dentition. J Speech Lang Hear Res 1968; 11: 288–
300.
Yaqoob O, O’Neill J, Gregg T, Noar J, Cobourne MT, Morris D. Management
of unerupted maxillary incisors. Available at: http://www.rcseng.ac.uk/fds/
publications-clinical/ManMaxIncisors2010.pdf (accessed 2014 November
14).
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:2
3
JO Month 2014 Clinical Section A novel approach for impacted incisors 9

Authors QueriesJournal: Journal of OrthodonticsPaper: 11559Title: A novel approach for treatment of the impacted maxillary incisor
Dear Author
During the preparation of your manuscript for publication, the questions listed below have arisen. Please attend to
these matters and return this form with your proof. Many thanks for your assistance
QueryReference
Query Remarks
1 Please supply the information for‘Con t r i bu t o r s ’ and ‘E th i c sapproval’.
Jo
urn
al
of
Ort
ho
do
nti
cs
jor1
1-5
59.3
d6/3
/15
07:2
8:2
3





























