Embed Size (px)
Citation preview

Spine Deformity 1 (2013) 365e370www.spine-deformity.org
A Radiological Evaluation of Lateral Vertebral Subluxation AssociatedWith Spinal Stenosis in the Lumbar Spine in Degenerative Scoliosis
Richard O.E. Gardner, FRCS (Orth), Peter A.G. Torrie, MRCS (Eng), Wendy Bertram, MD,Richard P. Baker, FRCS (Orth), Ian J. Harding, BA FRCS (Orth)*
Department of Orthopaedic Surgery, Frenchay Hospital, Bristol, United Kingdom
Received 14 January 2013; revised 14 May 2013; accepted 22 May 2013
Abstract
Study Design: Retrospective longitudinal cohort.Objective: To evaluate the different patterns of stenosis with lateral subluxation in degenerative lumbar scoliosis (DLS).Summary of Background Data: Lateral subluxation of the vertebra is commonly seen in DLS. Different patterns of subluxation occur atdifferent levels of the spine and are often associated with neurological compression that can be symptomatic requiring treatment. Thepattern and location of the stenosis are variable in DLS. No study to date has evaluated the site of stenosis seen on magnetic resonanceimaging with respect to the different patterns or locations of lateral subluxation.Methods: The standing radiographs and supine magnetic resonance imaging scans of 35 consecutive patients with DLS were analyzed anddemonstrated lateral listhesis on standing radiographs (average age, 70.2 years). Subluxation level, amount of listhesis, subluxation angle,axial rotation, and pattern or location of spinal stenosis were noted.Results: There were 60 subluxations in 35 patients. Open subluxations resulted in predominantly contralateral lateral recess and foraminalstenosis (71%; 17 of 24 patients). Closed dislocations demonstrated an ipsilateral pattern of stenosis (82%; 14 of 17 patients). Opensubluxations were most commonly present at L3e4 toward the convex apex, whereas closed subluxations were identified on the concavityof the curve, with L1e2 most frequently involved (53%; 9 of 17 patients). An association was identified with open dislocations involvingthe mid-lumbar spine and closed subluxations at L1e2 (p ! .001).Conclusions: Open and closed subluxations in DLS result in different patterns of spinal stenosis. The presence of unilateral stenosis shouldalert the clinician to the possibility of spinal deformity and lateral subluxation. After careful review of the anteroposterior standingradiograph, any lateral subluxation and its type can be determined. This may assist decision making in how to treat the stenosis whendeformity is present.� 2013 Scoliosis Research Society.
Keywords: Degenerative lumbar scoliosis; Lateral subluxation; Patterns of spinal stenosis
Introduction
Degenerative lumbar scoliosis (DLS) is a progressive3-dimensional deformity that occurs de novo in adulthood ina previously non-deformed spine [1]. Causative mechanismsinclude multilevel, asymmetric discopathies; arthritis anderosion of the facet joints; or a combination of both [1,2].
Author disclosures: ROEG (none); PAGT (none); WB (none); RPB
(none); IJH (none).
*Corresponding author. Department of Orthopaedics, Frenchay
Hospital, Frenchay Park Road, Bristol BS16 1LE, United Kingdom.
Tel.: (þ44) 1173 403744; fax: (þ44) 117 9806641.
E-mail address: [email protected] (I.J. Harding).
2212-134X/$ - see front matter � 2013 Scoliosis Research Society.
http://dx.doi.org/10.1016/j.jspd.2013.05.010
Lateral subluxation (lateral spondylolisthesis and lateralrotatory olisthesis [3]) of the vertebra is frequently presenton standing radiographs (Fig. 1). The deformity consists oflateral translation toward the convexity of the curve with orwithout axial rotation, and possibly some anterior trans-lation. It is said to be present in 13% to 20% of adults withdegenerative lumbar scoliosis [4]. The deformity may resultin mechanical compression of the exiting nerve roots[2,3,5], causing radicular symptoms in the lower limbs thatcan be intrusive and that may in fact be the only presentingclinical problem. Recently, a study described a close cor-relation between patient satisfaction, health status, andlateral subluxation in adult degenerative scoliosis [6]. Thus,

Fig. 1. Example of patient with degenerative lumbar scoliosis with lateral
subluxation: open subluxation at L2e3 and closed subluxation at L3e4.
