Embed Size (px)
Citation preview

Acute childhood illness at home:the parents' perspective
Sarah J. Neill MSc BSc PGDE RSCN RGN RNT
Senior Lecturer in Children's Nursing, Centre for Healthcare Education,
Nene University College, Northampton, Northampton General Hospital NHS
Trust, Northampton, England
Accepted for publication 17 September 1999
NEILLNEILL S.J. (2000)S.J. (2000) Journal of Advanced Nursing 31(4), 821±832
Acute childhood illness at home: the parents' perspective
This critical review of British literature explores the phenomenon of acute
childhood illness at home from the parents' perspective. The Literature was
searched using four CD-ROM databases: CINAHL, MEDLINE, ASSIA and
PSYCHLIT, augmented by hand searching of current journal issues. Sande-
lowski's (1995) stages of qualitative data analysis were used to develop a
rigorous approach to conducting qualitative overviews. The majority of child-
hood illness is of short duration and takes place in the child's own home. Yet
the research which addresses this area is limited. Mothers constantly monitor
their child's health, identifying illness as a change in behaviour of the child
from their perception of normal. Their usual response to illness is nonprofes-
sional care, including general nursing care and `over the counter'. When
mothers do seek help this is usually from the family doctor. Mothers are often
dissatis®ed with the help and advice they receive. This is partially explained by
the mismatches which occur concerning the perceptions of mothers and of
health care professionals regarding appropriate use of services and the needs of
these mothers and their children. The literature reviewed indicates a need to
address the service users perceptions of the services provided. Areas where
further research is required are identi®ed.
Keywords: acute illness, minor illness, common childhood illness,
parents, families, lay knowledge, literature review, qualitative overview,
general practitioners, primary health care
INTRODUCTION1
Children under 16 years comprise 20% of the population
(Central Statistical Of®ce 1994), 19% of consultations with
doctors in general practice and 15% of consultations with
practice nurses (McCormick et al. 1995). Acute childhood
illness constitutes a high proportion of child consultations,
with the most common reason for consultation being
diseases of the respiratory system Ð 27á6% of consulta-
tions at both 0±4 and 5±15 years (Health Committee 1997).
Yet research which explores parents' experiences, suggests
that families who consult health care professionals for help
and advice when their child is acutely ill, represent a small
proportion of all childhood illness at home. Between 59
and 99% of all episodes of acute childhood illness at home
are reported to be managed without recourse to health
professionals (Mayall 1986, Holme 1995).
Despite the fact that the vast majority of childhood
illness at home is acute in nature, research regarding
Correspondence: Mrs Sarah J. Neill, Beech House, Rectory Hill,
Cranford, Kettering, Northants, NN14 4AH, England.
E-mail: [email protected]
Ó 2000 Blackwell Science Ltd 821
Journal of Advanced Nursing, 2000, 31(4), 821±832 Integrative literature reviews and meta-analyses

community health care of children has, to date, focused
around the chronically ill or high dependency child (e.g.
Derouin & Jessee 1996, Richardson et al. 1992, Copeland
& Clements 1993, Hill 1993, Whyte 1994). `Theoretical
development regarding family process during acute
illness have been limited' (Rennick 1995, p. 258) to the
experience of the hospitalized child (Cleary 1992, Darby-
shire 1994, Neill 1996). This paper changes the focus
towards understanding the phenomenon of acute child-
hood illness at home. The review is limited to the
perspective of the child's parents, as minimal research
has, to date, been located which explores the experiences
of the child or the involvement of the wider family. See
Figure 1 for de®nition of the terms used within the
review.
The broad aim of the review is to explore parents'
experiences of acute childhood illness at home. Speci®c
questions which the review addresses are:
1 How do parents' identify acute illness in their child?
2 How do parents' respond to acute illness in their child?
3 What are parents' experiences of the health services
when their child is acutely ill at home?
Literature review methodology
The nature of the research in this area does not lend itself
to a formal systematic review or meta-analysis because the
research involved includes small-scale qualitative and
quantitative studies. There is considerable heterogeneity
within the literature reviewed in terms of methodology,
consequently, `it is inappropriate to use quantitative
methods to pool data from individual studies' (Droogan
& Song 1996 p. 21). Such quantitative approaches to the
analysis would also lack philosophical congruence with
the focus of the work Ð to develop an understanding of
the experiences of families when their child is ill at home.
Therefore the method used for this review is that of a
qualitative overview (Droogan & Song 1996, NHS Centre
for Reviews & Dissemination 1996). There is no clear
consensus on the best methods to use to conduct such a
review (NHS Centre for Reviews & Dissemination 1996),
consequently a framework has been developed to facilitate
a systematic and rigorous approach. The process used is
outlined below.
Inclusion criteria· Published research reports and literature reviews in the
last 15 years of English language publications of United
Kingdom (UK) origin.
· Family experiences of acute illness in the child (up to,
but excluding, adolescence) at home.
Material from other countries was excluded, as parents'
experiences are likely to be in¯uenced by the nature of the
health services provided. The age of the child was
restricted as the majority of acute childhood illness occurs
in the 0±9 years age group and health concerns in adoles-
cents focus around other issues.
Literature searching strategiesCD-ROM databases MEDLINE, CINAHL, PSYCHLIT, and
ASSIA, augmented by regular hand searching of current
issues of journals in local libraries and sourcing of
secondary references. The following key words and
phrases were used: child(ren), infant, parent, mother,
father, family, acute illness, minor illness, common
childhood illness, perceptions, experiences, home,
community, primary health care.
Literature reviewing processThe process used to critically review the literature has
been adapted from the method used for qualitative data
analysis (Sandelowski 1995). See Figure 2 for details of
the framework used.
Combining Sandelowski's (1995) stages with Gould's
(1994) critiquing strategy provided a framework which:
a) facilitated the systematic critical analysis of each paper,
whether qualitative or quantitative in nature; and
b) resulted in a rigorous process for synthesizing the
®ndings of the review. This approach ensured that papers
are reported accurately, bias avoided, their validity
assessed and the areas of agreement and disagreement
between research ®ndings identi®ed.
Figure 1 De®nition of terms.
S.J. Neill
822 Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832

THE FINDINGS OF THE REVIEW
Twenty-two papers representing 15 research studies and
one literature review were identi®ed which met the
criteria for inclusion in the review (see Figure 3). The
studies reviewed use a mixture of quantitative and qual-
itative methods, with interviews and questionnaires
predominating.
Methodological issues in the research reviewed
Research toolsSeveral of the quantitative studies use structured ques-
tionnaires which appear to have been developed from
professional experience rather than from earlier qualita-
tive research (Wyke et al. 1990, 1991, Clarke & Hewison
1991, Cantrill et al. 1996). Consequently it is not possible
to establish if these questionnaires really measure issues
of importance to families Ð rather, they are more likely to
measure issues professionals believe to be of importance.
These research tools must be viewed as of questionable
validity.
SamplingAcross all the papers data collection was primarily from
mothers. Where studies do include fathers, this is usually
only when the father is the major carer at home. Conse-
quently, even in these studies, fathers form a small
proportion of the sample. There is no readily available
data which explores the role of other family members in
Figure 2 Framework for critically reviewing the literature Ð developing a qualitative overview. Adapted from Sandelowski M. (1995)
Focus on qualitative methods. Qualitative analysis: what it is and how to begin. Research in Nursing & Health 18, 371±375.
Integrative literature reviews and meta-analyses Acute childhood illness at home
Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832 823
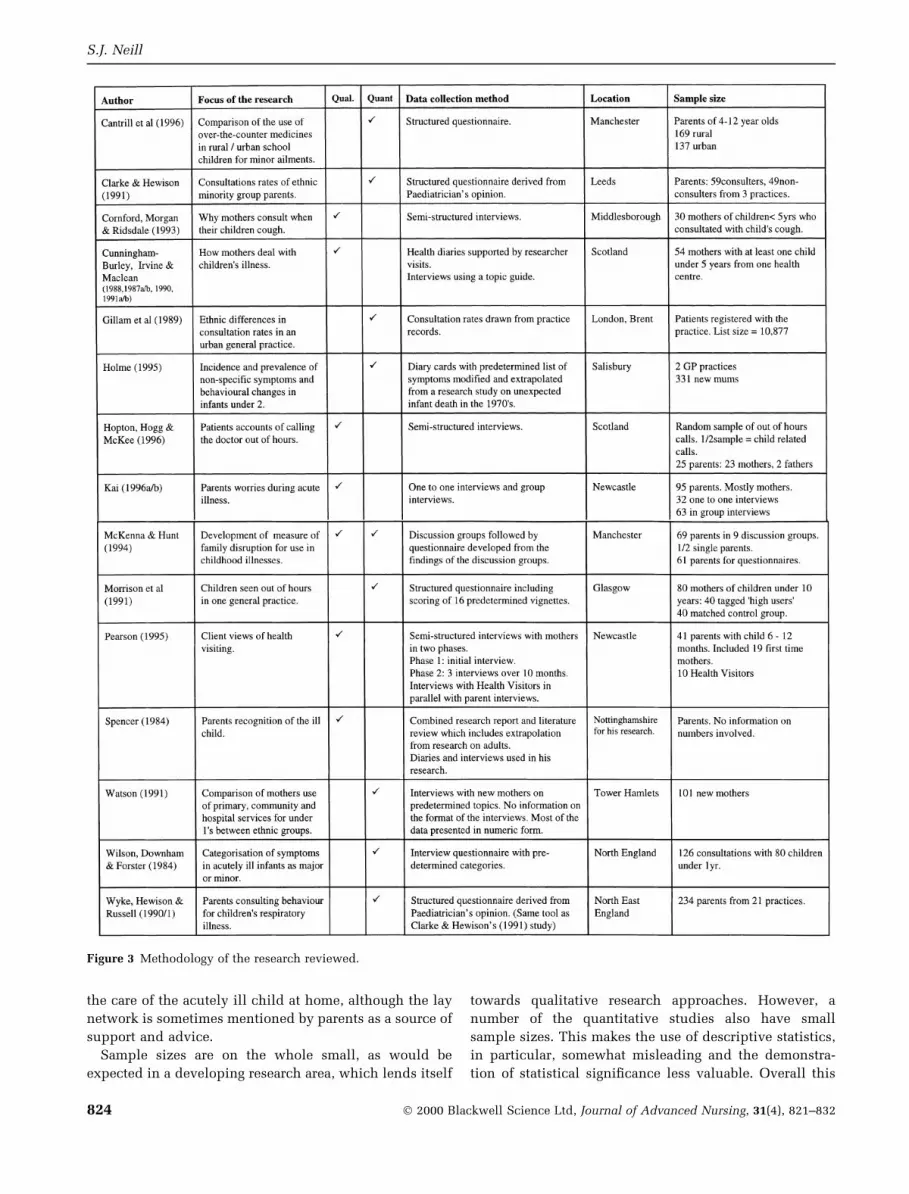
the care of the acutely ill child at home, although the lay
network is sometimes mentioned by parents as a source of
support and advice.
Sample sizes are on the whole small, as would be
expected in a developing research area, which lends itself
towards qualitative research approaches. However, a
number of the quantitative studies also have small
sample sizes. This makes the use of descriptive statistics,
in particular, somewhat misleading and the demonstra-
tion of statistical signi®cance less valuable. Overall this
Figure 3 Methodology of the research reviewed.