366 R.O.E. Gardner et al. / Spine Deformity 1 (2013) 365e370
careful assessment of the presence and nature of thesesubluxations is important in patient assessment.
Using computed tomography, Guillaumat and Tassin [1]described a pattern of open, closed, and parallel subluxa-tion (Fig. 2). Open subluxations occur when the disc is openon the side where the vertebra above is slipping; the disc iswedged open on the convexity of the curve. The mainmechanism was thought to be a marked vertebral rotation. Inclosed subluxations, the disc is closed on the side where the
Fig. 2. Schematic of open and closed sublux
vertebra above is slipping; the disc is wedged closed on theconvexity of the curve. The mechanism for this has beenpostulated to result from facet joint erosion rather thanvertebral rotation. When there was vertebral subluxation butno angulation between the vertebrae (ie, no open or closeddisc wedging), it was described as parallel subluxation [1].
Patients with DLS are often symptomatic on standing andhave relief from recumbence, because of changes that occurwith physiological loading. Supine magnetic resonanceimaging (MRI) scans show static stenosis when the spine isnot loaded, but studies have shown that supine MRI does notfully represent the degree of canal and nerve root stenosis[7-9]. However, standing MRI scans are not readily availableto investigate this dynamic problem; furthermore, patientshave difficulty in tolerating the scan because of discomfort inthe loaded position. If symptoms are intrusive and operativeintervention is indicated, accurate interpretation of thestanding and lateral radiographs is necessary to effectivelytreat spinal stenosis associated with a lateral subluxation.Operative treatment options include simple decompression,decompression, and single-level fusion in situ or multilevelsurgery with concomitant correction of deformity. Thedecision is based on many factors (eg, patient, surgeon,radiographs), but recognition of the presence of deformityand how lateral subluxation may contribute to the problemmay help in this process. In the sagittal plane, patterns ofstenosis seen in degenerative and lytic spondylolisthesis arewell recognized, but in the coronal plane no studies exist toevaluate slips in the coronal plane. Therefore, this studycompared standing radiographs with supine MRI to deter-mine the patterns (level, site, laterality, and magnitude) ofnerve root entrapment with open and closed lateral sublux-ations in DLS.
Materials and Methods
We analyzed the standing radiographs and supine MRIscans of 35 consecutive patients with DLS and lateral
ation in degenerative lumbar scoliosis.

Fig. 3. Measurement of lateral displacement of vertebral subluxation.
Fig. 4. Measurement of vertebral subluxation angle at affected levels.
367R.O.E. Gardner et al. / Spine Deformity 1 (2013) 365e370
subluxation (average age, 70.2 years; range, 60e86 years,21 women and 14 men). Inclusion criteria requiredpatients to be over 50 years of age and to havehad radiographic evidence of DLS on the anteroposterior(AP) standing radiograph, with 1 or more levels demon-strating lateral subluxation greater than 5 mm betweenadjacent vertebrae. Patients were excluded from thestudy if they had preexisting known spinal pathology(eg, adolescent idiopathic scoliosis, malignancy, spondy-lolysis, spondylolisthesis, spinal trauma) or had previouslyundergone surgery.
Statistical analysis was conducted using IBM SPSSversion 19 (Cambridge, UK). Fisher exact test was used toidentify any association between subluxation, vertebral level,and patterns of stenosis. The degree of rotation and lateraldisplacement of the vertebrae were not normally distributed;therefore, they were analyzed with Mann-Whitney U test.p ! .05 was considered significant.
Radiological parameters recorded included the following:
Standing radiograph
1. The level of vertebral body subluxation.2. The nature of that subluxation: open, closed, or
parallel (according to the Guillaumat and Tassin [1]classification).
3. Displacement (in millimeters) of the adjacent vertebra:the distance between the lateral edge of the vertebra
above compared with that below the subluxation(Fig. 3), as described by Ploumis et al. [4].
4. The angle of the subluxation, measured as the anglebetween the adjacent end plates of the 2 vertebraeinvolved (Fig. 4).
Supine MRI
1. Axial rotation relative to the midline: the anglebetween a straight line through the posterior aspect ofthe vertebral foramen and the middle of the vertebralbody and the sagittal plane [1] (Fig. 5).