S.J. Neill
824 Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832

means that the results cannot be generalized to other
populations.
Location of data collectionMany of the studies were carried out in the north of
England or in Scotland (Cunningham-Burley & Irvine
1987, Cunningham-Burley & Mclean 1987, 1988, Cunn-
ingham-Burley 1990, Wyke et al. 1990, 1991, Clarke &
Hewison 1991, Morrison et al. 1991, Pearson 1995, Hopton
et al. 1996, Kai 1996a, b). Thus, although many of the
®ndings demonstrated a degree of congruence, it cannot be
concluded that these ®ndings would translate to popula-
tions further south in the UK, given knowledge of the
`Health Divide' from the North to the South of the UK
(Townsend et al. 1992). There is also a strong tendency to
investigate urban and inner-city communities. Only two of
the studies reviewed collected any data from a rural
population (Wyke et al. 1990, Cantrill et al. 1996).
However, these were quantitative studies which did not
explore the perspective or experiences of parents in any
depth.
Speci®c methodological issues relating to individual
studies are addressed within the body of the review.
KEY THEMES
The following key themes were identi®ed from the review:
· Parental perception of the child's minor illness
· Parents' actions in response to illness in their child
· Seeking help from health services
· What do parents want from services?
· Mismatch between the perceived needs of parents and
services provided.
Each theme is explored, in turn, below.
Parental perception of the child's minor illness
A number of studies reveal ®ndings which address the
ways in which parents identify illness in their children.
Within this theme several subthemes emerged: `Normal
health', `Normal illness', `Behavioural change' and Partic-
ular concerns'.
Normal healthParents assess their child's health in relation to what they
perceive as `normal' health for their child (Pearson 1995,
Spencer 1984, Mayall 1986, Cunningham-Burley 1990,
Cunningham-Burley & Maclean 1991, Irvine & Cunn-
ingham-Burley 1991). This sense of normality is based
on the parent's common sense knowledge of minor
childhood illness and speci®c knowledge of their child
(Cunningham-Burley & Maclean 1991, Cunningham-
Burley 1990, Irvine & Cunningham-Burley 1991). Both of
these areas of knowledge develop over time, as the parents
develop in their role as parents, learning about changes
with the development of the child with the ®rst child and
through using the knowledge gained, with subsequent
children (Cunningham-Burley 1990, Irvine & Cunn-
ingham-Burley 1991, Pearson 1995). Thus parents'
concept of normality changes over time.
Normal illnessParents also perceive some kinds of illness as normal for
their child (Mayall 1986, Cunningham-Burley 1990, Irvine
& Cunningham-Burley 1991, McKenna & Hunt 1994). For
example parents in 3 studies (Irvine & Cunningham-
Burley 1991, Spencer 1984, Mayall 1986) attributed many
symptoms of minor illness to teething, a process seen as a
normal part of child development. Alternatively a speci®c
illness may itself be viewed as a normal childhood illness.
McKenna & Hunt's (1994) study of parents whose child
had had chickenpox, found that although the illness
disrupted the family, the illness was in itself considered to
be normal.
Mayall (1986) and Irvine & Cunningham-Burley (1991)
explored the parents' perceptions of the child with a
persistent minor illness and found that these children
were also seen as essentially healthy. These parents
attributed the child's illness to an innate predisposition
in that individual child.
This process of normalizing some of their child's
illnesses, either as an innate part of childhood or as a
particular predisposition in the individual child, may be
one way of maintaining their own image of their child as
`healthy'. Cunningham-Burly & Maclean (1991) proposed
that this is closely linked to the parent's own self-esteem
in their role as parents.
Behavioural changeGiven this tendency to want to normalize illness in the
child, how do parents identify illness in their child?
Parents recognize illness in their child through their
assessment of the child's behaviour (Spencer 1984, Mayall
1986, Cunningham-Burley 1990, Cunningham-Burley &
Maclean 1991, Irvine & Cunningham-Burley 1991, Corn-
ford et al. 1993) which they constantly compare to their
unique knowledge of what is the normal pattern of
behaviour for their child (Irvine & Cunningham-Burley
1991, Spencer 1984, Cunningham-Burley 1990), often
termed as `not his/her normal self' (Hopton et al. 1996,
Cornford et al. 1993).
The behavioural changes of most concern were found to
be changes in eating and/or sleeping patterns (Irvine &
Cunningham-Burley 1991, Cornford et al. 1993), crying for
no identi®able reason (Cunningham-Burley 1990) and
mood changes indicated by being irritable or more `clingy'
than normal (Mayall 1986, Cornford et al. 1993). These
changes in behaviour might be interpreted in several
ways. They might be seen as the precursor of illness, the
Integrative literature reviews and meta-analyses Acute childhood illness at home
Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832 825

result of illness, the problem itself or a problem for the
family in general (Cunningham-Burley & Maclean 1991,
Irvine & Cunningham-Burley 1991). An example of the
latter might be when a child keeps the family awake
through the night. Often, however, a behavioural change is
noted but the child is seen to return to normal the next day
(Cunningham-Burley & Maclean 1991).
Symptoms of particular concernIn the literature reviewed some symptoms of particular
concern to parents emerged. These appeared repeatedly in
different studies. Some of these concerns revolved around
speci®c symptoms that parents had reported as worrying
and as their reason for taking the child to see the doctor.
These were: respiratory symptoms, particularly a persis-
tent cough; a high temperature; and vomiting and pain
(Spencer 1984, Mayall 1986, Cornford et al. 1993, Holme
1995, Hopton et al. 1996, Kai 1996a), especially if the pain
was severe, unrelieved and unexplained (Hopton et al.
1996). Three papers report on two studies based solely
around respiratory problems in children (Wyke et al. 1990,
1991, Cornford et al. 1993) as a result of professional
knowledge of parents' concern with this symptom. Holme
(1995), Cunningham-Burley & Irvine (1987) and Wilson et
al. (1984) all reported that altered breathing and/or
coughing were the commonest reason parents gave for
consulting a doctor.
Another group of concerns that emerged were those
related to media-generated fears. Two papers noted the
effect of new media coverage of an outbreak of meningitis
(Hopton et al. 1996, Kai 1996a). The nonspeci®c nature of
the symptoms which may lead to meningitis makes
assessment of children with these symptoms, particularly
problematic both for parents and for their general practi-
tioners (GPs) (Taylor 1995).
Parents have also been identi®ed as fearing that they
will not recognize serious illness in their children (Kai
1996a). For some parents this was linked to `past frights',
when their child had been diagnosed by doctors to be
much more seriously ill than they had thought prior to
seeking medical advice (Hopton et al. 1996). This `fright'
serving to reduce the parents' con®dence in their own
ability to judge the state of their child's health.
Parents' actions in response to illnessin their child
Monitoring the child's healthParents constantly monitor the state of their child's health
(Cunningham-Burley 1990, Kai 1996a). It is from this
monitoring that parents are able to make their judgement
about the normality or abnormality of the child's state of
health. Cunningham-Burley's (1990) study provides
detailed information about the nature of the monitoring
process through the use of daily health diaries with
parents. However, it has to be noted that both the diaries
themselves and the supportive visits by the researchers
during the period of diary data collection, may have
served to heighten and arti®cially enhance the parents'
monitoring process.
Treating the child themselvesWhat is clear both from Cunningham-Burley & Irvine's
(1987) paper and Spencer's (1984) earlier combined
research report and literature review, is that parents make
every effort to treat the child themselves, although their
®rst response to minor symptoms is to take no action but
to `wait and see'. When symptoms persist their treatment
of the child may consist either of nursing actions and/or
the use of `over the counter' (OTC) remedies (Spencer
1984, Mayall 1986, Cunningham-Burley & Irvine 1987,
Cornford et al. 1993, Cantrill et al. 1996). The majority of
the OTC remedies were already present in the home
(Cantrill et al. 1996).
Home nursing actions included techniques taught to
parents by their GP such as sponging the child with a
fever, steam for croup, plenty of ¯uids for fever or the
child who is not eating (Cunningham-Burley & Irvine
1987). The reference to steam for croup dates this paper as
this technique is no longer recommended due to the risk
of scalds from boiling water. Nursing action identi®ed in
Mayall's (1986) work also included a change in diet/¯uids
for the child, treats, allowing the child to sleep on the sofa
where the parents could observe the child, wrapping or
undressing the child and keeping them indoors. Common
threads were the extra attention and time that the mothers
devoted to their children when they considered them to be
ill (Mayall 1986). This is also referred to by Spencer (1984)
as increased emotional support needed by the sick child.
The most common OTC remedies were analgesia, anti-
pyretics and cough medicines (Cunningham-Burley &
Irvine 1987, Cunningham-Burley & Maclean 1987, Cantrill
et al. 1996, Mayall 1986). All of these studies report a high
use of these easily available remedies. Parents are reluc-
tant to `bother the doctor' (Kai 1996a, Cunningham-Burley
& Maclean 1991) who acts as the gatekeeper to further
medicinal treatments.
Sources of support used by parents priorto calling the doctorTwo main sources of help appear in the literature Ð
pharmacists; and family/friends. Both of these sources are
reported as being used before parents resort to calling the
doctor.
Family and friends. Forty-seven per cent of the ®rst-
time parents in Mayall's (1986) research talked about the
information they received from friends and relatives. This
information included suggested diagnoses, advice on
nursing their child, home remedies and when to refer to
S.J. Neill
826 Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832

the doctor. In both Mayall's (1986) and Kai's ®ndings
(1996a) parents are described as using a `lay network'.
Where this network was smaller and parents did not have
people to whom to refer, an increased use of general
practice services resulted (Mayall 1986). This association
with social support is also highlighted in Reading's (1997)
review of the literature on poverty in childhood. Oakley
et al.'s (1994) research identi®ed that social support for
mothers resulted in better health for their children. This
effect was found to be strongest in families living in
poverty. This focus on the supportive network of family
and friends re¯ects a key theme within the dominant
philosophy of children's nursing Ð the need for children
to be viewed and cared for within the context of their
families (Royal College of Nursing 1995).
Pharmacists. Pharmacists are seen as much less threat-
ening than doctors (Cunningham-Burley & Maclean 1991).
Parents are reported as using the chemist as a source of
information in several studies (Spencer 1984, Mayall
1986, Cunningham-Burley & Maclean 1991, Morrison et
al. 1991, Cantrill et al. 1996, Kai 1996b). The high use of
OTC remedies would seem to support the idea that many
parents use this source of advice. However, when asked
the direct question few parents identify the pharmacist or
chemist as an information resource (Cantrill et al. 1996,
Mayall 1986, Morrison et al. 1991). In Mayall (1986) study
only 3% of parents referred to the chemist as a source of
advice. In addition, Kai's (1996b) ®ndings suggest that
parents who ask the pharmacist are referred back to their
doctor. For the parents, the chemist appears to act as a
bridge between lay and professional responses to illness.
Seeking help from health services
Two broad areas emerged in the literature concerning
parents eventual decision to use health services. The ®rst
provides some insight into the reasons parents decide to
consult health services whilst the second identi®es demo-
graphic trends in parents' use of health services. What
stands out overall is the focus on doctors as the only
source of help available once the resources of family,
friends and/or the local pharmacist are exhausted.