2. The side and degree of central, lateral recess, andforaminal stenosis. There have been numerous methodsdescribed for measuring the degree of spinal and lateralrecess stenosis. Schonstrom et al [10] proposed thedural sac cross-sectional area. Speciale et al. [11]demonstrated wide interobserver and intraobservervariability between clinicians when assessing theseverity of MRI findings. However, the researchers ofthe current study have been less concerned with thedegree of spinal stenosis than with the definite presenceof stenosis and its location and/or laterality. Therefore,they used a simplified method based on the classifica-tion system in Table 1 for measurements (Lurie et al.[12]). In statistical analysis, grade 2 or 3 was consideredto signify the definite presence of stenosis, and grade0 and 1 to be not stenotic, so as to limit any concernsabout interobserver error.
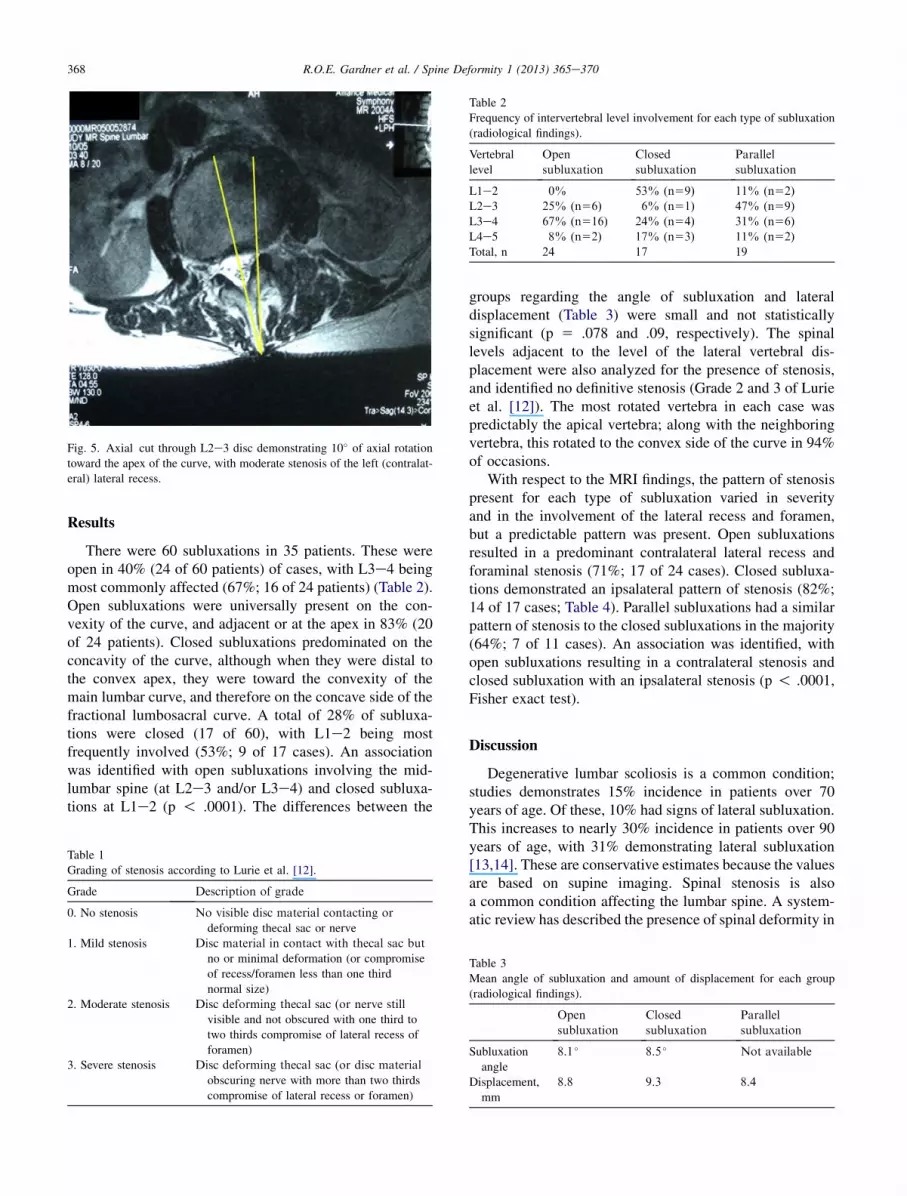
Fig. 5. Axial cut through L2e3 disc demonstrating 10� of axial rotation
toward the apex of the curve, with moderate stenosis of the left (contralat-
eral) lateral recess.
Table 2
Frequency of intervertebral level involvement for each type of subluxation
(radiological findings).
Vertebral
level
Open
subluxation
Closed
subluxation
Parallel
subluxation
L1e2 0% 53% (n59) 11% (n52)
L2e3 25% (n56) 6% (n51) 47% (n59)
L3e4 67% (n516) 24% (n54) 31% (n56)
L4e5 8% (n52) 17% (n53) 11% (n52)
Total, n 24 17 19
368 R.O.E. Gardner et al. / Spine Deformity 1 (2013) 365e370
Results
There were 60 subluxations in 35 patients. These wereopen in 40% (24 of 60 patients) of cases, with L3e4 beingmost commonly affected (67%; 16 of 24 patients) (Table 2).Open subluxations were universally present on the con-vexity of the curve, and adjacent or at the apex in 83% (20of 24 patients). Closed subluxations predominated on theconcavity of the curve, although when they were distal tothe convex apex, they were toward the convexity of themain lumbar curve, and therefore on the concave side of thefractional lumbosacral curve. A total of 28% of subluxa-tions were closed (17 of 60), with L1e2 being mostfrequently involved (53%; 9 of 17 cases). An associationwas identified with open subluxations involving the mid-lumbar spine (at L2e3 and/or L3e4) and closed subluxa-tions at L1e2 (p ! .0001). The differences between the
Table 1
Grading of stenosis according to Lurie et al. [12].
Grade Description of grade
0. No stenosis No visible disc material contacting or
deforming thecal sac or nerve
1. Mild stenosis Disc material in contact with thecal sac but
no or minimal deformation (or compromise
of recess/foramen less than one third
normal size)
2. Moderate stenosis Disc deforming thecal sac (or nerve still
visible and not obscured with one third to
two thirds compromise of lateral recess of
foramen)
3. Severe stenosis Disc deforming thecal sac (or disc material
obscuring nerve with more than two thirds
compromise of lateral recess or foramen)
groups regarding the angle of subluxation and lateraldisplacement (Table 3) were small and not statisticallysignificant (p 5 .078 and .09, respectively). The spinallevels adjacent to the level of the lateral vertebral dis-placement were also analyzed for the presence of stenosis,and identified no definitive stenosis (Grade 2 and 3 of Lurieet al. [12]). The most rotated vertebra in each case waspredictably the apical vertebra; along with the neighboringvertebra, this rotated to the convex side of the curve in 94%of occasions.
With respect to the MRI findings, the pattern of stenosispresent for each type of subluxation varied in severityand in the involvement of the lateral recess and foramen,but a predictable pattern was present. Open subluxationsresulted in a predominant contralateral lateral recess andforaminal stenosis (71%; 17 of 24 cases). Closed subluxa-tions demonstrated an ipsalateral pattern of stenosis (82%;14 of 17 cases; Table 4). Parallel subluxations had a similarpattern of stenosis to the closed subluxations in the majority(64%; 7 of 11 cases). An association was identified, withopen subluxations resulting in a contralateral stenosis andclosed subluxation with an ipsalateral stenosis (p ! .0001,Fisher exact test).
Discussion
Degenerative lumbar scoliosis is a common condition;studies demonstrates 15% incidence in patients over 70years of age. Of these, 10% had signs of lateral subluxation.This increases to nearly 30% incidence in patients over 90years of age, with 31% demonstrating lateral subluxation[13,14]. These are conservative estimates because the valuesare based on supine imaging. Spinal stenosis is alsoa common condition affecting the lumbar spine. A system-atic review has described the presence of spinal deformity in
Table 3
Mean angle of subluxation and amount of displacement for each group
(radiological findings).
Open
subluxation
Closed
subluxation
Parallel
subluxation
Subluxation
angle
8.1 � 8.5 � Not available
Displacement,
mm
8.8 9.3 8.4

Table 4
Pattern of stenosis for each type of subluxation (magnetic resonance
imaging findings).
Contralateral
stenosis
Ipsilateral
stenosis
Mixed
pattern
Open subluxation 74% (n517) 4% (n51) 22% (n55)
Closed
subluxation
12% (n52) 82% (n514) 6% (n51)
Parallel
subluxation
28% (n53) 63% (n57) 9% (n51)
369R.O.E. Gardner et al. / Spine Deformity 1 (2013) 365e370
stenosis as being a predictor for a worse outcome [15]. Thecurrent study identified patterns of spinal stenosis seen inlateral subluxation and defined different reproduciblepatterns of stenosis seen with open and closed subluxations.