Deciding to calling the doctorSeveral themes emerged in the reasons parents gave for
their decision to call the doctor. These include: abnormal
symptoms (Cunningham-Burley 1990, Hopton et al. 1996),
behavioural change (Hopton et al. 1996, Kai 1996b);
perceived increased severity of illness in their child (Wyke
et al. 1990, Clarke & Hewison 1991, Cornford et al. 1993);
feelings of helplessness or of being unable to cope with
their child's illness (Kai 1996b, Morrison et al. 1991) and
when their own attempts to treat the child have failed
(Cunningham-Burley & Irvine 1987, Hopton et al. 1996).
Kai (1996a) developed a theoretical model from his
qualitative study, which inversely links parents' perceived
threat of the child's illness to parents' sense of personal
control. This model suggests that the greater the perceived
threat to the child's health the more likely it is that a parent
will decide to seek professional help and advice.
Demographic patterns of health service useConsiderable attention has been paid in the medical
literature to the problem, as perceived by health profes-
sionals, of parents who use services most frequently.
However, this `medical problem' needs to be considered
from the perspective of the parents. Aside from the
symptoms of the child's illness, what other factors make
parents more likely to take their child to see the doctor?
The research in this area is mostly quantitative. Conse-
quently, the only conclusions which can be drawn are the
statistical relationships within data, i.e. which groups of
parents are most likely to use general practice services.
Two groups of parents emerged from the literature as more
likely to consult their family doctor with acute childhood
illness at home: those with lower socioeconomic status
and parents from ethnic minority groups.
Lower socioeconomic status. Parents from lower
socioeconomic groups are more likely to present to the
doctor with their child (Gillam et al. 1989). This ®nding is
not surprising as it is known that virtually all aspects of
health are worse in children living in poverty than those
living in af¯uent families (Reading 1997). Approximately
one third of children are living in conditions of poverty in
Britain today (Graham 1994). These children not only
make up a signi®cant proportion of the child population
but will be ill more often (Mayall 1986, Reading 1997) and
according to ®ndings of Watson (1991), Clarke & Hewison
(1991) and Wyke et al. (1990) they will be more seriously
ill than children in more af¯uent circumstances. Saxena et
al. (1999) re-analysis of data from the fourth national
survey of morbidity in general practice support these
®ndings. Spencer's (1984) paper considers the reasons
why socially deprived parents may present with more
seriously ill children. He suggests that these parents are
most vulnerable to breakdown of parenting skills and will
therefore fail to respond to their child's symptoms,
seeking help at a latter stage of the child's illness.
However, Morrison et al. (1991) do not concur with the
®ndings of the latter studies. In their study of children
seen out-of-hours, they found that the high users were
more likely to call the doctor than low users at the same
level of illness. However, this result was obtained by
asking parents to respond to vignettes. Their retrospective
examination of the data collected for each contact did,
however, identify the high user group as more socially
disadvantaged. Given the ®ndings presented above
concerning the relationship between lower socioeconomic
Integrative literature reviews and meta-analyses Acute childhood illness at home
Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832 827

status and poorer health, it would seem that the use of
vignettes may have led to erroneous conclusions.
Ethnic minority groups. Nine per cent of the child
population in the UK are from ethnic minority groups
(Central Statistical Of®ce 1994). One third of the ethnic
minority population consists of children, in contrast to
20% of the total population of the UK. Consequently this
is a signi®cant group of service users, particularly for areas
such as Leicester, which has a high proportion of ethnic
minorities Ð 39% in Leicester City East (Leicester City
Council 1997) in contrast to the national ®gure of 5á5%.
These ®gures are even more relevant when considered in
the light of the evidence that ethnic minorities also have
an increased incidence of socioeconomic deprivation
(Webb 1996). This would lead to higher rates of health
service use per head of the population, due to the
associated increased morbidity. Clarke & Hewison (1991)
found higher consultation rates in `Asian' groups with
increased scores for severity of illness. Watson's (1991)
investigation of health service use during the ®rst year of
life in Tower Hamlets, also found that the Bengali chil-
dren were reported to suffer more severe symptoms/
coughs/colds than children from the indigenous group.
Little information is available concerning the health
beliefs, views or perspective of parents from ethnic
minority groups concerning childhood acute ill health.
Clarke & Hewison's (1991) study conducted in Leeds, a
northern city with a high ethnic minority population, did
identify that ethnic differences in health beliefs do
contribute towards parents decision to consult their GP.
For example different beliefs were identi®ed concerning
the causes of coughs and colds. Indigenous families cited
germs and viruses, whilst `other groups' attributed these
illness to the weather. Interestingly it was the latter `other
groups' who were found to be more likely to consult.
However, the structured questionnaire design means that
parents were responding to a predetermined list, conse-
quently, their views may not be accurately represented.
What do parents want from services?
Whatever reason parents gave for deciding to seek help
from health services, several common themes emerged
which describe what expectations parents have of these
services. The most dominant theme is that of the parents'
desire for reassurance, closely followed by their desire for
information about their child's illness and care, their wish
to have their views respected and their competence as a
parent recognized and ®nally, for some parents, the desire
for medication for their child.
ReassuranceParents commonly reported that their primary need when
seeking advice from health care professionals was for
reassurance (Mayall 1986, Clarke & Hewison 1991, Irvine
& Cunningham-Burley 1991, Morrison et al. 1991, Corn-
ford et al. 1993). They wanted the doctor to con®rm that
they had taken all the necessary steps Ð that they had not
missed anything serious (Irvine & Cunningham-Burley
1991). One respondent in Cunningham-Burley &
Maclean's (1991, p. 37) paper is quoted as saying:
R28: I would prefer that the doctor would say `You're doing
everything you can. I can't help you anymore', but at least you are
settled in your mind and you've been and there is nothing else, so
you can just come back and get on with it.
In contrast, for some parents the reassurance came in the
form of a prescription which was seen as con®rming that
their child was ill (Kai 1996b) and therefore warranting
the attention of the doctor.
InformationWilson et al.'s (1984) study investigating GP consultation
for acute illness in infants, identi®ed that 51% of parents
recalled advice being given. Unfortunately, this study was
designed in an attempt to develop a list of major and
minor symptoms helpful to GP's, rather than to parents.
Consequently, they do not identify whether parents could
recall what advice had been given, whether parents
wanted advice from the consultations, or whether the
advice given was what the parents desired.
The desire for information is, however, identi®ed in
other research. Parents are reported to want information
about their child's illness and how to best to care for their
child (Mayall 1986, Cunningham-Burley & Maclean 1991,
Kai 1996b). In Kai's (1996b) study, parents sought infor-
mation from sources other than health care professionals.
These parents found that they had learnt more speci®c
information about children's illness from the media, in the
form of parenting magazines, television dramas and
publicity campaigns. This provides evidence of a more
positive role for the media than just providing frightening
material about outbreaks of disease.
Research in the ®eld of caring for the hospitalized child,
has found repeatedly that parents want more information
about their child's illness and care (e.g. Neill 1996, Kna¯
et al. 1988, MacDonald 1988, Evans 1994). Some parents
have been identi®ed as actively seeking information to
enable them to cope with their child's hospitalization
(Neill 1996, Kna¯ et al. 1988). In the former study,
receiving information had the effect of increasing parents'
sense of control. Conversely, when information was with-
held they experienced a loss of control (Neill 1996). Thus
it is not surprising that parents resort to the same coping
mechanisms when caring for an ill child at home.
Recognition of maternal competenceMothers in Cunningham-Burley & Maclean's (1991)
paper are described as `feeling stupid' or `silly' when
S.J. Neill
828 Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832

they consulted their family doctor about their child's
illness. Cunningham-Burley & Maclean (1991) explain
this sensation as related to a possible threat to the
mother's self-esteem, when their ability to mother their
child is open to scrutiny, as it is implicitly when they
need to call on the doctor to help them to care for their
sick child.
Other studies in the area also found that parents were
unhappy with their interactions with their child's GP.
Mayall (1986) found that some mothers (22%, n� 135) felt
that the doctor did not respect their views. Kai (1996b)
found that parents felt their con®dence had been under-
mined by remarks from professionals. While Hopton et al.
(1996) report that some patients felt that they had not been
taken seriously. Although not all the latter ®ndings
originate from parents Ð half the sample concerned adult
patients. Given these reports, the desire to have their
competence as a mother recognized, as identi®ed by
Mayall (1986) and Cunningham-Burley & Maclean (1991)
is predictable. Mothers are reported to want their concerns
to be treated seriously and their knowledge of their child
and the treatment they had already given to be recognized
by the doctor. Interestingly, such comments were not
made when the mothers discussed their interactions with
other health professionals.
MedicationSome of the parents in the research reviewed stated that
their expectations of their consultation with the doctor
was for a prescription (Mayall 1986, Cornford et al. 1993).
Wilson et al.'s (1984) audit of the outcome of consulta-
tions for infants with acute illness identi®ed that 81% of
parents left the surgery with a prescription. Yet in
Cunningham-Burley & Irvine's (1987) paper, mothers are
cited as not expecting a prescription, the `all clear' being
viewed as of more importance. Parents from ethnic
minority groups were, however, identi®ed as more likely
to want prescribed treatment (Clarke & Hewison 1991,
Watson 1991). In Watson's (1991) study the Bengali
mothers are reported to value prescribed treatment highly,
whilst in Clarke & Hewison's (1991) research Muslim
parents were identi®ed as the most likely to want
medications, when compared to White, Sikh and Afro-
Caribbean parents.
Kai's (1996b) study explored the desire for medication
further, through an examination of parents beliefs about
treatment. He found that parents' desire for antibiotics did
not relate to the cause of illness Ð parents did not
understand that antibiotics would be useless against viral
illness Ð but to the parents' perception of the severity of
their child's illness. Cornford et al.'s (1993) ®ndings
support Kai (1996b), as half the parents in this study are
reported to want antibiotics (to kill `germs' and break up
phlegm), especially if the illness was more severe. These
®ndings re¯ect the commonalities between studies
outlined earlier concerning how parents make sense of
their child's illness.
Overall, however, parents did not expect to leave the
surgery with a prescription (Cunningham-Burley & Irvine
1987, Clarke & Hewison 1991), although many received
one (Wilson et al. 1984). In Clarke & Hewison's (1991)
research, when parents were asked what they expected to
get from the doctor, fewer than 20% of families mentioned
antibiotics. The authors state that this is `contrary to a
popular myth among health care providers'. There is an
obvious mismatch here between the desires of parents and
what the GP's provide.
Mismatch between the perceived needsof parents & services provided
This mismatch is illustrated in two ways in the literature
reviewed above: doctors' over-estimation of parents'
expectations of a prescription (Cunningham-Burley &
Irvine 1987, Clarke & Hewison 1991); and parents' lack
of understanding of the rationale for the use of antibiotics,
linking severity of illness, rather than bacterial origin as
the cause of illness, with the need for antibiotics (Kai
1996b, Cornford et al. 1993). A further con¯ict cited in the
latter study, also concerns parents' lack of understanding
of the doctor's diagnostic processes:
Mothers often noted (sometimes with disbelief and even sarcasm)
that the cough appeared chesty to them but that the doctor said
the chest was `clear' after listening with a stethoscope. Cornford
et al. (1993, p. 195)
In addition to these misunderstandings, mothers in Irvine
& Cunningham-Burley's (1991) research, comment that
their competence to care for their child is questioned and
that they are made to `feel stupid' when they consulted the
GP. Callery (1997) discusses this con¯ict between
maternal and professional knowledge at some length,
identifying the power relationships which exist between
lay and professional groups. Consequently this discussion
will not be explored again here. It is evident however, that
considerable mutual dissatisfaction is likely to exist (Kai
1996a).