When unilateral stenosis is seen on MRI imaging in themid-lumbar spine, spinal deformity and lateral subluxationshould be considered and mandatory standing radiographsrequested, to facilitate careful evaluation of the spine ina loaded position and allow an analysis of any lateralsubluxation and coronal plane deformity that may bepresent. In the authors’ practice, because of the develop-ment of degenerative deformity above the age of 50 [16],any patient over the age of 50 undergoing spinal stenosissurgery has a preoperative standing radiograph as routine tocontribute to the assessment. Preoperative standing radio-graphs are also obtained in all patients whose MRI andclinical findings are inconsistent, and in all patients whohave a clinically apparent spinal deformity. It is essential topreoperatively appreciate the presence of spinal deformityin either the coronal or sagittal plane, because it maysignificantly modify the operative plan toward arthrodesisrather than simple decompression; furthermore, it facili-tates preoperative counseling of the patient regardingpotential outcomes.
The authors agree with use of the classification systemof Guillaumat and Tassin [1] to describe patterns ofvertebral body subluxation. By analyzing the AP standingradiograph according to their description, predictablepatterns of nerve root involvement can be noted. However,several refinements were identified in this study. Guillau-mat and Tassin suggested that open subluxations werea result of extreme vertebral rotation and that no vertebralrotation occurred in closed subluxations. Conversely, thecurrent authors found that both patterns of subluxationexhibited vertebral rotation, and that subluxation closest tothe apex of the curve tended to involve the most rotatedvertebra. However, open subluxations were more frequentlyadjacent to the apex and closed subluxations were moreperipheral.
Previous researchers have reported that L3e4 is themost common level involved [4]. The current findings weresimilar and concur with previous data: the L3e4 level wasmost commonly affected in 43% of cases (26 of 60) in total(open subluxations, 67%; closed, 24%; and parallel, 31%).L2e3 (16 of 60 cases), L1e2 (11 of 60 cases), and L4e5
(7 of 60 cases) were affected less commonly than L3e4 in27%, 18%, and 12%, of cases respectively. Closedsubluxations were most commonly noted at the proximalaspect of the lumbar deformity (L1e2, 53%), on theconcave side of the curve. The pattern was that of ipsa-lateral stenosis in 82%, but there was a similar degree ofvertebral body rotation and lateral listhesis compared withopen subluxations. The number of cases in the currentseries did not facilitate an analysis of closed subluxationsoccurring in the fractional lumbosacral area compared withthose occurring more proximally at the apex of the lumbarcurve, although the authors hypothesize that the more distalclosed or parallel subluxations rotate less. Parallel sublux-ations were less predictable in their pattern of central andforaminal stenosis, but they tended to share the patternexhibited by closed subluxations.
This anatomical/radiological study has limitations. Inparticular, the researchers did not correlate the identifiedpatterns of nerve root stenosis with clinical findings. Inpractice, clinical evaluation, nerve root blocks, and/orstanding myelography could be used as a further adjunct toconfirm symptomatic nerve root entrapment before surgicaldecompression. Knowledge of such information wouldenable assessment of the importance of these anatomicalfindings more concisely on clinical practice. Nevertheless,the presence of a lateral subluxationdwhether open orcloseddshould alert the surgeon to potential patterns ofstenosis that may be exacerbated on standing, especially ifthe slip is mobile. The use of bending plain film radiographsmay offer beneficial preoperative information with regard tothe degree and direction of dynamic instability of the slip, inaddition to inferring the likely level and side of stenosis. Inthe authors’ unit, it is standard practice to conduct bendingfilms only for preoperative patients, to provide objectiveevidence of curve stiffness and guide appropriate selectionof operative spinal levels. A further limitation is that thestudy compared supine MRI images with standing radio-graphs but the authors were unable to state clearly what washappening exactly on standing in this study. As upright MRIscanners become more widely available and scanning timesdecrease, making them more tolerable for patients withsevere nerve compression symptoms, a study similar to thiswould be of great interest. Furthermore, computed tomog-raphy myelography potentially offers an alternative anduseful imaging modality for assessment and correlation ofthe degree of stenosis as seen on supine MRI imaging;however, that was not the aim of this study.