DIRECTIONS FOR FUTURE RESEARCH
Although the research reviewed answers the questions set
(see Figure 4 for an overview of the answers to the
questions set for the review), the depth of the under-
standing of parents' and families' experiences when their
child is acutely ill at home is limited, as is the general-
izability of the research.
There is minimal evidence gathered from any family
member other than mothers. The lay network is referred to
but not explored. Given that the majority of childhood
acute illness at home is managed by families without
Integrative literature reviews and meta-analyses Acute childhood illness at home
Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832 829

reference to health care professionals, this lay network
needs further investigation. There is scope here for
research which explores the dynamics occurring in fami-
lies during childhood illness and the relationship to help
seeking behaviours and health service use.
The experiences of families in the South of England and
those in rural areas are under-represented across the
research. Qualitative research with minority ethnic groups
is absent, re¯ecting the tendency for qualitative studies to
focus on the dominant white population. Generally much
of the research to date, is grounded in a Eurocentric
understanding of illness (Webb 1996). There is a need to
explore the experiences and perceptions of rural commu-
nities and ethnic minority groups in relation to acute
childhood ill health, if services are to be designed to meet
their needs. This review has concentrated on the literature
from the UK. Clearly there is also a need in an age of
globalization for international and cross-cultural studies.
The role of other health care professionals does not
appear within the research. The impact of new service
developments such as: NHS Direct, GP co-operatives,
ambulatory care centres and the expansion, albeit slow, of
Community Children's Services, need to be assessed for
this client group.
Research is needed which will help to direct the future
development of services designed to meet the needs of
services users, within the context of the resource
constraints in today's British National Health Services
with its emphasis on clinical effectiveness and ef®ciency.
Services targeted to meet the needs of child and families
as identi®ed by the clients themselves have the potential
to facilitate the development of effective services.
Acknowledgements
Professor Jackie Campbell, Head of Research and Consul-
tancy, Centre for Healthcare Education, University College
Northampton.
References
Blakiston's Pocket Medical Dictionary (1979) 4th edn. McGraw-
Hill Book Company, New York.
Callery P. (1997) Maternal knowledge and professional knowl-
edge: co-operation & con¯ict in the care of sick children.
International Journal of Nursing Studies 43, 27±34.
Cantrill J.A., Johannesson B., Nicolson M. & Noyce P.R. (1996)
Management of minor ailments in primary schoolchildren in
Figure 4 Summary: review of the questions set for the literature review.
S.J. Neill
830 Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832

rural and urban areas. Child: Care, Health and Development 22,
167±174.
Central Statistical Of®ce (1994) Social Focus on Children. HMSO,
London.
Clarke A. & Hewison J. (1991) Whether or not to consult a
general practitioner. decision-making by parents in a multi-
ethnic inner city area. In Child Health Matters (Wyke S. &
Hewison J. eds) Open University Press, Milton Keynes,
pp. 74±87.
Cleary J. (1992) Caring for Children in Hospital. Parents and
Nurses in Partnership. Scutari Press, London.
Cornford C.S., Morgan M. & Ridsdale L. (1993) Why do mothers
consult when their children cough? Family Practice 10,
193±196.
Copeland L.G. & Clements D.B. (1993) Parental perceptions and
support strategies in caring for a child with a chronic
condition. Issues in Comprehensive Pediatric Nursing 16,
109±121.
Cunningham-Burley S. (1990) Mothers beliefs about and percep-
tions of their children's illnesses. In Readings in Medical
Sociology (Cunningham-Burley S. & McKeganey N.P. eds)
Tavistock/Routledge, London, pp. 85±109.
Cunningham-Burley S. & Irvine S. (1987) `And have you done
anything so far?' An examination of lay treatment of children's
symptoms. British Medical Journal 295, 700±702.
Cunningham-Burley S. & Maclean U. (1987) The role of the
chemist in primary health care for children with minor
complaints. Social Science and Medicine 24, 371±377.
Cunningham-Burley S. & Maclean U. (1988) Pharmacists and
primary care: some research ®ndings and recommendations.
Family Practice 5, 122±125.
Cunningham-Burley S. & Maclean U. (1991) Dealing with chil-
dren's illness. Mothers' dilemmas. In Child Health Matters
(Wyke S. & Hewison J. eds), Open University Press, Milton
Keynes, pp. 29±39.
Darbyshire P. (1994) Living with a Sick Child in Hospital. the
Experiences of Parents and Nurses. Chapman & Hall, London.
Derouin D. & Jessee P.O. (1996) Impact of Chronic Illness on
Childhood: Siblings' Perceptions. Issues in Comprehensive
Pediatric Nursing 19, 135±147.
Droogan J. & Song F. (1996) (.)) The process and importance of
systematic reviews. Nurse Researcher 4, 15±26.
Evans M.A. (1994) An. investigation into the feasibility of
parental participation in the nursing care of their child. Journal
of Advanced Nursing 20, 477±482.
Gillam S.J., Jarman B., White P. & Law R. (1989) (.)) Ethnic
differences in consultation rates in urban general practice.
British Medical Journal 299, 953±957.
Gould D. (1994) Writing literature reviews. Nurse Researcher 2,
17±27.
Graham H. (1994) The changing ®nancial circumstances of
households with children. Children and Society 8, 98±113.
Health Committee (1997) Third Report. Health Services for
Children and Young People in the Community. Home and
School. House of Commons Session 1996±7. The Stationery
Of®ce, London.
Hill D.S. (1993) Coordinating a multidisciplinary discharge for
the technology-dependent child based on parental needs.
Issues in Comprehensive Pediatric Nursing 16, 229±238.
Holme C. (1995) Incidence and prevalence of non-speci®c symp-
toms and behavioural changes in infants under the age of two
years. British Journal of General Practice 45, 65±69.
Hopton J., Hogg R. & McKee I. (1996) Patients' accounts of calling
the doctor out of hours: qualitative study in one general
practice. British Medical Journal 313, 991±994.
Irvine S. & Cunningham-Burley S. (1991) Mothers' concept of
normality, behavioural change and illness in their children.
British Journal of General Practice 41, 371±374.
Kai J. (1996a) What worried parents when their pre-school
children are acutely ill, and why: a qualitative study. British
Medical Journal 313, 983±986.
Kai J. (1996b) Parents' dif®culties and information needs in
coping with acute illness in preschool children: a qualitative
study. British Medical Journal 313, 987±990.
Kna¯ K.A., Cavallari K.A. & Dixon D.M. (1988) Pediatric Hospi-
talization. Family and Nurse Perspectives. Scott, Forseman &
Co., Glenview, Illinois.
Leicester City Council (1997) Annual Report of the Director of
Public Health, Leicestershire, 1996±7. Leicester City Council.
Leicester.
MacDonald M. (1988) Children discharged from hospital Ð what
mothers want to know. Nursing Times 84, 63.
Mayall B. (1986) Keeping Children Healthy. Allen & Unwin,
London.
McCormick A., Fleming D. & Charlton J. (1995) Morbidity Statis-
tics from General Practice 1991±2. Series MB5, no. 3. Of®ce of
Population Census and Survey, HMSO, London.
McKenna S.P. & Hunt S.M. (1994) A. measure of family disrup-
tion for use in chickenpox and other childhood illnesses. Social
Science and Medicine 38, 725±731.
Morrison J.M., Gilmour H. & Sullivan F. (1991) Children seen
frequently out of hours in one general practice. British Medical
Journal 303, 1111±1114.
NHS Centre for Reviews and Dissemination (1996) Understanding
Systematic Reviews of Research on Effectiveness. CRD Guide-
lines for Those Carrying Out or Commissioning Reviews. CRD
Report 4. University of York. NHS Centre for Reviews and
Dissemination, York.
Neill S.J. (1996) Parent participation. Part 1 and 2. British Journal
of Nursing 5, 34±40, 110±117.
Oakley A., Hickey D. & Rigby A.S. (1994) Love or money? Social
support, class inequality and the health of women and chil-
dren. European Journal of Public Health 4, 265±273.
Pearson P. (1995) Client views of health visiting. In Researching
User Perspectives on Community Health Care (Heyman B. eds),
Chapman & Hall. London, pp. 106±120.
Reading R. (1997) Poverty and the health of children and
adolescents. Archives of Disease in Childhood 76, 463±467.
Rennick J.E. (1995) The changing pro®le of acute childhood
illness: a need for the development of family nursing knowl-
edge. Journal of Advanced Nursing 22, 258±266.
Richardson M., Student E., O'Boyle D., Smyth M. & Wilkins
Wheeler T. (1992) Establishment of a state-supported, special-
ized home care program for children with complex health-
care needs. Issues in Comprehensive Pediatric Nursing 15,
93±122.
Royal College of Nursing (1995) Philosophy of Paediatric Nursing.
Royal College of Nursing, London.
Integrative literature reviews and meta-analyses Acute childhood illness at home
Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832 831

Sandelowski (1995) Qualitative data analysis. what it is and
where to begin. Research in Nursing and Health 18, 371±375.
Saxena S., Majeed A. & Jones M. (1999) Socioeconomic differ-
ences in childhood consultation rates in general practice in
England & Wales: prospective cohort study. British Medical
Journal 318, 642±646.
Spencer N.J. (1984) Parents' recognition of the ill child. In
Progress in Child Health, Volume 1. (Macfarlane J.A. eds),
Churchill Livingstone, Edinburgh, pp. 100±112.
Taylor R.J. (1995) Minor illness in infants Ð still a major worry for
parents? British Journal of General Practice 45, 62±63.
Townsend P., Whitehead M. & Davidson N., eds (1992) Inequal-
ities in Health: the Black Report and the Health Divide.
Penguin, London.
Watson E. (1991) `Appropriate' use of child health services in East
London: ethnic similarities and differences. In Child Health
Matters (Wyke S. & Hewison J. eds), Open University Press.
Milton Keynes, pp. 88±109.
Webb E. (1996) Meeting the needs of minority ethnic groups.
Archive of Disease in Childhood 74, 264±267.
Whyte D.A. (1994) Family Nursing. The Case of Cystic Fibrosis.
Avebury, Aldershot.
Wilson A.D., Downham M.A.P.S. & Forster D.P. (1984) Acute
illness in infants: a general practice study. Journal of the Royal
College of General Practice 34, 155±159.
Wyke S., Hewison J. & Russell I.T. (1990) Respiratory illness in
children: what makes parents decide to consult? British Journal
of General Practice 40, 226±229.
Wyke S., Hewison J. & Russell I.T. (1991) Children with cough:
who consults the doctor. In Child Health Matters (Wyke S.
& Hewison J. eds), Open University Press, Milton Keynes,
pp. 67±73.
S.J. Neill
832 Ó 2000 Blackwell Science Ltd, Journal of Advanced Nursing, 31(4), 821±832





