Open and closed subluxations in DLS result in predict-able patterns of spinal stenosis. This can be predicted inmany cases after a careful review of the AP standingradiograph. Conversely, unilateral patterns of stenosisshould alert the clinician to the possibility of spinaldeformity and lateral subluxation in particular. This mayhave treatment implications.
Degenerative lumbar scoliosis is both a dynamic andstatic condition. The true instability, resultant deformity,

370 R.O.E. Gardner et al. / Spine Deformity 1 (2013) 365e370
and spectrum of symptoms become evident only onstanding. Studies have shown that supine MRI does notfully represent the degree of canal and nerve root stenosis[7-9]; thus, a better understanding of the spine in a loadedposition and how it may contribute to the development andtreatment of spinal stenosis is essential. The authors believethat this study contributes to such an understanding.
References
[1] Guillaumat M, Tassin JL. Degenerative adult scoliosis. In:
Claus Carstens, Aain Deburge, editors. Surgical techniques in orthopae-
dics and traumatology. Elsevier; 2003. 55-120-D-10.
[2] Spivak JM. Current concepts reviewdDegenerative lumbar spinal
stenosis. J Bone Joint Surg Am 1998;80:1053e66.[3] Toyone T, Tanaka T, Kato D, et al. Anatomic changes in lateral spon-
dylolisthesis associated with adult lumbar scoliosis. Spine 2006;30:
E671e5.[4] Ploumis A, Transfeldt E, Gilbert T, et al. Degenerative lumbar scoli-
osis: radiographic correlation of lateral rotatory olisthesis with neural
canal dimensions. Spine 2006;31:2353e8.
[5] Trammell TR, Schroeder RD, Reed DB. Rotatory olisthesis in idio-
pathic scoliosis. Spine 1988;13:1378e82.
[6] Ploumis A, Liu H, Mehbod AA, et al. A correlation of radiographic
and functional measurements in adult degenerative scoliosis. Spine
2009;34:1581e4.
[7] Wang YC, Jeng CM, Wu CY, et al. Dynamic effects of axial loading
on the lumbar spine during magnetic resonance imaging in patients
with suspected spinal stenosis. J Formos Med Assoc 2008;107:
334e9.
[8] Will�en J, Danielson B, Gaulitz A, et al. Dynamic effects on the
lumbar spinal canal: axially loaded CT-myelography and MRI in
patients with sciatica and/or neurogenic claudication. Spine
1997;22:2968e76.
[9] Alyas F, Connell D, Saifuddin A. Upright positional MRI of the
lumbar spine. Clin Radiol 2008;63:1035e48.
[10] Schonstrom NS, Bolender NF, Spengler DM. The pathomorphology
of spinal stenosis as seen on CT scans of the lumbar spine. Spine
1985;10:806e11.[11] Speciale AC, Pietrobon R, Urban CW, et al. Observer variability in
assessing lumbar spinal stenosis severity on magnetic resonance
imaging and its relation to cross-sectional spinal canal area. Spine
2002;27:1082e6.[12] Lurie JD, Tosteson AN, Tosteson TD, et al. Reliability of readings of
magnetic resonance imaging features of lumbar spinal stenosis. Spine
2008;33:2482.
[13] Aaro S, Dahlbohn M, Svensson L. Estimation of vertebral rotation in
structural scoliosis by computerised tomography. Acta Radiol Diagn
1978;19:990e2.
[14] Aaro S, Dahlbohn M. Estimation of vertebral rotation and the spinal
and rib cage deformity in scoliosis by computerised tomography.
Spine 1981;6:460e7.
[15] Aalto TJ, Malmivaara A, Kovacs F, et al. Preoperative predictors for
postoperative clinical outcome in lumbar spinal stenosis: systematic
review. Spine 2006;31:E648eE663.
[16] Baker RP, Kilshaw M, Gardner R, et al. Abnormalities of the lumbar
spine in the coronal plane on plain abdominal radiographs. Eur Spine
J 2011;20:429e33.





![[Surgical management of vertebral column metastatic disease]](https://img.pdfslide.net/doc/110x75/634b64b6fbf5829b2b02136d/surgical-management-of-vertebral-column-metastatic-disease.jpg)























